Developmental Psychology (part 2)
1/88
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
89 Terms
Depressive disorders
Pervasive
Diverse
Debilitating
Depression: A Continuum
⬇ “Normal” state
⬇ Feeling sad/”depressed”/gloomy
⬇ Depression
⬇ Depressive Disorder (diagnosable)
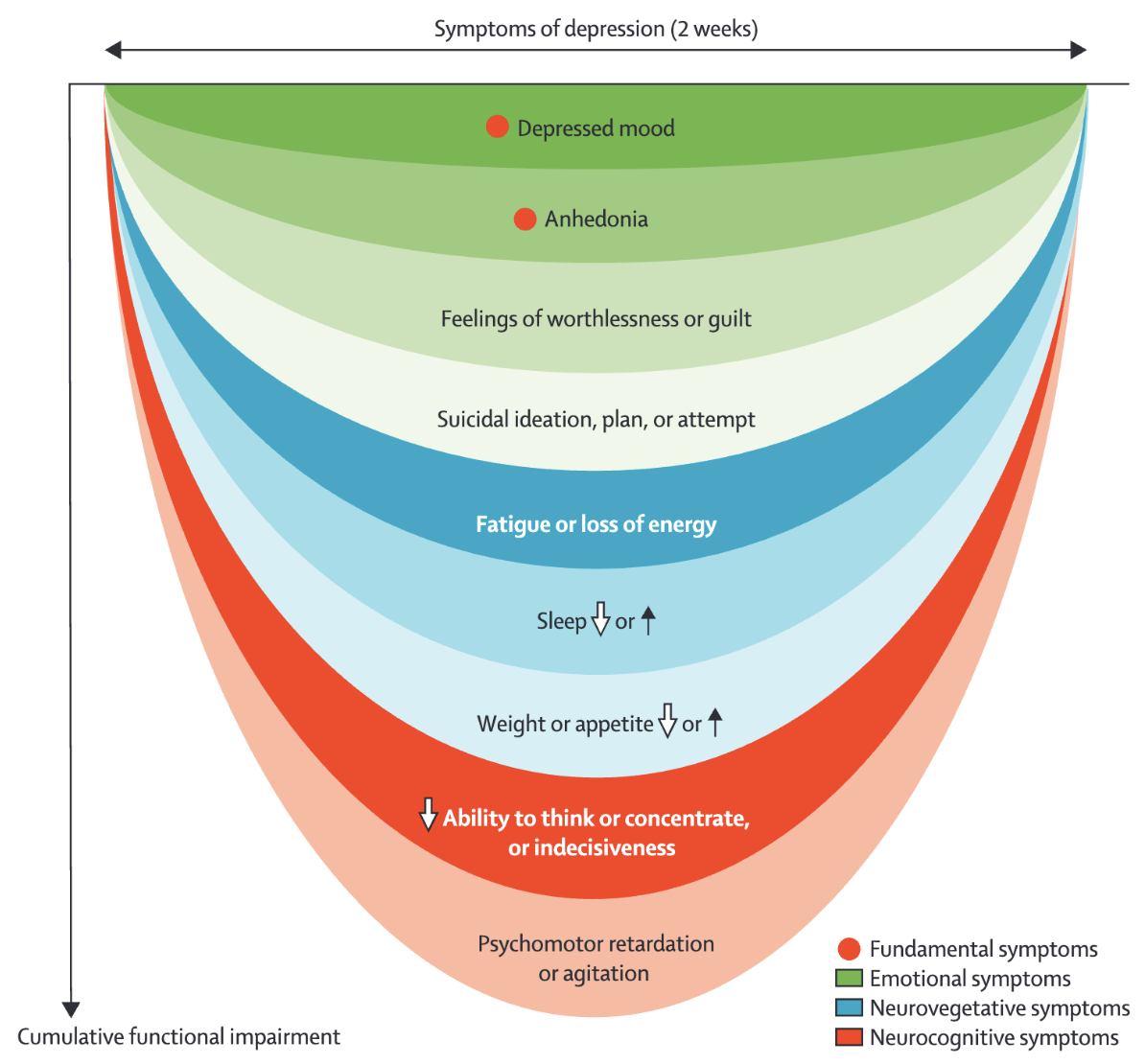
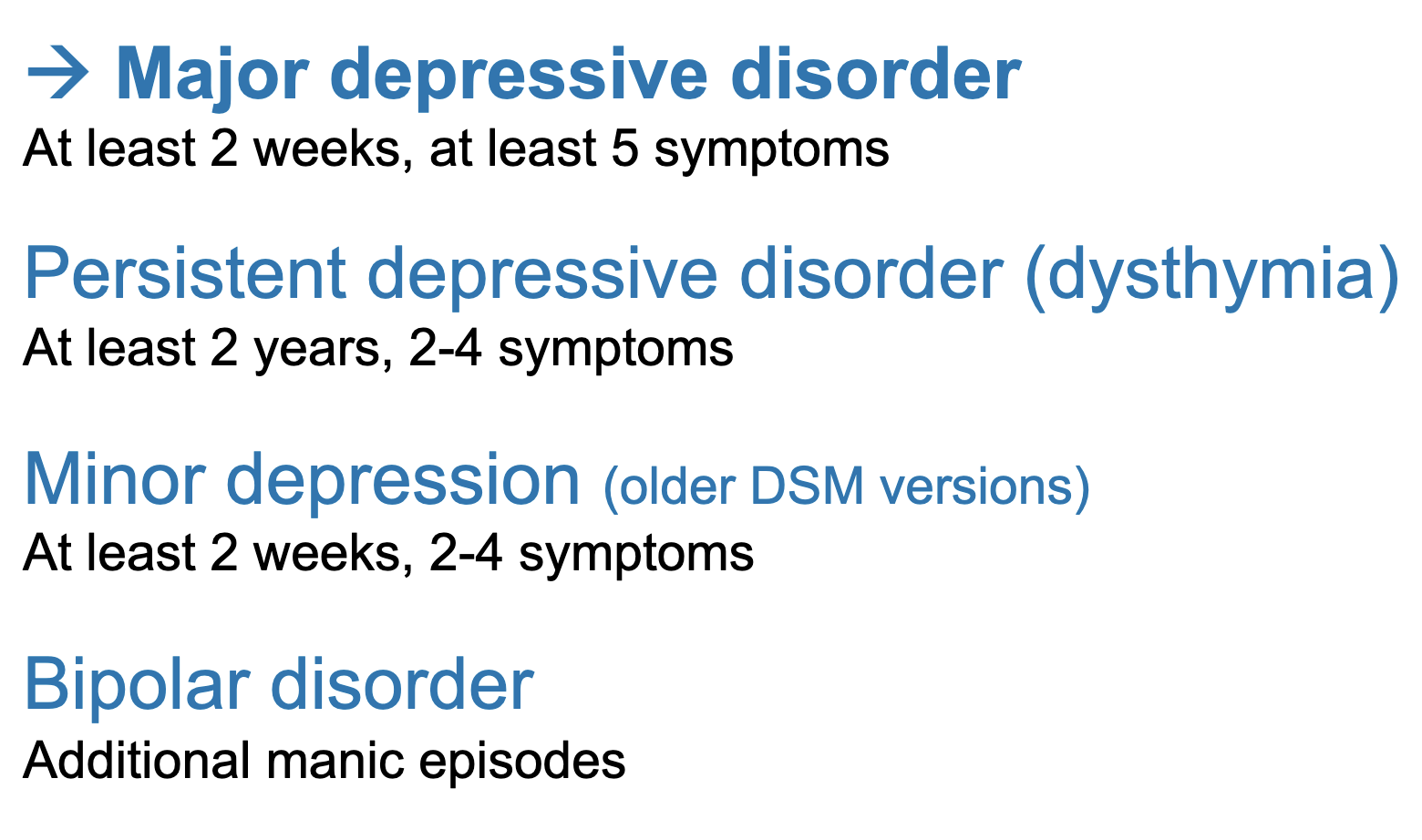
Depression: Diagnosis (DSM-5)
At least 2 core symptoms (2 weeks)
Anhedonia: No interest or pleasure in all or almost all activities
Depressed mood: most of the day, nearly every day
+ 4 other symptoms
Weight loss or gain, or decrease or increase in appetite
Sleep problems
Agitation or retardation, observable by others.
Fatigue or loss of energy
Feelings of worthlessness, guilt
Loss of focus, indecisiveness
Thoughts about death
+ Significant suffering / impairment in social or professional functioning
Symptoms of Depression
Cognition
Poor focus, indecisiveness, low self-esteem, hopelessness, suicidal thoughts, delusions
Neurovegitative
Disrupted sleep and appetite, psychomotor problems, catatonia, fatigue, amnesia
Emotion
Sadness, depressed mood, loss of interests, irritability
Clinical symptoms of MDD are usually accompanied by functional impairment
The greater the number and severity of symptoms (as opposed to particular symptoms), the greater the probability of the functional impairment.
Relevant Mood Disorders
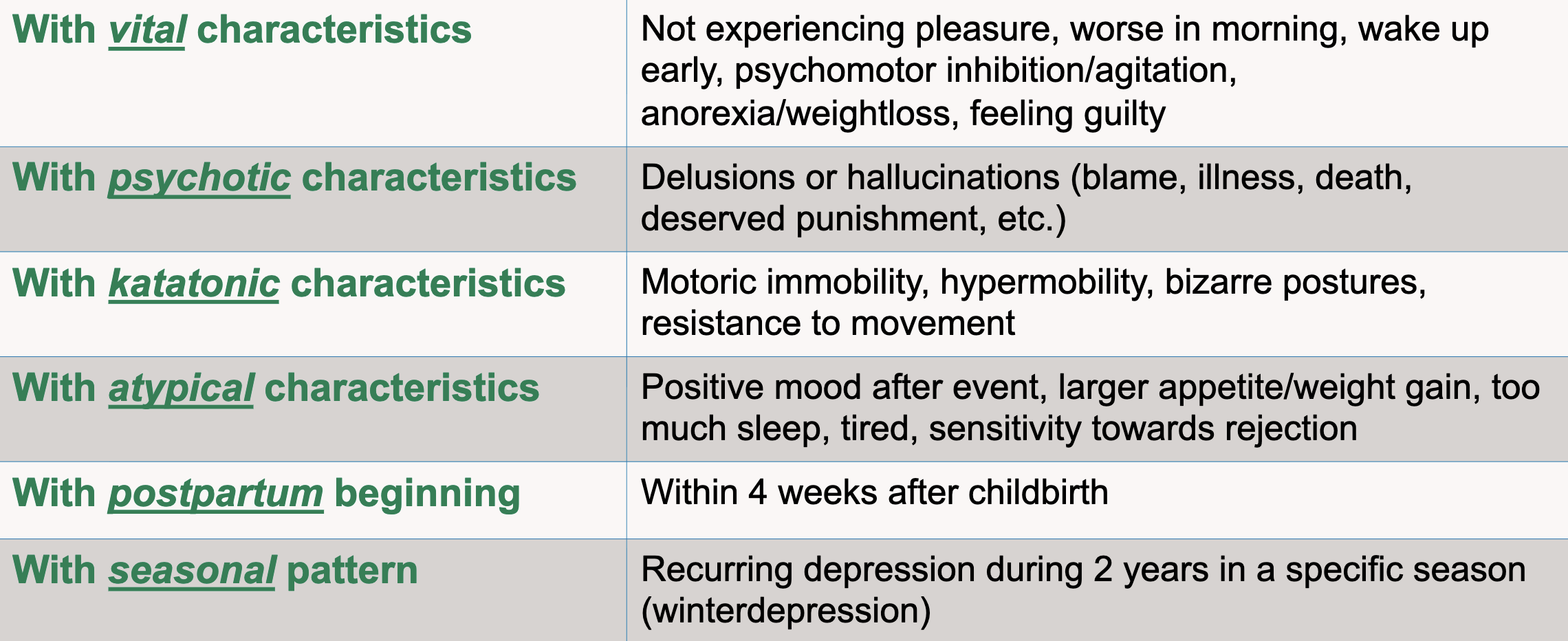
Depressive Disorder Subtypes
Depression, Suicidality, Suicide
Depression is the most important predictor of suicide
… but most people with depression are not suicidal!
Suicidality is associated with most mental disorders
Suicidality can best be seen as a separate problem that often co-occurs with depression
Suicidality is an important urgent indicator for treatment
Epidemiology: Prevalence Rates of MDD
In any given year, 4.4-5% of the world population has MDD
→ Increase of 41% from 1990 to 2023
Lifetime prevalence: approx. 10%
Epidemiology: Depressive Episodes
Average duration of episode is 6 months (but: wide variation)
Most acute episodes remit within a year, but 12-34% have chronic depression
High recurrence rates: 27-45% over 20 years in community samples, much higher in clinical samples
Recurrence risk increases with every additional episode
Epidemiology: Correlates & Comorbidity
Prevalence about twice as high in women as in men
High comorbidity: especially anxiety disorders, substance use disorders, personality disorders
Help-seeking is low (7-28%), even in countries with broadly available and free healthcare
Epidemiology: Children & Adolescents
Toddlers: 1 %
Primary school age: 1-2 %
Adolescents: ~5%
Young adults: 7.2%
Median age of onset: 26 (17-37) in high-income countries and 24 (17-35) in low- and middle income countries
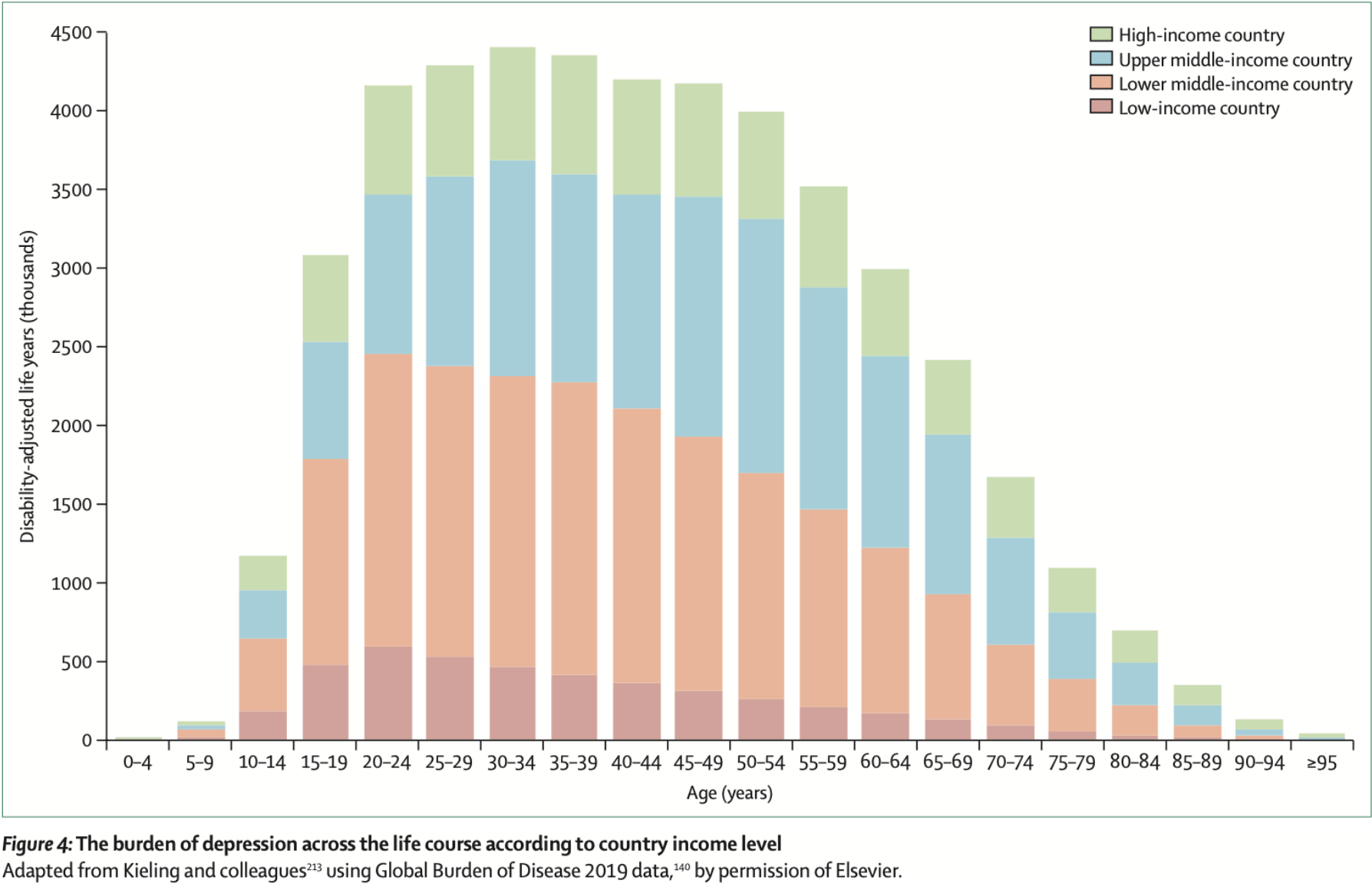
Disease Burden Compared to Other Mental Disorders
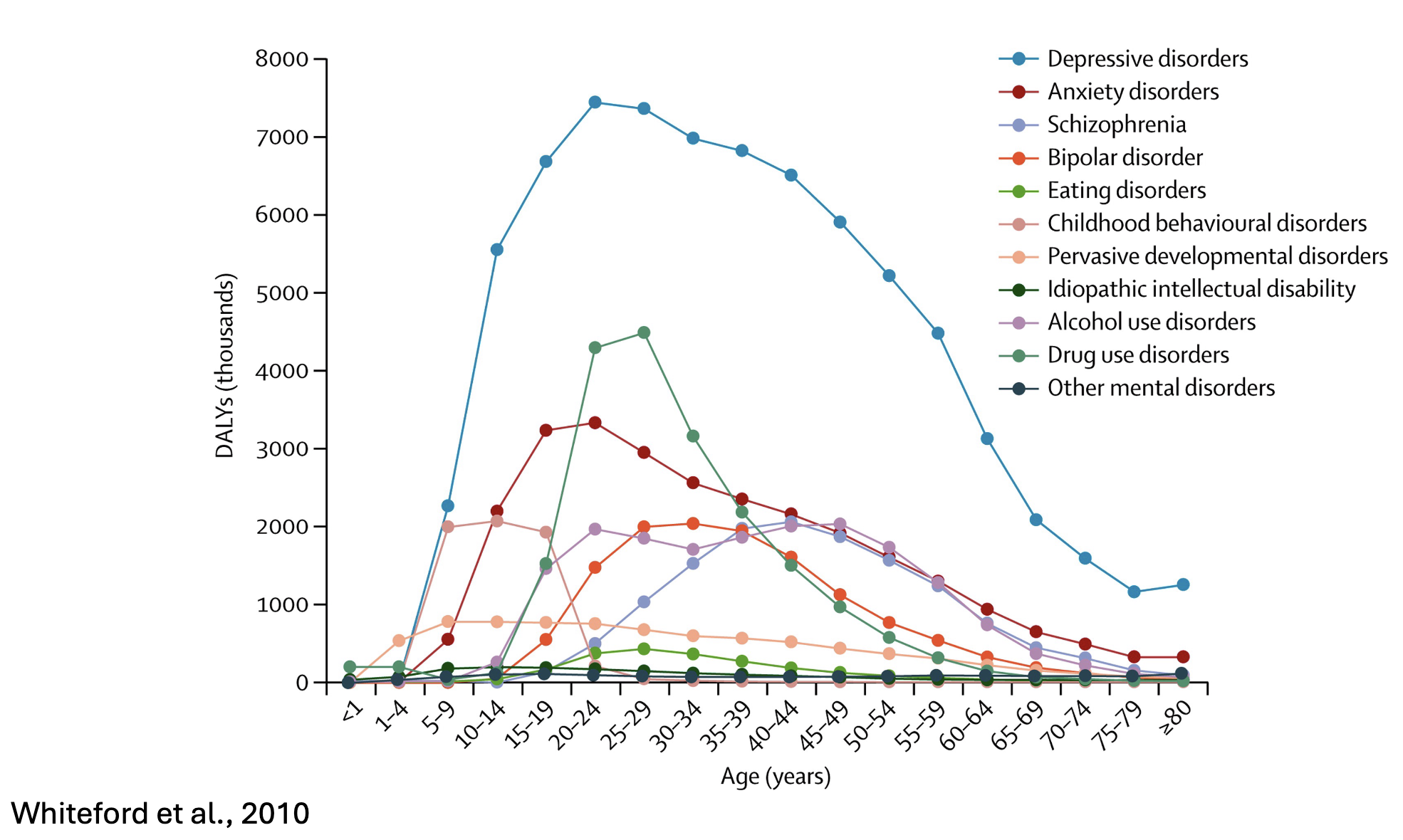
Depression: An Urgent Public Health Problem
High prevalence (30.3 million Europeans), 322 million worldwide and huge burden of disease
2.5 – 8.5 trillion USD in economic losses
Existing treatments can reduce burden of disease by no more than 35% (currently 15%)
Risk factors for MDD
Genetic risk
30-40% heritability, along with other internalising disorders
no specific/singular gene loci identified
Prenatal factors (brain damage, infections, complications)
Alcohol/substance abuse
Obesity
Childhood trauma
Cognitive style
Stressful live events, chronic stress, “daily hassles”
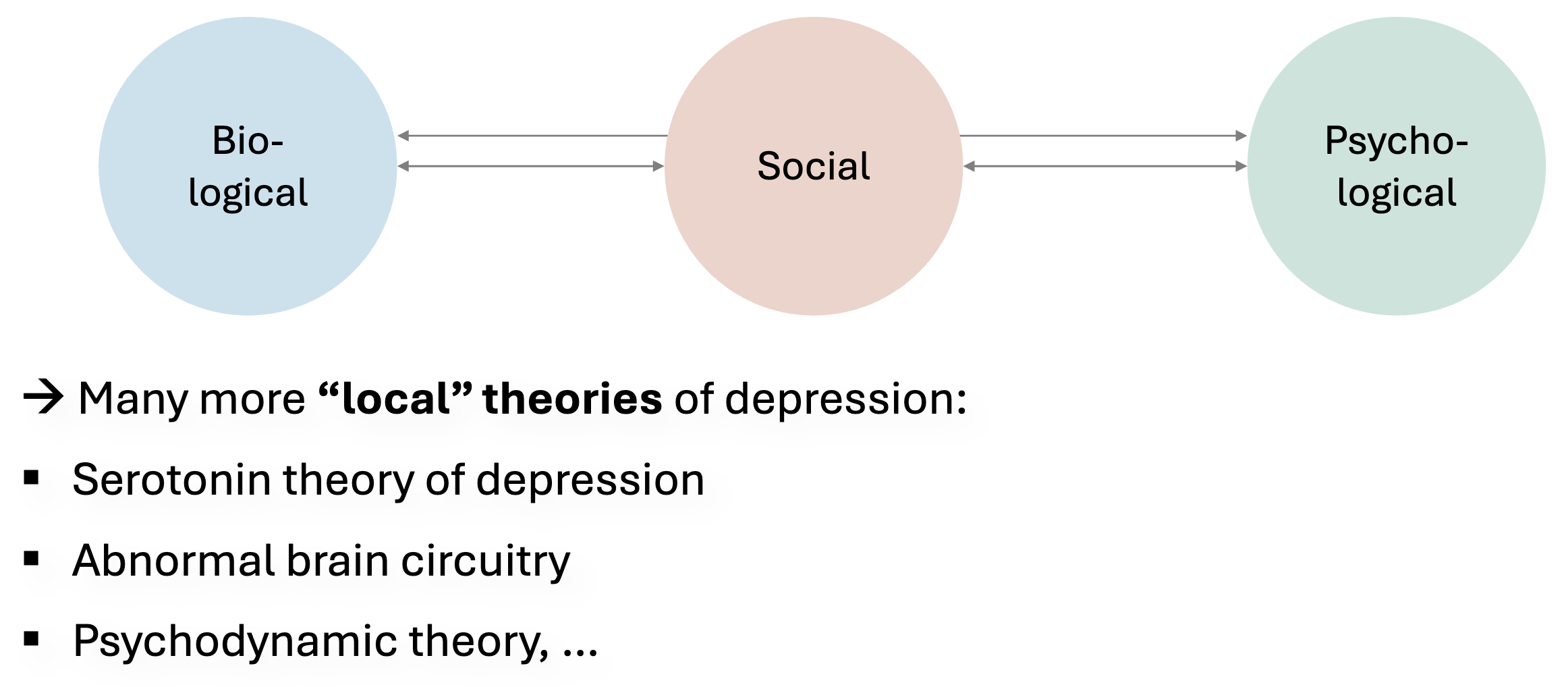
Biopsychosocial Model of Depression
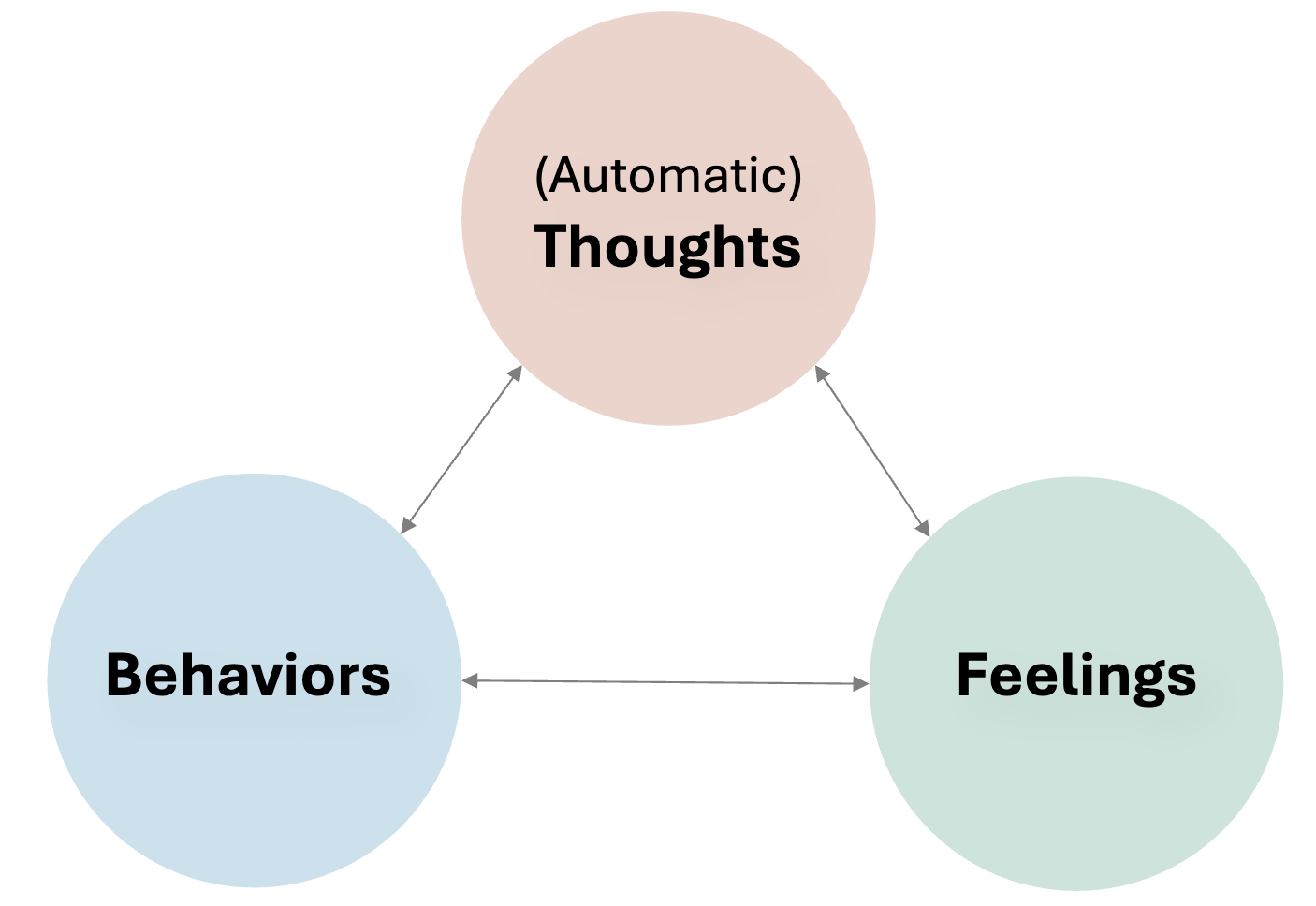
Beck’s Cognitive Model of Depression
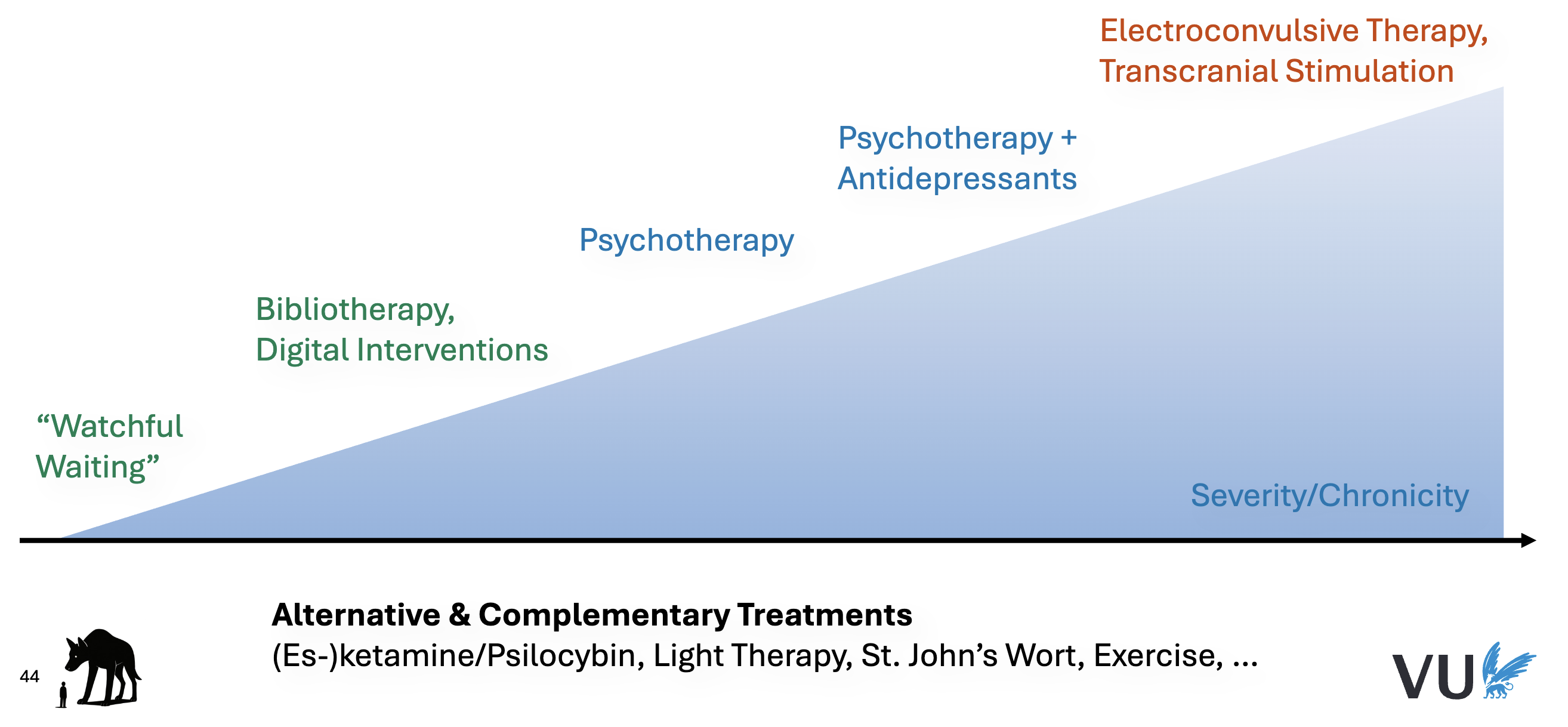
Treatment Options MDD
Antidepressants: Effects & Controversies
Types of antidepressants:
SSRIs (selective serotonin reuptake inhibitors; first-line in most cases)
SNRIs (serotonin-norepinephrine reuptake inhibitors)
Tricyclic Antidepressants (older; affect other receptors as well, more side effects)
MAOIs (monoamine oxidase inhibitors; inhibits enzymes metabolizing serotonin, some irreversible)
Effects & Controversies
Antidepressants are effective for depression, but effects are small-to-moderate
None is substantially more effective than the other
Long-standing debate in the 90’s and early 2000’s about the efficacy of antidepressants
For patients with milder symptoms, benefits may be very small
Consider side effects: irritability, sleep problems, weight gain, sexual side effects
Some patients have trouble stopping antidepressants (rebound effects)
Psychological Treatment for MDD
Various “families” of therapies, e.g.:
Cognitive behavior therapy (CBT)
Interpersonal therapy (IPT)
Psychodynamic therapy
Effects are moderate-to-large
No clear evidence that one is substantially more effective than the others
But some therapies (especially CBT) much better studied than others
Psychological Treatment & Pharmacotherapy
Patients prefer psychotherapy by wide margins (75%)
Effects of monotherapy are comparable short-term
Combined treatment is more effective than either psychotherapy and pharmacotherapy alone
First-line treatment from moderate symptoms upwards!
At the longer term, psychotherapy is probably more effective
Anxiety
Adaptive → Problematic → Pathological
Intensity, duration and pervasiveness
4 Ds: Dysfunction, Distress, Deviance, Danger
Adaptive / nonclinical: most children have one or two fears appropriate to their age
Problematic: interference with daily life and development
Risk Factors for development of anxiety disorders
Child factors:
Genetic predisposition
Temperament
Cognition
Environmental factors:
Insecure attachment
Education and parental style
Negative life events
Anxiety disorders – shared characteristics
Excessive fear and anxiety
Related behavioural disturbances
Fear: emotional response to real/perceived imminent threat
Anxiety: anticipation of future threat
Not attributable to physiological effects of:
Medication/substance
Medical condition
Anxiety disorders facts and figures
The most prevalent mental disorder worldwide*
About 5.7% of global population
40% of people with a mental disorder have an AD
47% increase from 2019-2023
Often early onset
Women are 1.66x more likely to develop an AD
Wax and wain over time
High comorbidity
High individual impairment
DSM-5: Anxiety Disorders
Separation Anxiety Disorder (e.g., parents leaving)
Selective Mutism
Specific Phobia
Generalized Anxiety Disorders (GAD)
Social Anxiety Disorder (SAD)
Panic Disorder
Agoraphobia
No longer considered anxiety disorders:
OCD
Acute stress disorder
PTSD
Anxiety: Average age of onset
Pre-school:
Selective mutism
Elementary school:
Separation anxiety
Specific phobia
Adolescence:
SAD (early)
OCD (early or late)
(Early) Adulthood:
Panic Disorder
Agoraphobia
GAD
Separation Anxiety Disorder
Non age-appropriate and excessive anxiety (or anticipation) of going away from home or leaving attachment figures
Excessive worry that caregivers may be harmed
Persistent refusal to go anywhere which may cause separation
Frequent nightmares about separation
Recurrent physical complaints when not in close proximity to attachment figures
Selective Mutism
A child shows consistent failure to speak in specific social situations in which there is an expectation for speaking (e.g., at school), despite speaking in other situations.
Interferes with educational achievement and social interaction
Duration: at least 1 month (not limited to the first month of school)
Not attributable to a lack of knowledge of, or comfort with, speaking
The disturbance is not better explained by other disorders
Often co-exist with social anxiety disorder
Early onset, later diagnosis
Specific phobia: DSM-5
A marked, intense fear / anxiety of a specific object or situation that substantially interferes with the person’s ability to function
Phobic object almost always evokes immediate and persistent fear / anxiety
Phobic object is actively avoided or endured with intense fear/anxiety
Fear / anxiety is out of proportion (irrational)
Persistent: >6months
Not better explained by another disorder
5 main categories
Animals, Natural environments, Blood-Injection-injury, Situational, Other
75% > 1 phobia present
Often difficult to recall specific reason for onset
Following a traumatic event
Informational transmission
Observational learning
Generalized Anxiety Disorder: DSM-5
Excessive anxiety and worry, occurring more days than not for at least 6 months about a number of events or activities
Difficulty controlling the worry
Associated with 3 or more other symptoms:
Clinically significant distress or impairment
Not attributable to medication, substance or other medical or mental disorder
Physically impairing
Social Anxiety Disorder: DSM-5
Marked fear/anxiety about one or more social situations in which the individual is exposed to possible scrutiny by others:
Social interactions
Being observed
Performing in front of others
Individual fears he/she will act in a way or show anxiety symptoms that will be negatively evaluated
humiliating or embarrassing
leading to rejection or offending others
Social situations (and behaviours) are avoided or endured with intense fear/anxiety
Social situations almost always provoke fear or anxiety
Fear/anxiety is out of proportion
Persistent: > 6 months
Clinically significant distress or impairment
Not attributable to substance, medication, or other disorder/condition
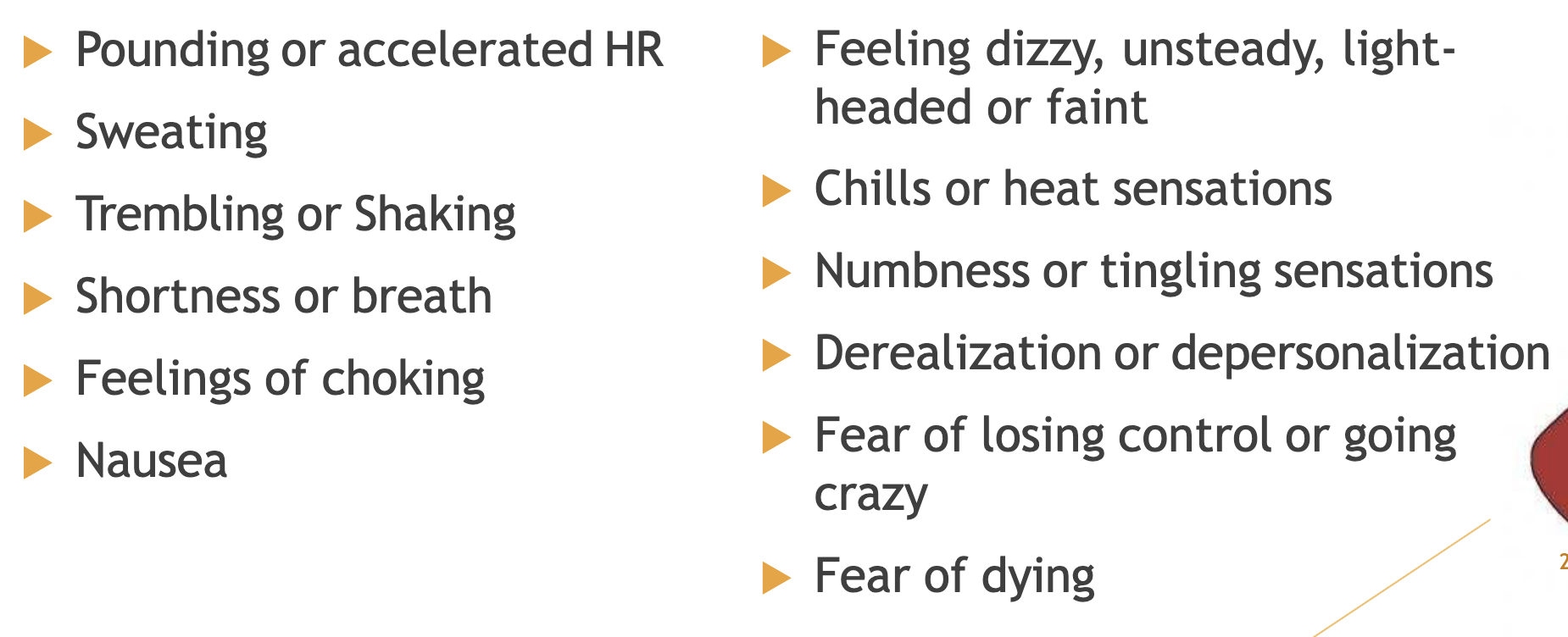
Panic attacks may occur
Panic Disorder: DSM-5
Recurrent unexpected panic attacks
Attacks are followed by one month period or more of (either/or):
Persistent worry about having additional attacks or their consequences
Significant change in behaviour because of the attacks
Not attributable to substance, medicine or other disorder
A panic attack ≠ panic disorder
Great variety in severity and frequency of attacks
Possible episodic outbreaks with years of remission in between
Agoraphobia: DSM-5
Marked fear or anxiety for more than 6 months about two or more of the following 5 situations:
Using public transportation
Being in open spaces
Being in enclosed spaces
Standing in line or being in a crowd
Being outside of the home alone
Situations are avoided or endured with intense fear
Interferes with routine or functioning
Obsessive Compulsive Disorder (OCD): DSM-5
Obsessions or compulsions (most often both)
Time-consuming (min. 1 hour per day)
Cause clinically significant distress or impairment in social, occupational, or other important areas of functioning.
Varying degree of insight
Avoidance
Obsessions: persistent and recurrent intrusive thoughts, ideas, images or impulses
Content; Disturbing, offensive or irrational themes
Related to uncertainty about frightening prospects
Causes severe distress and anxiety
Compulsions: repetitive behaviours, urges, rituals or mental acts
Regarded as excessive or exaggerated (especially in calmer moments)
Examples: Checking, Washing, Counting, Repeating routine activities, Reassurance seeking
Mental rituals: Excessive prayer, Repeating special phrases or numbers, Mental reassurance
Traumatic events
Exposure to one or more event(s) that involved death or threatened death, actual or threatened serious injury, or threatened sexual violation
According to DSM-5:
Direct exposure
Witnessing the trauma
Learning that a relative or close friend was exposed to a trauma
Indirect exposure to aversive details of the trauma, usually in the course of professional duties (e.g., first responders, medics)
Lifetime prevalence of common mental disorders in conflict settings:
Posttraumatic stress disorder (PTSD): 30.6%
Depression: 30.8%
Posttraumatic stress disorder
History:
“Soldiers Heart”, “Shell Shock”
Vietnam, KZ-syndrome
1980 diagnosis PTSD in DSMIII
Criterion B (one required): The traumatic event is persistently re-experienced, in the following way(s):
Unwanted upsetting memories, Nightmares, Flashbacks, Emotional distress after exposure to traumatic reminders, Physical reactivity after exposure to traumatic reminders
Criterion C (one required): Avoidance of trauma-related stimuli after the trauma, in the following way(s):
Trauma-related thoughts or feelings, Trauma-related reminders
Criterion D (two required): Negative thoughts or feelings that began or worsened after the trauma, in the following way(s):
Inability to recall key features of the trauma, Overly negative thoughts and assumptions about oneself or the world, Exaggerated blame of self or others for causing the trauma, Negative affect, Decreased interest in activities, Feeling isolated, Difficulty experiencing positive affect
Criterion E (two required): Trauma-related arousal and reactivity that began or worsened after the trauma, in the following way(s):
Irritability or aggression, Risky or destructive behavior, Hypervigilance, Heightened startle reaction, Difficulty concentrating, Difficulty sleeping
Risk factors for PTSD
Pretrauma
genetic vulnerability
being female
low age
intelligence
low SES
prior trauma
prior psychiatric symptoms
Peritrauma
perceived threat
negative interpretation of event
physiological arousal
anger and shame
dissociation during event
Posttrauma
social support
coping
negative interpretation of consequences of the event
new life events
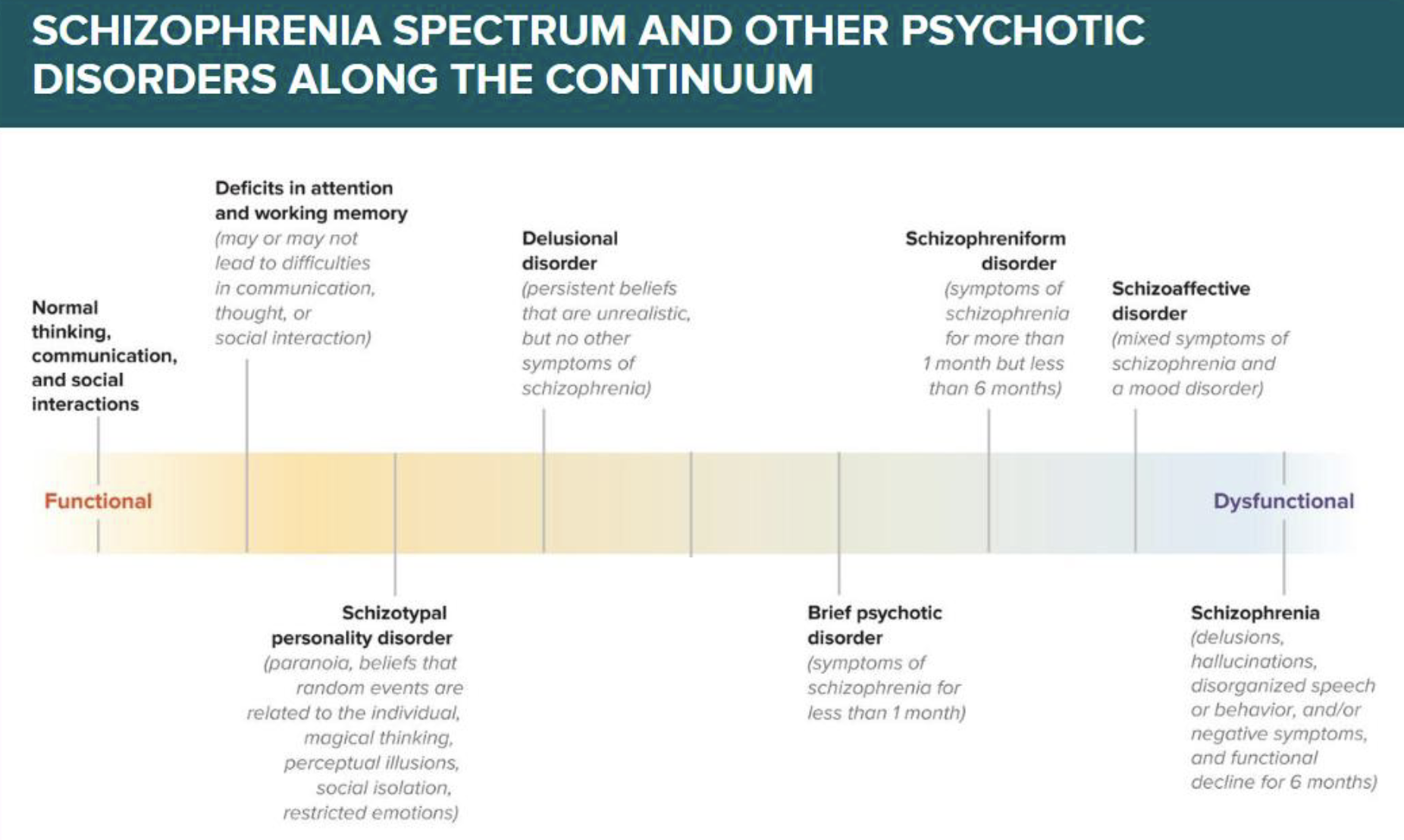
Spectrum of psychotic disorders
Psychosis symptoms
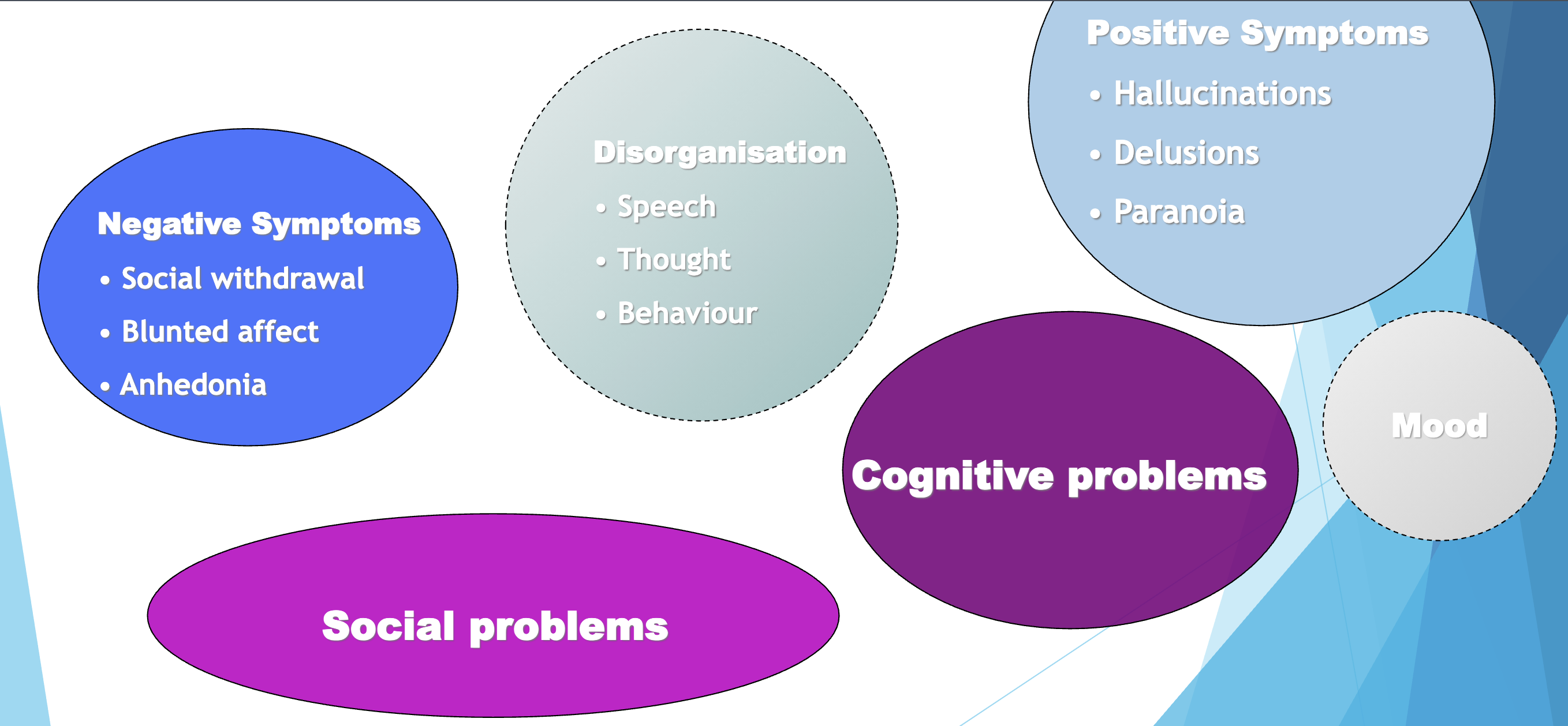
Positive symptoms
Present in a disorder and are not normally experienced by most individuals. Reflect an excess or distortion of normal functions.
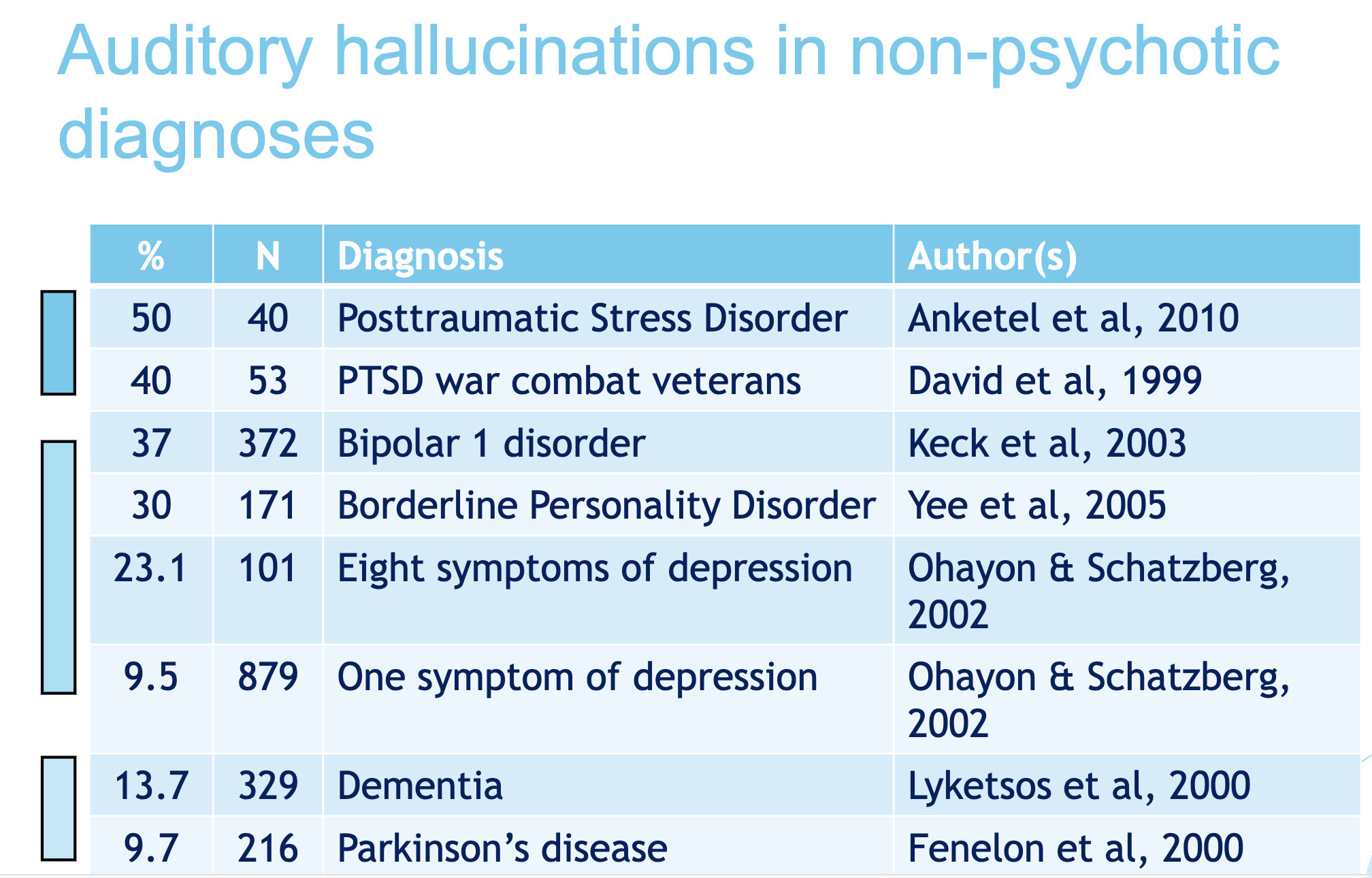
Hallucinations
Delusions
Hallucinations
Experience involving the apparent perception of something not present
Auditory
Visual
Tactile
Olfactory
Delusions
A delusion is a fixed belief in something that’s untrue (despite evidence of the contrary).
Persecutory – Paranoia
Grandiose
Reference
Erotomanic
Disorganisation
Speech: incoherent, Q&A don’t match
Thought: loose, weird associations
Behaviour: unpredictable, clumsy behaviour, catatonia (rigid)
Experiential negative symptoms
Avolition – reduced motivation to engage in meaningful activities
Anhedonia – reduced pleasure experience
Asociality – preference to be alone, not initiating social contact
Expressive negative symptoms
Alogia – poor speech due to thought problems
Blunted affect – reduced ability to express emotions (facial expression, intonation voice, movement)
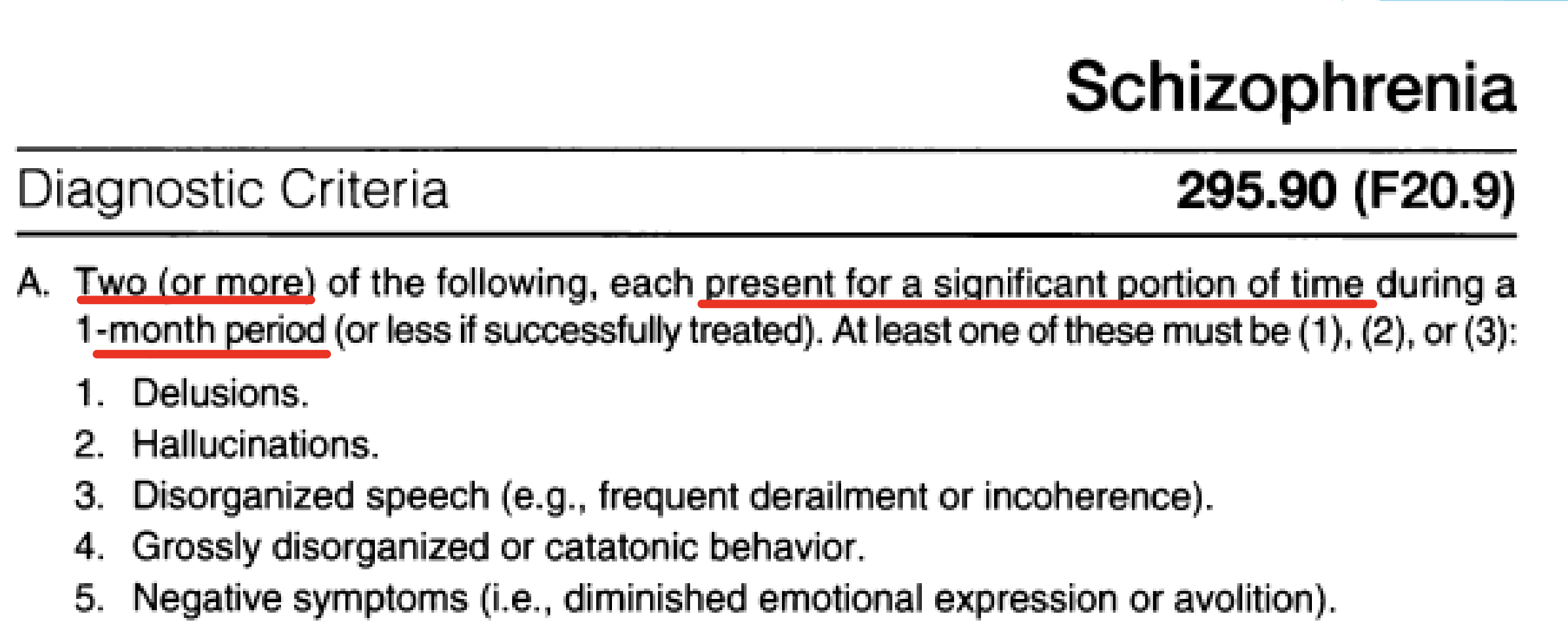
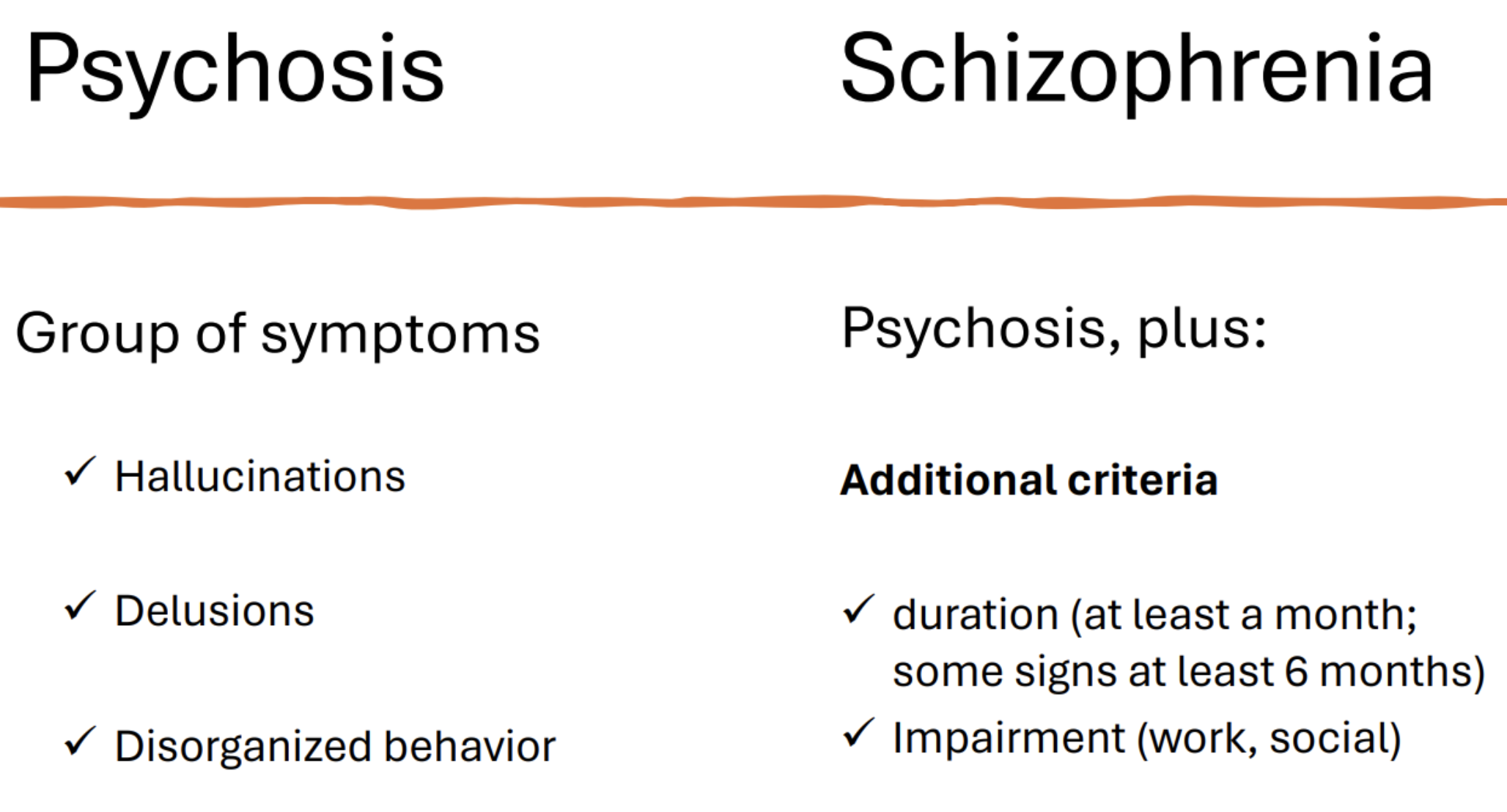
DSM 5 Criteria diagnosis schizophrenia
B: Social / professional disfunctioning
C: Duration: at least 6 months disturbed functioning, with 1 month symptoms
Excluding…
D. Schizoaffective or mood disorder
E. Use of medication, drugs or somatic disorder
F. Pervasive developmental disorder (ASD)
Psychosis vs. Schizophrenia
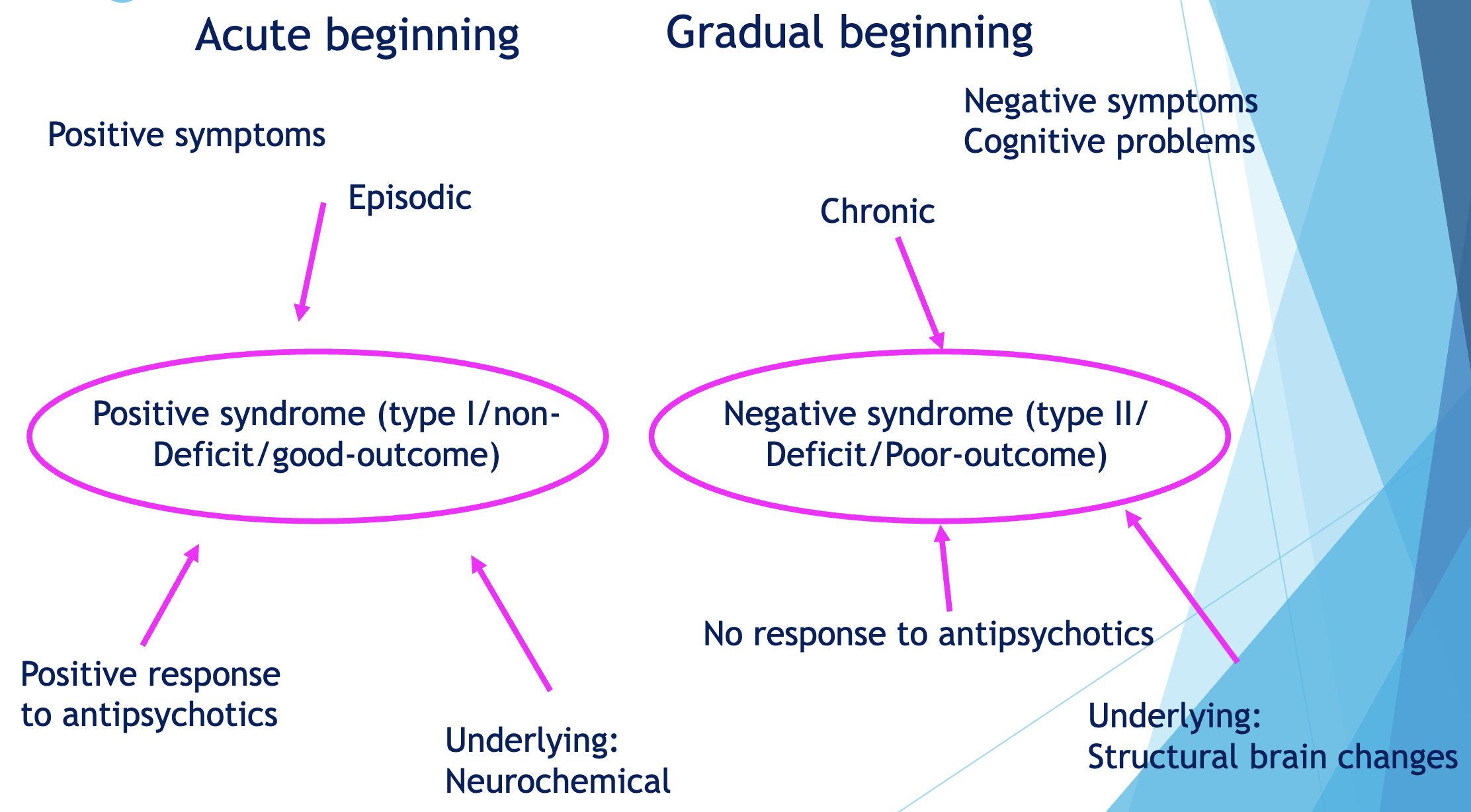
Schizophrenia as a heterogeneous disorder
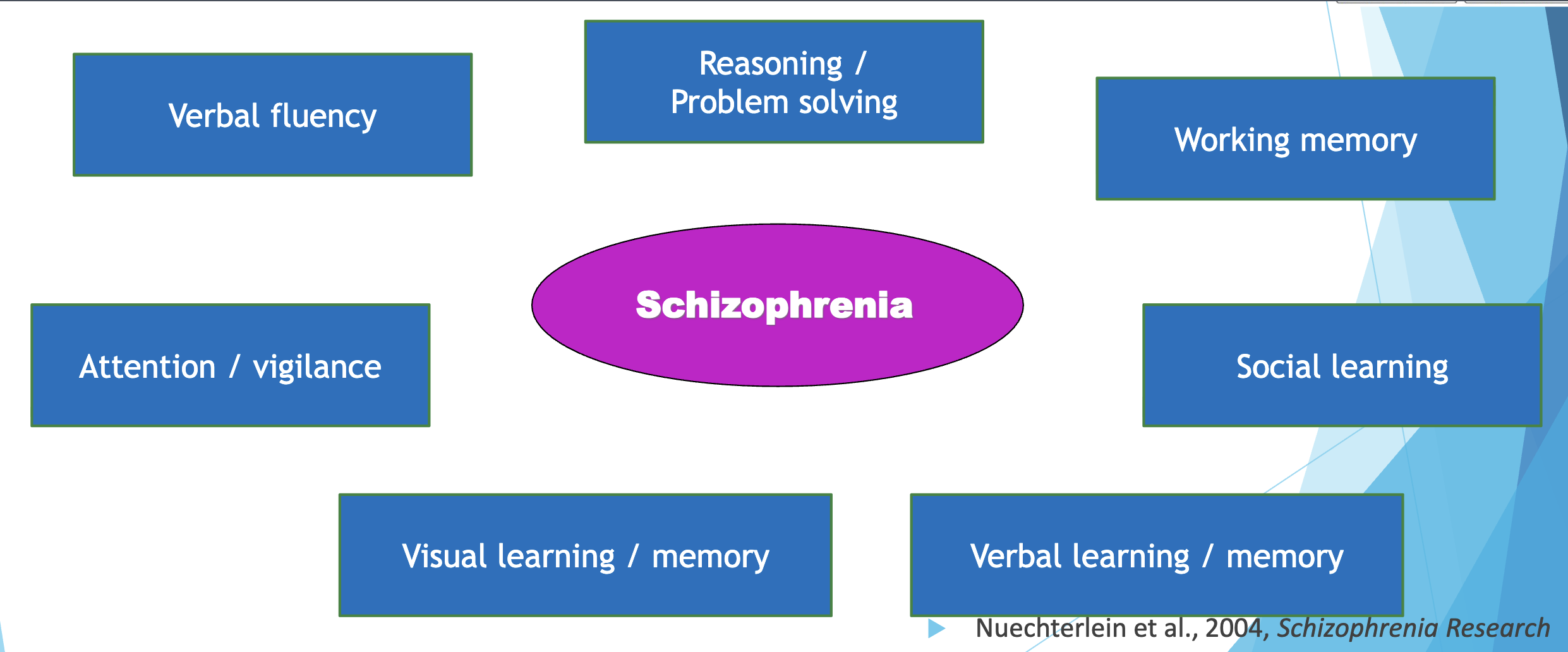
Other symptoms of schizophrenia: cognitive problems
Neurocognitive problems
Social cognitive problems
Social cognition deficits
Emotion recognition
more sensitive to negative emotions
neutral is negatively interpreted
Theory of Mind
problems interpreting situations
Social perception
Attribution style
externalising positive events
internalising negative events
Data gathering bias
jumping to conclusions: overconfidence
in the decision
Prevalence & Definition of Schizophrenia
“Schizophrenia is a severe, chronic mental disorder characterized by disturbances in thought, perception and behavior.” - DSM-5.
Prevalence: 0.3 – 1 % of the population
1.5–3.5% will experience during lifetime
0.2% new cases per year (incidence)
Typical age of onset: 16 – 30 adolescence/ early adulthood!
Important development is disrupted
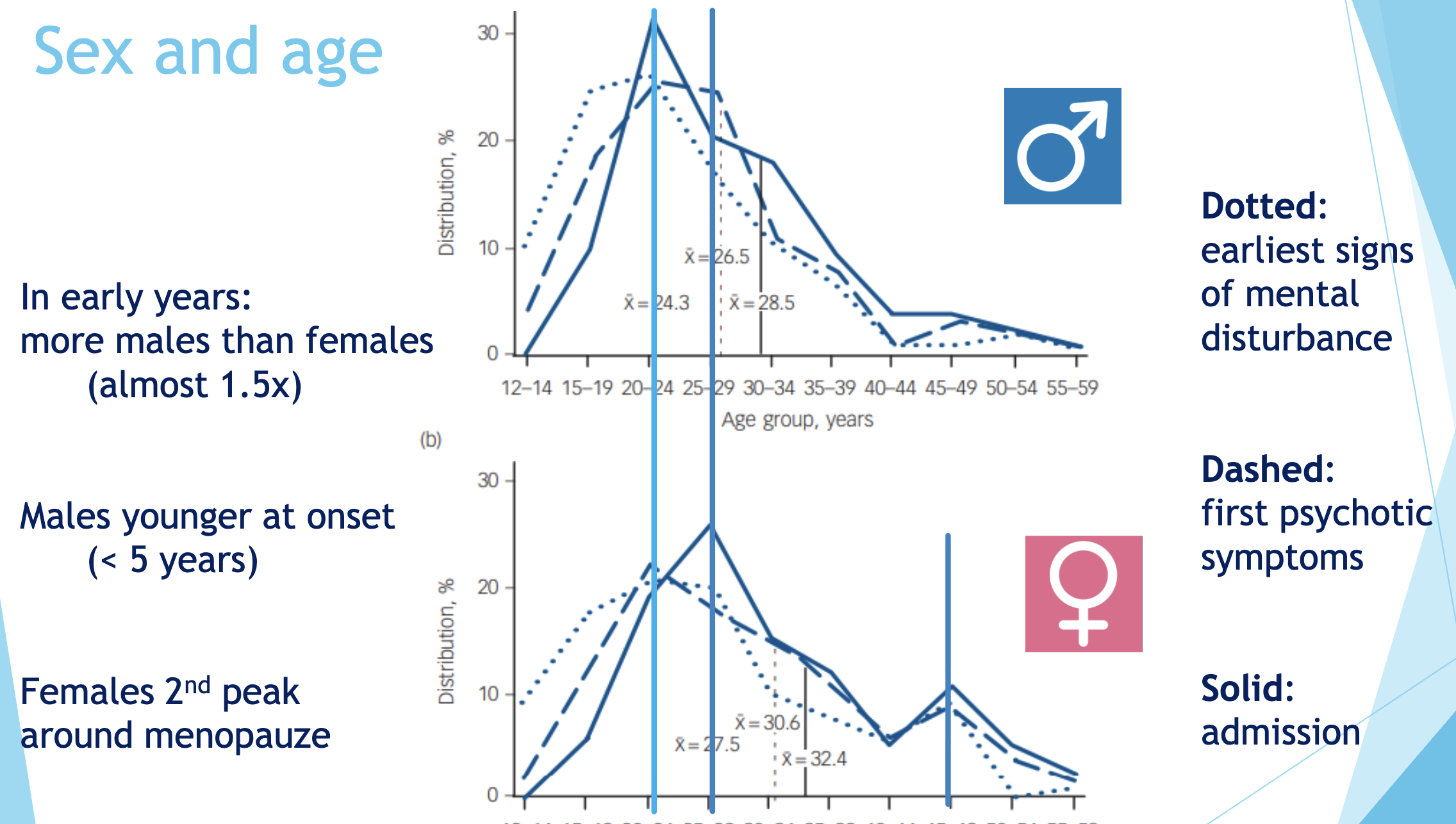
More common in males than females, but depending on age group
Schizophrenia and age & sex
Adolescence is the phase of risk
Comorbidity of schizophrenia
Important! Many schizophrenia symptoms overlap with other disorders (e.g., depression, bipolar disorder) and comorbidity is high.
Substance abuse (47%)
Anxiety & Depression (50%)
Panic disorder (15%)
PTSD (29%)
OCD (23%)
Costs of schizophrenia
Unemployment: more than in non-schizophrenia persons (70% vs. 28%)
Productivity loss: about 1/3 less productivity/income
Health care services: 10-20 years shorter life
Adolescent development interrupted → deficits
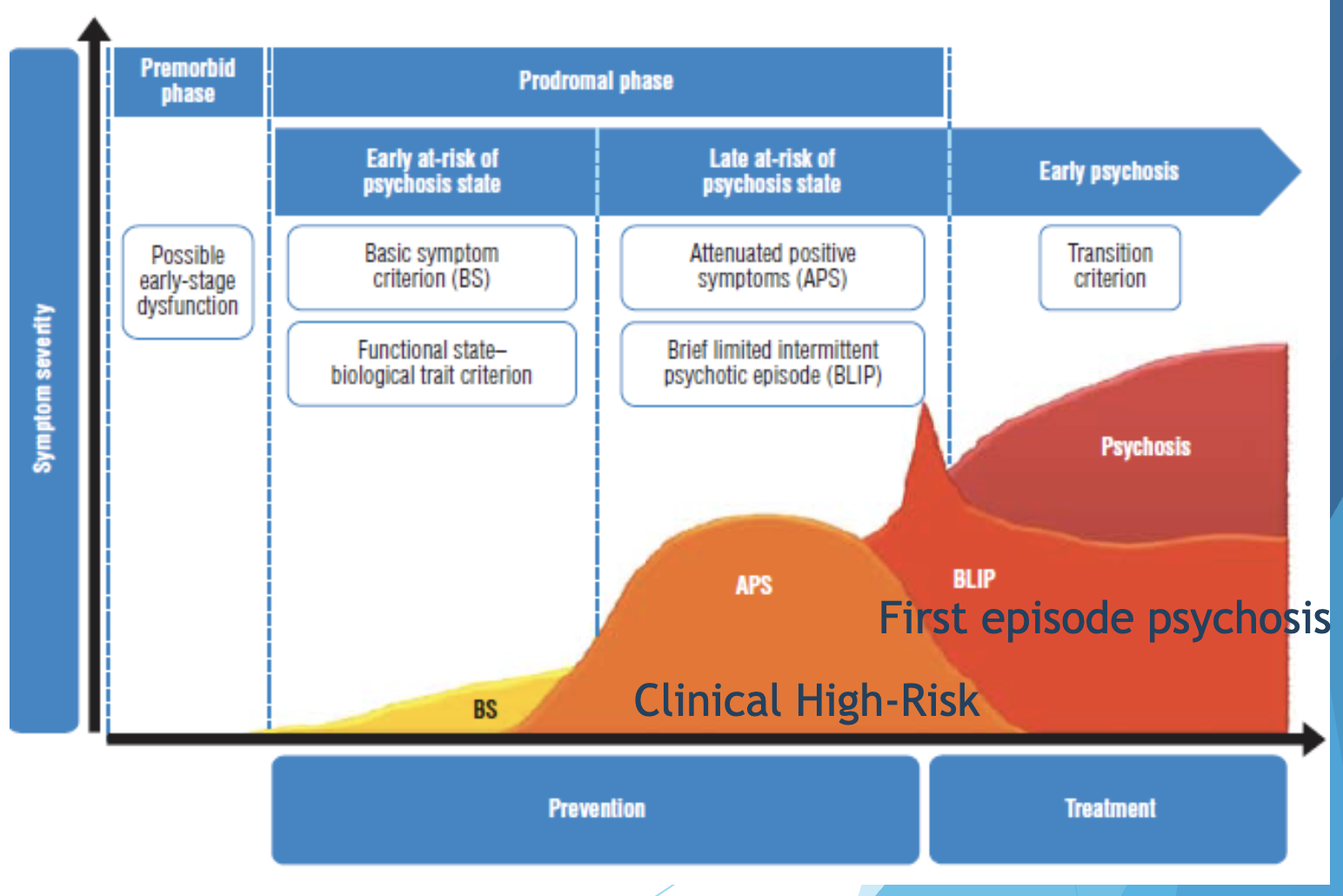
Developmental course of schizophrenia
Phases:
Premorbid phase – impairments in language, cognition, social functioning.
Prodromal phase – attenuated or milder symptoms of psychosis (high risk state).
Transition to (first episode of) psychosis - approx. 1/3 of at-risk individuals transition after 3 years
Psychosis outcome
10 years after diagnosis of schizophrenia (NL) …
25% are completely recovered
25% are strongly improved, relatively independent
25% are improved, but needs extensive network of help
15% are hospitalised, not improved
10% are deceased (mainly suicide)
Neurodevelopmental disorder
Pre- and perinatal risk factors: linked to aberrant synaptic pruning during adolescence
Developmental problems: Minor physical abnormalities and/or neurological soft signs
(Motor, social, cognitive)
Structural brain abnormalities
(Ventricular enlargement, grey matter reductions, white matter disruption)
Heritability of schizophrenia
Genes are necessary, but not sufficient for the development of schizophrenia.
Heritability 80-90%
Environmental factors in schizophrenia
Childhood:
Rearing (attachment/ communication styles): paranoia
Brain injury
Abuse (trauma) - hallucinations
Adolescence – adulthood:
Substance abuse - cannabis (initiate or aggravate)
Migration / ethnicity - paranoia
Urbanicity
Social adversity
Life events, trauma
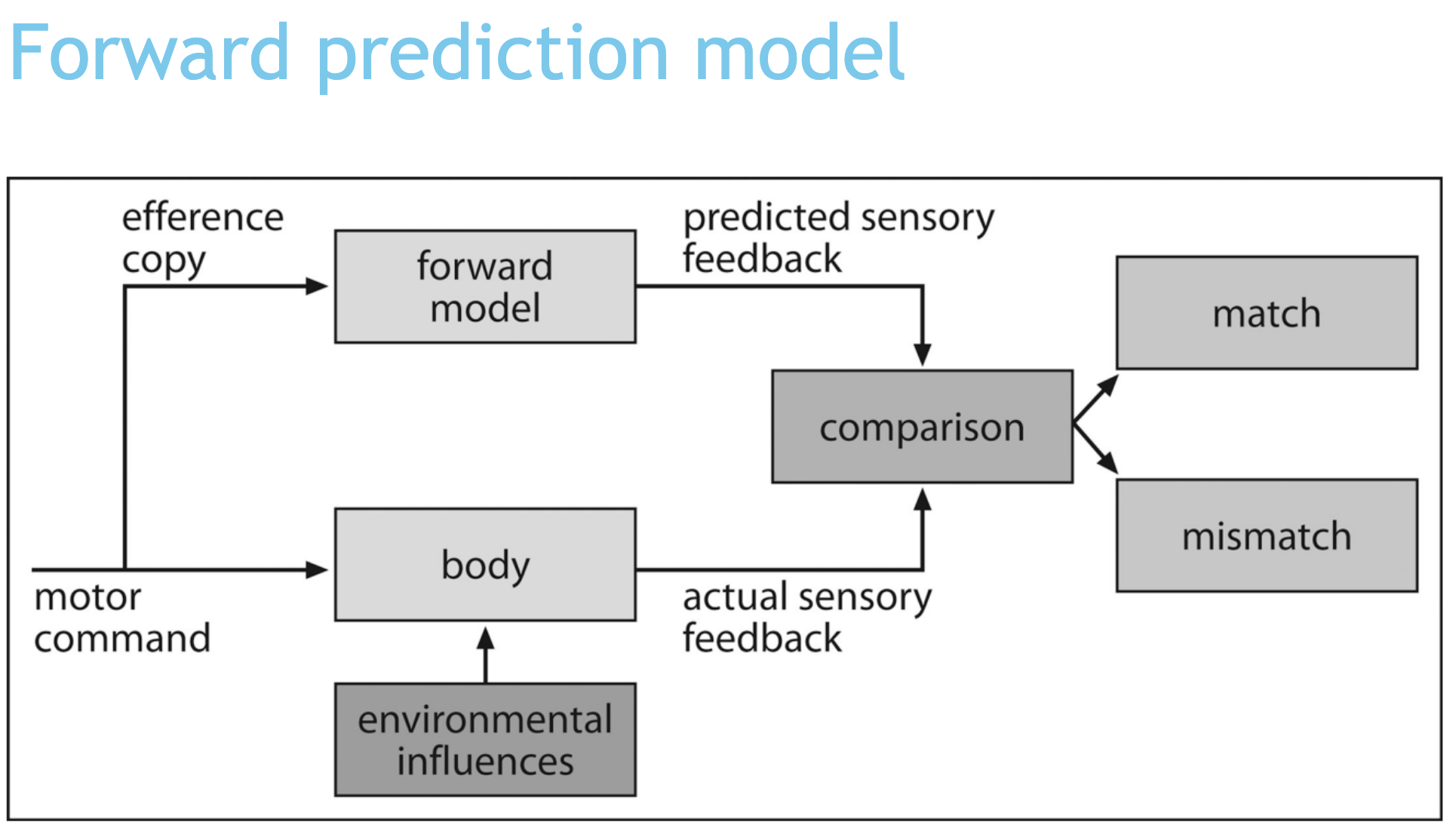
Developmental mechanisms: Cognitive models of hallucinations
Internal voice seems externally generated →
Source attribution
Self monitoring
Forward prediction model
Psychological models of schizophrenia
Aberrant salience (dopamine)
Giving importance / attention to “unimportant” stimuli
Also in ToM
Prediction error (N-Methyl-D-aspartic acid (NMDA) receptors) - delusions
Wrong predictions, explained “differently” to make sense
Abnormal attributions - paranoia
Source monitoring (grey matter reductions in mPFC) – hallucinations
→ Connected to each other!
Salience hypothesese
DA secretion can lead to irrelevant stimulus-reward associations
→ unimportant things become important
Hallucinations – giving importance to internal representations,
→ seem to be external stimuli
Delusions – a ‘top-down’ cognitive explanation of increased importance or of insecurity (need for closure)
→ trying to explain the event
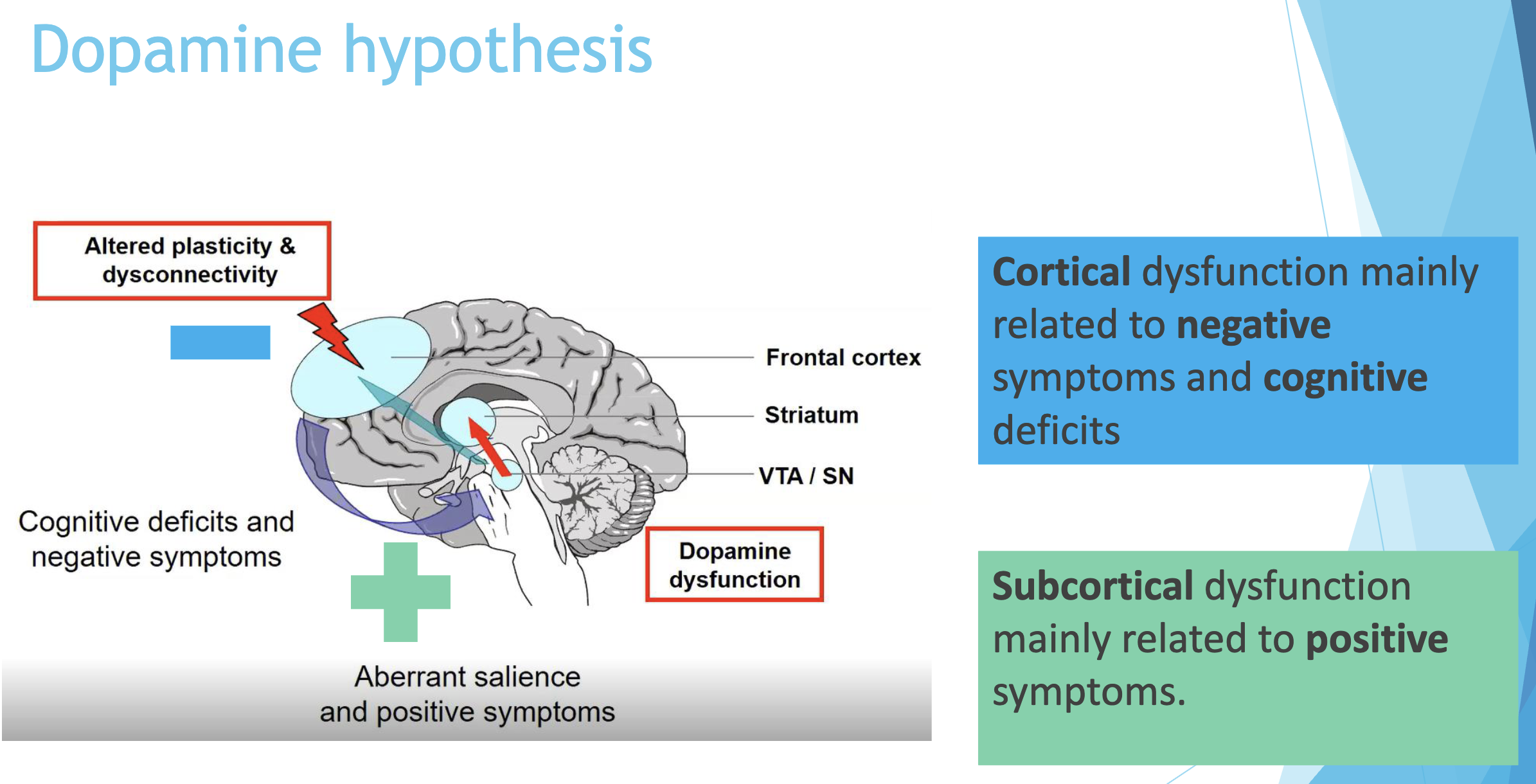
Dopamine and symptoms
Important in reward learning
Important for salience, motivation and attention
Excessive dopamine levels increase salience
→ Leading to positive symptoms like delusions
Medication almost exclusively on DA
1/3 of patients is treatment resistant
→ then Clozapine is prescribed
Dopamine sensitisation
No tolerance (getting used to it), but hyper-sensitive
(c.f. stress, but unlike drugs)
Environment impacts on several neurotransmitter systems, but the dopaminergic system is prone to sensitisation
Treatment of schizophrenia
Antipsychotic medication
Dopamine: risperidone, olanzapine, quetiapine, aripiprazole
Treatment resistant: clozapine
D2 & D4 receptors; Serotonine; Histamine, acetylcholine,
Indirect effect on glutamate (not on NMDA receptors)
Cognitive behaviour therapy (CBT)
Cognitive remediation
“Newer” approaches
In the social environment rather than in an institution (FACT teams)
Integrating first, then other treatment:
Individual placement and support (IPS)
Feeding and Eating Disorders
Disturbance of eating or eating-related behaviour that results in
(1) the altered consumption of food
(2) significantly impaired health and / or functioning
DSM-5 Feeding and Eating Disorders
Feeding Disorders
Pica
Rumination Disorder
Avoidant / Restrictive Food Intake Disorder (ARFID)
Eating Disorders
Anorexia Nervosa (AN)
Bulimia Nervosa (BN)
Binge-Eating Disorder (BED)
Feeding and eating disorders are largely mutually exclusive
Obesity is considered a medical problem, not an eating disorder
Pica
Persistent (1+ month) eating of non-nutritious, non-food substances
Prevalence is unknown
Can occur in typically developing children, but most often comorbid with ASD / IDD
Can result in medical complications and emergencies
Rumination Disorder
Persistent (1+ month) and repeated regurgitation of food
Spontaneous
Food may be re-chewed, re-swallowed, or spit out
Prevalence is unknown
Associated with malnutrition, especially in infancy
Avoidant / Restrictive Food Intake Disorder (ARFID)
Lack of interest in food
May be based on appearance, smell, taste, texture, brand, presentation, or a past negative experience with the food
1+ of the following symptoms:
Substantial weight loss or failure of expected weight gain
Nutritional deficiency
Dependence on a feeding tube or dietary supplements
Significant psychosocial interference
Prevalence unknown
Major Features of Eating Disorders
Weight Concerns
Feeling overweight much of the time
Viewing one’s weight negatively
Body Dissatisfaction
Distress with one’s appearance
Eating Problems
Restricted eating or dieting
Lack of control over eating
Anorexia Nervosa: Symptoms
Restriction of energy intake relative to requirements leading to a significantly low body weight
Intense fear of gaining weight or becoming fat, or persistent behaviour that interferes with weight gain, even though at a significantly low weight
Disturbance in the way in which one's body weight or shape is experienced, undue influence of body weight or shape on self-evaluation, or persistent lack of recognition of the seriousness of the current low body weight
Anorexia Nervosa: Types
Restricting Type: The person does not regularly engage in binge eating.
This is a subtype that is typically associated with the stereotypical view of anorexia nervosa.
Binge-Eating/Purging Type: The person regularly engages in binge eating and purging behaviours, such as self-induced vomiting and/or the misuse of laxatives or diuretics.
The binge eating/purging subtype is similar to bulimia nervosa; however, there is no weight-loss criterion for bulimia nervosa
Anorexia Nervosa: Severity
Based on BMI
Mild: >17
Moderate: 16-16.99
Severe: 15-15.99
Extreme: < 15
Prevalence, Development, and Course of AN
12-month prevalence among females is ~0.4%
Onset typically during adolescence/puberty
Often begins after stressful event or life transition
Course and outcome are highly variable
But most experience remission within 5 years
Risk Factors for AN
Temperament
Perfectionism
Environmental
Cultures that value thinness
Genetic and physiological
Heritable
Brain abnormalities
Functional Consequences of AN
Death from medical complications
Leukopenia
Anemia
Dehydration
Low hormone levels
Heart problems
Kidney problems
Osteoporosis
Electrolyte imbalance
Hypotension
Hypothermia
Dental enamel erosion
Increased suicide risk
Treatment of AN
Treatment for anorexia nervosa tries to address three main areas:
Restoring the person to a healthy weight
Reducing or eliminating behaviours or thoughts that originally led to the disordered eating
Treating the psychological disorders related to the illness
Binge episode
Eating a large amount of food in a short period of time, AND
2000+ calories in <2 hours
A sense of lack of control over the eating
Compensatory behaviour
Inappropriate behaviour that is done in order to prevent weight gain
Classified as "purging" or "non-purging"
Bulimia Nervosa
Recurrent episodes of binge eating
Recurrent inappropriate compensatory behaviour
Self-evaluation is unduly influenced by body shape and weight
The binge eating and inappropriate compensatory behaviours both occur at least once a week for 3 months
The disturbance does not occur exclusively during episodes of anorexia nervosa
Bulimia Nervosa: Prevalence, Development, and Course
Prevalence in females is 1-1.5%
Onset in adolescence / young adulthood
Binging may onset after dysfunctional dieting
Course is chronic
Diagnostic crossover with AN and BED
High comorbidity
Bulimia Nervosa: Risk factors
Temperamental
Impulsivity
Environmental
Childhood abuse
Genetic and physiological
Heritable
Childhood obesity
Early pubertal maturation
Bulimia Nervosa: Functional Consequences
Dental Problems
Swelling of salivary glands
Esophageal problems
Chronic diarrhea
Bowel problems
Suicidal ideation
Binge Eating Disorder
Recurrent episodes of binge eating
Binge eating is not associated with the recurrent use of inappropriate compensatory behavior as in bulimia nervosa
Marked distress regarding binge eating
The binge eating occurs at least once a week for 3 months
Binge eating does not occur exclusively during the course of bulimia nervosa or anorexia nervosa
BED: Prevalence, Development, and Course
Prevalence in females is 3.5% and 2.0% in males
Onset largely unknown
Dysfunctional dieting may onset after binging
Remission rates are high(er)
Crossover is uncommon
High comorbidity
BED: Risk factors
Temperamental
Impulsivity
Genetic and physiological
Heritable
BED: Functional Consequences
Obesity and associated health risks
High blood pressure
Diabetes
Heart disease
Sleep apnea
BN vs. BED Severity
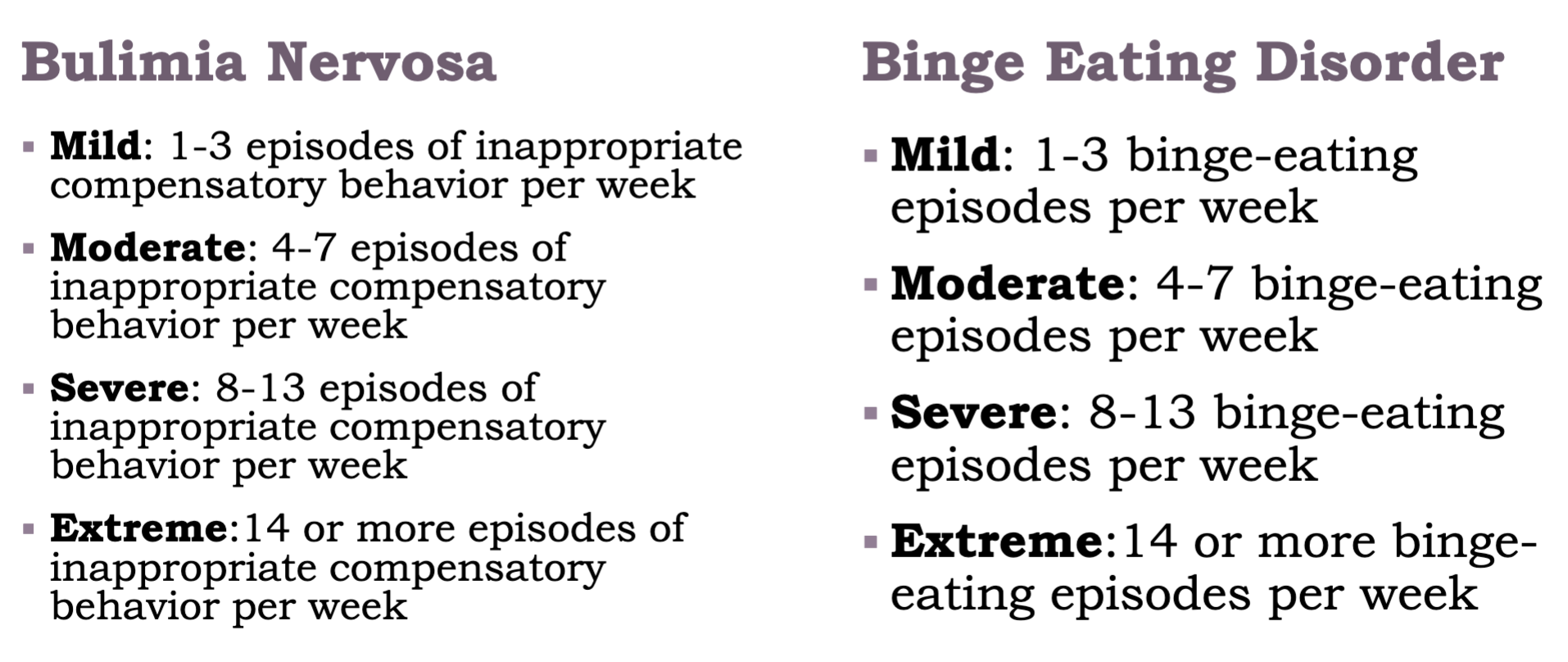
Treatment for BN & BED
Cognitive Behavioural Therapy
Break the binge-purge cycle
Reduce binging and purging behaviours
Challenge automatic negative thoughts
Learn adaptive coping strategies
Nutritionists may also help with structured meal plans and exercise regimens
Medication (SSRIs) can help ease impulse control problems and reduce binge eating