Chapter 24 Water & Electrolytes Outline
1/41
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
42 Terms
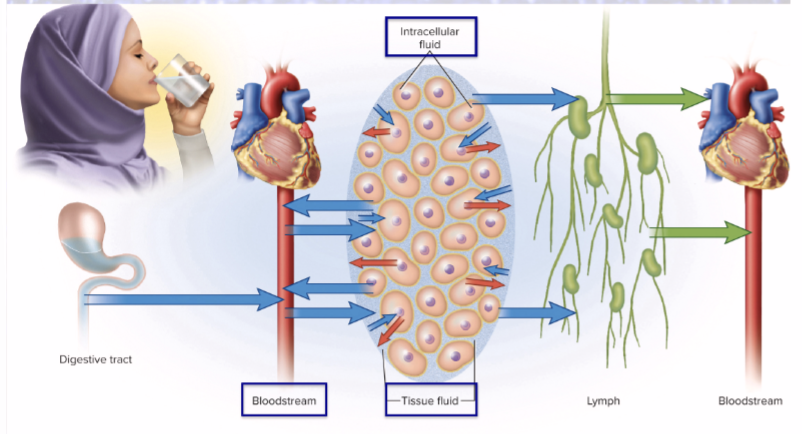
How much fluid is intracellular fluid?
65% (most)
How much fluid is extracellular fluid?
35%
25% tissue fluid
8% blood plasma & lymphatic fluid
2% transcellular fluid (cerebrospinal, synovial, pericardial)
Electrolytes
(salt) help govern water distribution and total water content
osmosis restores balance
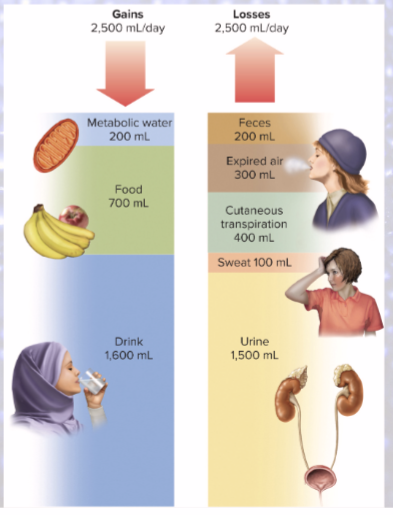
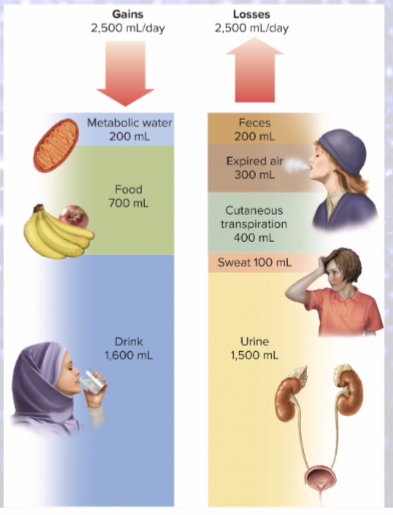
fluid balance: gains = losses
2,500 mL/day
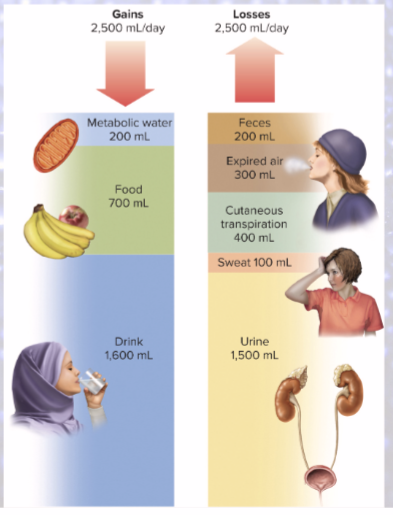
Water is gained from what 2 sources?
preformed water (2,300 mL/day)
food and drink
metabolic water (200 mL/day)
from aerobic metabolism & dehydration synthesis
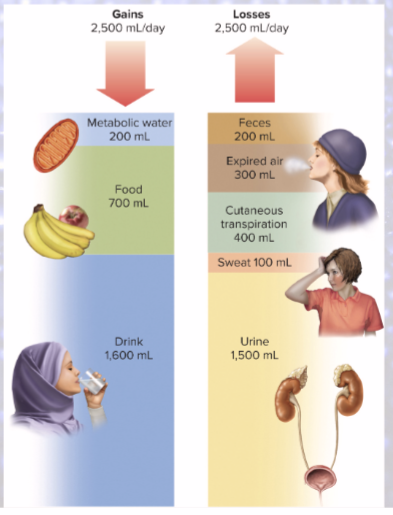
Sensible water loss
(observable)
1,500 mL/day in urine
200 mL/day in feces
100 mL/day in sweat
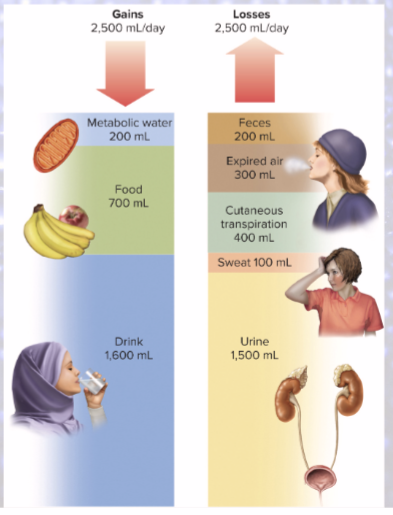
Insensible water loss
(unnoticed)
300 mL/day in BREATH
400 mL/day in CUTANEOUS TRANSPIRATION
Obligatory water loss
Sensible (urine, feces, sweat) and insensible (breath, cutaneous transpiration) water loss combined
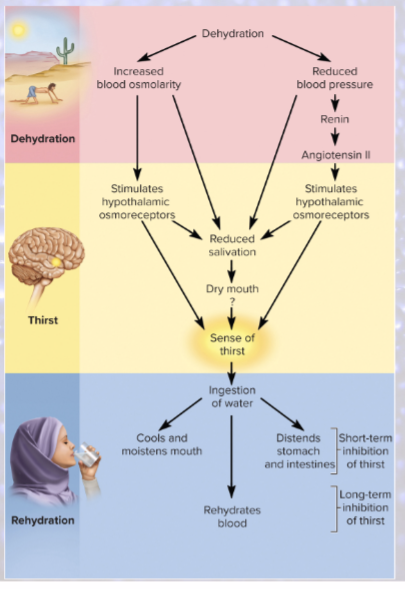
What mechanism triggers thirst in response to dehydration?
osmoreceptors detecting increased plasma osmolarity
(angiotensin II is produced when BP drops)
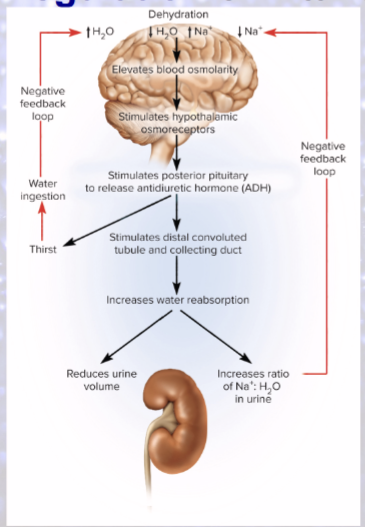
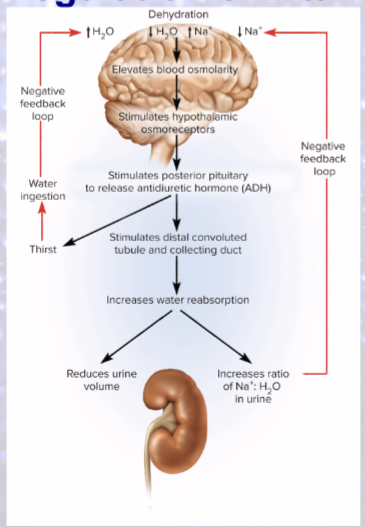
Dehydration
decreases blood volume and BP
increases blood osmolarity
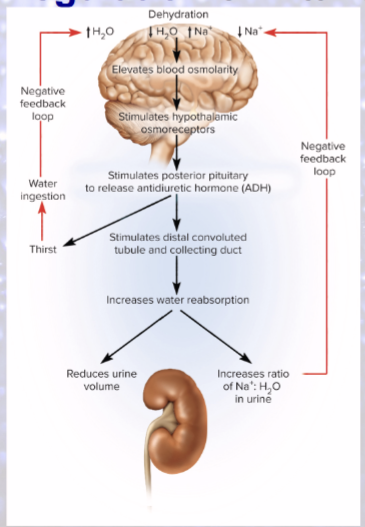
Hypothalamus produces what in response to dehydration?
ADH!
salivation inhibited (sympathetic)
Cerebral cortex role in dehydration?
makes us “feel” thirsty
intense sense of thirst if only 2-3% increase in plasma osmolarity
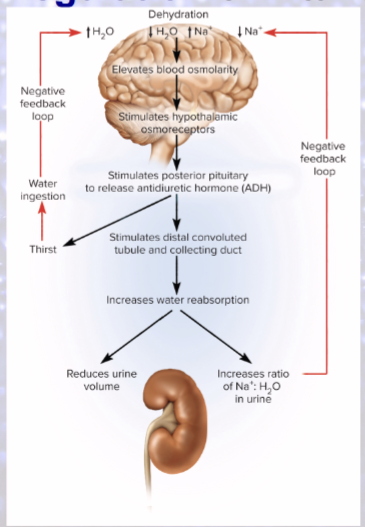
1.) Which hormone increases water reabsorption without altering sodium reabsorption?
ADH
Long-term inhibition of thirst
absorption of water from small intestine reduces blood osmolarity
stops osmoreceptors
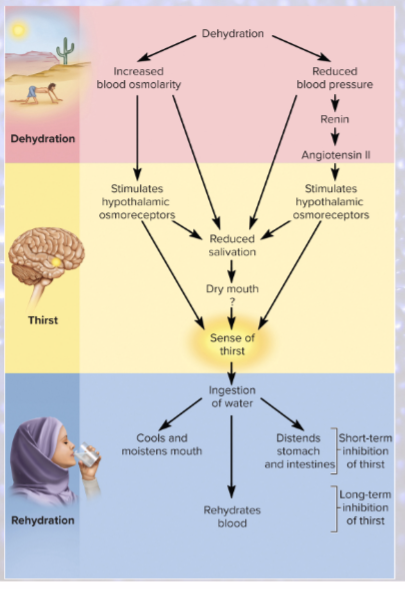
Short-term inhibition of thirst
cooling/moistening of mouth
distension of stomach and small intestine
DESIGNED TO PREVENT OVERDRINKING
variation in urine volume =
significant control of water output (kidneys can only slow rate of loss)
changes in urine volume linked to adjustments in sodium reabsorption
as sodium reabsorbed or excreted, water follows
can concentrate urine with ADH, independently of sodium
in CDs, water reabsorbed but sodium still excreted
volume
both sodium and water lost/retained
concentration
more water than sodium lost/retained
fluid deficiency examples
hypovolemia (volume) or dehydration (concentration)
fluid excess examples
volume excess or hypotonic hydration (concentration)
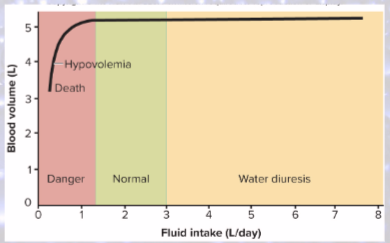
hypovolemia
sodium and water decreased (volume); osmolarity CONSTANT
ex: hemorrhage, severe burns, chronic vomiting/diarrhea
dehydration
body loses significantly MORE water than sodium
osmolarity RISES (concentration)
ex: diabetes mellitus, diabetes insipidus, profuse sweating, diuretics
who are most vulnerable to dehydration?
INFANTS
high metabolic rate, greater body surface-to-mass ratio, immature kidneys cannot concentrate urine effectively
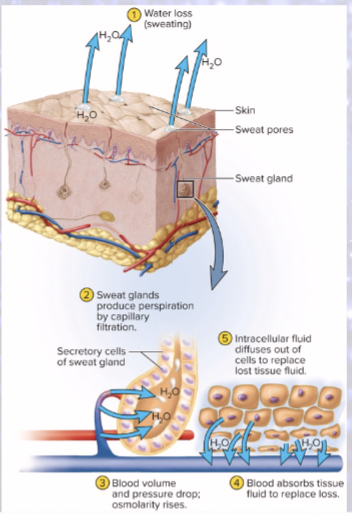
dehydration from excessive sweating
sweat from capillaries
blood volume and BP drop, osmolarity rises
blood absorbs tissue fluid to replace loss!
tissue fluid pulled from ICF
all 3 compartments lose water
fluid excess
kidneys so effective at excreting more urine to compensate for excess intake
renal failure can therefore cause fluid retention
volume excess
both sodium and water retained
ECF isotonic (volume)
cause: aldosterone hypersecretion or renal failure
Hypotonic hydration
more water than sodium retained/ ingested
ECF becomes hypotonic (concentration)
cause: overdrinking water or ADH hypersecretion
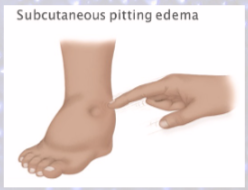
Fluid sequestration
excess fluid accumulates in particular location
EDEMA (abnormal accumulation of interstitial (in-between cells) fluid)
Hemorrhage
blood can pool in tissues during fluid sequestration (excess fluid)
Effusion
fluid in cavity (ex: pleural) during fluid sequestration (excess fluid)
Physiological functions of electrolytes
many metabolic processes
determine electrical potential across cell membranes
affect osmolarity of body fluids, therefore water content
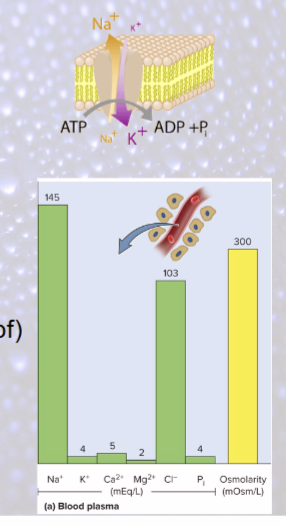
sodium functions
critical ion for RMPs, APs (Na+—K+ pump)
principal cation in ECF
90-95% osmolarity of ECF
most significant solute in determining total body water
How much sodium do we need each day and how much does the American diet have?
need= 0.5 grams of sodium/day
get= 3-7 a day
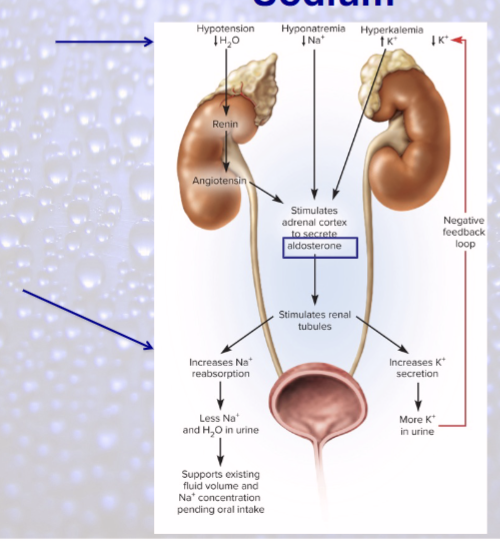
Aldosterone
“salt-retaining hormone”
secreted in response to hyponatremia and hypotension (low BP)
if hypotension, via renin—angiotensin—aldosterone mechanism
Natriuretic peptides (ANP)
inhibit sodium and water reabsorption
Hypernatremia
high concentration of sodium
consequences: hypertension, edema
Hyponatremia
low concentration of sodium
drinking too much plain water after profuse sweating
quickly corrected by excretion of excess water
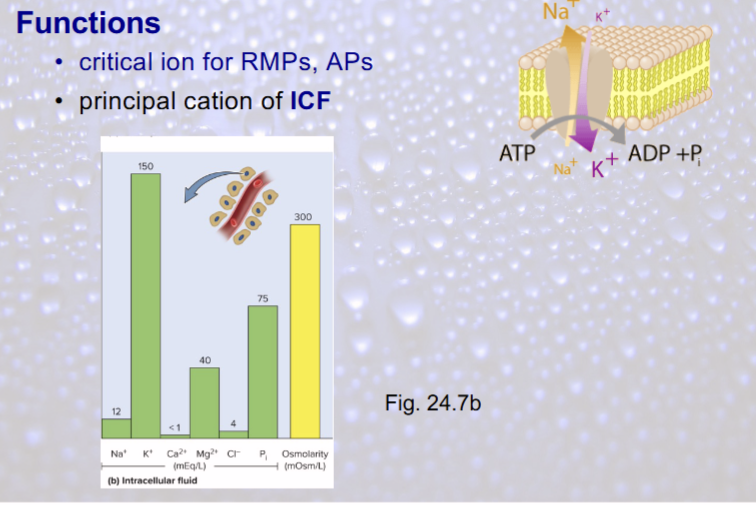
Potassium functions
critical ion for RMPs, APs
principal cation of ICF
Potassium homeostasis closely linked to that of sodium
most potassium reabsorbed by PCT
DCT and collecting duct secrete potassium in response to blood levels, mediated by aldosterone

Most dangerous imbalances
hyperkalemia and hypokalemia (potassium)
Hyperkalemia
if extracellular potassium rises quickly (injury), makes nerve and muscle cells more excitable
if rises slowly (renal failure), nerve & muscle cells become less excitable
Hypokalemia
from sweating, chronic vomiting, or diarrhea
neurons and muscle cells hyperpolarized, less excitable