Renal Dysfunction
1/24
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
25 Terms
List causes of urinary tract obstruction
Interference of flow of urine at any site along tract and urine accumulates
causes =
tumors (benign prostatic hyperplasia or carcinomas)
stones - calculi (inflammation of gi tract)
trauma (loss of peristalsis)
pregnancy (loss of bladder muscle function
neurogenic bladder (edema)
The outcome of obstruction is
compression of the kidney structures from accumulation of urine, with ischemic atrophy of the papilla and medulla. May result in failure to concentrate urine and large amount of dilute urine.
Major types of stones
Calcium = 75-80% of stones. Idiopathic, often found in middle aged men with family history. Association with hypercalciuria, hyoeruricosuria, and prolonged immobilization
Struvite = 15% of stones. Crystals of magnesium, ammonium phosphate - precipitated by urea- splitting organisms (Pseudomonas and Proteus) found in alkaline urine, common in women
Uric Acid stones (gout) = Caused by high levels of uric acid in the urine, due to high purine diets (meat/fish/poultry) and concentrated acidic urine
Major clinical manifestation of renal calculi is
pain which will vary in location and severity
the pain can be severe and require narcotic analgesia for relief
Treatment of renal calculi and goal of treatments
Goal: is to prevent new stone formation and to reduce the size of stones that have already formed
reduce stone forming substances in urine through diet changes and high fluid intake
altering pH of urine
surgical removal
lithrotripsy (high energy shock waves fragment stones for excretion
lasers - break up stones
urethral catheters - inserted past the obstruction
nephrostomy tube - may be inserted into the renal pelvis
Describe the neurogenic bladder
Urinary tract obstruction caused by an interruption of the nerve supply to the bladder. Characterized by underactive bladder function
upper motor neuron lesion causes loss of voluntary control of voiding
lower motor neuron lesions cause loss of both voluntary and involuntary control of urination
What is the neurogenic bladder commonly associated with?
Usually associated with infection due to:
bladder distention and urine retention
placement of catheters
development of stones caused by bone resorption due to physical immobility
development of a fever frequently accompanied by chills, shivering, bacteriruia
What is the most common renal neoplasm & their clinical manifestations
Renal cell carcinoma = 85%, most common renal neoplasm and represents approx 2% of cancer deaths
most often in men 50-60 years
tumors usually occur unilaterally and spread through the lymph nodes and blood vessels
What is the most common cause of urinary tract infection and what microbes are involved?
Caused by bacteria and are diagnosed by culture of urine with counts of 100,000 bacterial per ml of urine
gram negative E.coli, Klebsiella, Enterobacter
Pseudomonas or proteus into urethra or bladder
can occur anywhere along urinary tract
Most common site of UTI and the different types of this inflammation
Cystitis = inflammation of bladder and most common site
hyperemic = red mild inflammation
hemorrhagic = diffuse hemorrhage
suppurative = pus formation
ulcerative = sloughing of the bladder mucosa
gangrenous = necrosis of the bladder wall
Why do women more commonly develop cystitis?
Shorter urethra, closeness of urethra to the anus, contamination of vaginal secretions
The usual causative organism in acute pyelonephritis
An infection of the renal pelvis. Causative organism usually bacteria refluxed from the bladder (vesiocuretral) - E.coli
Chronic pyelonephritis vs acute pyelonephritis
Chronic = defined as recurrent autoimmune infection of the kidney with inflammation and scarring. more likely to occur in patient who have renal infections associated with some type of obstructive pathologic condition. chronic obstruction prevents elimination of bacteria resulting in progressive inflammation, causing fibrosis and scarring
pelvis and calyces become dilated and blunted; gradual destruction of the tubules occurs with atrophy and scarring
Acute = infection of the renal pelvis and interstitium. inflammatory process is usually focal and irregular, primarily affecting pelvis, calyces and medulla. This causes infiltration of WBCs, inflammation and purulent urine.
Nephritic vs nephritis (glomerulonephritis) glomerular disease
Nephritic = characterized by hematuria with red cell casts and varying degrees of proteinuria (symptoms)
Nephritis = an inflammation of the glomerulus (most common cause of chronic and end stage renal failure)
How do glomerular disorders affect function?
Glomerular damage causes a decrease in —> glomerular membrane surface area
edema - associated with hypoalbuminemia and/or salt and water retention from reduced GFR. May need diuretics or dialysis
glomerulonephritis - inflammation of the glomerulus that can be caused by immunologic abnormalities, drugs or toxins, vascular disorders, systemic diseases
glomerulonerphritis - most common cause of chronic and end-stage renal failure
Most frequent cause of acute glomerulonephritis
Caused by post-streptocaoccal infection and it is seen 7-10 days post strep
abrupt onset of symptoms:
hematuria
oliguria
RBC casts
edema
proteinuria
hypertension
decreased GFR
Good-Pasture Syndrome
Associated with the antibody formation against both pulmonary capillaries and glomerular basement membranes.
occurs in men 20-30 yrs
extensive proliferation of cells in bowman’s space with crescent formation
rapid decline in glomerular function —> failure in a few weeks or months
prognosis is poor; dialysis or transplantation may be required
Chronic glomerulonephritis
Includes a variety of glomerular diseases with progressive courses leading to renal failure
pathologic changes seen include:
prolifeation of mesangial cells
focal or diffuse segmental fibrosis and glomerular deterioration
tubular dilation and atrophy
Nephrotic syndrome
The excretion of 3.5 grams or more of protein in the urine per day is a characteristic of glomerular injury. Characterized by proteinuria
May interfere with the immune system
other clinical findings include:
hypoalbuminemia
edema
lipiduria
hyperlipidemia
When does renal failure occur
Decline in renal function is about 25% of normal or a GFR of 25-30 ml/min. When less than 10% of renal function remains = end stage renal failure (ESRF). Can be acute and rapidly progressive (reversible). Slow and chronic over a period of months/years = irreversible
Azotemia and uremia
Azotemia = increased serum urea and creatinine levels
Uremia = elevated creatinine and urea levels, accompanied by fatigue, anorexia, nausea, vomiting, pruritis and neurologic changes
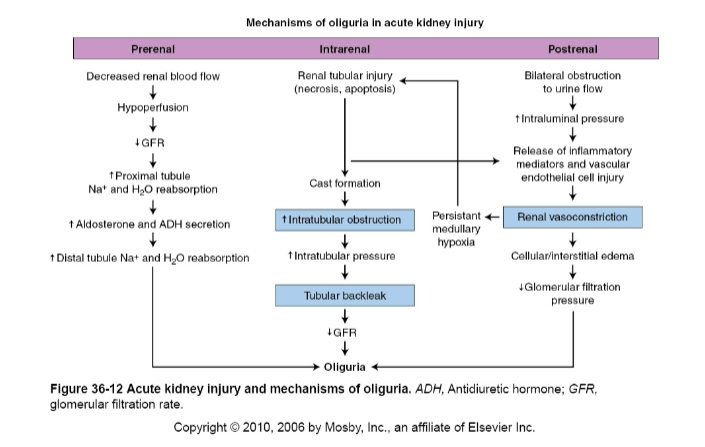
Prerenal vs intralrenal vs postrenal acute failure
Prerenal = caused by impaired renal blood flow (vasoconstriction, hypotension, hypovolemia, hemorrhage, inadequate cardiac output
Intrarenal = may result from acute tubular necrosis, cortical necrosis, acute glomerulonephritis, malignant hypertension, DIC, renal vasculitis
Postrenal = usually occurs with urinary tract obstruction that affects the kidneys bilaterally
Oliguria/anuria and diuresis
oliguira/anuria = may last ½ weems. BUN (blood urea nitrogen) and creatinine levels rise
diuresis = increase in urine volume with fluid losses of 3-4 L/day. Mineral wasting
Primary goal of therapy in renal failure
Goal of therapy = maintain life until renal function as been recovered.
correcting fluid imbalance
treating infections
Clinical couse of chronic renal failure
asymptomatic; decreased renal reserve
renal insufficiency; more than 75% of renal tissue destroyed (GFR is 25% of normal)
end stage of renal failure or uremia; approx 90% of nephron mass has been destroyed
GFR is 10% or less of normal = creatinine and BUN (blood urea nitrogen) increase = patient show symptoms
death unless transplant or dialysis performed