OPP OMS 1 Sem 2
1/99
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
100 Terms
what are the axes of SI and IS motion?
SI → sacral flex/extend @ middle transverse (S2)
IS → innominate/pelvic @ inf. transverse axis (S3)
NOTE: respiratory/cranial @ sup. transverse (S2)
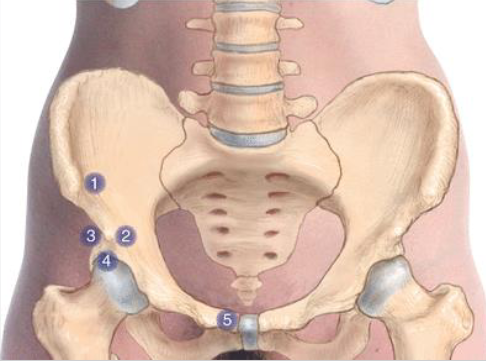
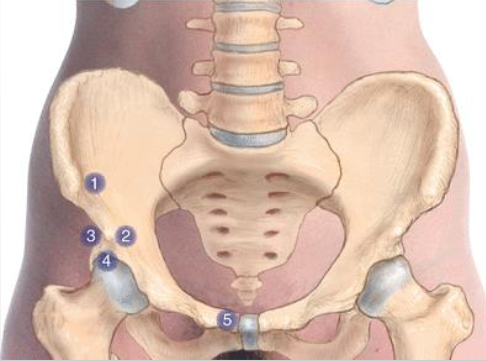
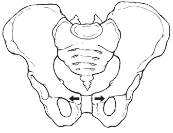
what are the landmarks for a pelvic diagnosis?
Iliac crest
ASIS + PSIS → thumbs inf. (height + width)
pubic tubercle → sup. surface
medial malleolus → thumbs inf.
what are the indications for CS?
lawrence jones, 1955
acute injury
neural component (hyper shortened)/ hypertonic
hospitalized/ frail
other treatment uncomfortable
what are the absolute contraindications for CS?
lack of consent
can’t tolerate position (acute fracture, torn ligament) or exacerbates
neuro symptoms manifest
vascular /neuro syndrome (basilar insufficiency, neuroforaminal compromise)
degenerative spondylosis w/ local fusion
what are relative contraindications to counterstrain?
pt. can’t relax/apprehension/can’t tolerate
upper cervical hyper rotation/extension w/ vertebral a. disease or lig. instability, dens malformation, osteoporosis
severe acute rheumatological flare
CT disease, arthritis, parkinson’s
what are the steps of CS?
contact tender pt. → establish 10/10
place pt. in position of ease until tenderness reduced by 70%
hold 90 seconds
passively to neutral
reassess (dec. 70%)
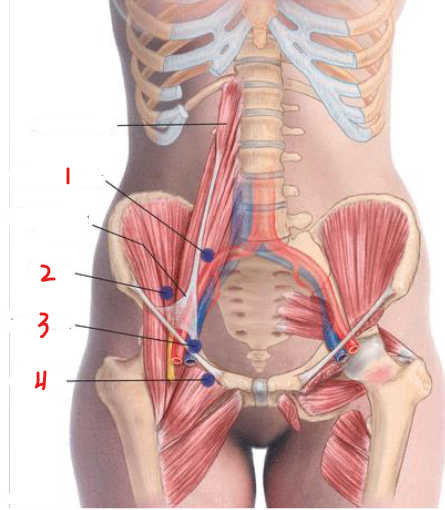
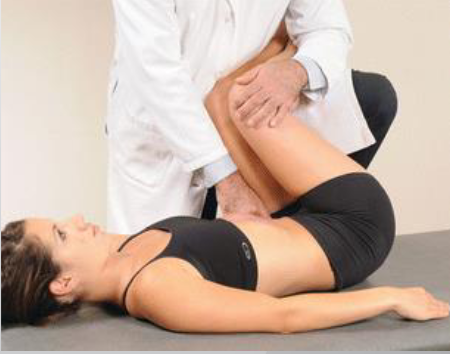
psoas CS?
2/3 from ASIS to midline, deep
hip flexion, SB lumbar spine towards, some hip ER
F ST er
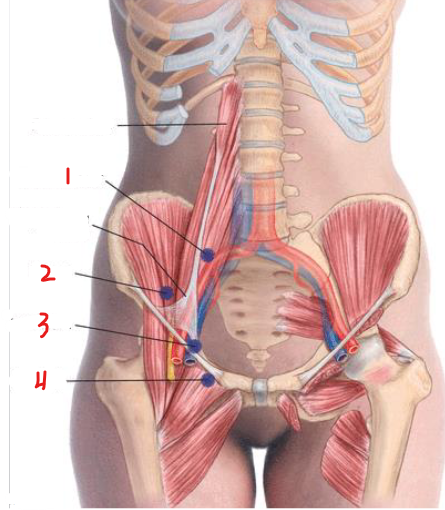
iliacus CS?
1/3 from ASIS to midline, deep post. lat.
hip flexion, hip ER + knee flexed
F ER
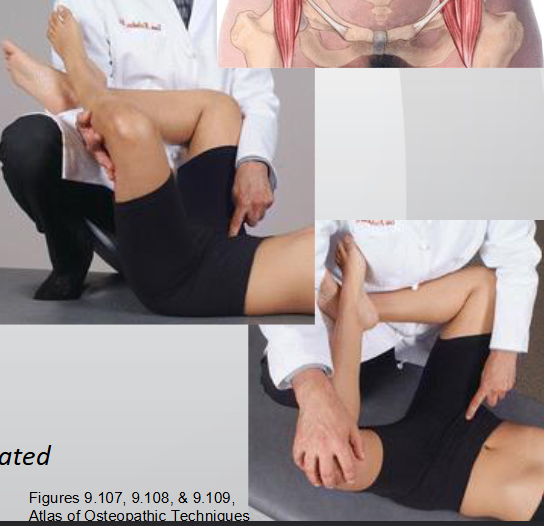
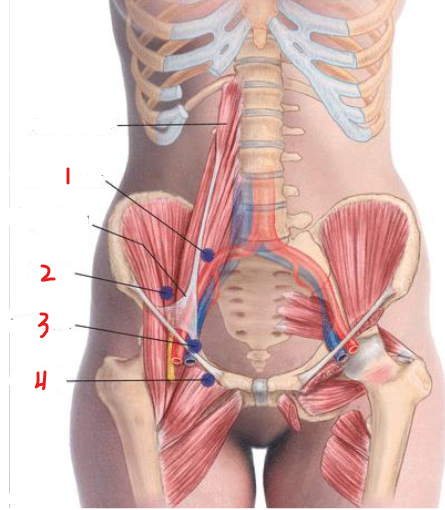
low ilium CS?
sup. ilio pubic eminence
ipsilateral hip flexion
F

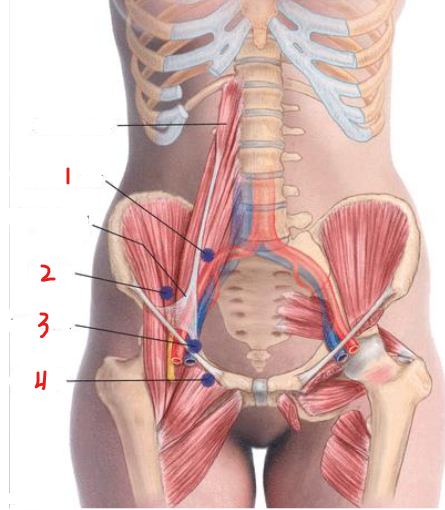
inguinal CS?
lat. pubic tubercle
thigh flex w/ good over evil, ipsilateral lower leg pulled lat. for IR of affected hip
F ADD IR
AL1 + AL5 CS?
stand on same side, pt. supine w/ hips + knees flexed
flex to level, side bend (ankles), knees (pelvis) toward → rotates torso + segment away
AL1 → F St RA (StaR)
AL5 → F SA Ra (SaRa)

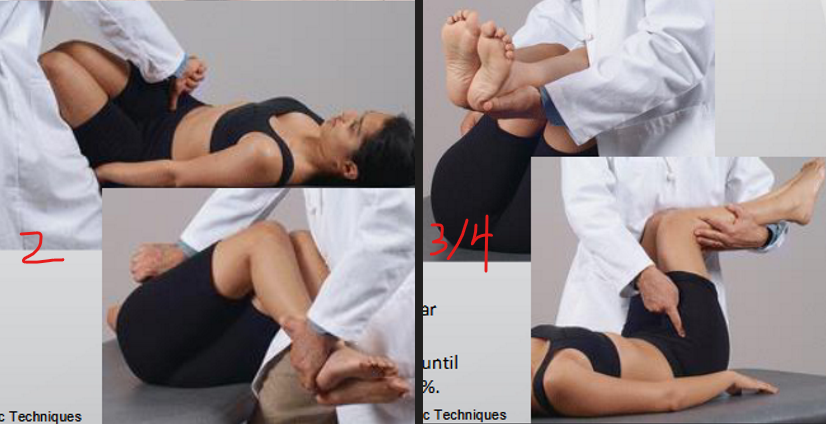
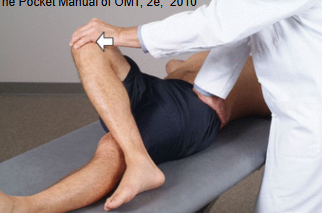
AL2, AL3, AL4 CS?
stand on opposite side, pt. supine w/ hips + knees flexed
med., lat., inf. to AIIS
flex to level, SB away → rotates torsos + segment toward
AL2 → SB @ ankle
AL3/4 → SB @ knees
F SA RT
tender vs trigger
tender:
locally tender + jump response
NO pain pattern + NO radiating pain
in muscle, tendon, etc.
trigger:
locally tender + jump response
pain pattern + radiating pain
in muscle + in taut band of tissue
twitch response
dermographia
how to lateralize the pelvis + sacrum?
standing flexion test (pelvis), seated flexion test (sacrum)
lateralize to side that is most superior
ASIS compression test (post. med)
lateralize to side that is more stiff
how do you diagnose the pelvis?
assess PSIS, ASIS (+ midline distance), pubic tubercle, medial malleolus
record relative to lateralized side (i.e L lateralization → left ASIS sup. or inf.)
what are the characteristics of an anteriorly rotated innominate SD?
on lateralized side → ASIS inf., PSIS sup., MM long, PT slight inf.
on opposite side → ASIS sup., PSIS inf., MM short
what are the characteristics of a posteriorly rotated innominate SD?
on lateralized side → ASIS sup., PSIS inf., MM short, PT slight sup.
on opposite side → ASIS inf., PSIS sup., MM long
what are the characteristics of an innominate outflare + inflare SD?
outflare (rotated out) → (on lateralized side) ASIS lat. + PSIS med. towards lateralized side
inflare (rotated in) → (on lateralized side) ASIS med. + PSIS lat. towards lateralized side
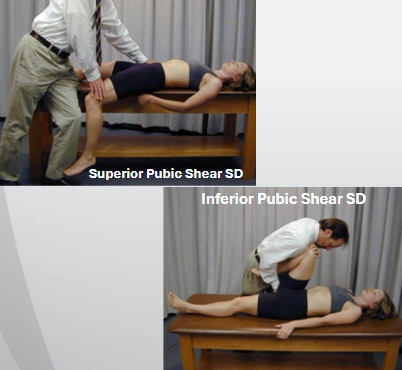
what are the characteristics of a superior and inferior pubic shear?
sup. shear → ASIS sup. MM short, PSIS sup., PT sup.
inf. shear → ASIS inf., MM long, PSIS, inf., PT inf.
indications for ME?
myofascial SD (dec. hypertonicity, lengthen muscle, stretch), SD of articular origin (mobilize joint, improve ROM)
improve circulation/respiration, inc. muscle tone
absolute contraindications for ME?
fracture/dislocation in region
lack of consent/cooperation
lack of SD
relative contraindications for ME?
moderate/severe strains
severe osteoporosis
severe illness (post. surg./ICU)
innominate PIR ME anterior rotation SD treatment?
pt. supine, stand on involved side
flex, ER, ABduct hip
pull ischial tuberosity ant
pt. push against shoulder (3-5x, 3-5 sec, 3-5 oz, 2 sec. relax)

innominate PIR ME posterior rotation SD treatment?
pt. supine, stand on involved side
hold opposite ASIS to stabilize
leg + ischium off table → leg extended
pt. push thigh upwards

innominate PIR ME inflare SD treatment?
pt. supine, stand on opposite side holding contralateral hip
flex hip + knee (foot above opposite knee) → ABduct hip (should feel @ ASIS)
pt. push knee up/inwards
innominate PIR ME outflare SD treatment?
pt. supine, stand on involved side (monitor PSIS)
flex hip + knee w/ foot on knee → ADduct knee (should feel @ PSIS)
pt. push knee out

innominate PIR ME shear SD treatment?
pt. supine
ABduct + IR leg to gap SI joint
sup. shear → lean back for traction @ SI joint, pt. hike hip up
inf. shear → compress @ SI joint, pt. push towards you

how to lateralize for sacral/ SI joint diagnosis?
seated flexion test → thumbs under, eye level
higher PSIS → lateralize
ASIS compression test → posterior push (dominant eye over)
more stiff → lateralize
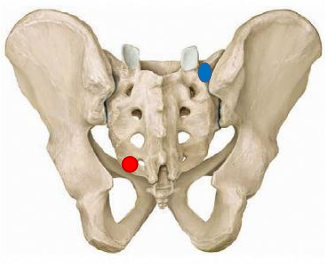
what are landmarks for sacral/SI joint diagnosis?
sacral base
PSIS
sacral sulci → thumbs medial to PSIS, deeper/ant. sulci (+)
ILA → palm on drop off, go lateral, deeper/ant. ILA (+)
what are the special tests for sacral diagnosis? what do positive results determine?
BBT/sphinx test → (+) not improved/worsened symmetry
lumbar spring → (+) lack of spring
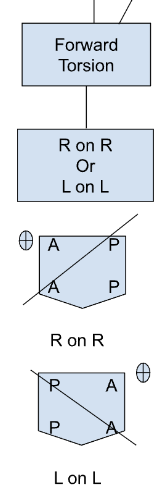
extension/backward torsion
diagnosis of forward sacral torsion?
axis is opp. of lateralization (seated flexion test)
R on R → left sulci + ILA both ant.
L on L → right sulci + ILA both ant.
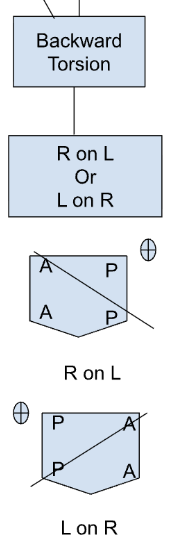
diagnosis of backwards sacral torsion?
axis is opp. of lateralization (seated flexion test)
R on L → right sulci + ILA both post.
L on R → left sulci + ILA both post.
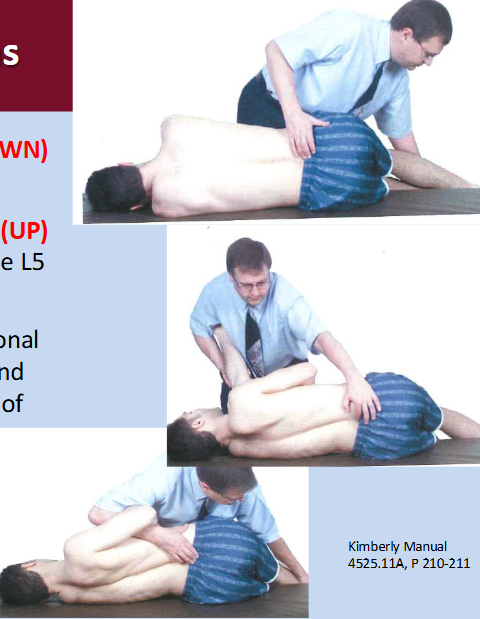
what is the movement of L5 relative to forward and backward torsions?
forward (neutral) → L5 follows Type 1 (NSRRL/NSLRR)
backward (nonneutral) → L5 follows type 2 (FSSRR/FSLRL)
sacrum is extended → L5 has to be flexed
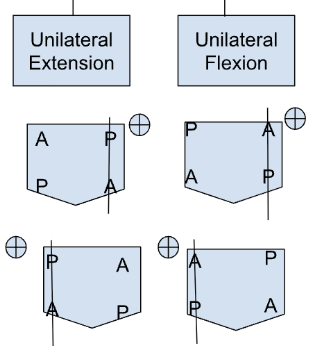
diagnosis of unilateral extension? unilateral flexion?
extension:
lateralized side → sulci post., ILA ant.
other side → opposite
flexion
lateralized side → sulci ant., ILA post.
other side → opposite
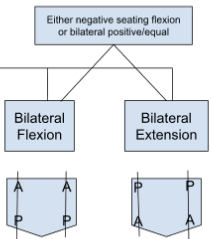
diagnosis of bilateral extension/flexion?
(-) seated flexion OR bilateral (+)/equal
extension → sulci post., ILA ant.
flexion → sulci ant., ILA post.
during what sacral diagnoses is the sacrum extended?
backward torsion
unilateral/bilateral extension
(+) BBT, (+) spring test
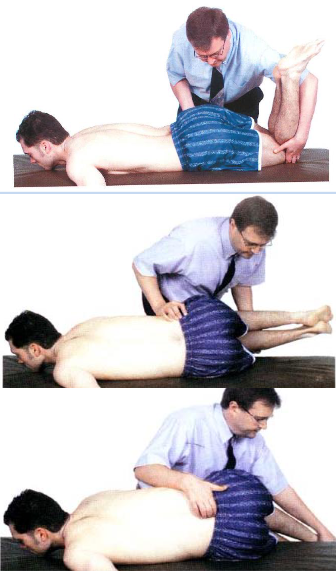
forward sacral torsions MET
side of oblique axis down on table (lateral recumbent)
hug the table, down (rotate to side of oblique axis)
localize sacral base (bend knees + flex hips >90)
drop pt. leg over table, support w/ your knee (down)
pt. lift to ceiling
backward sacral torsion MET
side of oblique axis down (lateral recumbent)
pull on lower shoulder, up (rotate to L5)
localize sacral base (bend knees + flex hips <90)
drop pt. legs over table, support w/ your knee (down)
pt. lift to ceiling
unilateral sacral flexion ME?
pt. prone, stand on opposite side of flexion
palpate flexed sacral sulcus → ABduct pt. same leg (loose SI joint) + IR
heel of caudad hand on ILA w/ cephalad on top → downward force
pt. inhale → resist, pt. exhale → follow (encourage extension)

unilateral sacral extension?
pt. in sphinx, stand on opposite side of extension
caudad hand ABduct pt. same leg (loose SI joint) + IR
hypothenar on sacral sulcus, stabilize w/ caudad on top
inhale → resist, exhale → follow (encourage flexion)

bilateral sacral flexion ME?
place caudad hand on ILA, cephalad reinforce
inhale → force extension
exhalation → downward pressure (prevent flexion)

bilateral sacral extension ME?
pt. prone OR sphinx
contact sacral sulci w/ caudad hand, cephalad reinforce
inhale → inc. ant. force/resist
exhale → encourage flexion/follow

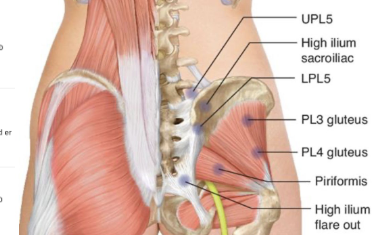
posterior pelvic CS points?
UPL5 (sup. PSIS) → E Add er/ir
high ilium sacroiliac (lat. PSIS, press med.) → E Abd ER
LPL5 (inf. PSIS, press sup.) → F IR Add
high ilium flare out (lat. ILA or coccyx) → E Add
PL3/4 lat. (gluteus medius @ PSIS, TFL) → E Abd er
3 → 2/3 lat. PSIS to TFL
4 → post. margin TFL

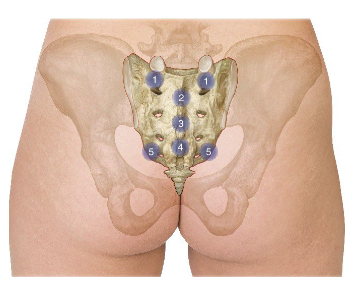
sacral CS points?
PS1 bilateral (med. to PSIS @ S1/sacral base) → PA pressure on opp. ILA
PS2, PS3, PS4 midline (@ level) → F + E
PS5 (med. + sup. to ILA) → PA pressure on opp. sacral base
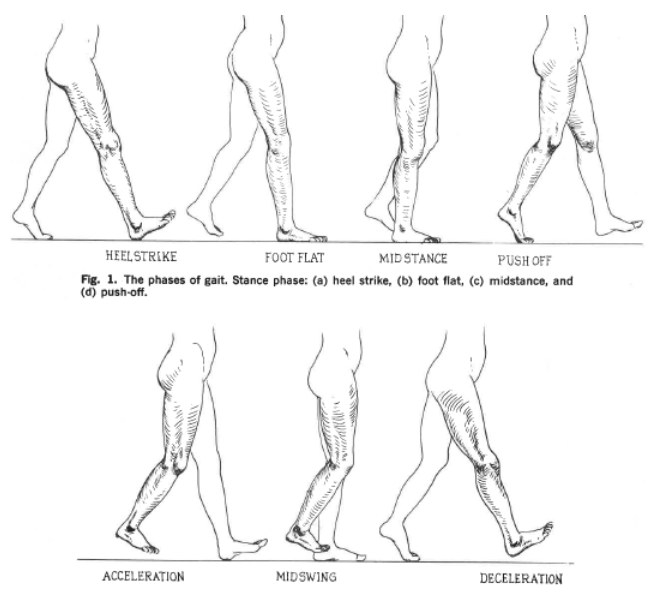
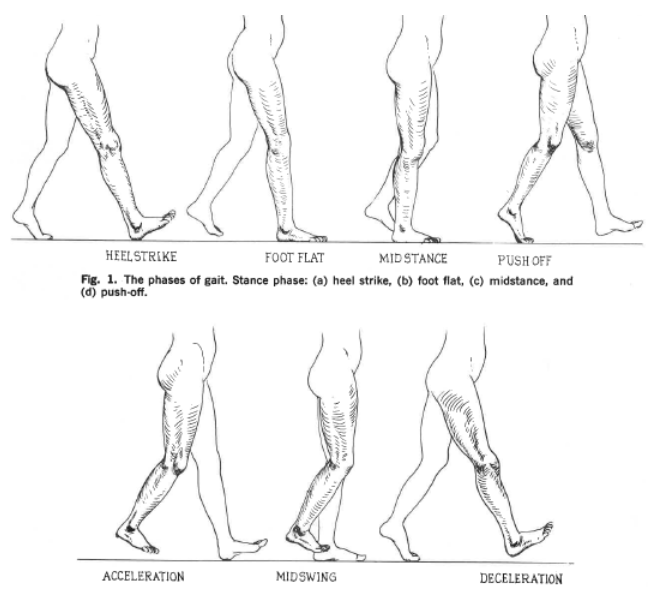
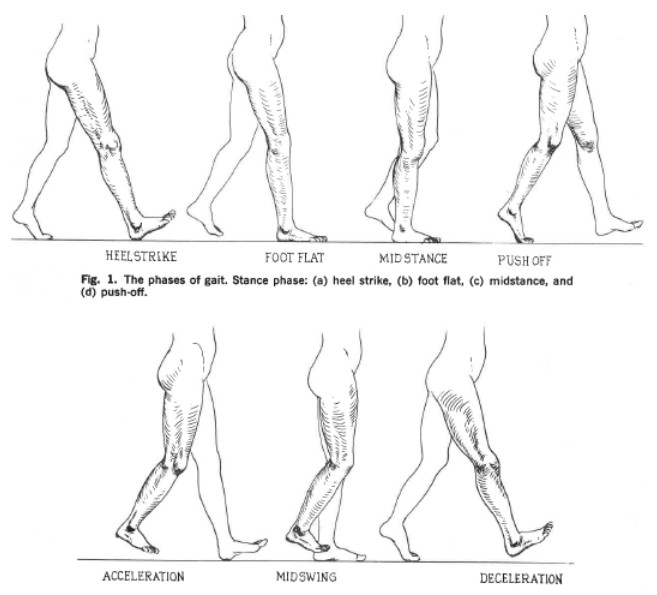
what are the typical phases of gait?
stance (60%): weight shift to R. foot
heel strike, foot flat, midstance (bears weight), push (toe) off
swing phase (40%): R. foot suspended
acceleration, midswing, deceleration
what is innominate motion during gait?
rotation w/ every step
stance phase (heel strike) → post. rotation
swing phase (toe off) → ant. rotation
what is sacral motion when Left vs Right leg is weight bearing?
neutral oblique axis w/ lumbar sidebending towards side of weight bearing leg
L. leg → L rotation on L oblique axis (L/L)
L5 NSLRR
R. leg → R rotation on R oblique axis
L5 NSRRL
what is arm movement during gait?
pendulum → opposite direction of ipsilateral leg
what type of treatment is HVLA?
high velocity, low amplitude
direct + passive
treats joint SD
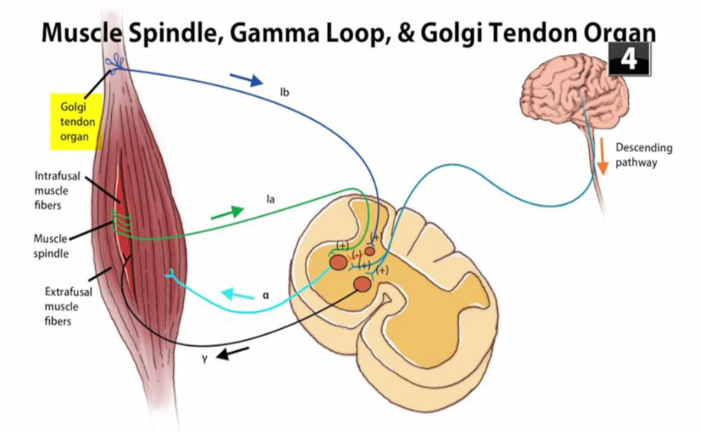
what is the muscle spindle mechanism of HVLA?
joint capsule repositioned → stimulate golgi tendon 1b aff. neuron
synapses w/ inhibitory 1b interneuron → synapse w/ a-motor neuron
muscle relax → ROM improve
what is the mechanism of action of HVLA?
restore articular motion
release entrapped synovial folds
disrupt periarticular/articular micro-adhesions
reset aberrant nociceptive/mechanoreceptor activity
vacuum/cavitation
HVLA indications? dosage?
articular SD
joint motion restriction (distinct, firm articular barrier)
sicker pt. → lower dose
long-term use discouraged
HVLA relative contraindications?
apprehension
acute herniation, radiculopathy, whiplash/sprain
osteopenia/osteoporosis, spondylolisthesis (bone disease)
atypical joint facet, hypermobile state
Hx of inflammatory disorders (RA, SLE, IMD, psoriasis, scleroderma)
implanted devices
HVLA absolute contraindications?
upper cervical (advanced RA, DS, dwarfism, chiari malformation)
fracture/dislocation/spinal or joint instability
joint fusion (ankylosing spondylosis, klippel-feil)
vertebrobasilar insufficiency
acute inflammatory disorders
malignancy
myelopathy, cauda equina/spinal pathology
HVLA approach + after?
approach: diagnose SD w/ firm end feel, localize segment to restrictive barrier, avoid overloading/guarding, release-enhance
after: reassess tissue texture, asymmetry, ROM, tenderness + intersegmental motion @ joint level
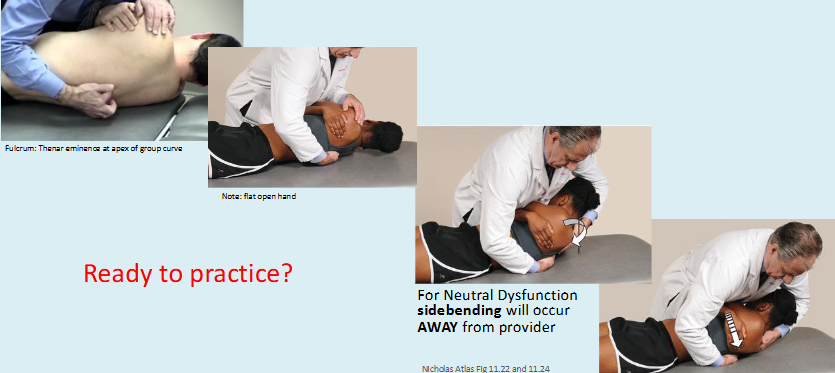
sequence for supine thoracic HVLA?
prepare tissue
stand on opp. side of rotation+ pt. top arm ipsilateral to rotation component
taut thenar eminence over transverse process w/ spinous process in palm
pt. thoracic area relax on fulcrum + adjust in F/E (or N)
localize w/ SB (toward/Type2 or away/Type1)
control over thoracic/head/neck
take up slack w/ exhalation → short + quick thrust @ end of exhalation
supine direct HVLA Type I neutral SD?
extend thorax over fulcrum
SB away from you
thrust perpendicular to fulcrum
supine direct HVLA for Type II flexed SD?
extend thorax to localize
SB towards you (opposite of rotational SD)
force-vector for thrust directed cephalad
reassess

supine direct HVLA for Type II extended SD?
flex thorax
SB towards you (opposite of SD)
force-vector for thrust directed caudad
reassess

crossed-hand prone HVLA for Type II flexed SD?
pt. prone
stand on opp. side of rotation
caudad thenar eminence on post. contralateral transverse process w/ fingers facing sup. (cephalad hand opp. for SB)
take up SB + AP slack w/ exhalation
short + quick thrust @ end of exhalation in direction of fingers
greater pressure on post. transverse process

crossed-hand prone HVLA for Type I neutral SD?
pt. prone
stand on same side of rotation
caudad thenar eminence inf. to opposite transverse process w/ fingers to head (cephalad hand opp. for SB)
move hand fingers pointing to take up slack (eminences should be level w/ process now)
short + quick thrust @ end of exhalation
greater pressure on post. transverse process

HVLA L1-L5 Type I Neutral long-lever SD?
pt. lat. recumbent (rotation side down) w/ DO face pt.
palpate under segment → flex knee + hip until segment neutral
pt. drops top leg over side of table until detect motion at segment
switch palpation hand → cephalad hand through elbow w/ forearm on pec/shoulder
caudad forearm btwn PSIS + greater trochanter
pelvis rotated ant. + shoulder/spine rotated post. → take up slack w/ exhalation
force vector towards spine

HVLA L1-L5 Type II non-Neutral (flexion) long-lever SD?
pt. lat. recumbent (rotation side down) w/ DO facing pt.
palpate under segment → extend (push legs/pelvis post.)
restrict top leg → pt. extend bottom leg → place ankle in popliteal fossa
switch monitor hands → pull pt. bottom arm forward until rotation felt under segment
caudad forearm post. to greater trochanter + cephalad hand grasping elbow
force vector → shoulder caudad + pelvis cephalad

superior pubic shear ME? inferior pubic shear ME?
sup.: leg off table w/ ischial tuberosity on table + support opp. ASIS→ pt. push up + slight medial
inf.: flex + ADduct hip, support ipsilateral ischial tuberosity → pt. push knee into your shoulder

pubic compression ME?
flex hips + knees w/ feet on table
ABduct knees w/ forearm btwn knees
pt. ADduct (pull in) against force
3-5 sec force, 2 sec relax, 3-5x
revaluate
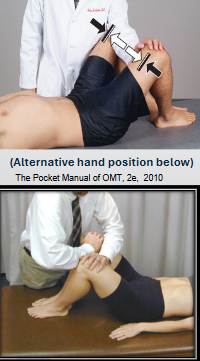
pubic gapping ME?
note: end of midterm
flex hips + knees w/ feet on table
ABduct knees (~18 inches) → ADduct knees while pt. ABduct against force
3-5 sec force, 2 sec relax, 3-5x
revaluate

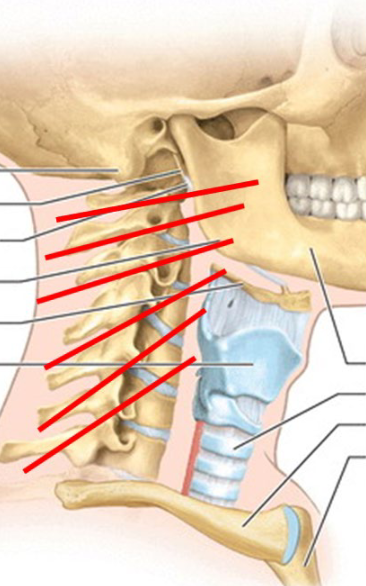
anterior cervical anatomical landmarks? posterior?
ant.:
hyoid → C2-C4
thyroid cartilage → C4-C5
cricoid cartilage → C6
suprasternal notch → T2
post.:
bump under inion → C2
prominent spinous process → C7
what is the structure of C1 and C2?
C1 (atlas) → ring shaped, no body or spinous process
C2 (axis) → anatomically atypical, but functionally typical
odontoid process (dens)
major motions of the cervical region? what is the diagnosis?
OA → flex/extend
Dx: SB + rotate opposite (type 1)
translate ease → opp. SB
AA → rotational
Dx: only rotation
C2-C7 → rotation + SB, flex/extend
Dx: SB + rotate same (type 2)
translate ease → opp. SB
cervical facet orientation? when do facets open?
facet orientation → BUM (facets open w/ flex)
upper facets (C2-C3) → angled near transverse plane
lower facets (C4-C7) → angle tangential to transverse + coronal plane
facets/articular pillars open w/ flexion (forward bending)
w/ SB + rotation → contralateral side open
indications of soft tissue? relative contraindications?
indications: hypertonic muscles, tension in fascia, improving circulation, preparation, abnormal visceral/somatic reflex
relative CI: fracture/open wound, ST/bony infection, abscess, DVT, coagulopathy, neoplasm, directly over site of recent operation
absolute → lack of consent
characteristics of soft tissue technique?
direct/passive
low amplitude, rhythmic
mechanisms:
deep pressure → sustained inhibitory pressure
kneading → rhythmic, lat./perp. stretch
traction → sustained linear force, long. separation of myofascial structures
other mechanisms of soft tissue technique?
effleurage → stroking distal to prox., move fluid
petrissage → deep kneading/squeezing express fluid
tapotement → strike muscle belly, inc. tone + perfusion
skin rolling → myofascial release, break adhesive bands
suboccipital inhibition vs release ST techniques?
inhibition → bilateral ant. force (to ceiling)
release → @ C2, ant. force + cephalad traction

cervical supine vs longitudinal traction ST technique?
supine → cradle occiput + under mandible, f + cephalad traction
longitudinal → contact cervical paravertebral muscles, ant. force + cephalad traction

cervical longitudinal vs contralateral kneading ST technique?
longitudinal → contact cervical paravertebral muscles, ant. force + cephalad traction rhythmic
contralateral → caudad hand contact cervical paraspinal + draw ant. rhythmically, cephalad hand stabilize forehead

cervical forward bending forearm fulcrum bilateral vs unilateral ST technique?
bilateral (FB) → cross arms under head + palms on shoulders, flex neck
unilateral (FB, SB, R) → flex head w/ one hand, slide 2nd hand over opp. shoulder, rotate head along forearm to elbow until tension felt

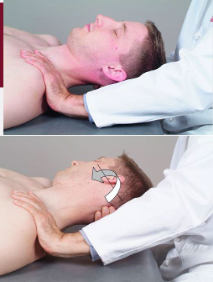
supine lateral traction w/ shoulder cervical ST technique?
one hand on pt. AC joint on side of treatment
other hand under occiput from other side→ gently rotate head away from treatment side
until tension felt → return to neutral
CS indications + contraindications?
indications: tender pt., acute injury, SD, hospitalized/frail, hypertonic muscle
relative CI: can’t relax/tolerate/comm., vert. a. disease, upper cervical (lig., dens, osteoporosis), RA, arthritis, PD
absolute: lack consent, neurological symptoms, degenerative spondylosis
what are the components of muscle tone?
intrafusal fibers → muscle length
GTO → tendon tension
yMNs → regulate gain of stretch reflex via adjusting intrafusal fibers
sets baseline act. in aMNs
pathophysiology of a CS tender point?
agonist contract → muscle spindle lengthens → CNS inc. y eff. to tighten
lengthens antagonist → CNS detects dec. spindle firing → inc. y eff. drive → hypersensitive muscle spindle (new normal) + lock in contraction → tender pt.
treat via passively shorten muscle → spindle aff. fibers dec → y eff. fibers firing dec./reset
tender vs trigger vs chapman treatment?
tender → CS
trigger → firm pressure
chapman → direct inhibition, rotary motion
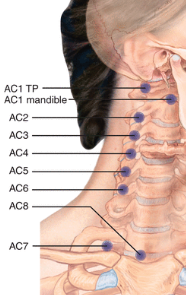
AC1* tender points treatment?
mandible or transverse process
RA
neck pain, headache (migraine, TMJ)
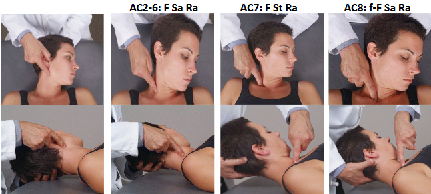
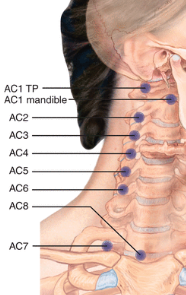
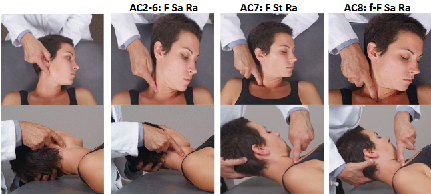
AC2-6 tender points treatment?
transverse process
F Sa Ra
neck pain, headache
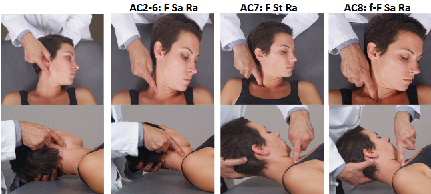
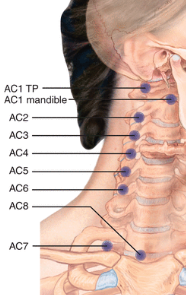
AC7* tender point treatment?
post. sup. clavicle
F St Ra
Flex a STRAw into 7-up
lower cervical or SCM restriction
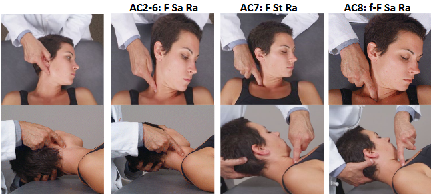
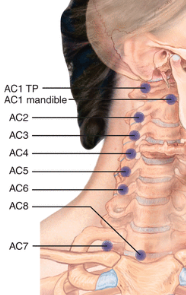
AC8 tender point treatment?
sup. med. clavicle @ sternal attachment to SCM
f-F Sa Ra
lower cervical or SCM restriction
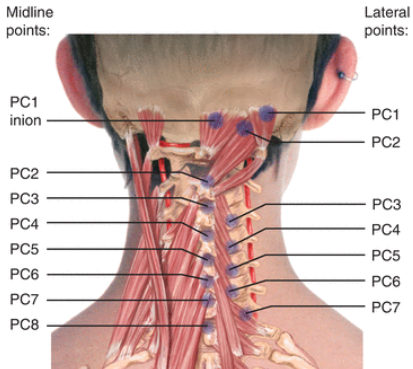
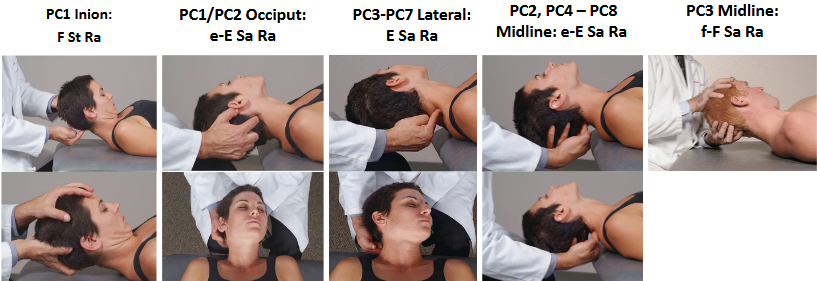
PC1 tender point treatment?
inion* → F St Ra
occiput → e-E Sa Ra
post. lat. headache, pain behind eye
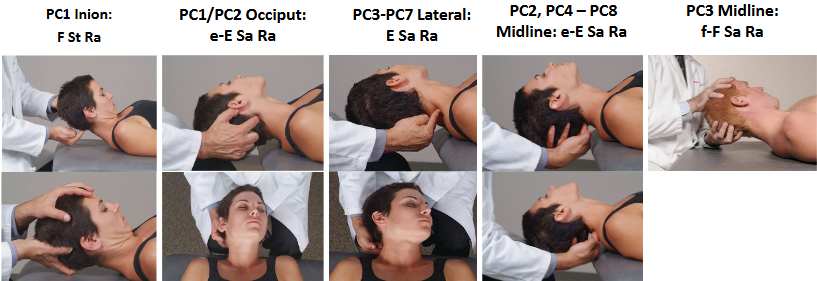
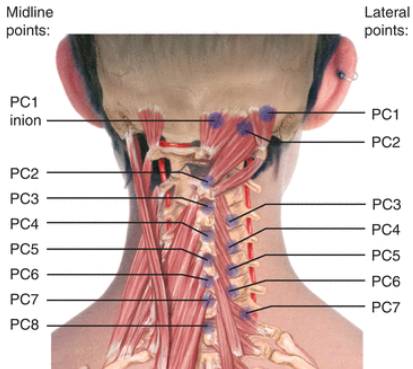
PC2 tender point treatment?
occiput → e-E Sa Ra
midline spinous process → e-E Sa Ra
periorbital/temporal headache
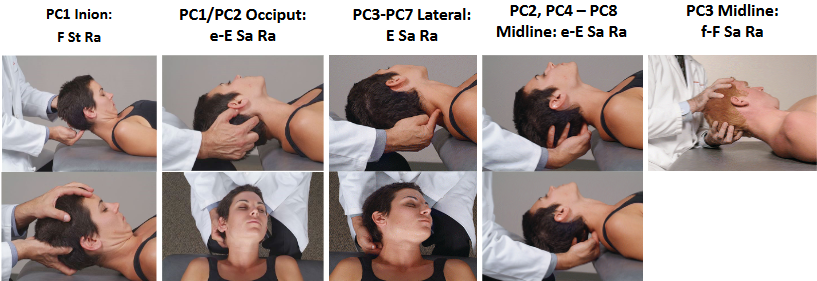
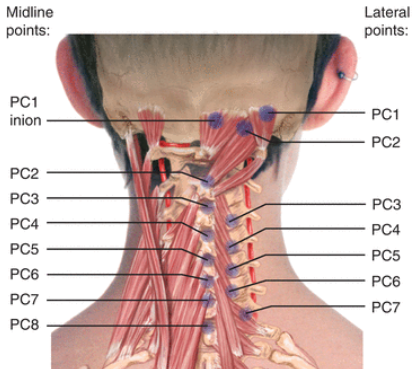
PC3-PC8 tender point treatment?
PC3* midline → f-F Sa Ra
PC4-PC8 midline (bottom of spinous process above) → e-E Sa Ra
neck pain + headache
trapezius MET?
flex neck to barrier
pt. extend head w/ equal force

oculucephalogyric reflex MET?
extension → pt. look up, relax, DO extend head to near barrier
flexion → pt. looks down
R. SB → look up + right
L. SB → look up + left

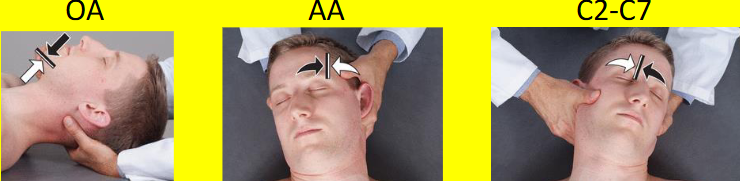
OA, AA, C2-C7 MET?
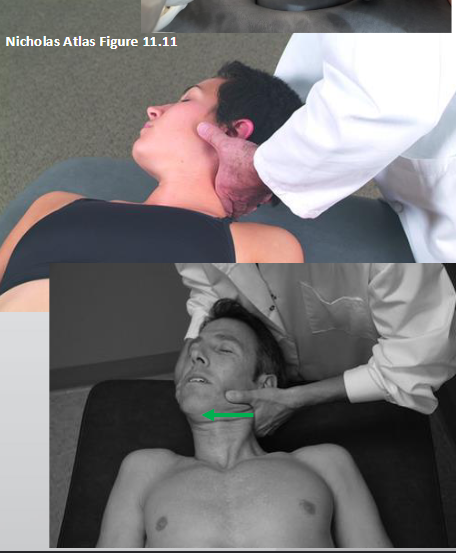
OA → contact suboccipital muscle + under chin, engage barriers
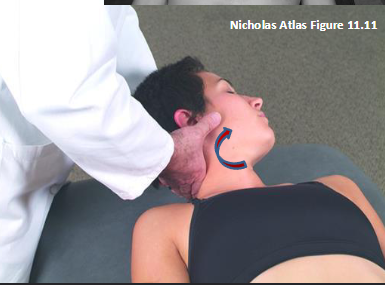
AA → gently flex, rotate into barrier
C2-C7 → 2nd MCP @ articular pillar of segment being treated, slight flexion → engage barriers
special tests cervical HVLA?
hoffman’s sign → UMN lesions (myopathy)
dorsiflex wrist, extend middle finger + stabilize PIP → flick DIP (+ = flex + adduct thumb/ flex index finger)
lhermitte sign → cervical myelopathy via cord compression
flex head + hip (+ = electric shock down spine)
spurling’s test → cervical radiculopathy
head extended, SB, rotated TOWARD affect side (+ = pain radiating down same arm)
SD end feels? treatment?
articular → via facet joint w/ muscle guarding (treat w/ HVLA)
muscular → hypertonicity
short restrictor → type 2, intrinsic segmental
long restrictor → type 1, int. + deep
fascial/ligamentous → shortening
edema-causing → less slack via fascial distension
contraindications HVLA?
relative: HNP, acute radiculopathy, acute spasm strain, osteopenia/porosis, spondylolisthesis, hypermobility, implants, inflammation Hx
absolute: down syndrome/RA (AA unstable → transverse lig. of dens rupture), chiari malformation, achondroplastic dwarfism (foramen magnum narrow), joint fusion (ankylosis/spondylosis), fracture, klippel-feil (fusion of 2+ segments), vertebrobasilar insufficiency, acute inflammatory, malignancy, spinal cord pathology
typical cervical vertebrae HVLA (rotational emphasis)?
contact articular pillar w/ right 2nd MCP, rest thumb on bony facial surface
stand on side of rotational ease
ant. translate pillar → flex until segment → rotate (to barrier) + SB (to ease)
take up slack as pt. exhales → rotational thrust to barrier
typical cervical vertebrae HVLA (sidebending emphasis)?
contact articular pillar w/ right 2nd MCP, rest thumb on bony facial surface
stand on side of rotational restriction
ant. translate pillar → flex until segment → SB (to barrier) + rotate (to ease)
take up slack as pt. exhales → translatory thrust to barrier
OA cervical HVLA?
contact articular pillar w/ right 2nd MCP, rest thumb on bony facial surface
stand on side of rotational ease
sup. traction + slight ant. pressure (extension)
rotate head to barrier → then SB into barrier → slight ant. pressure
rotational thrust

AA cervical HVLA?
contact articular pillar w/ right 2nd MCP, rest thumb on bony facial surface
stand on side of rotational ease
flex head 45 → slight ant. pressure
rotate into barrier → take up slack w/ breaths → end of exhale → rotational thrust

which nerve roots commonly cause cervical radiculopathy? tests for cervical radiculopathy vs myelopathy? red flags for cervical pain?
C6, C7
radiculopathy (spurling, shoulder abduction, neck distraction, valsalva) vs myelopathy (lhermitte, hoffman, babinski, hyperreflexia, clonus)
trauma, constitutional symptoms, UMN lesion, age <20 or >50, and concurrent chest pain/diaphoresis, SOB