maternity chapter 17: complications of newborn
1/78
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
79 Terms
perterm neonates - most important predictors of an infants health and survival are:
period of gestation
birth weight
what are the leading causes of infant death in the U.S. AFTER congenital malformations
prematurity
LBW
nonmodifiable risk factors for preterm labor and birth
previous PTB
mult. gest.
uterine or cervical anomaly
race or ethnic group
pregnancy induced HTN
short interval btwn. pregnancies
Premature ROM
Bleeding in thr second or third trimester
Family history of premature birth
modifiable risk factors for PTL/PTB
age pregnancy at <17 or >35 yo
unplanned preg.
low socioeconomic status or poverty
low education level
domestiv ciolence, unsafe environment
life stress
IVF and pregnancy after IVF
low prepregnancy weight or obesity
health problems that can be treated: HTN, diabetes, clotting problems, anemia
STI or other infections along GU tract
substance or alcohol use
cig smoking or second hand smoke
long hours of work or standing
late or no prenatal care
airpollution or exposure to other toxins such as lead or paint
ballard gest. age assessment and tool
figures 15-5 and 15-7 in Durham XD
what is the brazelton neonatal behavioral assessment scale
evaluates the neonates responses to the environment
what is the neuromuscular assessment of gest. age on ballard score
posture
square window
arm recoil
popliteal angle
scarf sign
heel to ear
Posture: ballard score, in preterm infant
have immature flexor muscles, floppy

Posture: ballard score, in full term infant
hold their arms close to the body with elbows sharply flexed

ballard score: square window test on pre term infant

ballard score: square window test on fullterm infant

arm recoil on baby : ballard score

popliteal angle on preterm baby

popliteal angle on term baby

scarf sign in term baby

scarf sign in preterm baby

heel to ear in term baby

heel to ear in preterm baby

physical characteristics in ballard score assessment
skin
lanugo
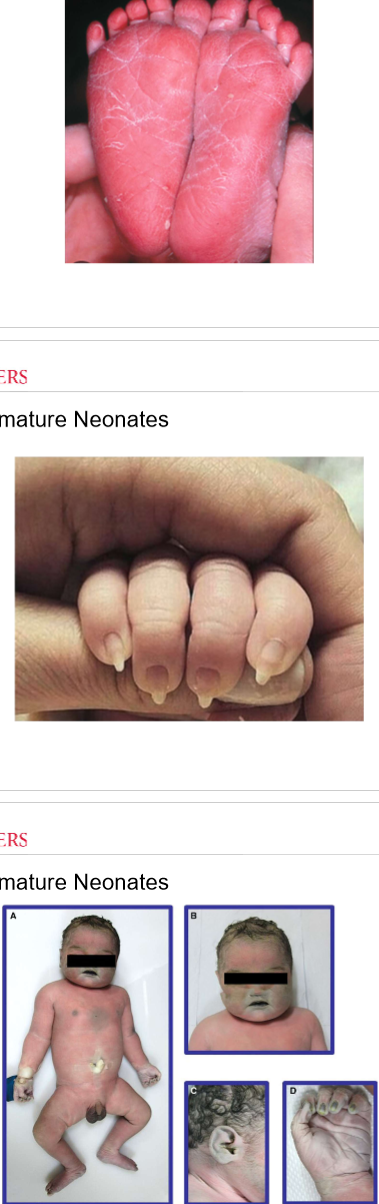
plantar surface
breasts
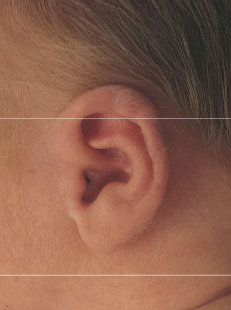
eyes and ears
genitals
skin in preterm baby
transluscent because it is thin and has little sq fat beneath surface. skin is red, sticky, fragile, veins visible
skin in term baby
thicker, color is paler, few veins visible, vernix only present in creases
peeling, cracking of skin - check out ankles and feet
skin in post term baby
deep cracked skin and dry and thick as leather
lanugo in preterm baby
increases in amount until 28 wks
mostly shed by 32-36 weeks
lanugo in term baby
may still seen in upper bacl, shoulders, ears, sides of forhead
lanugo in post term baby
usually no lanugo
plantar surface in preterm baby
few creases seen across the entire foot

pantar surface of postterm baby
deep creases

breasts with preterm baby
nipples, areola, and size of breast buds are not visible
breast with term baby
breast buds may enlarge until they are ~1 cm at term
ears and eyes in preterm baby

ears and eyes in term baby
female genitals in preterm baby
labia majora doesnt rly cover minora and clitoris at all
female genitals in term baby
labia majora cover minora and clitoris compleltely
male genitals in term baby
pendulous scrotum with deep rugae
male genitals in preterm baby
testes may not be descended and rugae are few
gestational age and infant size
small for gest age: below 10th percentile
large for gestaional age: above 90th percentile
appropriate for gest. age: btwn 10th and 90th percentile
monitor for complications common to age and size of infant
behavioral changes: orientation
ability to pay attentuon to interesting visual or auditory stimuli
behavioral changes: habituation
infants response to bisual, auditory, or tactile stimulation
infants typically habituae to unpleasant stimuli such as bright lights
behavioral changes: self consoling activities
normal newborns are able to self console
bringing hands to mouth, sucking on dists, listening to voices, watch objects in environment
preterm infants, il, exposed to drugs prenatally are less likely to self console
behavioral changes: parents response
nurse should note parents response to infants behavior and facilitate attachment and bonding
deep sleep
no body movement except an oaccasional startle reflex
external stimuli are less likely to awaken the infant
no eye movements occur
light sleep
makes up the largest portion of sleep
neonate may easily startle, may smile or make brief fussy sounds
have random body movemnts and display rapid eye movement (REM)
neonate will be much easier to wake up than while in deep sleep
drowsy
intermitten body movement occurs
eyes open and close and have a dul, heavy-lidded appearance
external stimuli will most likely wake the noenate
quiet alert
neonates eyes are wide open with a bright look
infant is relaxed and most attentive to environment and caregivers present
providing visual or other pleasurable stimuli often can maintain this state
active alert
there is a considerable body movement with periods of fussiness or irritability
neonate response to disturbing stimuli (such as excessive noise or activity, cold, fatigue, or hunger) with incr. motor activity and fussiness
consoling or correcting interventions may settle the infant back to a quiet alert state
crying state
there is a high motor activity and the noenate is difficult to calm
eyes are opened or tightly closed and there is an extreme response to unpleasant stimuli
crying is the noenates communication signal that limits have been reached
self consoling can occur, whereas other times the caregiver will need to intervene
neutral thermal environment
premature neonates are unable to protect themselves against fluctuations in environmental temp because of thin, immature skin and limitef stores of subcutaneous brown fat
nurses must implement interventions to maintain a neutral thermal environment (NTE) and prevent cold stress
nursing actions of neutral thermal environemnt
dry infant immediately after birth
place plastic barriers made of polythylene over preterm neonates (less than 32 wks gestation) after birth to prevent heat loss
use of a chemical warming mattress
prewarm all supplies and equipment
control environmental temperature with use of the servo control setting on transpor equipment, radiant warmers, and incubators
what is respiratory distress syndrome (RDS)
life threatening lung disorder that results from small, underdeveloped alveoli and insufficient levels of pulmonary surfactant > cause an alteration in elveoli surface tension that eventually results in atelectasis
Incidences of RDS are inversely related to gestational age and birth weight, affecting 51% of neonates bron weighing less than 1000 g
complications of RDS
patent ductus arteriosus
pneumothorax
bronchopulmonary dysplasia
pulm. edema
hypotension
anemia
oliguria
hypoglycemia and altered calcium and sodium levels
retinopathy of prematurity
seizures
intraventricular hemorrhage
assessment findings of RDS
RDS varies based on degree of prematurity
resp. difficulty begins immediately or within a few hours after the deluvery
tachypnea
retractions
audible expiratory grunting
nasal flaring
skin color is gray or dusky
breath sounds are decr. and + crackles
tachycardia
nursing actions for RDS
provide resp. support
maintain patent airway
if noenate is intrubated, assess for correct placement of endotracheal tube
listen for equal breath sounds
admin O2 as per order
Minimize O2 demand by maintaining a neural thermal environment and decr. risk of cold stress
Monitor I&Os
what are postmarture neonates
neonates born >=42 wks of GA
can result in an LGA or SGA infant
LGA - unknown reason
SGA - placenta is no longer functioning optimally and fetus is forced to use its SQ fat and glycogen stores
risk factors for post mature neonates
anencephaly
history of post term pregnancies
first pregnancy
grand multiparous women
complciations of postmature neonates
meconium aspiration
fetal hypoxia r/t placental insufficiency
neurological complications seizures r/t fetal hypoxia
hypoglycemia r/t decr. glycogen stores
hypothermia r/t loss of SQ fat
polycythemia r/t compensatory response caused by altered oxygenation
assessment findings of postmature neonates
dry, peeling, cracked skin
lack of vernix
profuse hair
long fingernails
thin, wasted appearance
meconium staining (green or yellow staining on skin, nail beds, or umbilical cord)
hypoglycemia
poor feeding behavior
nursing actions of post mature neonates
assess the prenatal record and intrapartum history including APgard scores for risk factors
Assess the noenate for:
GA with use of gestational age scoring system
Respiratory distress
Cyanosis
O2 sat if resp. distress or cyanosis is present
signs of meconium staiing
Blood glucose levels
Vitals
weight
gross anomalies
Monitor for hypoglycemia
Jitteriness, irritability, poor feeding, apnea, grunting, lethargy
Provide early and frew. feedings if resp. status is stable
early and frew. feeding reduce the risk of hypoglycemia
Monitor I&Os
Postterm infants may be poor feeders and thus at risk for inadequate fluid intake
what is meconium aspiration syndrome
is a cause of repsiratory failure in term and post term neonates
assessment findings of meconium aspiration
meconium stained AF
greenish or yellowish discoloration of skin, nails, umb. cord
Resp. depression
Low APGAR scores
Signs of resp. distress
Chest may appear barrel shaped
Atelectasis
nursing actions of meconium aspiration
assist with suctioning and resuscitation at the time of delivery
assess neonate for:
Resp. distress such as grunting, flaring, retracting, cyanosis, and tachypnea
Complications of MAS, such as acidosis, hypoglycemia, hypocalcemia, pneumonia, pneumothorax, BPD, and persistent pulmonary hypertension
Neurological problems secondary to asphyxia
admin O2 or assisted ventilation as per order
monitor blood glucose
Complication of resp. distress is an incr. metabolic rate and thus a higher incidence of hypoglycemia
manage neonates receiving cooling, iNO, or ECMO
hyperbilirubinemia
neonatal jaundice is the yellow orange tint that can visualized in the sclear and skins of neonates with hyperubinemia (incr. bilirubin in the blood)
hyperbilirubinemia is categorized into 2:
physiological jaundice
pathological jaundice
unconjugated (also called indirect) + conjugated (Direct) =
total serum bilirubin (TSB)
unbound (unconjugated) bilirubin
can deposit into tissue and cross the blood brain barrier
it cannot be excreted and can settle in tissues, causing jaundice
kernicterus: accumulation in baby’s brain = brain damage
conjugated bilirubin
is bound to albumin and once bound is water soluble
it is nontoxic and can be exceted through the GI tract
serum bilirubin
cannot be excreted until it is conjugated
physiological jaundice
hysiological jaundice results from hyperbilirubinemia that commonly occurs after the first 24 hours of birth and during the first week of life
it is caused by the breakdown of RBCs (hemolysis)
phys. jaundice: incr. risk for hemolysis is due to:
neonates reabsorb incr. amounts of unconjugated bilirubin in the intestine due to lack of intestinal bacteria,d ecr. GI motility, and incr. beta-gluuronidase ( a deconjugating enzyme)
diminished cnjugation of biirubin in the liver
higher RBC mass relative to body weight than adults
shorter RBC life span of 70-90 days, compared with 120 days in adults
high bilirubin production
assessment findings of physiological jaundice
phys. jaundice is typically visible after 24 hours of life
TSB levels generally peak on day 3 of life in term neonates and on days 5-6 in preterm neonates
jaundice is characterized by a yellowish tint to the skin and sclera of the eyes
As TSB levels rise, jaundice will progress from the newborns head down toward the trunk and lower extremities
what is pathologic jaundice
results when various disorders exacerbate physiological processes that lead to hyperbilirubinemia of the newborn
such disorders can result in pathological unconjugated or conjugated hyperbilirubinemia
because conjugated hyperbilirubinemia is always pathological, further investigation must be done to determine its cause
pathologic jaundice: common cause of conjugated hyperbilirubinemia include -
parenteral nutrition (most common cause in the NICU, especially in preterm infants)
idiopathic neonatal hepatitis
biliary atresia
bile duct stenosis
metabolic and genetic defects
endocrine disorders
infection
some medications
shock
pathologic jaundice: common cause of unconjugated hyperbilirubinemia include -
breastfeeding jaundice (early onset)
breast milk jaundice (late onset)
Rh and ABO incompatibilities
Glucose-6-Phosphate dehydrogenase (G6PD) deficiency
Hemoglobinopathies
Blood sequestration (bruising, cephalohematoma, intracranial bleeding)
polycythemia
metabolic and endocrine disorders
GI obstruction
infection
pathologic jaundice assessment findings
criteria to differentiate pathological jaundice from phsyiological jaundice in a full term neonate:
Jaundice that occurs within the first 24 hours of life
TSB levels that incr. > 0.2 mg/dL per hour
jaundice lasting >2 weeks
TSB exceeding rhe 95th percentile for age in hours
A high direct bilirubin (1.5-2 mg/dL)
Risk factors, med management, and nursing actions are similar for both physiological and pathological jaundice
maternal risk factors - pathologic jaundice
american indian, east asian, or mediterranean descent
ABO incompatbility (e.x. the mother has blood type O and neonate has blood type A or B)
Rh incompatibility (mother is Rh neg and the neonate is Rh positive)
Breastfeeding
Diabetes
Use of oxytocin or bupivacaine during labor
neonatal factors - pathologic jaundice
delayed cord clamping, which incr. RBC volume
Hypoxia, asphyxia, acidosis, and temperature instability
delayed or infrequent feedings, or lethargy
excessive weight loss after birth
bruising or cephalohematoma
Prematurity
G6PD deficiency
bacterial or viral infection
care of neonate receiving phototherapy
assess degree of jaundice with use of transcutaneous meter per unit policy
visually assess degree of jaundice by using a finger to blanch the neonates skin on the face, upper trunk, abdomen, thigh, and lower leg and feet. the skin will appear yellow after the pressyre is released and before skin returns to normal color
document the assessment findings
how rapidly the degree of jaundice progresses guides the method of treatment
Implement phototherapy as ordered
intensive phototherapy lights should be positioned 12-16 inches from the infant and 2 inches fom the top of an incubator
a photometer should be used to measure irradiance of lamps to facilitate optimal treatment
vitals including temp monitoring should be done per agency protocol
monitor I&Os, phototherapy results in incr. insensible fluid loss
assess side fx of phototherapy
observe eyes for discharge and tearing
animal studies have indicated that retinal damage may occur so opaqye eye shields must be used to prevent potential eye damage
assess position of eye shield to ensure it does not occlude nares
loose stools
dehydration
hyperthermia
lethargy
skin rashes
what is group b strep
primary cause of neonatal meningitis and sepsis in the U.S.
assessment for GBS
anterpartum screning: rectovaginal swab at 36 0/7 to 37 6/7 weeks of gestation
If positive, need intrapartum antibiotic prophylaxis
no abx needed if a pt has a scheduled c-sec is perfomred in the setting of intact membrances
infants with early onset GBS sepsis become symptomatic by 12-24 hours of age