Chapter 19
1/47
Earn XP
Description and Tags
Thorax and Lungs
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
48 Terms
What brain regions control breathing?
Medulla and pons (involuntary control)
Neuro pop quiz - brain damage to medulla and pons caused what type of posturing?
Decerebrate posturing!! Very bad
If a COPD has an O2 sat of 88%, why can’t you just give them enough oxygen to get up to 95% + ?
COPD pts have high CO2 already, so their bodies stop using CO2 as a trigger and rely on low O2 levels to tell them to breathe (aka hypoxic drive)
So if u give them O2, it makes the brain think they don’t need to breathe → causing resp failure
When a pt uses ____ muscles for breathing, this is indicative of COPD. Why?
accessory
Diaphragm becomes flattened and less effective, so COPD pts use accessory muscles to increases expansion and lets more air in
What accessory muscles are used in COPD pts?
Sternocleidomastoid
Scalene
Trapezius
Intercostal
Abdominal muscles
Injury to ___ results in loss of diaphragm function
spinal cord above C3
C3 → phrenic nerve, which controls diaphragm
Inspiration/increase in chest cavity → ____ pressure
Expiration/decrease in chest cavity → ____ pressure
inspiration: less pressure in lungs
expiration: greater pressure lungs
What are some subjective questions to ask for lung/thorax issues?
coldspa for dyspnea
cough sx
medications
chest pain
smoking hx
family hx
lifestyle (exercise, smoking)
pack years
How would you differentiate dyspnea that is caused by cardiac vs lung/thorax issues?
when do you experience orthopnea/SOB
while laying down: cardiac
all the time: lung/thorax
do you experience SOB that wakes you up at night?
indicative of HF, COPD, asthma
Why do you ask about medications when assessing cough?
Some meds, like ACE-inhibitors and beta-blockers, cause a dry nonproductive cough
A continuous cough is often linked to… ?
Acute infection
An early morning cough is linked to…?
Chronic bronchial inflammation or smoking
An evening cough may be caused by…?
Daytime irritant exposure
A nighttime cough may associated with…?
Post nasal drip or sinusitis
How can you differentiate heart/lung/GI related chest pain?
Cardiac: chest pain upon exertion
GI: heartburn, tummy issues, relieved by antacids
Lung: green sputum + fever (resp infection)
Describe what some sputum colors could indicate
White - viral/cold
Yellow/green - bacterial
Rust - pneumonia/TB
Pink/frothy - pulmonary edema
Brown/black - blood maybe
Odee sputum - irritation, chronic bronchitis, infection
Thique sputum - dehydration
What’s a pack year? How do you calculate it?
A value that helps determine a pt’s risk of cancer
(# of packs per day) * (# of years smoked)
What pack year value warrants screening?
20 pack year history b/w ages of 50-80; they need yearly screening
COLDSPA for dyspnea
C - describe difficulty breathing
O - when did it begin?
L - N/A
D - how long do episodes last?
S - impact on ADLs
P - what aggravates/relieves it?
A - cough, edema, chest pain, sputum
What can tripod positioning in adults indicate?
COPD
What is an abnormal finding in the AP diameter assessment
1:1 ratio, which would indicate a barrel chest due to chronic lung hyperinflation (emphysema)
How does pectus excavatum (funnel chest) look like?
A sunken sternum
How does pectus carinatum (pigeon chest) look like?
Protruding sternum
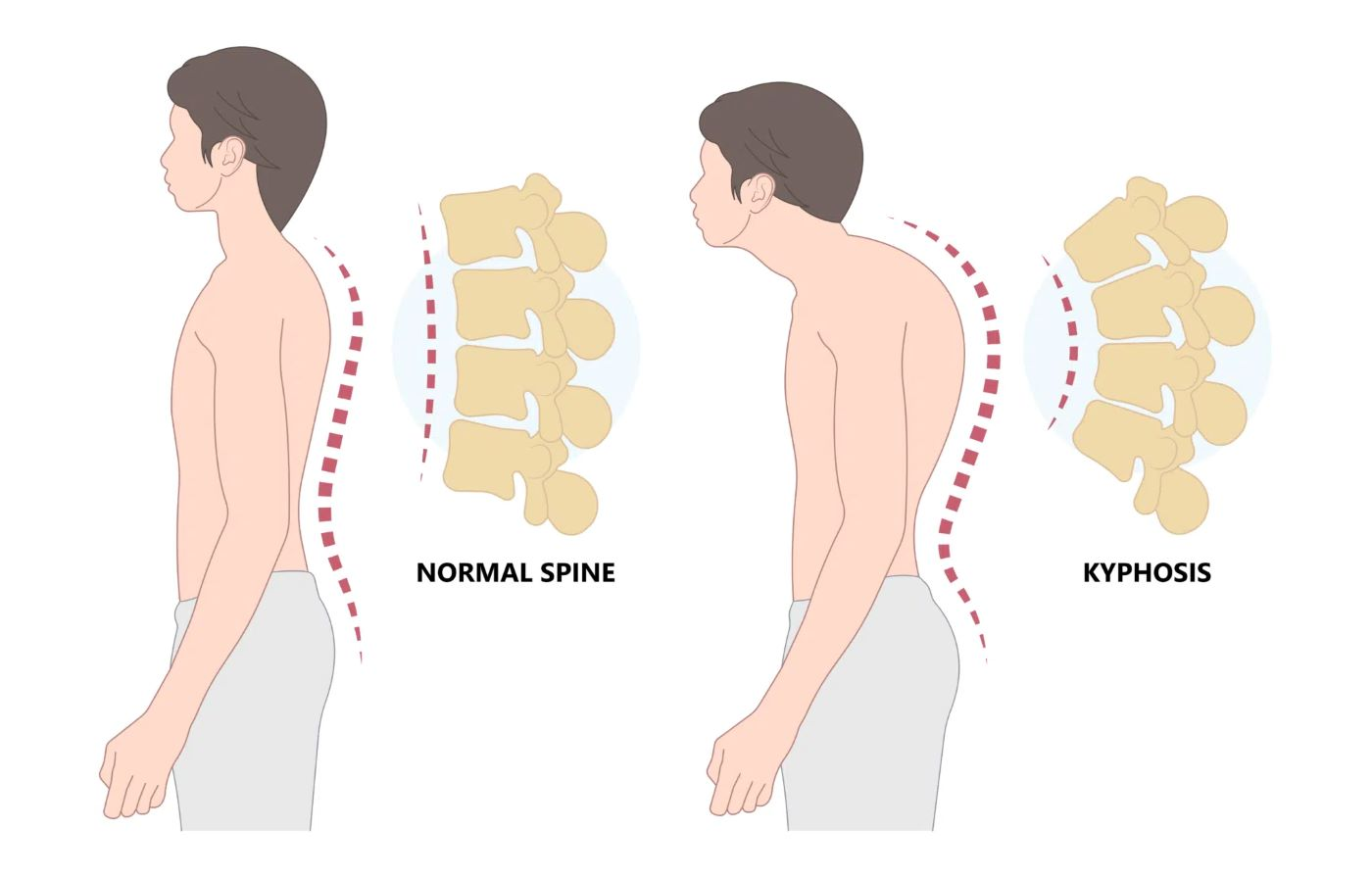
Is kyphosis normal in older adults?
Yea, but not great since it decreases lung expansion capacity
How do you assess ease of respirations?
Check for:
pursed lip breathing
nasal flaring
accessory muscle use
What is fremitus?
Transmission of sound (air) through lung tissue
How do you assess for fremitus?
Have pt say 99 repeatedly and feel the vibration each time in diff parts of the pt’s back
It should be rlly clear near clavicles and decrease in intensity as you go down to lung bases
Increased fremitus means…?
Decreased fremintus means…?
Increased - consolidation (from fluid, blood, pus, pneumonia)
Decreased - excess air (copd, emphysema)
Think - sound travels faster in water than air
What’s creptius?
Rice-krispie/crackly noise that happens when you palpate b/c of air escaping into fatty tissue
What would unequal chest expansion mean?
Pneumonia, pneumothorax, atelactasis
What does diaphragmatic excursion measure?
The expansion of lungs during respiration
Explain the difference b/w atelectasis and pneumothorax
atelactasis: collapse of alveoli due to blockage or external pressure
pneumothorax: collapsed lung b/c of air leaking into the space b/w the lung and chest wall
What are the 5 different sounds you’re listening to when percussing?
1 - resonance: normal lung sound; medium loud, low pitch, hollow
2 - tympanic: drum-like, normal over tummy
3 - dullness: over solid organs OR consolidated lung, tumor, pleural effusion
4 - flatness: over bone
5 - hyperresonance: mad loud, low pitch, seen in emphysema or pneumothorax
Why would a tympanic sound over the thorax indicate large pneumothorax?
Pneumothorax happens when air enters pleural space. That air displaces the lung tissue and fills the pleural space, causing the drum-like tympanic sound that is heard over air-filled spaces
Think of it this way - odee air in lungs = giant resonant drum = tympanic drum-like
If an abnormal sound is heard, what should you do?
Have the pt cough, then reassess
What are the 3 normal breath sounds? Where are they located and how long are their inspiration/expiration?
1 - bronchial: hurd near trachea and thorax; short inspiration and long expiration
2 - bronchovesicular: near sternum and b/w shoulder blades; equal inspiration/expiration
3 - vesicular: near peripheral lung fields; long inspiration and short expiration
How would the trachea move in obstructive atelectasis?
trachea shifts towards the affected side, causing less breath sounds
loss of air volume creates pulling affect, so it pulls the trachea
How would the trachea move in pneumothorax?
trachea shifts away from affected side, causing absent breath sounds
buildup of air pushes trachea away
How would the trachea move in pleural effusion/hemothorax?
trachea shifts away, so there’s absent sounds over affected area
buildup of fluid pushes trachea away
What auscultation sound would be present in emphysema?
prolonged breath sounds/air-trapping—> so hyperresonance
How do you assess for bronchophony? What would an abnormal finding mean?
Ask pt to say “99” and see if it sounds muffled (normal) or clear (abnormal)
Abnormal finding indicates lung consolidation
How do you assess for egophony? What would an abnormal finding mean?
Ask pt to say “E” and see if it sounds like eee (normal) or aaa (abnormal)
Abnormal finding means lung consolidation or compression
How do you assess for whisphered pectoriloquy? What would an abnormal finding mean?
Ask pt to whisper “1-2-3” and see if it sounds faint/inaudible (normal) or clear (abnormal)
Abnormal findins means lung consolidation or compression
List some adventitious sounds you may hear and what it can indicate
Crackles - fluid in alveoli → HF, pulmonary edema OR COPD, asthma, emphysema
Wheezes - asthma, emphysema
Friction rub - pleuritis
Stridor - harsh honking, airway obstruction (PRIORITY PATIENT!!!)
What’s the difference b/w sibilant and sonorous wheezes?
They differ in pitch and underlying cause
Sibilant - musical pitch; cause by asthma/emphysema
Sonorous - low pitch snoring; seen in bronchitis
What is normal lung/thorax stuff in older adults?
kyphosis (curved thoracic spine)
reduced lung expansion
weak cough reflex
higher risk of pneumonia, atelectasis
few functioning alveoli
sternum/ribs are more prominent b/c of less fat
What are two major lung cancer risk factors
Smoking and radon
Bronchophony, egophony, and whispered pectoriloquy are all positive in pneumonia - why?
B/c there’s excess fluid in the lungs, and sound travels better in liquid/solid than in air