Upper Respiratory Disorders
1/70
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
71 Terms
What is the primary definition of epiglottitis?
Acute inflammation of the epiglottis and surrounding supraglottic structures leading to rapid airway obstruction.
What is the most common cause of epiglottitis in children?
Haemophilus influenzae type b (Hib).
What is the critical danger of performing a direct throat exam on a patient with suspected epiglottitis?
It can trigger laryngospasm, leading to complete airway obstruction.
How does the onset of epiglottitis compare to croup?
Epiglottitis has a rapid onset (hours), whereas croup develops gradually over 1-2 days.
What are the hallmark signs of epiglottitis?
Rapid onset, high fever, severe sore throat, drooling, muffled 'hot potato' voice, and inspiratory stridor.
What is the 'tripod position' in the context of epiglottitis?
Sitting upright, leaning forward on outstretched arms, chin thrust forward, and mouth open to maximize airway.
What are the 'four D's' associated with epiglottitis?
Dysphagia, Drooling, Dysphonia, and Distress.
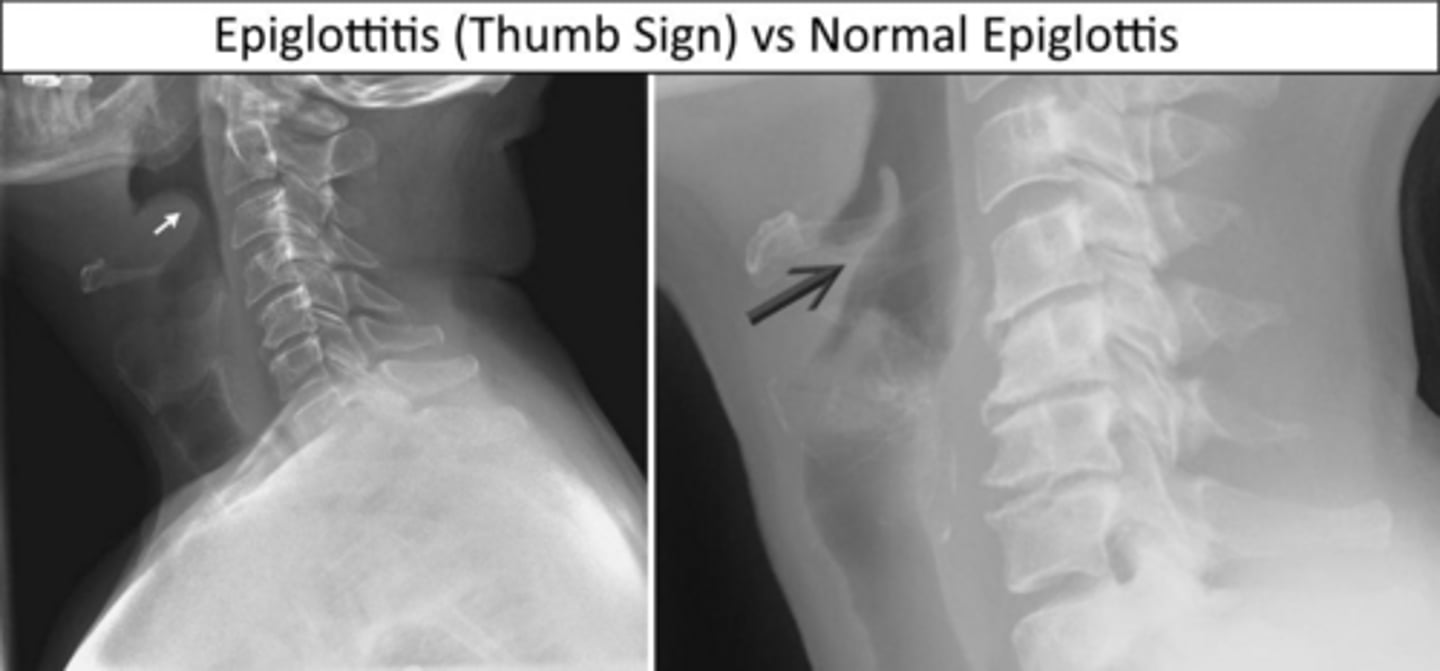
What radiographic finding is characteristic of epiglottitis?
The 'thumb sign' on a lateral neck X-ray, indicating a swollen epiglottis.
What is the number one priority in the management of epiglottitis?
Airway management.
Why should a patient with epiglottitis be kept calm?
Agitation and crying increase oxygen demand and can worsen airway obstruction.
What is the primary nursing diagnosis for a patient with epiglottitis?
Ineffective Airway Clearance related to supraglottic edema.
What is the purpose of the Hib vaccine?
It prevents most pediatric cases of epiglottitis caused by Haemophilus influenzae type b.
Which radiographic finding distinguishes croup from epiglottitis?
The 'steeple sign' on an AP neck X-ray, indicating a narrowed subglottic space.
What is the definition of croup?
Inflammation of the larynx, trachea, and bronchi (subglottic region) causing a narrowed airway below the vocal cords.
What is the typical age range for croup?
3 months to 3 years, with a peak incidence around 2 years.
What is the most common etiology of croup?
Viral infections, most commonly parainfluenza viruses.
What is the classic triad of symptoms for croup?
Barking 'seal-like' cough, inspiratory stridor, and hoarseness.
How does the fever in croup compare to the fever in epiglottitis?
Croup typically presents with a low-grade fever, whereas epiglottitis presents with a high fever.
Why is it important to allow a child with epiglottitis to be held by a parent?
It reduces agitation and helps protect the airway.
What should be kept at the bedside for a patient with epiglottitis?
Intubation tray and tracheostomy kit.
What is the primary difference in clinical appearance between a patient with croup and one with epiglottitis?
A patient with epiglottitis appears toxic, whereas a patient with croup is generally not toxic-appearing.
What is the standard pharmacological treatment for epiglottitis once the airway is secured?
IV antibiotics (such as ceftriaxone or ampicillin-sulbactam) and IV corticosteroids.
Why is adult epiglottitis often missed?
The larger airway diameter in adults buys time, creating false reassurance despite the potential for progression to complete obstruction.
What is the most distinctive clinical finding of croup?
A barking, seal-like cough.
What radiographic finding is associated with croup?
The 'steeple sign' on an AP neck X-ray, indicating subglottic airway narrowing.
What is the primary nursing intervention for mild croup at home?
Cool mist humidifier or exposure to cool night air, along with keeping the child calm and hydrated.
Why must a patient be observed for 2-4 hours after receiving nebulized racemic epinephrine?
To monitor for rebound worsening of symptoms.
What is the main pharmacological treatment for moderate to severe croup?
Dexamethasone (a corticosteroid) to reduce subglottic edema.
What are the key clinical differences between croup and epiglottitis?
Croup: gradual onset, barking cough, no drooling. Epiglottitis: sudden onset, high fever, drooling, toxic appearance.
What radiographic finding is associated with epiglottitis?
The 'thumb sign' on a lateral neck X-ray, indicating a swollen epiglottis.
Which influenza virus type is the most prevalent and severe?
Type A.
What is the difference between antigenic drift and antigenic shift in influenza?
Antigenic drift involves small, gradual mutations; antigenic shift involves major genetic reassortment that can lead to pandemics.
What are the hallmark symptoms of influenza?
Sudden onset of high fever, severe myalgia, marked fatigue, headache, dry cough, and sore throat.
What is the leading cause of flu-related deaths?
Secondary bacterial pneumonia.
What is the clinical pattern of secondary bacterial pneumonia following influenza?
Initial improvement followed by a worsening condition with a new fever and productive cough.
What is the time window for starting Oseltamivir (Tamiflu) to be effective?
Within 48 hours of symptom onset.
What type of isolation precautions are required for influenza?
Droplet precautions (surgical mask).
Why is aspirin contraindicated in children with viral illnesses like influenza?
It carries a risk of Reye syndrome (hepatic encephalopathy).
Which influenza antiviral should be avoided in patients with asthma or COPD?
Zanamivir (Relenza), as it may trigger bronchospasm.
What is the recommendation for the flu vaccine during pregnancy?
The inactivated flu vaccine is recommended in all trimesters.
Which flu vaccine formulation is contraindicated in pregnant women and immunocompromised patients?
The live attenuated nasal spray (FluMist).
When can a patient with influenza be removed from isolation?
When they have been afebrile for at least 24 hours.
Are antibiotics indicated for the treatment of croup?
No, because croup is viral.
What is the primary difference in onset between the flu and the common cold?
Flu has a sudden onset; the common cold has a gradual onset.
What are the signs of severe croup that require emergency care?
Stridor at rest, significant retractions, cyanosis, or decreased level of consciousness.
What is the causative agent of strep pharyngitis?
Group A β-hemolytic Streptococcus.
What is the primary pathogen associated with bacterial pharyngitis?
Group A Streptococcus (GAS) or Streptococcus pyogenes
What clinical findings help differentiate bacterial pharyngitis from viral pharyngitis?
Absence of cough, rhinorrhea, and hoarseness
What is the gold standard diagnostic test for streptococcal pharyngitis?
Throat culture
What is the primary nursing priority for a patient diagnosed with strep pharyngitis?
Ensuring the patient completes the full 10-day antibiotic course to prevent rheumatic fever
What are the three major complications of untreated Group A Streptococcus infection?
Rheumatic fever, post-streptococcal glomerulonephritis, and peritonsillar abscess
How is Scarlet Fever clinically distinguished from standard strep pharyngitis?
The presence of an erythrogenic toxin-mediated sandpaper rash
What are the hallmark physical signs of Scarlet Fever?
Sandpaper rash, strawberry tongue, and circumoral pallor
When is a patient with strep pharyngitis no longer considered contagious?
After 24 hours of appropriate antibiotic therapy
What are the signs of a peritonsillar abscess?
Unilateral throat swelling, trismus, 'hot potato' voice, and uvular deviation
What is the primary mechanism of Obstructive Sleep Apnea (OSA)?
Pharyngeal soft tissue collapse during sleep causing repeated airway obstruction
What is the strongest modifiable risk factor for OSA?
Obesity
What is the gold standard diagnostic tool for OSA?
Polysomnography (sleep study)
What does the Apnea-Hypopnea Index (AHI) measure?
The number of apnea or hypopnea events per hour of sleep
What is the first-line treatment for OSA?
Continuous Positive Airway Pressure (CPAP) therapy
Why is CPAP adherence considered a critical nursing priority?
It is the most common barrier to effective treatment and prevents airway collapse during sleep
What is the primary perioperative risk for patients with OSA?
Increased risk of airway obstruction due to sedation and supine positioning
What tool is used to screen surgical patients for OSA?
STOP-BANG questionnaire
What is a common cause of OSA specifically in children?
Enlarged tonsils or adenoids
What systemic complication can arise from chronic hypoxemia in untreated OSA?
Secondary polycythemia (increased RBC production)
What is the clinical significance of Pastia's lines in Scarlet Fever?
Linear petechiae found in skin folds
How does the timing of Rheumatic Fever differ from Post-strep Glomerulonephritis (PSGN)?
Rheumatic fever occurs 2-4 weeks later; PSGN occurs 1-3 weeks later
What is the recommended nursing action if a rapid strep test is negative but clinical suspicion is high?
Confirm the diagnosis with a throat culture
What are the hallmark daytime symptoms of OSA?
Excessive daytime sleepiness, morning headaches, and difficulty concentrating
What lifestyle modification can significantly improve the AHI in OSA patients?
Weight loss
What is the purpose of the humidifier attachment on a CPAP machine?
To reduce nasal dryness