Mam Phys Exam 3: Pulmonary
1/61
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
62 Terms
What does the respiratory system do
Clears air of pathogens and diseases
Exchange O2 and CO2
Adjust blood pH
Vocalization
What is a challenge that the respiratory system faces
It is a significant source or heat and water loss
Why did internal lungs evolve
The surface area must be moist to allow gases to move from the air to the blood. Internal lungs allow for a constant humid environment that prevents drying out.
How do the lungs move air in and out of the body?
The lungs use a pressure differential. Air flows from areas of high pressure to low pressure.
When the diaphragm contracts and shrinks, the lungs expand. This creates negative pressure inside the lungs, causing air to rush in to equalize the pressure difference.
Resistance to flow
1/r^4 determines resistance to flow.
The bronchioles are the main source of resistance and can be controlled
Smooth muscle on the bronchioles can dilate due to SNS activation (Epinephrine)
Compliance = deltaV/deltaP
Requirements for Air entering the body
Air must be warm, clean and moist
How does the body achieve the 3 requirements for entering air
Warm: The airway is “long” giving the air enough time to be warmed by the body’s heat
Moist: The mucus lining the airways evaporate and moisten the air (This is why breathing through your nose is better at moistening and heating the air than your mouth)
Filtering: Cillia in the airway are covered in watery saline that traps and kills incoming bacteria and viruses.
How is the saline layer maintained/created
Cl- is transported out of the epithelial cells using the CFTR apical channel and is transported down its ion gradient.
Na+ is actively kept in high concentrations in the ECF using a K+ Na+ antiporter. Na+ passively diffuses out of the ECF into the airway
The high salt concentration causes water to flow into the lumen.
Mechanism of filtering
The mucus traps the dirt/bacteria and the cillia move the mucus up towards the mouth/pharynx.
The dirt is then spit out or swallowed (destroyed by stomach enzymes)
How does cystic fibrosis work
The CFTR channel is defective or not working which causes less Cl- to be pumped into the airway.
This decrease in ion concentration causes less fluid to move into the airway which causes the mucus to become thick and traps cillia
The trapped cillia can no longer push debris upwards which cause bacteria to grow in the lungs
Alveoli
Site of gas exchange
Similar to capillaries the alveoli have a massive SA compared to the rest of the airway which means that air moves the slowest to facilitate gas exchange
Type I Alveoli
Make up 95% of the alveolar surface
These are extremely thin cells which allows gas to rapidly flow through them
A basement membrane physically fuses the capillary and alveoli together so that gas exchange is even faster (barely any interstitial fluid between the two)
Type II Alveoli
Create a chemical known as surfactant.
Surfactant allows the alveoli to expand during breathing
These cells also regulate the amount of fluid in the alveoli by actively pumping ions out of the sac (water follows)
Pressure and Flow through the lungs
The pulmonary circuit contains .5 Liters or 10% of the blood volume
The circuit receives the entire volume of the right ventricle (5L/min)
Despite this pulmonary artery pressure is only 25/8 mmHg. This is because there is not much resistance in the pulmonary circuit due to shorter vessels and larger surface area. Right ventricle does not contract as hard.
What does the low pulmonary BP mean for hydrostatic force?
The hydrostatic force is low in the lungs which causes less fluid to be filtered out into the interstitial space. The little fluid that is filtered is easily removed by the lymphatic system.
How do the lungs expand and contract
The diaphragm contracts and the ribs push outwards —> Low pressure in lungs which causes air to enter.
High pressure from diaphragm relaxation and rib internal pressure causes the air to leave the lungs.
The lungs “deflate” due to elastic recoil which is a feature due to elastin and collagen that allows them to stretch.
Surroundings of lung
The lungs are surrounded by the pleural sac which allows the lungs to slide against the chest wall during breathing.
Intrapleural pressure
The lungs naturally want to deflate due to elastic recoil (alveoli are at 0 mmHg )
The chest wall naturally wants to expand due to its own elastic recoil (4 mmHg)
The intrapleural pressure is -4 mmHg relative to the atm (This causes the chest wall to push inwards and the lungs to push outwards. This balances the two forces and maintains equilibrium)
Decreases during inspiration as opposing forces increase the volume. However it remains attached to both the lungs and chest wall because of surface tension.
Alveolar pressure
Anytime Palv is less than 0 (relative to atmosphere) air flows into the lungs.
When Palv is greater than 0 air flows out of the lungs
Tidal volume
The volume of air that moves during a single normal inspiration or expiration. The avg tidal volume is about 500 mL
Inspiratory reserve volume
If you inhale as hard as you can, the volume above your normal tidal volume is your IRV.
IRV is usually 6x greater than tidal volume
Expiratory reserve volume
the amount of air exhaled after a normal exhale is your ERV.
Usually about 1100 mL
Residual volume
Even if you try to exhale or blow out all of your lungs some will always remain in your airway.
This volume exists because the lungs are attached to the ribs by the pleural membrane which keeps them partially inflated at all times.
Dead space volume
Volume in the upper airways
This air does not reach the alveoli and undergo gas exchange.
Alveolar ventilation = RR * (Tidal volume - DSV)
Vital Capacity of Lung
The sum of IRV + ERV + Tidal Volume
Total Lung Capactity
VC + Residual Volume
Mechanism of Surfactant
There is naturally a thin layer of fluid/water between the alveoli and the air to facilitate gas exchange.
This water-air interaction creates surface tension that increases in strength as the curvature of a surface increases (in the alveoli as they expand) (There is almost a bubble of water)
Surfactant decreases surface tension by replacing water molecules at the surface (amphipathic phospholipids)
According to Law of LaPlace, this inward force is greatest in small alveoli and surfactant helps prevent collapse by reducing the overall inward force.
Law of LaPlace
Pbubble = 2 * surface tension / radius
The pressure points inwards to prevent the bubble from expanding
Respiratory distress syndrome in babies
Surfactant is not yet produced
Alveoli collapse under inward force from surface tension.
Leads to death
Solution: Stimulate surfactant production using glucocorticoid or synthetic surfactant
Importance of Compliance
Compliance = deltaV/deltaP
Essentially how much force needed to expand a lung
Both higher and lower compliance can be bad.
High compliance (Emphysema) : Destruction of elastin reduces elastic recoil of lungs, allows them to inflate more at the cost of not fully relaxing/deflating. Leads to less airflow overall and breathing difficulty
Low Compliance (fibrosis): Lung scarring makes it harder for lung to inflate, decreasing overall airflow and leads to breathing difficulty
Histamine
A powerful bronchoconstrictor produced by Mast Cells during an immune response
Severe allergic reactions can lead to widespread bronchoconstriction which can stop breathing
Innervation of bronchioles
Controlled entirely by the PNS.
Can be controlled endocrinely through epinephrine binding to B2 receptors to cause bronchodilation
FEV1
Forced Exhalation Volume in 1 Second
What determined the concentration gradient for gases
1) Gas exchange in the alveoli (Po2 decreases and Pco2 increases relative to atm)
2) Mixing of atm air with air in the dead space
3) Saturation of alveolar air with water vapor
Henrys law
Concentration = solubility * partial pressure
Because of this, the gas moves according to its partial pressure rather than its concentration
Air is more concentrated than water but both have the same P02 which means they are at equilibrium
(O2 is less soluble in water)
(CO2 is soluble in water and dissociates into H+ and HCO3-)
Gas exchange
Final arterial gas pressure matches that of the alveolar air
Gas is equilibrated extremely quickly (takes only a quarter of the capillary)
IF alveolar air gas partial pressures change, the blood gas will also change
Relationship between alveolar ventilation and partial pressures
As alveolar ventilation increases, the pressure of oxygen increases while the pressure of CO2 decreases.
Yet normal ventilation is only 4 L/M why not increase ventilation?
As CO2 decreases, the amount of carbonic acid decreases which leads to an increase in blood pH
Also increase reaches plateau so wasted effort
Hemoglobin
95% of O2 carried by RBC’s.
O2 binds to a Heme molecule (Hemoglobin carries heme)
Heme has a Fe+3 ion which is what binds to the oxygen
Hemoglobin has 4 subunits, each containing one heme molecule
how does spO2 work
At around 700-800 nm wavelength Hb and Hb-Oxy absorb light differently
Shining this wavelength through your finger you can tell how much heme is bound O2 and how much isnt.
Carbon monoxide
Competitive agonist for heme because it binds stronger than oxygen to heme.
Blocks any more O2 from binding and can lead to you dying
Shows up on spO2
Globin proteins
a, b y subunits
Adult hemoglobin (2a 2b)
Fetal hemoglobin (2a 2y)
Fetal subunits bind stronger to O2 than adult. This is due to babies not having working lungs which forces them to steal O2 from the mother.
Myoglobin: Muscles store their own heme/oxygen
CO2 transport
1) Diffuse into bloodstream from systemic tissues (limited by solubility 7%)
2) Binding to Hemoglobin(NOT HEME) (23%)
3) Carbonic anhydrase converts CO2 to HCO3. HCO3 is transported into the bloodstream by a HCO3 Cl- antiport (75%)
When reaching the alveoli, the PCo2 is significantly less in the alveoli. Dissolved CO2 diffuses into the alveoli. This drop in PCO2 causes the reverse reaction of CA to be favored, converting HCO3 into CO2 which is then also diffused out.
Why is having bicarbonate in the bloodstream good
HCO3 can act as a buffered system.
Resists changes to pH from things such as lactic acid and other chemicals
How does O2 detach from heme
When Po2 decreases the binding affinity of O2 to heme decreases
Increased temp, CO2, 2,3 DPG and decreased pH decrease the binding affinity of O2
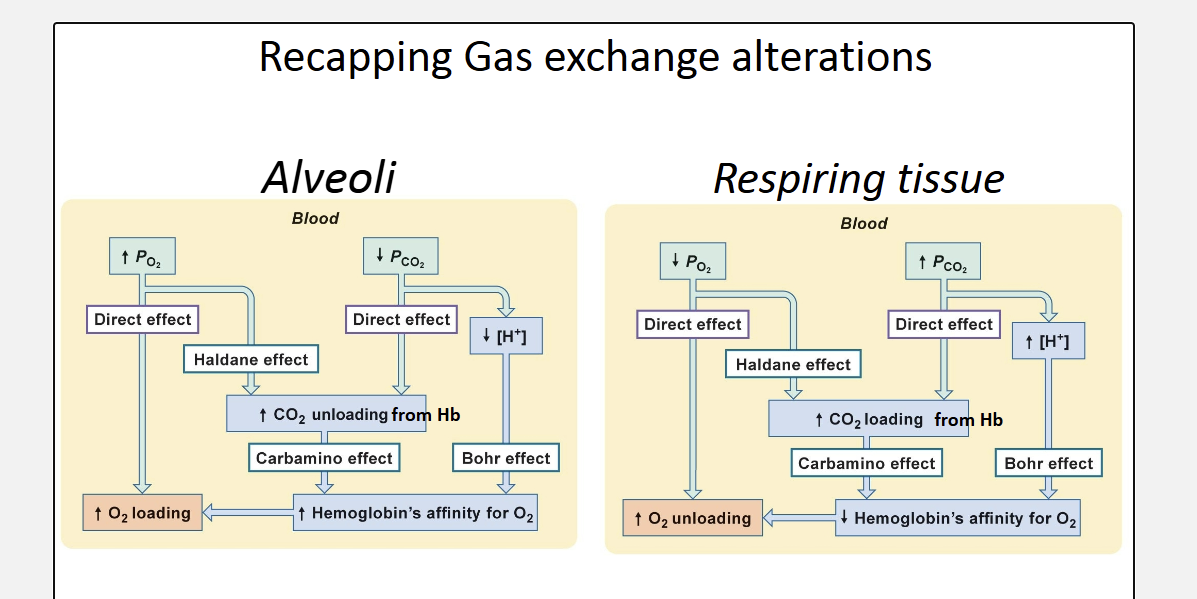
In metabolic tissues/tissues that need O2, the products of respiration help decrease the affinity of O2 which allows for O2 release into the tissues.
Carbamino effect
CO2 binds to the amino terminus groups of hemoglobin
This causes a conformational change in the protein which decreases the affinity for O2
PCO2 in tissues is high due to metabolism which allows for better O2 unloading
Bohr effect
CO2 + H20 leads to H+ and HCO3
This decrease in pH around tissues leads to a decrease in O2 affinity to heme which allows for better unloading.
2,3 Diphosphoglycerate
RBS do not have nucleus or mitochondria and rely on glycolysis for ATP
Produce this molecule in hypoxic conditions
Binds to hemoglobin and prevents reloading of O2 and allows for better unloading of O2.
SYSTEMIC adaptation to hypoxia
Haldane Effect
Oxygenation decreases CO2 capacity
As blood is oxygenated in the lungs, the influx of O2 binds to Heme, decreasing the binding affinity for CO2 which allows for CO2 unloading in the lungs
Perfusion and vasoconstriction
Paracrine regulation can cause vasoconstriction
In the pulmonary system: Increase in CO2 → increase in H2CO3- —→ pH increase —→ vasoconstriction around alveoli that are underventilated
This diverts blood to alveoli that are actually ventilated so that blood is not “wasted:”
Perfusion matches ventilation
What happens if there is a blockage in an capillary
Reduced blooflow to an alveolus leads to bronchoconstriction to divert air to alveoli with better perfusion
Regional differences across the lung
The pressure at the top of the lung is larger, leading to bigger alveoli.
High alveolar pressure in the top of the lung can compress arteries (which already have low pressure)
Neural control of respiration
PRG
DRG (Dorsal respiratory group): Contain chemoreceptors that detect pH and contain motor neurons that innervate the diaphragm
VRG (Ventral respiratory group): Pre-Buttinger complex is the breathing rhythm generator for unconscious breathing. Contain opioid receptors which when stimulated decrease breathing rate to dangerous levels. q
NTS
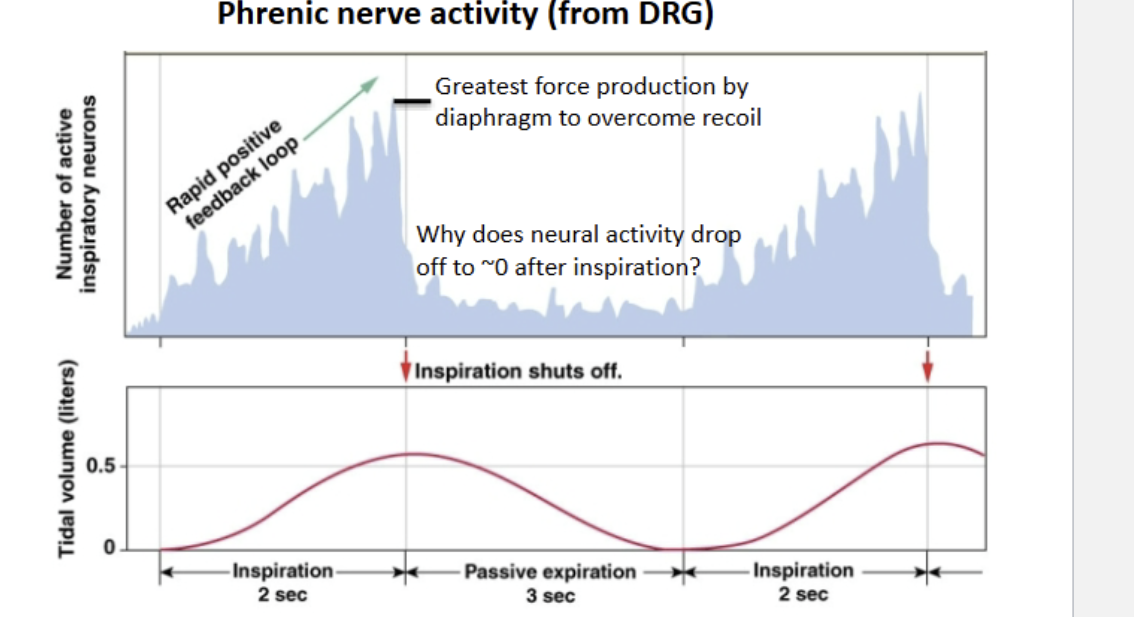
Phrenic nerve activity
The phrenic nerve has rapid positive feedback to build to a stimulus that can overcome elastic recoil in the lungs. This recruits more motor units for a deeper contraction and deeper breath
After peak contraction, MN activation falls to 0 because exhalation is entirely passive
Conscious breathing
Intentional ventilation feeds into regions of the brain that control emotion.
Glomus cells
Found on carotid sinus and aorta (same as baroreceptors)
Sense pH, CO2, O2
When Po2 < 60mmHg, O2 sensing activates (Hypoxic drive)
Usually CO2 and pH are the most used stimulus
End result is calcium induced exocytosis of neurotransmitters onto nerve dendrites
Brainstem chemoreceptors
CO2 can freely diffuse into CSF
This means that the pH of CSF is adjustable according to CO2 levels
Chemoreceptors in the medulla activate and send signals to the ventilation centers.
3 Methods of Breathing control
1) Conscious control —> Limbic system —> Medulla —> Somatic MN’s (Diaphragm, intercostals)
2) CO2 —> Medullary chemoreceptors —- Medulla
3) O2 and pH —→ Carotid and Aortic chemoreceptors — > Afferent Sensory neurons — Medulla
Why does Po2 decrease at higher altitudes
Less total pressure
Humidity stays the same inside you so the decrease in pressure due to water vapor is more evident
Dead space air mixing with higher altitude
What happens to vessels during long term, global lung hypoxia
Normally when an alveolus is under ventilated, local vasoconstriction occurs to divert blood flow.
If EVERY alveoli is under ventilated, ALL of them have vasoconstriction which leads to increased pulmonary pressure
This increases hydrostatic pressure which leads to edema.
The edema increases the distance between the alveoli and capillary which decreases the rate of gas exchange.
What happens to blood pH at high altitudes
It increases
At high altitudes, you are hyperventilating.
This blows off more CO2, decreasing the pH of the blood (respiratory alkalosis)
What happens to breathing rate? Chemoreceptors are less active (they sense low pH) which leads to a decreased breathing rate.
How can a CA inhibitor prevent respiratory alkalosis
It slows the reverse reaction
When CO2 decreases equilibrium pushes the reverse reaction
Without CA this shift takes much longer and can delay the increase in pH