Chapter 14 - Eating and feeding disorders
1/41
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
42 Terms
Disordered eating habits
A person’s belief that cultural standards for attractiveness, body image, and social acceptance are closely tied to the ability to control one’s diet and weight gain
Western sociocultural values and preoccupation with weight and dieting
May be internalized and expressed in children as young as age 7-10
In a study of grades 5 to 8; _____ had tried to lose weight in the past 7 days.
60%
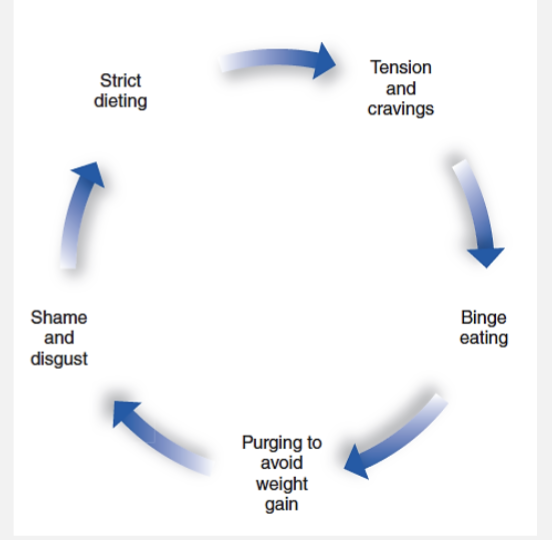
Dieting may lead to a vicious cycle of:
weight loss and weight gain
Overeating
the “false hope syndrome"
initial commitment to change appearance = short-term mood and self-image boost, which then decreases after failure.
binge eating and subsequent purging.
The Binge purge cycle
Purging is followed by disgust and self-recrimination, which prompts renewed vows of abstinence and sets the stage for the whole cycle of dieting, overeating, dietary failure, and affective distress to begin again
metabolic rate
The body’s balance of energy expenditure. Metabolic rate is determined by genetic and physiological makeup, along with eating and exercise habits.
Individual metabolism then self-monitors and self-regulates behaviour
set point
A comfortable range of body weight that the body tries to “defend” and maintain
90% to 95% of those who lose weight regain it within several years
If fat levels decrease below our body’s typical range, the brain (specifically, the hypothalamus) compensates by ________
slowing metabolism.
the body fights against weight gain by increasing metabolism and raising body temperature in an effort to burn off extra calories
Major hormonal determinants of physical growth rate during childhood are the
growth hormone (GH) and thyroid hormone
Additional gonadal steroids kick in during adolescence to produce a further growth spurt and skeletal maturation
_______ of growth hormone production occurs after the onset of deep sleep (may explain why eating and sleep disorders coexist in some younger children)
50% to 75%
childhood obesity
a chronic medical condition characterized by an excessive accumulation of body fat relative to gender- and age-based norms.
Approximately _____ children and adolescents in the US are obese
1 in 5
_____ hormone carries instructions to the brain to regulate energy and appetite
Leptin
(Leptin deficiencies have been found with severe obesity)
Treatment for obesity
Prevention or intervention of childhood obesity involves the individual’s health and family resources
Restricting diets are not usually recommended
Treatment should:
Address the parents’ knowledge of nutrition
Increase the child’s physical activity
Should instill active, less sedentary routines for both parents and child
Avoidant/restrictive food intake disorder (ARFID)
Characterized by a sudden or marked deceleration of weight gain and a slowing or disruption of emotional and social development prior to age 6
At least one of the following characteristics must be present:
significant weight loss
significant nutritional deficiency
dependence on enteral feeding (feeding tube) or oral nutritional supplements
marked interference with psychosocial functioning
With ARFID, some manifest by avoiding or restricting food based on __________
sensory characteristics
The cause of ARFID is …
multifactorial: biological, medical, psychological, and environmental factors—and their interaction.
history of vomiting, food allergies, gastrointestinal difficulties, low interest in feeding, family eating environments, accessibility and exposure to healthy, varied food items
Fear of eating-related issues such as choking and low appetite
ARFID is highly comorbid with
autism spectrum disorder - 21%
For treatment, a Manualized version of __________ adapted for use with ARFID patients
family-based treatment (FBT)
Focus on eating behaviors such as increasing variety, using psychoeducation, and rewards-based behavioral therapy
PICA
The ingestion of inedible substances, such as hair, insects, and chips of paint, for a period of at least 1 month
Prevalence of PICA?
One of the more common (12%) and usually less serious eating disorders
Affects mostly young children and adults with intellectual disabilities
More prevalent among institutionalized children and adults
Causes of PICA?
Specific causes not isolated, usually appearing within first 2 years
Often without adequate stimulation or supervision
Suspected vitamin or mineral deficiency
No evidence of genetic factors
Treatment for PICA?
Treatments are based on operant conditioning procedures and teaching caregivers to keep the child’s environment tidy and removing dangerous substances
Anorexia Nervosa
Individual purposely takes in too little nourishment, resulting in body weight that is very low and below that of other people of similar age and gender
Individual is very fearful of gaining weight, or repeatedly seeks to prevent weight gain despite low body weight
Individual has a distorted body perception, places inappropriate emphasis on weight or shape in judgments of herself or himself, or fails to appreciate the serious implications of her or his low weight
Anorexia - Restricting type
During the past 3 months, the individual has not engaged in recurrent episodes of binge eating or purging behavior (i.e., self-induced vomiting or the misuse of laxatives, diuretics, or enemas). This subtype describes presentations in which weight loss is accomplished primarily through dieting, fasting, and/or excessive exercise.
Anorexia - binge eating/purging type
During the past 3 months, the individual has engaged in recurrent episodes of binge eating or purging behavior (i.e., self-induced vomiting or the misuse of laxatives, diuretics, or enemas).
Persons with anorexia are ______ below average weight
15% or more
Prevalence of anorexia is ~____ of adolescents
0.3%
Bulimia Nervosa
(A) Recurrent episodes of binge eating. (large, without control)
(B)Recurrent inappropriate compensatory behavior in order to prevent weight gain (vomiting; laxatives, diuretics or enemas, or other medications; fasting; or excessive exercise.)
(C)both occur, on average, at least once a week for 3 months.
(D)Self-evaluation is unduly influenced by body shape and weight.
(E)The disturbance does not occur exclusively during episodes of anorexia nervosa.
Prevalence of bulimia is ___ of adolescents
~1%
Persons with bulimia are within ____ of average body weight
10%
Binge eating disorder
(A) Recurrent episodes of binge eating (large, without control)
(B)The binge eating episodes are associated with three (or more) of the following:
Eating much more rapidly than normal
until feeling uncomfortably full
Eating large amounts of food when not feeling physically hungry
Eating alone because of feeling embarrassed by how much one is eating
Feeling disgusted with oneself, depressed, or very guilty afterward.
(C)Marked distress regarding binge eating is present.
(D)The binge eating occurs, on average, at least once a week for 3 months.
Prevalence of binge eating disorder is ____ of adolescents
~1.5-3%
Bulimia and BED seems to be a
culture-bound syndrome, with dominance in western region ideals
Anorexia is seen
across the world, but manifests differently.
Subtypes may be different, and unable to detect using western diagnostics.
Onset of anorexia is usually between ages
14 and 18
Rate of mortality for anorexia is _______
significant (5%)
Of survivors: fewer than one-half show full recovery, one-third show fair improvement, one-fifth continue on a chronic course
fluctuating pattern that involves a restoration of typical weight followed by relapse
Single best predictor or risk for developing an eating disorder is _________
being an adolescent female
Biology may contribute to the
maintenance (not cause) of the disorder in their effects on appetite, mood, perception, and energy.
It has been suggested that imbalances of ______, which regulates hunger and appetite, may be implicated
serotonin
Causes and risks of eating disorders
Western culture self-worth, happiness, and success are determined primarily by physical appearance
Teenage girls: weight loss and being skinny are more important than many other issues
Mass media influences perceptions of body dissatisfaction
Consider stress factors, including family factors, struggle for autonomy/control
Psychosocial treatments for eating disorders generally include
Family therapy and individual therapy
Cognitive–behavioral therapy and interpersonal psychotherapy,
Cognitive training and dialectical behavioral therapy
More recently, virtual or telehealth-based practices
Family based treatment (FBT) based on five principles
The clinician holds an agnostic view of the cause of the illness
The clinician takes a non-authoritarian stance in treatment
Parents are empowered to bring about the recovery of their child
The eating disorder is separated from the patient and externalized
FBT utilizes a pragmatic approach to treatment with the focus on the present moment