PUBH 6012 Exam 3 Actual questions and answers with 100% accuracy(VERIFIED BY PROFESSOR)
1/107
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
108 Terms
What Is Medicare?
A health insurance program for adults over age 65 and individuals with certain terminal conditions and disabilities
Enacted under Lyndon B. Johnson under Title XVIII of the
Social Security Act in 1965
Medicare is the __________ largest social insurance program in the United States
second
Medicare is administered by....
The Centers for Medicare and Medicaid Services, a federal agency
What is one pathway to Medicare eligibility?
Over 65 years of age and qualify for Social Security benefits (10 years or 40 quarters of earning)
What is the second pathway to Medicare eligibility?
Disability: must qualify for Social Security Disability Income (SSDI) and have been collecting such benefits for at least 24 months
What is the third pathway to Medicare eligibility?
Diagnosis of end-stage renal disease (ESRD), or Lou Gehrig's disease (amyotrophic lateral sclerosis, ALS), and receiving SSDI payments (no waiting period)
Being a U.S. citizen or permanent legal resident gets you ___________________ in Medicare
Entitlement to Part A and eligibility to enroll in Parts
B, C, and D
Medicare Part A
hospitals/inpatient services
Medicare Part B
physicians/outpatient services
Medicare Part C
managed care plans
Medicare Part D
prescription drug plans
Part A Coverage
Includes Inpatient Hospital Care, Skilled Nursing Facility Care, Home Health Care, and Hospice Care.
Part A does not cover
Long-term care
The mandatory 2.9% payroll tax covers ______ of Part A funding
90%
Hospital Insurance Trust Fund is financed by
Mandatory 2.9% payroll tax (Employers pay 1.45%, Employees pay 1.45% for incomes up to $200,000 individual/$250,000 couple)
Sources that cover 10% of Part A funding:
• Taxation on Social Security benefits
• Premiums for those ineligible for Part A
• Interest earned on Hospital Insurance Trust Fund
Part B Coverage
• Physician services (including in a hospital)
• Outpatient services, including durable medical equipment
• Drugs administered by a physician (e.g., chemotherapy)
• Specified preventive services (vaccines and cancer screenings)
• Home health visits
Part B enrollment is...
voluntary
(Cost sharing is 20% coinsurance after deductible is met)
General federal tax revenue covers ______ of Part B costs
73%
Monthly premium covers ______ of Part B costs
24%
"Traditional Medicare" or fee-for-service
Medicare Parts A and B
(Providers are paid based on services rendered (within reason))
Medicare Advantage
Medicare Part C
(managed care (or capitated) plan.
• Medicare pays a set amount of money to a private insurance company to
cover beneficiary care
Managed Care (or capitated) plan
Medicare pays a set amount of money to a private insurance company to cover beneficiary care
Part C financed by...
• Hospital Insurance Trust Fund (42% of Medicare Advantage
spending on parts A and B benefits in 2021)
• Supplemental Medical Insurance Fund (for Parts B and D
benefits)
• Medicare Advantage (MA) cost sharing, deductibles, and
premiums (equal to Part B premiums)
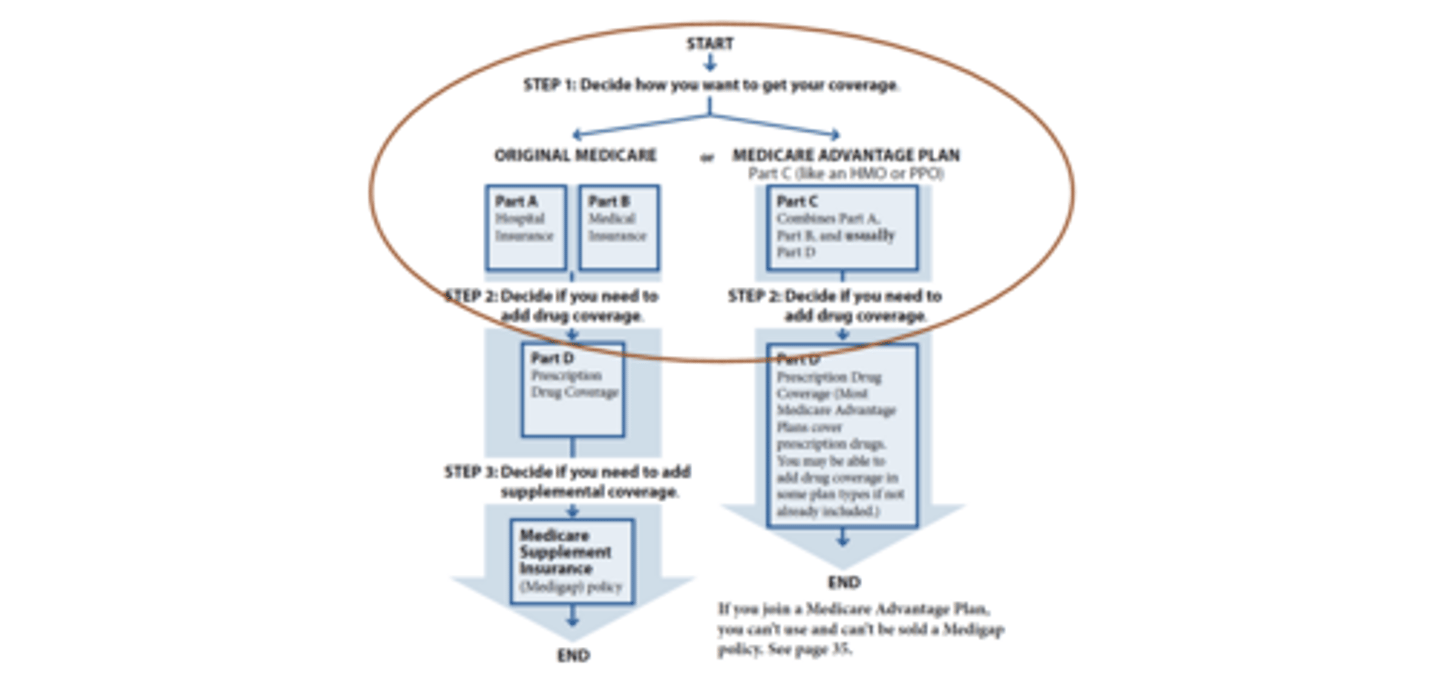
Decisions Medicare Beneficiaries Must Make Each Year
Original Medicare or Medicare Advantage Plan
Part D was created by....
Medicare Modernization Act of 2003, effective 2006
Part D is
voluntary
(90% of all Medicare beneficiaries have creditable drug coverage)
Part D covers
outpatient prescription drugs
(Coverage required for: immunosuppressants, antidepressants, antipsychotics, anticonvulsants, antiretrovirals, and antineoplastics)
Part D offered as
stand-alone prescription drug plans (PDPs) or Medicare Advantage (MA-PDs)
Part D beneficiary costs
• Monthly premium (varies by plan: wide variation nationwide)
• Annual deductible (varies, capped at $505 for 2023)
• Sliding scale small additional premium if income more than
$97,000/$194,000 (from $12.20 up to $76.40)
Part D is financed by
• General revenues (74%)
• Beneficiary premiums (15%)
• State contributions (11%)
(Beneficiary premiums covered about one-fourth of drug coverage)
The Inflation Reduction Act of 2022
Included a provision allowing Medicare to negotiate prescription drug prices
Inflation Reduction Act Changes
Beginning in 2025...
• Department of Health and Human Services negotiates Part B and Part D drug prices for eligible drugs
• Caps prescription drug price increases
• Limits beneficiary out-of-pocket expenditures to $2,000
• Caps insulin costs for Medicare beneficiaries at $35 per month
Supplemental Coverage
Beneficiaries enrolled in traditional Medicare may obtain
additional coverage to help with out-of-pocket costs
(This option is not available for Medicare Advantage
enrollees)
Supplemental coverage options
• Medigap
• Employer-sponsored insurance
• Medicaid
Medigap
Additional insurance offered by private companies to assist with cost sharing
There are 10 plan types available, strictly regulated; prices vary widely by state and plan
All plans of the same letter offer the same benefit package so that beneficiaries can compare
Employer-sponsored supplemental coverage plans
These benefits are less common as fewer employers offer retiree health benefits to employee
State Medicaid programs
Varying levels of assistance with Medicare's premiums and cost sharing for Medicare beneficiaries with low incomes and modest assets (known as "dually eligible beneficiaries")
How Do Providers Get Paid?
Basic Structure & Prospective Payment
Basic Structure
• Define products and services Medicare is buying
• Set relative values for services to be provided
• May be individual services or bundles of services
• Make adjustments (e.g., disproportionate share hospital [DSH], graduate medical education [GME], Physician Quality Reporting Initiative [PQRI], meaningful use—percent
reduction or bonus to the in rate)
Prospective Payment
• Bundled services
• Medicare Prospective Payment System (PPS) applies to hospitals, SNFs, but moving toward similar model for physicians
• Compare to traditional fee-for-service
Solvency of the Medical Insurance Trust Fund dependent on three factors:
1. Economic growth (unemployment level, wages)
2. Trends in health care spending
3. Demographics (increased Medicare enrollment)
Inpatient Prospective Payment System (IPPS)
system in which Medicare reimburses hospitals for inpatient hospital services according to a predetermined rate for each discharge.
Diagnostic Related Groups (DRG)
a classification system used by Medicare and Medicaid to determine payment for health services based on diagnosis, surgical procedures, age, and other information
Outpatient Prospective Payment System (OPPS)
The Medicare prospective payment system used for hospital-based outpatient services and procedures that is predicated on the assignment of ambulatory payment classifications
Ambulatory Payment Classification (APC)
Prospective payment system used to calculate reimbursement for outpatient care according to similar clinical characteristics and in terms of resources required.
Accountable care organizations (ACOs)
Groups of providers coordinate care to Medicare patients to reduce inefficiency and medical errors; ACOs share savings with Medicare
Episode-based payment initiatives
Improve coordination and quality by linking payment for services received under an episode of care (such as knee replacement)
Primary care transformation
Enhance relationship between primary care physicians and patients to facilitate higher quality and better manage chronic conditions
Physicians—from sustainable growth rate (SGR) to Merit-Based Incentive Payment System (MIPS)
If SGR were allowed to take effect, there would have been a 29.5% reduction in physician reimbursement rate for 2012, a 26.5% cut for 2013, and a 24% cut for 2014
New basic structure is MIPS with alternative payment models as options (e.g., ACOs)
Medicare Access and CHIP Reauthorization Act of 2015 (MACRA)
Under the new Quality Payment Program, doctors choose
either:
• Merit-Based Incentive Payment System (MIPS)
• Alternative Payment Models (APMs)
Medicaid Basics
• Authorized by Social Security Act Title XIX
• Signed into law in 1965
• Joint federal-state public insurance program
• Entitlement
• Safety net
Foundations of Medicaid: Entitlement
Eligible Individuals are entitled to a defined set of benefits,
States are entitled to federal matching funds
Foundations of Medicaid: Federal-State Partnership
Federal- Sets core requirements on eligibility and benefits
Partnership
State- Flexibility to administer the program within federal guidelines
Medicaid play a central role in our healthcare system...
Health Insurance Coverage For 1 in 4 Americans
Assistance to 10 million Medicare Beneficiaries
> 50% Long-Term Care Financing
Support for Health Care System and Safety-Net
State Capacity to Address Health Challenges
Medicaid's Role as a Safety Net
• 9/11
• Hurricane Katrina
• Flint water crisis
• Opioid epidemic
• COVID-19 pandemic
Medicaid Traditional Eligibility
• Income
• Assets (No asset limit for eligibility based on low income, State option for eligibility based on old age or disability)
• State resident
• Citizenship/immigration status
• Category
Medicaid Eligibility- Categorical
An individual must fit within a category (e.g., pregnant women) covered by the program
Medicaid Eligibility- Income
An individual/family must earn no more than the relevant income limits, which are expressed as an FPL percentage (e.g., 133% of the FPL)
Medicaid Eligibility- Resources
An individual/family must not have nonwage assets (e.g., car, household goods) that exceed eligibility limits
Medicaid Eligibility- Residency
An individual must be a U.S. resident and a resident of the state in which they are seeking benefits
Medicaid Eligibility- Immigration Status
Immigrants must meet certain requirements, including having been in the country for at least 5 years (for most immigrants)
Medicaid Citizenship/Immigration Requirements
• Undocumented people ineligible
• Legal immigrants with qualified status generally eligible
after five years in the United States
• State option to cover pregnant people and children who
are legal immigrants with less than five years of residency
Medicaid Eligibility Before 2014
To be eligible for Medicaid before the Affordable Care Act's
(ACA) expansion, a person had to both be poor and fit into
a covered category.
• Pregnant
• Disabled (meeting strict federal standards)
• Elderly
• Children
• Parents of dependent children
Who Was Left Out of Medicaid Before 2014?
Poor, Childless Adults
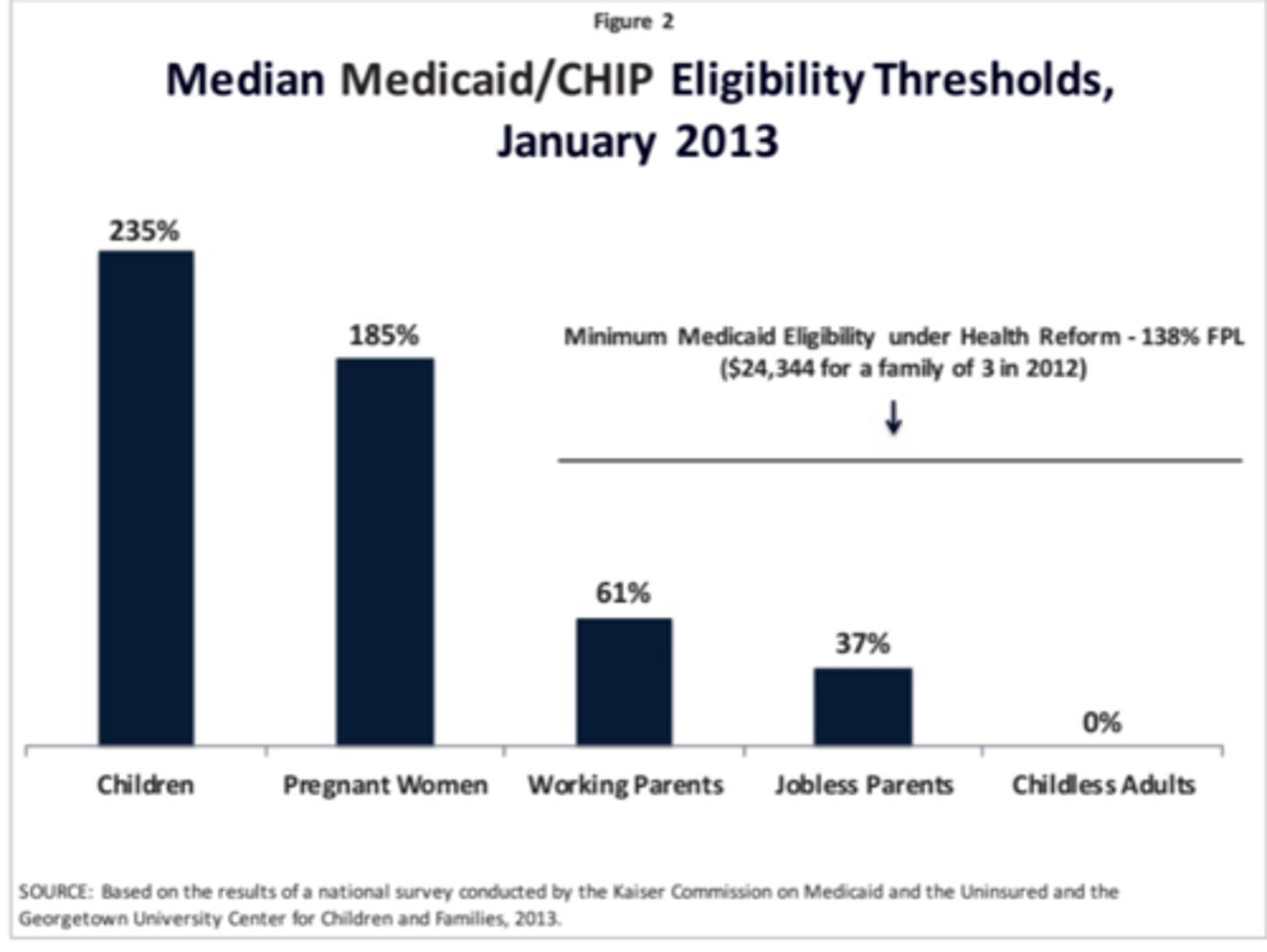
The ACA's Medicaid Expansion
• Beginning in 2014, states would cover nearly all non-
elderly people with incomes at or below 138% FPL.
• The federal government funded 100% of states' costs in
2014 through 2016, gradually decreasing to 90% in 2020
and thereafter.
the ACA Medicaid expansion would cover adults up to 138% FPL
in all states
138% FPL in 2023 equals $20,120/year for an individual and $34,307/year for a family of three.
NFIB v. Sebelius (2012)
The Court found that the Medicaid expansion was unconstitutionally coercive because states did not have adequate notice to voluntarily consent to this program change, and all of a state's existing federal Medicaid funds potentially were at risk for noncompliance
Consequently, Medicaid expansion is a state option
In states that have not adopted the Medicaid expansion...
Poor adults fall into a coverage gap, earning too much to qualify for Medicaid but too little for subsidies for marketplace coverage.
Mandatory State Plan Benefits
• Physician services
• Lab and X-ray services
• Inpatient hospital services
• Outpatient hospital services
• Early Periodic Screening, Diagnostic, and Treatment (EPSDT) (birth through age 21)
• Family planning
• Federally qualified health centers (FQHC) and rural health clinic services
• Nurse-midwifery
• Certified nurse practitioner
• Nursing facility
• Home health for those in nursing facilities
Optional State Plan Benefits: Acute Care
• Prescription drugs
• Medical/remedial care by nonphysician
• Rehabilitation and other therapy
• Clinic services
• Dental services
• Durable medical equipment (DME), prosthetics, eyeglasses
• Primary care case management
• Tuberculosis (TB) services
• Other specified medical or remedial care
Optional State Plan Benefits: Long-term Care
• Intermediate care facilities for intellectual/developmental disabilities
• Inpatient/nursing facilities in mental disease institution (65-plus)
• Inpatient psychiatric hospital (under 21)
• Home/community-based waiver
• Home health care
• Targeted case management
• Respiratory care
• Personal care services
• Hospice care
• Program of All-Inclusive Care for the Elderly (PACE)
EPSDT Benefit (Birth to Age 21)
Early: identifying problems early, starting at birth
Periodic: checking children's health at periodic, age-
appropriate intervals
Screening: doing physical, mental, developmental, dental, hearing, vision, and other screening tests to detect potential problems
Diagnosis: performing diagnostic tests to follow up when a risk is identified
Treatment: treating the problems found
Medicaid's benefits reflect the needs of the population it serves...
Low-Income Families:
•Pregnant Women: Pre-natal care and delivery costs
•Children: Routine and specialized care for childhood development (immunizations, dental, vision, speech therapy)
• Families: Affordable coverage to prepare for the unexpected (emergency dental, hospitalizations, antibiotics)
Individuals with Disabilities:
•Child with Autism: In-home therapy, speech/occupational therapy
•Cerebral Palsy: Assistance to gain independence (personal care, case management and assistive technology)
•HIV/AIDS: Physician services, prescription drugs
•Mental Illness: Prescription drugs, physicians services
Elderly Individuals:
•Medicare beneficiary: help paying for Medicare premiums and cost sharing
•Community Waiver Participant: community based care and personal care
•Nursing Home Resident: care paid by Medicaid since Medicare does not cover institutional care
Medicaid Alternative Benefit Plans
• Benefit package for expansion adults
• Coverage can be equivalent to a benchmark plan (federal
employees, state employees, largest non-Medicaid health
maintenance organization [HMO] in state)
• However, most states align coverage with state plan benefit package
• Must include EPSDT, family planning, mental health parity, 10 essential health benefits, access to FQHC/rural health clinics, nonemergency medical transportation
Medicaid Delivery Systems
Fee-for-service and Capitated managed care
Medicaid Delivery Systems: Fee-for-service
• Traditional model
• State reimburses, providers set rate for each service
• Enrollees see any provider who contracts with state
Medicaid Delivery Systems: Capitated managed care
• Predominant model today
• Health plans receive set monthly payment per enrollee
• Enrollees limited to network providers
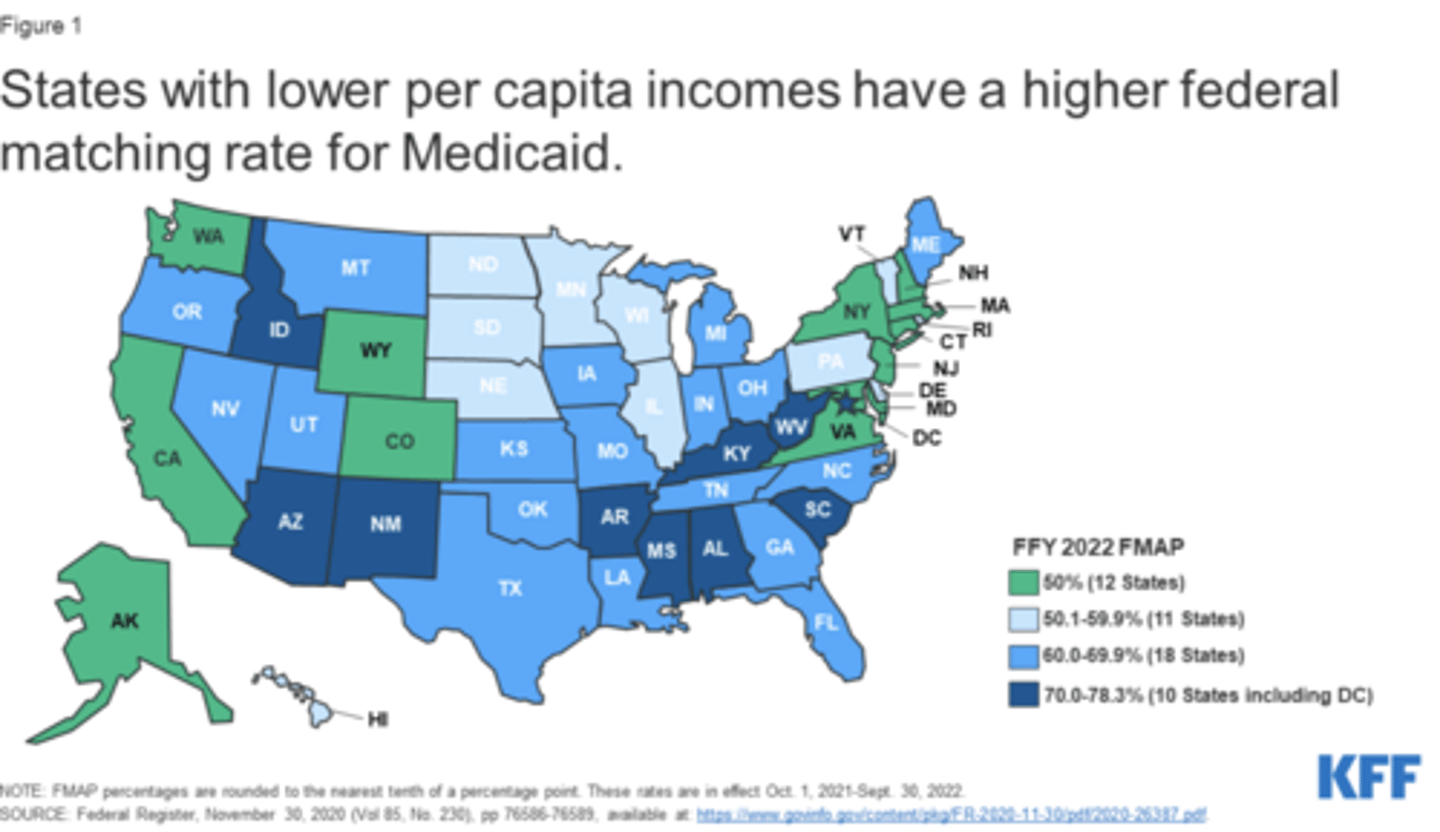
Federal Medical Assistance Percentage (FMAP)
• Formula based on state per capita income relative to national average
• Ranges from 50% to about 78%
• Some services/populations receive an enhanced FMAP
(e.g., expansion adults)
• Congress historically has temporarily increased the FMAP
to support states (e.g., COVID-19 pandemic, economic
downturns, natural disasters)
States with lower per capita incomes have a _______ federal matching rate for Medicaid
higher
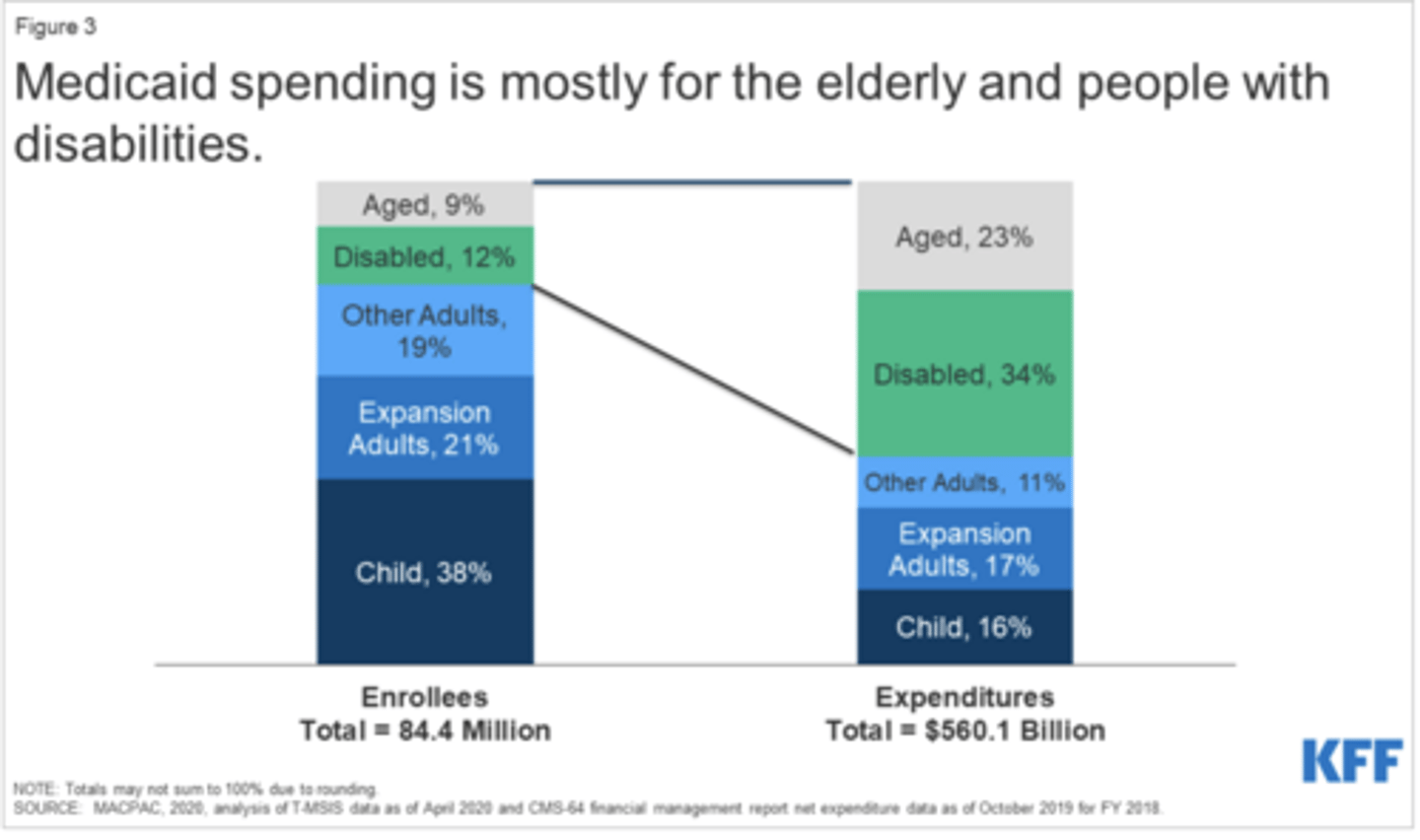
Medicaid spending is mostly for ....
the elderly and people with disabilities
CHIP Basics
• Authorized by Social Security Act Title XXI
• Signed into law in 1997
• Joint federal-state public insurance program
• Uninsured children in families with income above Medicaid
limits
• State option to cover pregnant women
• Capped federal funding
• Currently authorized through 2027
States can choose to administer their CHIP program as:
• An expansion of their Medicaid program
• A separate CHIP program
• A combination of the above
Benefits in Separate CHIP Programs
Benchmark coverage
Must include:
• Well-baby and well-child visits
• Dental
• Mental health parity
• Vaccines
Vision and hearing are optional
CHIP Financing: Federal Matching Rate
Federal government provides matching funds up to a cap
for each state
Enhanced federal matching rate, compared to Medicaid
• Generally, about 15 percentage points higher than state's
Medicaid rate
• Averages 71% nationally
Medicaid Continuous Enrollment Requirement
Everyone enrolled on or after 3/18/20 must remain enrolled
Regular Medicaid Eligibility Process
It includes application, verification, redetermination, and renewal steps
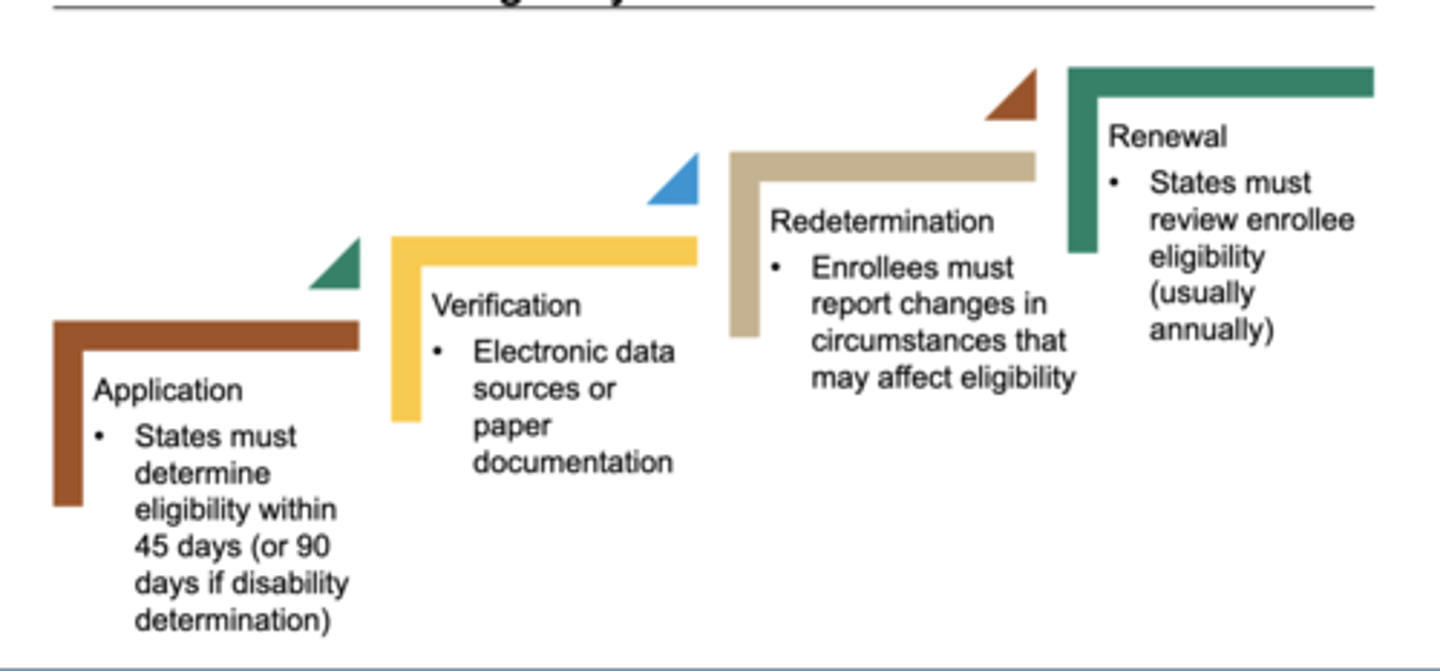
How did continuous enrollment affect the regular medicaid enrollment process?
Backlogs, suspended, outdated...
SDOH Are Everywhere
Health disparities reflect fundamental decisions about how society is structured
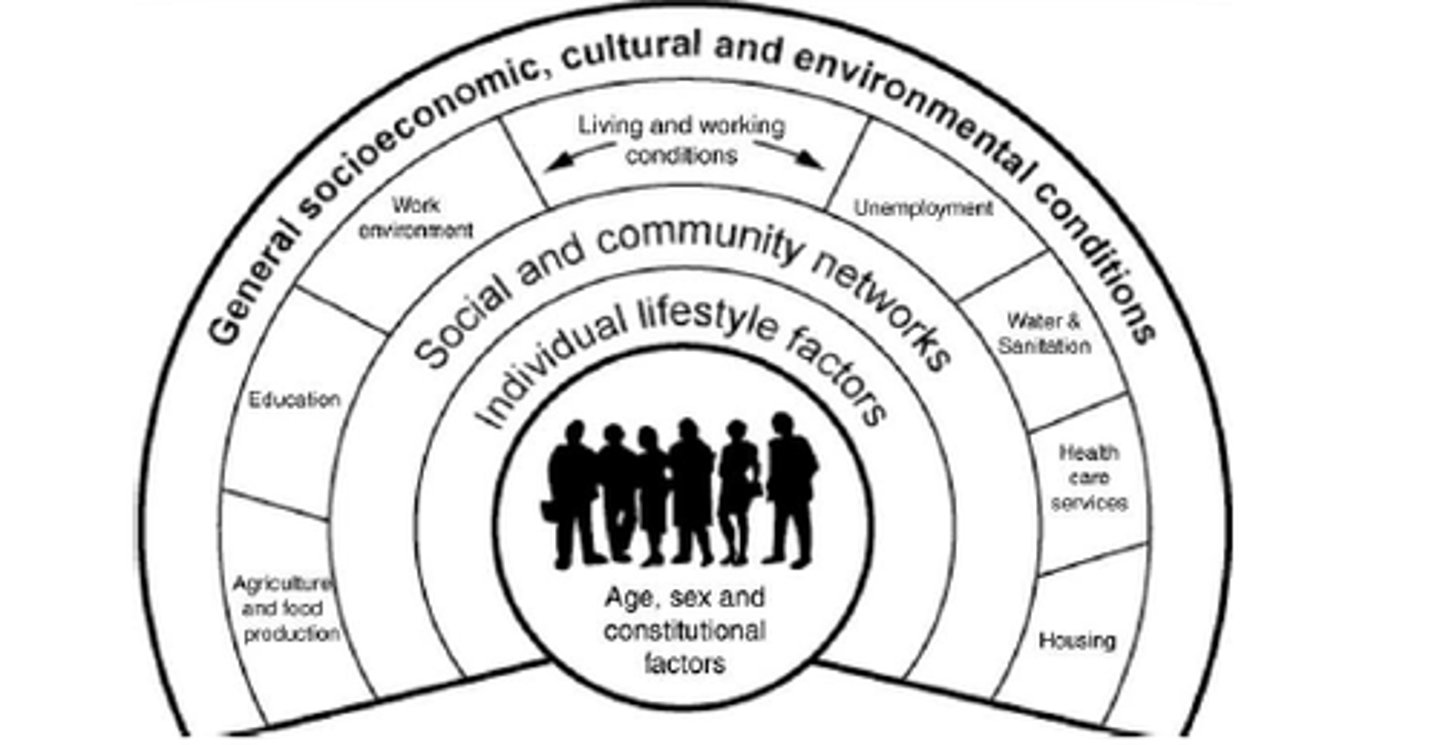
Two broad categories of health disparities:
- Health (STATUS) disparities
- Health (CARE) disparities
Defining Health STATUS Disparities
"Differences in the incidence, prevalence, mortality and
burden of diseases and other adverse health conditions that
exist among specific population groups in the United States.
Research on health disparities related to socioeconomic
status is also encompassed in the definition." National
Institutes of Health (2000)
Defining Health CARE Disparities
"...racial or ethnic differences in the quality of healthcare that are not due to access-related factors or clinical needs,
preferences and appropriateness of interventions." Institute of Medicine (2002)
High Quality Health Care Is...
Safe: avoiding injuries to patients from the care that is intended to help them
Timely: reducing waits and sometimes harmful delays for those who receive as well as those who give care
Efficient: avoiding waste, including waste of equipment, supplies, ideas, and energy
Effective: providing services based on scientific knowledge to all who could benefit and refraining from providing services to those not likely to benefit (avoiding underuse and overuse, respectively)
Equitable: providing care that does not vary in quality because of personal characteristics such as gender, ethnicity, geographic location, and socioeconomic status
Patient-centered: providing care that is respectful of and responsive to individual patient preferences, needs, and values and ensuring that patient values guide all clinical decisions
What Are Disparities in Health Care Quality?
Racial or ethnic disparities are differences in the quality of health care received by members of different racial or ethnic groups that are not explained by other [acceptable or appropriate] factors.
Emergency preparedness
The ability to prevent, prepare for, protect against, respond to, and recover from health emergencies
Public health emergencies
Scale, timing, or unpredictability threaten to overwhelm routine capabilities to provide health care
• Span a broad range of emergency and disaster situations,
including natural hazards, acts of terrorism, and large-scale
infectious disease outbreaks
With two major events came the sharp realization that the United States could not properly respond to a large-scale bioterrorism attack on the country
2001 anthrax attacks and the attack on the World Trade Center
What Is the Role of Public Health in Emergency Preparedness?
• Public health's role in emergency preparedness is first to
plan effective strategies to minimize morbidity and mortality following an emergency or disaster.
• As a starting point, public health is responsible for participation in the hazard vulnerability assessment of the
community or jurisdiction.
Public Health Threats
• Biological threats
• Natural disasters
• Chemical and radiological materials
Ready for Emergencies (CDC)
• Emergency operations
• Laboratory response
• Strategic National Stockpile
• Safeguarding research
• State and local readiness
• Global emergency preparedness