Neuro II Final Study Guide
1/149
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
150 Terms
Be able to create a problem list and associated goals for a patient.
What is a problem list?
Goals need to be what two things? Goals need to be based off of?
Problem list: patient's current and past health concerns that are relevant to their care ➔ It's a living document that's updated as the patient's condition changes.
It's important to keep the problem list accurate, current, and consistent
Problems that are no longer relevant should be removed
Newly diagnosed chronic conditions should be added
Relate to functionality, PLOF, CLOF
SMART goals (Specific, Measurable, Attainable, Realistic, Timely)
goals should be based off the pts limitation list (what are their functional limitations? PLOF compared to CLOF? etc.)
must have functional goals included in goals (goals need to be SMART and functional). Functional goals must:
State time frames (PLOF vs CLOF)
State who
Identify the behavior
Identify the conditions
Identify the degree specifically
Need to be stated in functional terms.
Ex: The patient will ambulate independently with straight cane on level surfaces 100 feet within one week.
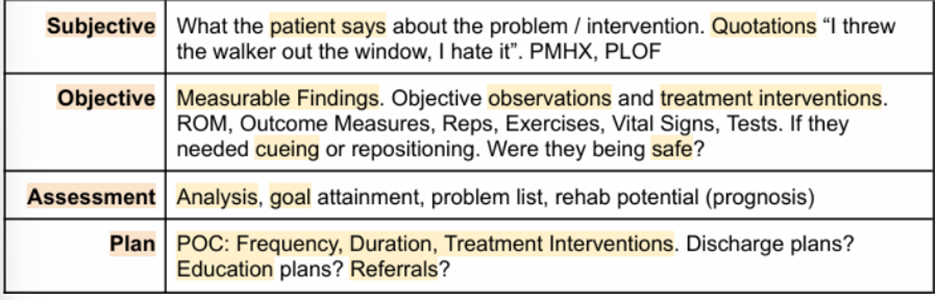
Be familiar with SOAP Notes.
subjective
hx of pt, PMHx, medications (side effects, MOA), PLOF, lifestyle/home, complications, complaints, goals, etc.
past tx or any good/bad experiences from previous PT
objective
hx taken from charts, numerical signs, vital signs, mental status, cognitive perceptual status, inspection of skin/edema, pain scale, cranial nerves, muscle tone, MMT, special tests, functional balance tests, gait, and any other measurements that are appropriate for this pt
assessment
problem list, relation to goals and intervention
LTGs and STGs (SMART):
must have time frames, state who, identify behaviors and conditions and the degree specifically, need to be stated in functional terms
ex. "pt will be able to ambulate independently with a straight cane on level surfaces 100ft within one week
must be pt focused, but may include caregiver/family education
rehab potential (always aim for good/excellent)
plan
frequency, duration, tx interventions, discharge plans, education plans, referrals (OT, SLP, social work, etc.)
Describe the process for obtaining medical marijuana or CBD products in Florida (4 steps).
1) get diagnosed with a qualifying medical condition by a qualified physician
2) be entered into the medical marijuana use registry by their qualified physician
3) apply for a registry identification card (patients and their caregivers)
4) fill your order at a licensed medical marijuana treatment center
What diagnoses or conditions qualify for medical marijuana under Florida law?
cancer
epilepsy
glaucoma
HIV/AIDS
PTSD
amyotrophic lateral sclerosis (ALS)
Crohn's disease
Parkinson's disease
multiple sclerosis (MS)
terminal condition diagnosed by a physician other than their PCP
medical conditions of the same kind or comparable to the others listed
chronic nonmalignant pain caused by a qualifying medical condition, or that originates from a qualifying medical condition, and persists beyond the usual course of the qualifying condition
What are the implications for a physical therapist in relationship to medical marijuana?'
Can we treat if the patient is high? Why or why not? How much should they take so its not an issue?
What does it help with?
You should educate patients on?
Always ask if? What should you be looking out for?
If the patient falls, the might do what? If they have comorbidities or a history of falling, what should you do if needed?
Good for what type of management?
cannot treat if they are high bc they can't give reliable feedback!
if they take as prescribed it should not be an issue (at the appropriate level)
helps with pain management which can optimize rehab time
educate your pts on appropriate use (tell them to listen to their MD)
always ask if they use marijuana (look out for dizziness, loss of balance, cognition, mental status, etc.)
if they fall, they might blame you; if they have comorbidities or have a history of falling, maybe call the MD and adjust the dose if needed
spasticity management
How can medical marijuana or CBD products help a patient?
pain management
What are some potential side effects and adverse reactions related to medical marijuana?
CBD use during _______ is not recommended.
May cause ______ damage.
May interfere with?
What type of side effects would be expected?
Cannabis use disorder?
Negative neurological effects?
Cardiovascular risk?
Respiratory risk?
Physiological issues?
CBD use during pregnancy is not recommended
liver damage
interference with other drugs you are taking (may lead to injury or serious side effects)
Symptoms:
drowsiness or sleepiness-->driving: negatively affects skills required for safe driving
diarrhea or changes in appetite
changes in mood, such as irritability
unintentional poisoning
cannabis use disorder: physical dependency and controlling their use
negative neurological effects (brain health): memory, learning, attention, decision making, coordination, emotions, and reaction time (driving)
cardiovascular risk (heart health): can make the heart beat faster and raise BP
can increase risk of MI and stroke--> importance of health history!
respiratory risk (lung health): smoked cannabis, regardless of how it is smoked, can harm lung tissues and cause scarring and damage to small blood vessels
psychosocial issues (mental health): linked to social anxiety, depression, and schizophrenia
Be able to describe methods of marijuana delivery (6)
pill--> Marinol (FDA approved for N/V)
topicals containing CBD (cannabidiol)
vaping
smoking
sublingual spray
edibles (tea--> instructions on how long to steam)
How do CBD products potentially relate to drug testing? Why are poppy seeds bad before a drug test?
they test for THC, not CBD
make sure what you are taking does not have THC
poppy seed could show up on urine tests as heroin!
What is the structure and function of the peripheral vestibular system?
PVS are your what structures? They are responsible for?
Where do the vestibular labyrinth lie? what movement sensors does it have?
3 primary functions of peripheral vestibular system? How does it do each?
PVS= inner ear structures--> sensory organ responsible for position of body/head; detects motion and proprioception
the vestibular labyrinth lies within the temporal bone on each side of the skull
contains 2 types of movement sensors: semicircular canals and otoliths
3 primary functions of the Peripheral Vestibular System
1) visual clarity: ensuring that clarity is maintained despite changes in head position
stabilization of visual images on the fovea of the retina during head movement to allow clear vision--> achieved through the VOR, which enables the eyes to move in the opposite direction of head motion
2) postural stability: maintaining postural stability, especially during head movement
coordination muscle responses that help the body stay upright and balanced
3) spatial orientation: providing information used for spatial orientation
provides continuous feedback about head position and movement relative to gravity, essential for navigating the environment and adjusting movements
Vestibular Subjective Exam
If pt reports feeling dizzy what should you try to get them to do? Why?
For vertigo, what are the two types and their differences?
What other thing would you looks for during examination?
What can be done to get a numerical/better idea of the patients dizziness?
If pt reports feeling dizzy, try to get them to explain what dizzy means to them; do they feel like their feet are unstable? Is the world spinning? Does it feel like they are spinning?
“dizzy” does NOT tell us much
vertigo: nausea, room is spinning, throwing up (ask duration of s/s)
neuritis: will last days to weeks
BPPV: lasts about 10 minutes (if last weeks= NOT BPPV--> refer out!)
Other things to look out for:
lightheadedness: feeling of passing out, orthostatic hypotension
disequilibrium: losing balance, feeling like pt will fall
oscillopsia: stationary objects appear to move, triggered by darkness because the eye is trying hard to adjust.
duration and circumstances of s/s
What can be used to assess how dizzy:
visual analog scale--> scale 1-10
Dizziness Handicap Inventory
includes physical, functional, and emotional domains
very important because these pts have fear movements leading to anxiety or depression
motion sensitivity quotient
What is the VOR and how is it tested?
What is it mediated by? How?
What is the relationship of eye velocity to head velocity is called? What does it mean? What does saccade mean? Eye position should arrive at?
VOR is tested via what test and a positive finding means?
allows eyes to move at the same velocity but opposite direction as the head
mediated by the SCC: hair cells deflected--> sends info to vestibular nuclei--> sends info to CNS nuclei of eyes
the relationship of eye velocity to head velocity is called the VOR gain
as head moves in one direction, the eyes move in the opposite direction with equal velocity; saccade= difference in velocity where the eyes try to catch up
eye position should arrive at a point in time that is equal with the opposite directed head position
tested via:
head impulse test--> positive findings= saccades
What is the difference between a saccade and nystagmus?
First, what are they both considered?
For saccades: What is it and what is it used for? Not typically caused by what? What happens if someone has corrective saccades?
For nystagmus: What is it and what is is composed of? What direction does the nystagmus move? When observing the eyes for resting nystagmus, what must you remember so the results are accurate and how can this be avoided?
What should you suspect if they don’t respond to treatment or the nystagmus does slow down?
If the nystagmus does slow down what should you suspect?
both are considered involuntary eye movements
saccades:
normal rapid eye movements; used to reposition the eyes on a target of interest
not typically caused by vestibular lesion
corrective saccades (catch up)--> vestibular hypofunction--> vestibular involvement
nystagmus:
eye movement due to a peripheral vestibular lesion
composed by both slow and fast component eye movements
begins to slow down as the otoconia begins to settle (canal issue); if it continues to persist, it could be the cupula (very rare)
the direction of the nystagmus is named by the direction of the fast movement: R side movement= R nystagmus
when observing the eyes for resting nystagmus, remember that the pt may be able to suppress it in the light or if focusing on a target
tell the pt "look at my nose"; have them look beyond you, or do it in darkness
if they don't respond to tx or nystagmus does not slow down= CUPULA involvement
if nystagmus does slow down= crystals are settling= CANNALS are involved
How can a physical therapist differentiate between a central or peripheral vestibular lesion?
CNS: What can cause injury to the CNS? Demyelinating diseases?
Nystagmus?
________ and _____ _____ are indicative of a? What does this mean? When is this an emergency?
An ocular tilt reaction consists of what three things?
What are the red flags of a central lesion? What should you do if suspected? What test would be positive?
CNS
injury to the CNS: CVA, TIA, vertebral artery, vertebrobasilar insufficiency, TBI
demyelinating diseases: MS
nystagmus: pure vertical nystagmus may indicate central lesion
lateropulsion and head tilt are indicative of a central lesion (pusher syndrome): pt tend to fall to one side (in the absence of a substance issue= WHOOP WHOOP!)
an ocular tilt reaction consists of 3 key components:
1) ocular torsion: both eyes rotate (torsion) in the same direction
2) head tilt: the head tilts toward the AFFECTED side
3) skew deviation: one eye moves up while the other moves down
red flags of a central lesion
REFER TO MD!
diplopia that lasts >2 weeks after the onset of a peripheral vestibular loss
persistent pure vertical positional nystagmus (bidirectional, HINTS)
spontaneous up-beating nystagmus
- (+) test for skew deviation (vertical misalignment, HINTS)
What is the HINTS examination?
Worrisome HINTS exam: What are the components and how does it work?
Which patients do you perform the HINTS exam on?
test used to differentiate central (stroke) from peripheral (vestibular neuritis) causes of acute vertigo and nystagmus
Worrisome HINTS exam: presence of ANY of the 3 components indicate a (+) finding (stroke or central pathology): a normal HIT, direction-changing nystagmus, OR skew deviation
3 components
1) head impulse test (HIT): ask the pt to fixate on a near target (PT's nose), grasp the pt's head, and apply a brief, small-amplitude (5-10°), and high-acceleration (3000-4000 deg/sec) head turn, first to one side and then to the other; when the head stops moving, the clinician looks to see it the eyes are still directed toward the target and watches for corrective saccades toward the target
a normal HIT result means the eyes remain fixed on the target after head rotation, suggesting a central lesion (worrisome); an abnormal HIT result (catch-up saccade), may indicate VOR deficit
abnormal finding is a GOOD finding; shows the person has a nerve problem (vestibular neuritis), not a brain problem
2) nystagmus: bidirectional nystagmus suggests a central cause (worrisome), which unidirectional nystagmus suggests peripheral
3) test of vertical skew: cover one eye then the other, observing if the eye moves medially and up/down
vertical misalignment of the eyes (skew deviation) suggests a central lesion (worrisome)
Only perform exam on patient with hours or days of continuous, ongoing vertigo and spontaneous nystagmus
Side Note: Having normal HINTS and NOT experiencing continuous, ongoing vertigo and spontaneous nystagmus is OKAY! Now, if your patient has the vertigo and nystagmus but all the tests are “normal”, we get worried because it is not following vestibular diagnoses patterns which would usually cause these symptoms, hinting to something more serious like stroke.
Be able to provide testing and treatment for a patient with BPPV.
What is it? Difference between Canalithiasis and Cupulolithiasisor? Which one do you test for first and and with what test? The ear going down is what side? What if its bilateral?
Goals of treatment? What is canalith repositioning and liberatory maneuver?
CNS:
What processes information from the PVS? This is why pts with stroke?
Many vestibular reflexes are controlled by processes that exist primarily within the?
Extensive connections between what structures?
Vestibular pathways appear to terminate in? This suggests?
it is a disorder of the inner ear caused by dislodged otoconia; occurs when the otoconia from the otoliths fall into the canals, stimulating the hair cells
canalithiasis: otoconia are free floating
cupulolithiasisor: otoconia stick to the cupula
examination: testing for canalithiasis first= Dix-Hallpike test and Log roll test
the ear going down is the side being tested; if bilateral, treat the worse side first
goals of tx:
educate the pt about self-treatment-> Brandt-Daroff Exercises (HEP)
replace the otoconia into the otoliths
Canalith Repositioning tx: movement of free-floating debris out of the involved SCC and into the vestibule (canalithiasis)
Liberatory (Semont) Maneuver: FAST; quickly shift the head to reposition the debris away from the cupula in the affected canal (cupulolithiasis)-> "S" in Semont= same side
Decrease vertigo
Increase balance
Return to daily activity involving head motion
CNS
the brain processes the information from the PVS
this is why pts with strokes misinterpret of motion signals leading to perceptual problems
many vestibular reflexes are controlled by processes that exist primarily within the brainstem (including VOR)
extensive connections btwn the vestibular nuclei and the reticular formation, thalamus (sensory relay station), and cerebellum (balance and coordination)
vestibular pathways appear to terminate in a unique cortical area, suggesting a distinct region in the brain dedicated to vestibular perception
How would a therapist know which side needed to be treated with bilateral BPPV?
treat the worst side FIRST
How would the treatment for a unilateral vestibular loss compare with a bilateral vestibular loss?
Bilateral Vestibular Lesion:
Most common cause is? Primary complaints? no nausea or vertigo UNLESS it's?
must use ________ of other mechanisms to try to gain ______ ______ because?
Goals and outcomes?
Physical therapy will heighten what two systems?
BPPV is not a?
Unilateral vestibular loss:
Most common cause is? Acutely, the patient will have? Prognosis?
Start with what movements? Progress to what movements?
Goals and outcomes?
PT will address what three things?
Bilateral vestibular loss:
the most common cause is ototoxicity (damage to the inner ear caused by certain medications or toxins)
primary complaint is disequilibrium, oscillopsia, and gait ataxia (unique to BVH)
no nausea or vertigo UNLESS it's asymmetrical (cannot be BPPV)
must use substitution of other mechanisms to try to gain gaze stability bc the system will not grow back
goals and outcomes:
reduce subjective complaints of gaze instability-> X1 exercises with your thumb (close eyes, shake head, open and refocus on the thumb in front of you), sequenced eye and head movements, imaginary targets (thumb out and close eyes, then open)
improve balance (static and dynamic)
instruct the pt in a HEP that includes walking: they are not moving bc they are scared but not moving will get them worse!
educating the pt in activities that may be difficult
increased safety awareness: fall prevention
PT will heighten the visual and somatosensory systems!
BPPV is NOT a bilateral vestibular lesion
Unilateral vestibular loss:
Most common causes: viruses, trauma, vascular events
Acutely, the patient will have: vertigo, nausea, resting nystagmus, oscillopsia with head movement, postural instability and disequilibrium (due to asymmetry)
→ pt tells you they get dizzy when they unload the dishwasher
Prognosis: The system has an amazing ability to recover since the nuclei “talk” to each other through interneurons.
Start with L and R movements then progress to up and down exercises
Goals and outcomes:
Improve stability of gaze during head movement through the VOR
Produce retinal slip so the system is “pushed” to recover: X1 exercises (move the head, x stays static) or X2 exercises (head and x go in opposite directions) if their neck is okay to do this
Make these harder by: standing, walking, being in busy gym environment
Decrease motion sensitivity: provoking activities, habituation training,
Reaching down to ”unload the dishwasher” repeatedly
Improve postural stability (static and dynamic = Dualtask Airex)
Use the alphabet on the floor or wall as they are standing and tell them to look for specific letters while standing still
Establish a HEP that includes walking: They are not moving because they are scared but not moving will get them worse!
Dual tasking during walking, simulate people walking by, scanning the aisles at the grocery store
➔ PT will address the oscillopsia, postural instability and disequilibrium!
Be familiar with other diagnoses involving the vestibular system, such as Meniere's Disease or motion sickness
Meniere's disease is caused by?
Symptoms?
Pts may be prescribed what?
Physical therapy can be helpful once they?
Motion sickness is caused by? Where should you look?
Meniere's disease
caused by fluid buildup in the inner ear, increased endolymphatic pressure within the ear
symptoms: ear fullness, vertigo, tinnitus, and hearing loss
pts may be prescribes medication (such as diuretics) to control fluid buildup and alleviate symptoms
physical therapy can be helpful once they are stable (MD clearance for PT), especially for balance dysfunction and other residual problems
motion sickness
sensory conflict: your eyes (visual) are seeing something, your vestibular system is perceiving something else, your somatosensory is getting other information
"look at the horizon" bc it doesn't move
Perilymphatic Fistulas?
Mal de Débarquement Syndrome?
Migraine Related Dizziness and cervicogenic Dizziness?
Perilymphatic Fistulas: Abnormal connection between the inner ear and middle ear, often requiring surgical intervention (Burst and require surgery: wait for MD clearance!)
Physical therapy can be helpful once they are stable (MD clearance for PT), especially for balance dysfunction and other residual problems
Mal de Débarquement Syndrome: Individuals experience a persistent sensation of motion or rocking after being exposed to motion, such as a boat or airplane trip.
‘Land sickness’ in French = lasts for MONTHS
Migraine Related Dizziness and cervicogenic Dizziness
Ask about what triggers the migraines and tell them to avoid them
If they are having a migraine, don’t treat them! Wait until it is over, then continue treatment
Help them identify triggers to avoid them
Treat what you find (are they dizzy, are they losing balance?)
Contraindications for vestibular rehab?
Not appropriate for what conditions? (4)
Or if pt presents with?
Once post op be observant for?
Not appropriate for:
Unstable vestibular disorders: Menieres disease
Uncontrolled migraine
PLF
Unrepaired superior semicircular canal dehiscence
Or if pt presents with:
Sudden loss of hearing
Increased feeling of pressure or fullness of ears
Severe ringing
Once post-op:
Be observant for discharge of fluid from ears or nose (CSF fluid)
Pts with acute neck injuries may not be able to tolerate the CRM, or some of the GSE’s
How would you respond if a patient experienced a sudden hearing loss? If you see leakage what does that mean? What is contraindicated?
immediate referral to the hospital! (could be a stroke)
if you see leakage, could be CSF or a flare up of Meniere's
PT CONTRAINDICATED!
What treatment would be appropriate for a patient with Vestibular Schwannoma (acoustic neuroma)?
What is it? What nerves does it impact?
PT is for pts experiencing? What is needed first?
Involves what exercises and helps compensate for what dysfunction?
tumor affecting CN VIII (vestibulocochlear) and VII (facial)
PT for pts experiencing balance issues and dizziness due to the tumor or after surgery (MD clearance for PT)
involves gaze stabilization, habituation, and balance training exercises
helps compensate for vestibular dysfunction and improve overall function
What are the three systems involved in balance control?
Of one of those systems, what are its three parts and wahc does each aprt do?
1) CNS integration
2) sensory systems: visual, vestibular, somatosensory
3) motor systems
For the sensory systems, what are its three parts and what does each part do?
For the vestibular system, the primary motor functions of the vestibular system include what three things?
Sensory organization: visual system
visual proprioception: orientation of the body parts with reference to the environment
relays information about the external environment
decreased visual acuity will have a negative impact on postural stability
Sensory Organization: Somatosensory Input
somatosensory input: cutaneous and pressure sensations (surface information)
receptors detect relative orientation and movement of body parts, and orientation of the support surface
include stretch reflexes, flexor withdrawal, crossed extensor reflexes, automatic postural reactions
Sensory Organization: Vestibular System
detects angular acceleration and deceleration forces acting on the head (SCC)
detects linear acceleration and orientation of the head in reference to gravity (otolith organs- saccule and utricle)
primary motor functions of the vestibular system include:
1) stabilization of gaze during head movements (VOR)
2) righting reactions of the head, trunk, and limbs (labyrinthine righting reactions)
3) regulation of muscle tone and postural muscle activation
Describe the motor strategies for balance recovery.
This is one of the three main functions of what system?
What is the ankle strategy?
Weight shifting strategy?
Hip strategy?
Suspensory strategy?
Stepping/Reaching strategy?
Combination strategy?
Standing vs sitting balance strategies?
Reactive vs anticipatory strategies?
one of the 3 main functions of the vestibular system
1) ankle strategy
used for small, slow perturbations on a firm surface (first line of defense)
relies on distal-to-proximal muscle activation or orientation
2) weight-shifting strategy
controls side to side weight shifts using the hips and trunk
often used when adjusting foot position or reaching
3) hip strategy
engaged when the ankle strategy is insufficient; larger, faster perturbations (on narrow or unstable surfaces)
involves proximal-to distal muscle activation
4) suspensory strategy
involves lowering the body by flexing the knees, hips, and ankles (lowering COM)
used in dynamic balance tasks, especially during sports or uneven terrain
5) stepping/reaching strategy:
used when other strategies fail, requiring a step or reach to prevent a fall (last resort)
6) combination strategies:
real-world balance recovery is often not isolated to one strategy but a blend
7) standing vs. sitting balance strategies
standing: requires more ankle, hip, and stepping strategies
sitting: relies more on trunk control and weight shifts (important for neuro pts)
8) reactive vs. anticipatory postural strategies
reactive: automatic responses after an external perturbation (slipping on ice)
anticipatory: preemptive adjustments before movement (stabilizing the core before reaching for an object)
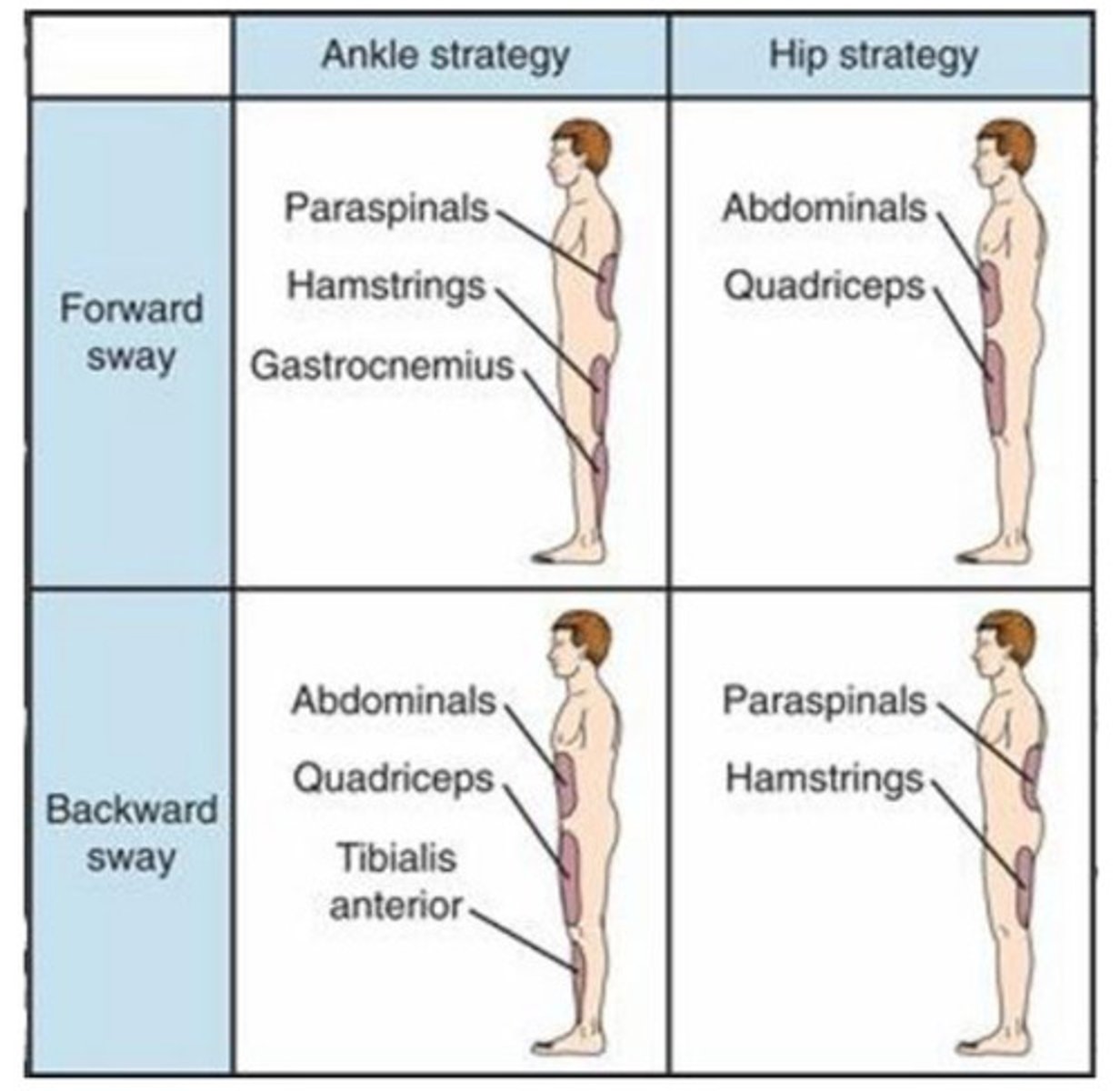
What is the muscle activation with these strategies?
For ankle when being pushed forward? When pushed back?
weight shifting?
Hip when being pushed forward? When pushed back?
suspensory?
For stepping and for reaching?
ankle strategy
pushed forward: gastrocnemius (PF)-> hamstrings-> paraspinals
pushed backward: tibialis anterior (DF)-> quadriceps-> abdominals
weight-shifting strategy
hip abductors (gluteus medius), adductors (adductor group), trunk muscles
hip strategy
pushed forward: abdominals-> quadriceps
pushed backward: paraspinals-> hamstrings
suspensory strategy
quadriceps, hamstrings, gluteals, and core muscles
stepping/reaching strategy
stepping: hip flexors, quadriceps, and dorsiflexors
reaching: arm muscles (deltoid, triceps, biceps)
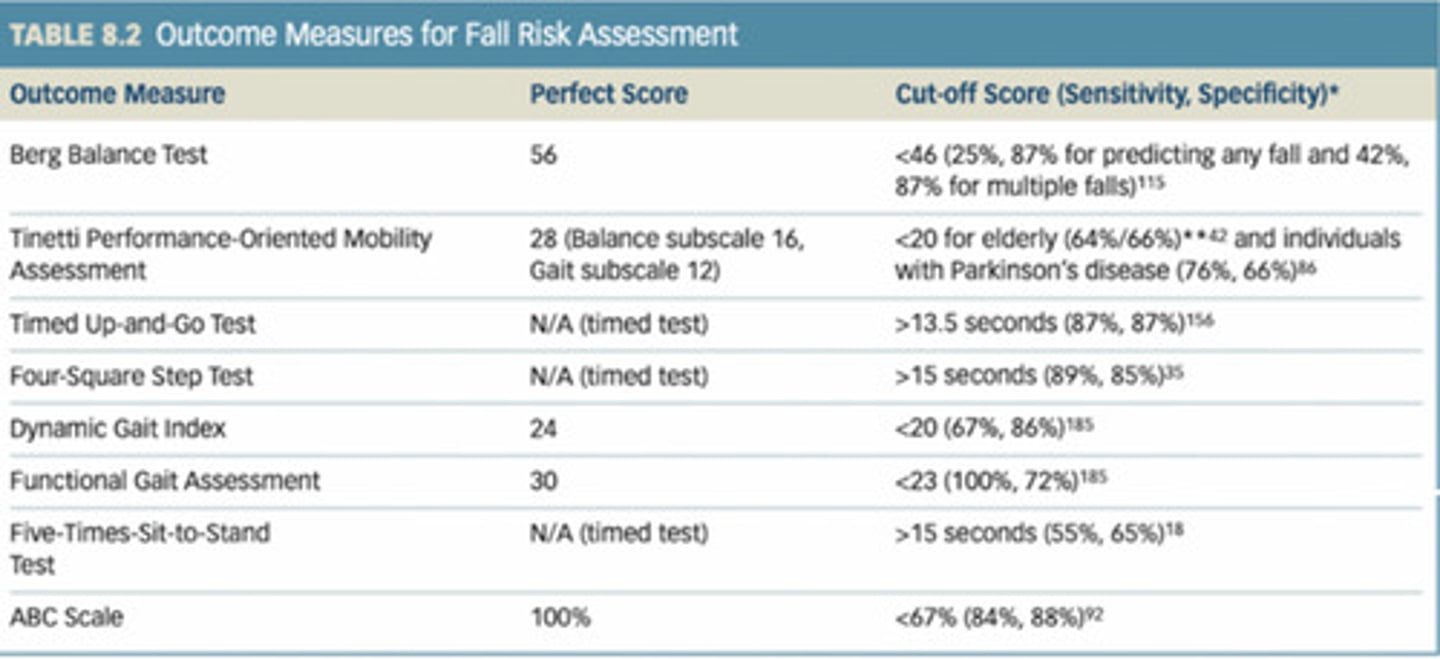
Be able to create a treatment plan related to the results of various balance and vestibular tests.
For the following outcome measure, what is the perfect score and what is the cutoff score?
Berg balance test
Tinetti performance - oriented mobility assessment
Timed up and go test
Four square step test
Dynamic gat index
Functional gait assessment
Five times sit to stand test
ABC scale
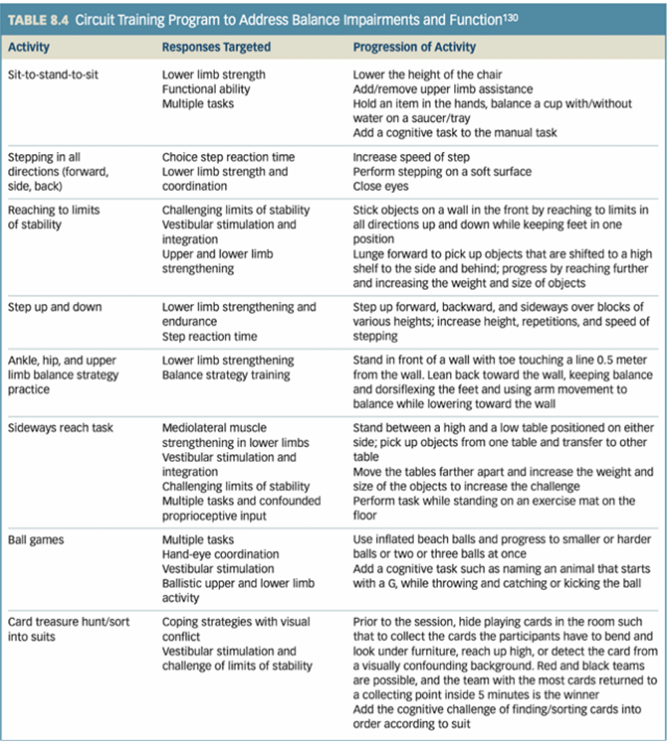
Be able to prescribe balance activities based on a case scenario.
For the following activities, what are the responses targeted and the progression of activity?
Sit to stand to sit
Stepping in all directions (forward, side, back)
Step up and down
Ankle, hip, and upper limb balance strategy practice
Sideways reach task
Ball games
Card treasures hunt/sort into suits
How do safety considerations and environmental modifications relate to balance impairments?
For instance what if someone is furniture walking?
Have proper ______ if the visual is impaired
-if someone is furniture walking, don't take away the furniture!
-have proper lighting if the visual is impaired
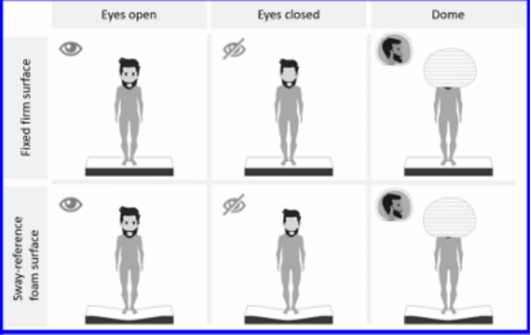
What are the six conditions utilized on the Clinical Test for Sensory Interaction in Balance examination? Which conditions would suggest vestibular dysfunction?
What are the three systems this tests? What does it always test?
For each condition state how they a performed and what systems are involved in each
CTSIB tests: visual, somatosensory, vestibular (it ALWAYS tests vestibular!)
Condition 1: eyes open, firm surface. All three systems
Condition 2: eyes closed, firm surface. Somatosensory and vestibular reliance
Condition 3: eyes open, firm surface, visual conflict (dome). Somatosensory and vestibular reliance
Condition 4: eyes open, foam surface. Vison and vestibular reliance
Condition 5: eyes closed, foam surface. vestibular reliance
Condition 6: eyes open, foam surface + visual conflict (dome). vestibular reliance
When considering balance or other functional tests, what is the Minimally Clinically Important Difference (MCID)?
Can be used to?
It helps determine what?
MCID: the smallest change in a test score that is perceived as MEANINGFUL and indicates a significant improvement or decline in FUNCTION
can be used to make goals
it helps determine whether an intervention has a real impact on a pt's condition rather than just a statistically significant change
How can this value (MCID) be used in writing patient-centered functional goals?
incorporating MCID into goal setting ensures alignment with best practices and provides objective justification for treatment efficacy
when claims are denied, referencing MCID offers strong, evidence-based support for appeals, demonstrating the intervention's direct impact on the pt's functional improvement
ex: 6MWT; MCID is a 50-meter difference
Be able to prescribe adaptive equipment as related to balance/functional loss and safety training.
Cane
Walker (standing, rolling, four wheel)
Hemi walker
Forearm (Lofstrand) crutches
Wheelchair
Home safety and functional aids
cane: provides mild support for balance impairments; best for unilateral weakness, mild vestibular dysfunction, or early-stage balance loss
walker: provides more stability for moderate-to-severe balance issues
standard walker: requires lifting, best for weight-bearing restrictions
rolling walker (2WW): easier to advance, good for patients with limited endurance
four-wheeled walker (4WW): includes a seat for rest, ideal for pts with fatigue or endurance issues
hemi walker: designed for unilateral weakness (post-stroke pts); provides more support than a can but is lighter than a standard walker
forearm (Lofstrand) crutches: used for long-term mobility support with more freedom than a walker; best for neuromuscular conditions (MS)
wheelchair: best for severe balance/motor impairments like ALS, SCI, advanced MS (power wheelchair)
home safety & functional aids: grab bars, raised toilet seat with handles, shower chair & non-slip mats
Given patient information, be able to perform differential diagnosis testing for a patient who complains of dizziness.
What three questions should you be asking them/yourself?
With vertigo, neurites will last how long? BPPV last how long?
are they losing balance because they can't see (DM related) or is it truly vestibular?
is it because they had a stroke and their depth perception has been thrown off?
how long is it lasting?
with vertigo, neuritis will last days to weeks & BPPV lasts about 10 minutes
Review the Life After Stroke: A Guide for Patients and Caregivers.
resource to give to pts
No other info on Amandas or Ashley’s guide
Identify the risk factors for a stroke.
Modifiable and Non modifiable
-modifiable: smoking, sedentary lifestyle, BP, cholesterol, diet
-non-modifiable: age
Promote prevention strategies for stroke.
What two things are important when dealing with stroke? AHA spoke about the importance of those two things with what campaign?
If someone has had a stroke, what is very important to prevent? Why?
-early recognition and prompt intervention ("brain attack" campaign by the AHA)
-think about preventing the SECOND stroke! (having one stroke increases the risk of having a second one)
What is (BE)FAST?
-B: BALANCE: SUDDEN LOSS OF BALANCE
-E: EYES: LOSS/CHANGE OF VISION IN ONE OR BOTH EYES
-F: FACE: FACE LOOKS UNEVEN (DROOPING)
-A: ARM: ARM/LEG WEAK/HANGING DOWN
-S: SPEECH: SPEECH SLURRED OR TROUBLE SPEAKING/SSEMS CONFUSED
-T: TIME: CALL 911 NOW!
Essentially how to identify a stroke is occurring
What is the pathology of a cerebrovascular accident?
ischemic stroke
Has opportunity to be saved with?
More or less common?
What two things can cause it to occur?
Conditions that cause what can lead to this type of stroke?
During the stroke, your brain is being deprived of what 2 things?
Disrupts cellular ________ → ________ = _______ _______
What is the most common site of a ischemic stroke (What artery)?
Hemorrhagic stroke
Better or worse outcomes?
What is it?
Occurs due to rupture of _____ ______ or what?
This causes what 3 things?
ischemic stroke
has opportunity to be saved w/TPA
more common
thrombus or embolus blockage
conditions that cause low systemic perfusion pressures (inadequate blood flow through the body's tissues due to reduced arterial pressure)
deprives brain of oxygen and glucose
disrupts cellular metabolism--> mitochondria= energy source
middle cerebral artery is the most common site for an ischemic stroke
hemorrhagic stroke
more tragic-->WORST OUTCOME
abnormal bleeding into the extravascular brain areas
result of rupture of a cerebral vessel or trauma
increased intracranial pressures, injury to brain tissues, and restriction to distal blood flow
What is the difference between a CVA and TIA?
TIA--> symptoms should resolve WITHIN 24 HRS
vascular event, warning sign of a stroke to come
refer to MD for proper medication! regardless, always call 911 if someone is showing signs of a stroke bc you don't know if it is a TIA or a CVA
What is the medical management of an ischemic stroke?
Acute
Pharmacological
Neurosurgical
acute management: make sure the pt doesn't die; stabilize them
pharmacological management:
thrombolytics: break down the clot
antiplatelet therapy: aspirin
don't ignore stroke pain!
neurosurgical management:
thrombectomy: physically removing the clot
decompressive craniectomy
What is the medical management of a hemorrhagic stroke?
surgery ASAP to stop the bleed
Be familiar with the NIH Stroke Scale. How can this scale be clinically useful?
First, what is the scale? For grading, what is the scoring like?
Clinical importance?
Levels of consciousness (What does each score mean from 0 to 3)
NIH Stroke Scale: numerical scale to determine stroke severity; health care providers record the person's performance in 11 categories and determine functional deficits
Scoring is between a 0 - 3, and 3 is scored only if the person makes no movement (other than reflexive posturing) in response to noxious stimulation (if applicable to the part of the scale, as some sections only let you grade from 0 - 2)
clinical importance
determines stroke severity
guides treatment decisions
tracks recovery & progression
standardized communication: helps healthcare teams discuss pt status clearly
level of consciousness
alert; keenly responsive
not alert; but arousable by minor stimulation to obey, answer, or respond
not alert; repeated stimulation, obtunded-> requires strong or painful stimulation
responds only with reflex or is totally unresponsive, flaccid, and areflexic
What is the penumbra?
How does tPA impact penumbra?
the penumbra is the area of brain tissue surrounding the core infarct (irreversibly damaged tissue) in an ischemic stroke
administration of tPA (tissue plasminogen activator) 3-4.5 hours of symptom onset protects the penumbra and can allow it to recover by breaking up the blood clot
the penumbra is functionally impaired but still salvageable
What is an ischemic cascade?
What are the steps of it (9)
series of damaging cellular events triggered by reduced blood supply to the brain
steps of the ischemic cascade
decreased O2 & glucose supply
failure of ATP production
failure of ATP dependent ion pumps
disruption of ionic homeostasis-> sodium (Na+) and calcium (Ca2+) accumulate inside cells, causing cellular swelling (cytotoxic edema)
excess glutamate release-> leading to excitotoxicity
calcium overload-> activates enzymes that damage cell membranes, proteins, DNA
oxidative stress & free radicals-> further damages neurons
inflammatory response-> worsens brain injury and contributes to secondary damage
apoptosis (neuronal cell death)-> irreversible infarction if blood flow is not restored
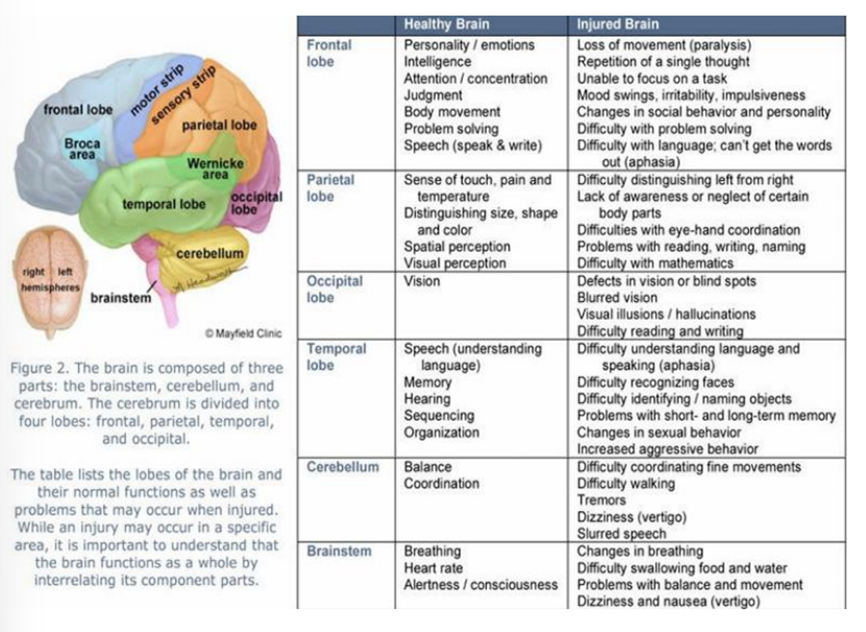
Identify the different parts of the brain and the associated functions.
For each of the following, say what it does in a healthy brain vs how its impacted in an injured brain
Frontal, parietal, occipital, temporal lobes
Cerebellum
Brainstem
Frontal lobe
— Healthy brain:
Personality / emotions
intelligence
Attention / concentration
Judgment
Body movement
Problem solving
Speech (speak & write)
— Injured brain
Loss of movement (paralysis)
Repetition of a single thought
Unable to focus on a task
Mood swings, irritability, impulsiveness
Changes in social behavior and personality
Difficulty with problem solving
Difficulty with language, can’t get the words out (aphasia)
Parietal lobe
— Healthy brain:
Sense of touch, pain and temperature
Distinguishing size, shape and color
Spatial perception
Visual perception
— Injured brain
Difficulty distinguishing left from right
Lack of awareness or neglect of certain body parts
Difficulties with eye-hand coordination
Problems with reading, writing, naming
Difficulty with mathematics
Occipital lobe
— Healthy brain:
Vision
— Injured brain
Defects in vision or blind spots
Blurred vision
Visual illusions / hallucinations
Difficulty reading and writing
Temporal lobe
— Healthy brain:
Speech (understanding language)
Memory
Hearing
Sequencing
Organization
— Injured brain
Difficulty understanding language and speaking (aphasia)
Difficulty recognizing faces
Difficulty identifying / naming objects
Problems with short- and long-term memory
Changes in sexual behavior
Increased aggressive behavior
Cerebellum
— Healthy brain:
Balance
Coordination
— Injured brain
Difficulty coordinating fine movements
Difficulty walking
Tremors
Dizziness (vertigo)
Slurred speech
Brainstem
— Healthy brain:
Breathing
Heart rate
Alertness / consciousness
— Injured brain
Changes in breathing
Difficulty swallowing food and water
Problems with balance and movement
Dizziness and nausea (vertigo)
Identify the differences seen in patients with injury to the right or left hemisphere.
right hemisphere injury: difficulty with executive function, spatial-perceptual tasks; quick, impulsive, overestimate their ability, L side neglect, R gaze preference
left hemisphere injury: difficulty with communication, language, numbers, and reasoning; motor and visual deficits on the R, L gaze preference, anxious, disorganized
Identify major features of the different vascular syndromes, especially those discussed in class.
ACA - What are the affected areas? Clinical features?
MCA - What are the affected areas? Clinical features?
ICA - What are the affected areas? Clinical features?
PCA - What are the affected areas? Clinical features?
Lacunar stroke - What are the affected areas? Clinical features?
Cerebellum stroke - What are the affected areas? Clinical features?
Vertebrobasilar artery syndrome- What are the affected areas? Clinical features?
Locked in syndrome - What are the affected areas? Clinical features?
anterior cerebral artery syndrome (ACA)
affected area: medial frontal & parietal lobes
clinical features: contralateral weakness & sensory loss (LE> UE), urinary incontinence (frontal lobe), personality changes, apathy, or impulsivity
middle cerebral artery syndrome (MCA)
affected area: lateral frontal, temporal, & parietal lobes; basal ganglia
clinical features: contralateral weakness & sensory loss (UE>LE), Broca's aphasia (if the dominant hemisphere is affected), contralateral homonymous hemianopia, neglect (if right hemisphere is involved), unilateral neglect, perceptual deficits
internal carotid artery syndrome (ICA)
affected area: ACA and MCA territories (larger area of the brain)
clinical features: severe motor/sensory deficits (both UE/LE), cortical blindness (if the PCA also affected), can lead to coma or death
"I" for eyes; "internal"--> "in" everything (whole body)
posterior cerebral artery syndrome (PCA)
affected area: occipital lobe, thalamus, & brainstem
clinical features: contralateral homonymous hemianopia (visual loss), visual agnosia (can't recognize objects), prosopagnosia (can't recognize faces), memory loss, thalamic pain syndrome (severe/chronic pain)
Lacunar Strokes (Small Vessel Disease) •
Affected Area: Small, deep brain structures (basal ganglia, thalamus, pons). •
Clinical Features: pure motor stroke (internal capsule or pons), pure sensory stroke (thalamus), ataxic hemiparesis (cerebellar involvement), dysarthriaclumsy hand syndrome (pons), no cortical deficits (aphasia, neglect), multiinfarct dementia (multiple strokes lead to accumulation of deficits)
Cerebellum Stroke
Affected Area: Cerebellum
Clinical Features: dysmetria, scissoring gait, ataxia, dysdiadokinesia
Vertebrobasilar Artery Syndrome
Affected Area: Brainstem, cerebellum, and occipital lobe.
Clinical Features: Dizziness, vertigo, nausea/vomiting, diplopia, dysphagia, ataxia (lack of coordination)
Locked-In Syndrome
Affected Area: Ventral pons (corticospinal and corticobulbar tracts).
Clinical Features: Complete paralysis (except for eye movements, typically vertical gaze), no speech or limb movement, preserved cognition and sensation, communication is possible via eye movements or blinking.
Be familiar with pharmacological management following a CVA.
Thrombolytics
Anticoagulants
Antiplatelets therapy
Antihypertensive agents
Angiotensin II receptor antagonists
anticholesterol agents/statins
antispasmodics/spasmolytics
antispastics
anticonvulsants
antidepressants
thrombolytics: dissolves blood clots
anticoagulants (Warfarin [Coumadin], Heparin}: prevents clot formation
antiplatelet therapy (Aspirin): prevents platelets from sticking together, reducing thrombus formation
antihypertensive agents (ACE inhibitors, Beta-blockers, Calcium channel blockers): lowers BP to prevent stroke
angiotensin II receptor antagonists (Losartan [Cozaar]): blocks angiotensin II to relax blood vessels and lowers BP
anticholesterol agents/statins: lowers cholesterol, prevents atherosclerosis strokes
antispasmodics/spasmolytics (Diazepam [Valium]): relaxes muscles and spasticity
antispastics (Baclofen [Lioresal], Tizanidine [Zanaflex]): relaxes muscle and spasticity
anticonvulsants (Clonazepam [Klonopin]): controls seizures, CNS depressant
antidepressants (Fluoxetine [Prozac], Sertraline [Zoloft]): post-stroke depression
What would be the components of a comprehensive physical therapy examination for a patient with a stroke?
cognition
cardiopulmonary
cranial nerve integrity
sensation & vision
we need to do a better job on assessing vision!
pain
joint integrity & flexibility
motor function
stages of motor recovery
obligatory synergy patterns (look at the strongest components***)
tone: Modified Ashworth Scale
reflexes: DTR, pathological (Babinski), tonic
coordination
motor planning
motor praxis: ability to plan & execute coordinated movement
ipsilateral pushing --> Pusher syndrome
muscle strength
do MMT on strong side but on involved, have them do STS or rolling in bed
hemiplegia/hemiparesis
presence of associated reactions: if R CVA (L weak), you resist R leg (L leg goes into a movement)
postural control and balance/functional testing/status
gait & locomotion
integumentary integrity
aerobic capacity & endurance
stroke specific instruments
What are the neurological complications following stroke?
altered consciousness
aphasia
fluent aphasia (Wernicke's/receptive aphasia): difficulty with comprehension
nonfluent aphasia (Broca's/expressive aphasia): difficulty with speech
global aphasia: difficulty with both production and comprehension of language
dysarthria: motor disorder preventing fluent speech (linked to dysphagia)
dysphagia: risk of aspiration and nutritional needs
may need a MBS (Modified Barium Swallow) study to rule out
cognitive dysfunction: attention (quiet, closed environment recommended), memory, executive function, multi-infarct dementia (multiple strokes lead to accumulation of deficits, Lacunar stroke), delirium (confusion, hallucinations)
delirium is transient (tends to go away when things calm down) and if sudden >dementia does not get better
altered emotional state: pseudobulbar affect anxiety, irritability, frustration, depression (medications support groups)
perceptual dysfunction: body scheme/body image (unilateral neglect), spatial relations, agnosia (not recognizing things, inability to process sensory input)
seizures
bladder and bowel dysfunction
cardiovascular and pulmonary dysfunction: were not active before stroke
using an AFO forces you to be more active!
DVT & PE: sedentary
osteoporosis and fracture risk: sedentary
sleep disturbances: insomnia, sleep apnea, sleep disturbances could lead to a stroke, good sleep wake cycle (circadian rhythm) is crucial!
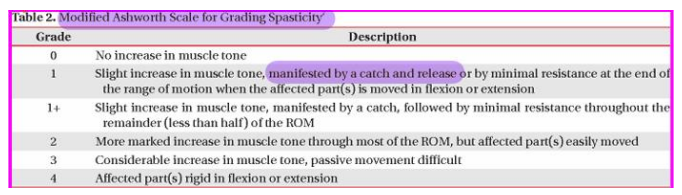
Be able to assess and measure a patient's tone. Be able to use the Modified Ashworth Scale.
What are the steps (3)?
Grading scale?
position the pt comfortably in supine, ensuring the muscle being tested is relaxed
move the joint passively through its full available ROM at a consistent, moderate speed
(technique: if muscle flexes, place in maximal flexion then move to full extension rapidly)
feel for resistance to passive movement and assign a score based on the MAS (velocity dependent)
grading scale
0 - no increase in muscle tone
1 - slight increase in muscle tone, manifested by a catch and release or by minimal resistance at the end of the ROM when the affected part(s) is moved in flexion or extension
1+ - slight increase in muscle tone, manifested by a catch, followed by minimal resistance throughout the remainder (less than half) of the ROM
2 - more marked increase in muscle tone through most of the ROM, but affected part(s) easily moved
3 - considerable increase in muscle tone, passive movement difficult
4 - affected part(s) rigid in flexion or extension
Identify synergistic flexion and extension patterns for the upper and lower extremity. Which components are strongest in each synergy?
UE synergies
1) flexion synergy
scapular retraction/elevation
shoulder ABD & ER
elbow flexion (strongest)
forearm supination
wrist & finger flexion
2) extension synergy
scapular protraction
shoulder ADD & IR (strongest)
elbow extension
forearm pronation (strongest)
wrist & finger flexion or extension
LE synergies
1) flexion synergy
hip flexion (strongest)
hip ABD & ER
knee flexion
ankle DF & IV
toe extension
2) extensor synergy
hip extension, ADD & IR (Hip extension and ADD strongest)
knee extension (strongest)
ankle PF & IV (ankle PF strongest)
toe flexion
How can the patient's upper extremity be protected during movement and upright activities?
Prevent what and promote what two things?
How can subluxation be prevented? E stim should go on what muscles?
Why should you WBAT?
What can be used to stability and what can be used for support?
prevent impingement promote scapular upward rotation and elevation
prevent subluxation by elevating the arm with a GivMohr sling and KT tape; e-stim to medial and posterior deltoid/supraspinatus
WBAT for proprioception
air splint for stability, KT tape for support
Define the Stages of Motor Recovery. How can these help to guide treatment? (Identify each stage, what each stage entails, and what treatment can be done)
1) flaccidity: no voluntary movement or reflex activity
tx focus= prevent contractures, maintain ROM, and use PROM
2) synergies, some spasticity: minimal voluntary movement-> early synergistic movements appear (involuntary, patterned muscle contractions)
tx focus= encourage activation of weak muscles, initiate WB activities
3) marked spasticity: spasticity peaks, synergistic movements dominate
tx focus= strengthen isolated movement, introduce AAROM, avoid reinforcing synergy patterns
4) out of synergy, less spasticity: some isolated movement-> voluntary movement begins outside of synergy patterns
tx focus= improve coordination, emphasize functional tasks, work on isolated joint movements
5) selective control of movement: more control, less reliance on synergy patterns
tx focus= strengthen individual muscle control, refine movement patterns, incorporate functional tasks
6) isolated, coordinated movement: isolated joint movements are smooth and controlled
tx focus= fine motor coordination, balance, strength training
What is Pusher Syndrome? How can it be managed?
Misperception of what, causing what?
What activities can this be seen in?
Key interventions? (What types of feedback can be used and how? What types of training are ideal for this syndrome?)
What side should you guard on?
ipsilateral pushing: neurological condition seen in pts with stroke or brain injury, where they actively push toward their weaker, hemiparetic side using their stronger limbs (causes lateral postural imbalance)
misconception of vertical orientation, leading to postural imbalance
seen in various postures and activities (sitting, standing, and walking)
key interventions
visual & sensory feedback: use mirrors to help pts align with visual verticals; have them touch a stable surface (wall, chair) with a non-affected hand for reference
weight shifting & postural training: encourage active midline orientation by shifting weight toward the stronger side
task-specific training: lateral reaching tasks to promote midline awareness (guard on weaker side)
Guard on weaker side
Which is more effective for Pusher Syndrome, active or passive correction? Do not do what to patients with this syndrome and why? What are some cues you can used to help guide a patient?
active; DO NOT PASSIVELY MOVE THEM!! pt doesn't respond well to passive repositioning (being pushed into correct posture)
-"lean towards the wall"
-"lean towards me"
What would be appropriate treatment protocols for a patient with a flaccid UE or LE?
Effective position of the pt in bed: Put a pillow under what and why? What should be offloaded and how? Put pillow where when sidelying?
Bed mobility and transfers: Proper rolling towards the affected or unaffected side when at home or with nurses? What should be worked on at therapy?
effective position of the pt in bed:
put a pillow under the affected UE while supine to promote extension
offload the heels by putting a pillow under the calves
put a pillow between the LE and the arm when side lying
bed mobility and transfers:
proper rolling towards unaffected side at home or with nurses for safety
work on the affected side in therapy to strengthen
How can spasticity be managed?
What type of stretching is ideal and for how long? Why? What can help maintain muscle length?
What is autogenic inhibition and how does it work (mediated by what)?
WB joints approximation for?
Strengthen what muscles?
Positioning techniques: What positions and why?
E stim used for?
Avoid spasticity triggers such as?
What medication are used to treat spasticity?
Straps should be used for? Are free weights open chain or machine closed chain better for spasticity?
prolonged, slow stretching (hold for 30-60 sec)--> targets hypertonic muscles to reduce stiffness; splinting or orthotics may help maintain length
autogenic inhibition: neuromuscular reflex that causes a reduction in muscle activity following an excessive or sustained increase in tension, primarily mediated by Golgi tendon organs (GTOs)
WB joint approximation for muscle recruitment
strengthen antagonists (opposite muscles)--> ex. strengthen DF to reduce PF spasticity
positioning techniques--> prevents contractures (side-lying, weight-bearing postures)
e-stim (NMES, TENS)--> activates weak muscles or fatigues spastic ones
avoiding spasticity triggers (fatigue, stress, infections)
medications: Diazepam (Valium), Baclofen (Lioresal), Dantrolene Sodium (Dantrium), Botox injections to manage focal spasticity
use straps for hands and feet, closed chain exercises and machines instead of free weights and open chain
Why is it important to avoid learned non-use?
when a pt neglects using a weaker limb due to difficulty or frustration, it leads to further loss of function (muscle atrophy and further weakness)
if you don't use it, you'll lose it
When are compensatory strategies appropriate?
You should encourage what first, then integrate compensatory strategies when needed to?
What are the two reasons to learn compensatory strategies
if not achieving full recovery
encourage restorative therapy first, but integrate compensatory strategies when needed to maintain function (not likely to regain it)
1) recovery is limited or unlikely (chronic stroke with severe deficits)
2) pt has safety concerns (fall risk, difficulty holding objects securely)
Be able to prescribe activities for a patient with a stroke, based on a case scenario.
To encourage engagement, the activities need to be?
Use of feedback (what 2 types)
Practice need to be physical and?
Attention to? This relates to what framework?
Monitor for what two things?
-patient engagement--> meaningful activities
-use of feedback (intrinsic and extrinsic)
-practice (physical and mental)
-attention to learning environment--> Gentile's Taxonomy
-monitor for physical and mental fatigue--> adjusting dose and progression
Be able to apply Gentile's Taxonomy to a patient scenario. Based upon a case scenario, design the appropriate treatment environment.
What are the 4 sections?
example case scenario: a post-stroke patient with R hemiparesis is working on improving STS transfers and ambulation with an AD:
Apply Gentiles Taxonomy and outline each of the 4 sections for this patient.
(^ For this, the example ashley gave makes no sense so forget what it says there, just follow what evelio told u)
1) stationary individual in stationary environment
2) moving individual in a stationary environment
3) stationary individual in a moving environment
4) moving individual in a moving environment
🔹 1. Stationary individual in stationary environment
• Body stability
• Stable, predictable environment
________________________________________
🔹 2. Moving individual in stationary environment
• Body transport introduced
• Environment still stable
________________________________________
🔹 3. Stationary individual in moving environment
• External environment becomes:
o Variable / unpredictable
________________________________________
🔹 4. Moving individual in moving environment (MOST COMPLEX)
• Body transport + environmental variability
________________________________________
How can mental practice (motor imagery) be applied during patient treatment?
if the pt is cognitively aware, instruct them to run through the exercise in their head, so mental repetitions promote neuroplasticity
Kinda like mental image training
How can neuroplasticity be promoted?
What three things? For one of those things, what is it so important?
salience (important/significant) mental imagery, repetition, intensity
INTENSITY MATTERS BC IT PROMOTES NEUROPLASTCITY!--> Karvonen Formula: THR= [(HRmax-HRrest)x intensity] + HRrest
Be familiar with constraint induced therapy.
What is it? Promotes what and prevents what? Must be _____ to the pt.
Pts should be?
Lasts up to how long and in intervals that are how long? Rests should be?
What other item is used to give visual feedback to the pt?
restrict the unaffected limb and perform intensive, repetitive tasks with the affected limb
promotes neuroplasticity and prevents learned non-use; must be salient to the pt!
pts should be cognitively aware
lasts up to 15 minutes in 5-minute intervals with short rests
includes mirror therapy: artificial visual feedback makes it possible for the pt to "move" the affected limb
Apply strategies to improve sensory function based upon a case scenario.
? No info on Ashley’s or Amanda’s guide
How can mirror therapy be used to promote movement in a patient's hand? How does it work?
neuroplasticity activation
the brain perceives the affected limb as moving, activating mirror neurons and motor pathways
tricks the brain into thinking that the involved limb is moving like normal
helps retrain the brain-body connection and improve voluntary movement
How can body weight support, virtual reality, and/or robotics be applied to patient care management?
When would body weight support or the Lokomat be appropriate for a patient (robotic tech)? Describe the robotic assistance, therapist efficiency, and precautions.
How does the Alter G treadmill work? This allows for what activities? Cons?
How might gaming or virtual reality be incorporated into patient treatment? VR driving helps with what and music glove hand therapy helps with what?
When would body weight support or the Lokomat be appropriate for a patient (robotic tech):
Works well with neurological patients, pediatric neuromuscular rehabilitation, severe muscle atrophy
Robotic Assistance: Lokomat is especially suitable for patients needing consistent, repetitive gait patterns → severe spasticity or poor motor control.
Therapist Efficiency: For patients requiring long-duration gait training that may be physically demanding for therapists to manually assist.
Precautions: check for pressure injuries. The harness lifts from the hips which may lead to femoral artery issues. Pts w/ cognitive deficiency might not be able to give feedback of level of comfort.
(2) How does the Alter G treadmill work?
Reduced gravity
Works by using differential air pressure (DAP) technology to reduce the user's body weight, allowing for low-impact exercise and rehabilitation.
CON: Therapist cannot give physical cues because the patient is enclosed in the treadmill
(3) How might gaming or virtual reality be incorporated into patient treatment?
Makes rehab engaging and interactive while promoting specific functional goals.
VR can simulate real-world challenges, such as navigating through crowds
Driving: attention, reaction time, visual scanning, and decision-making
Music Glove Hand Therapy: finger dexterity, strength, and coordination
What role does electrical stimulation play? Functional component? Spasticity management?
Activates ____ muscles or fatigues ______ ones.
FES uses what? What does this allow it to do?
Give an example of e stim on the LE being used to help functionally.
Give an example of e stim application on UE. What patient population would this help?
spasticity--> activates weak muscles or fatigues spastic ones
functional electrical stimulation (FES) use low-level electrical currents to activate/facilitate muscle contraction
e-stim activates DF during swing phase: a heel switch or motion sensor detects the walking cycle and triggers stimulation at the right time
UE applications: hand grasp & release- helps stroke or SCI pts with grasping objects
Be able to identify and prescribe treatment strategies for patients with cognitive-perceptual deficits.
What approach is very important? What questions should you ask yourself about the patient? How can a social worker help?
Visual impairments: Acuity? Oculomotor control? Intact visual fields? Diplopia? Homonymous hemianopsia (What type deficit)?
Body scheme impairments: Unilateral neglect? Anosognosia? Somatoagnosia? Right-left discrimination? Finger agnosia?
use a team approach-> extremely important w/home arrangements & safety
can they go home alone? will they set their house on fire? will they confuse a household item with food?
have the social worker (supported by physician/OT/SLP) help find a home for them where they'll be SAFE
visual impairments
acuity: Snellen chart, 20ft away smallest line person can read
oculomotor control: smooth pursuits-> tx: bubbles, following object
intact visual fields: cover one eye, check for peripheral vision
diplopia: double vision-> tx: eye patching, sx, Botox, referrals
homonymous hemianopsia: can only see one side; R/L
sensory deficit! 1 side gets cut out vs. neglect is a cognitive perceptual deficit
body scheme impairments
unilateral neglect: unable to register stimuli on one side of body-> tx: work on getting the pt to address that side (stand on affected side, hot/cold, loud noise)
anosognosia: denial that limb is paralyzed-> tx: getting pt to address the limb
somatoagnosia: difficulty distinguishing body parts-> tx: pt or therapist stimulate the body part to bring awareness through sensation
right-left discrimination: inability to discriminate between R/L side of body-> tx: colored stickers on extremities and point to the different colors
finger agnosia: unable to identify fingers-> tx: rough textures for tactile/sensory input, identifying games
Be able to identify and prescribe treatment strategies for patients with cognitive-perceptual deficits. (continued)
Spatial relations disorders: figure-ground discrimination? form discrimination? spatial relations? position in space? topographic disorientation? depth and distance perception? vertical disorientation?
What is agnosia and what are the three types?
What is apraxia? What are the two types?
spatial relations disorders
figure-ground discrimination: inability to distinguish figures from an embedded background-> tx: practice identifying objects in threes and then introduce more
form discrimination: confusion w/objects of similar shape-> tx: practice describing, identifying, demonstrating items (pencil-toothbrush)
spatial relations: inability to perceive the relationship btwn objects, unable to tell when objects are too close/far apart/approximately lined up-> tx: "sit next to me", "lay down on the bed", activities that encourage crossing over midline
position in space: difficult to interpret spatial concepts "up, down, over, under"-> tx: place 4 different items in a row, facing the same way and then add a 5th and have it upside down, ask pt to identify if there's an odd one out
topographic disorientation: difficulty finding one's place to another (person gets lost in a familiar place)-> tx: verbal cues, give directions and see if they can find the end point
depth and distance perception: judgment of depth is off, misjudge distance, difficulty navigating stairs/curbs-> tx: practice different depths and heights
vertical disorientation: pts lean to the side (not in midline)-> tx: cueing, mirror (Pusher Syndrome)
agnosia
inability to recognize/make sense of incoming information despite intact sensory capacities → visual object (don't recognize what they see), auditory (don't recognize what they hear), & tactile agnosia (don't recognize what they feel)
apraxia
disorder of voluntary skilled learning movement
ideomotor apraxia: able to carry out habitual tasks automatically, but unable to perform on command; often preservative
ideational apraxia: failure in conceptualization; inability to perform a purposeful motor task at all; cannot verbally describe the process or functions of objects
What functional activities would be especially difficult for a patient lacking depth perception?
pouring liquids
grabbing objects (misjudging distance when reaching)
using stairs or curbs (difficulty gaging step height)
crossing the street (judging distance & speed of cars)
cutting food or using knives (risk of injury)
driving or parking (judging distance to cars, curbs, or pedestrians)
catching or throwing a ball (hand-eye coordination issues)
What strategies would be helpful for a patient with unilateral neglect?
First, what is it? Not due to? What side does it typically occur on?
Treatment strategies: Sit on left or right? What if they are very inattentive? Give an example
How can sensory input be used?
What item can be used to help them see they have the other half of their body? What therapy can be used if their hand is not able to move?
Unilateral Neglect
Unilateral neglect is the inability to register and integrate stimuli and perceptions from one side of the body (body neglect) and the environment or hemispace (spatial neglect)
NOT DUE to sensory loss
Typically seen on the left
Treatment Strategies
Sit on the left. If they are really inattentive, start on the right and transition to the left.
Example: Dr Roberts had a patient that loved TV. She slowly (over weeks) started moving the TV to the left to promote that side (motivation)
Use motivating factors!
Use sensory input → tap on the left side, running water, hot & cold, etc.
Use a mirror so they can see they have a body on the left
Mirror Box Therapy if the hand is not able to move
How does hemianopsia compare with unilateral neglect?
Hemianopsia is what type of deficit? What about unilateral neglect?
Which one is the patient aware of if they have it? Which is harder to treat?
hemianopsia: sensory deficit (visual)
you could teach them how to fix it bc they are AWARE of it (they can only see one side)
easier to treat compared to neglect
Unilateral neglect: cognitive perceptual deficit
they cannot fix it bc they are NOT AWARE of it (cannot register stimuli on one side)
more challenging than hemianopsia
Demonstrate knowledge about treatment strategies to promote motor control and functional abilities. For each of the following state what each treatment would entail
Bed mobility - What movements? What patterns can be used?
Wheelchair mobility
Transfers
Gait and balance
ROM - What muscles should you focus on?
Strength training
Aerobic conditioning
bed mobility: bridging, rolling (PNF patterns D1/D2 UE & LE), supine to sit via side lying (breaks the task into manageable steps for easier execution)
wheelchair mobility: propulsion training, WC skills (turns, ramps, curbs, and uneven surfaces), weight shifts to prevent pressure injuries
transfers: sliding boards, pivot transfers, stand pivot vs. squat pivot
gait & balance: parallel bars, step-through patterns, cross-stepping, and dual-task walking, balance challenges (EO/EC, foam, perturbations)
ROM: joint mobilization & stretching (focus on tight hip flexors, hamstrings, and PFs)
strength training: task-specific (STS, step ups, reaching tasks), PNF strength techniques (repeated contractions & slow reversals)
aerobic conditioning: seated UE ergometers, recumbent bikes, monitoring HR & BP
What are the parameters for high intensity training for a patient recovering from stroke or head injury?
? No info on Ashley’s or Amanda’s guide.
Come back to this and use the value from neuro LAB ty evelio
What are the possible mechanisms of a traumatic brain injury (4)
-falls (32%)
-motor vehicle/traffic accidents (19%)
-struck by/against events (18%)
-assaults (10%)
What is a concussion? AKA mTBI
Can be caused by what two things?
If some gets a concussion, does that mean they will lose consciousness or not?
Why should you take concussion seriously?
brain injury when the brain is shaken inside the skull (aka mTBI)
can be caused by a direct force to the head or an indirect force
they MAY OR MAY NOT lose consciousness (before if they did lose consciousness, it was not considered a concussion)
CONCUSSION IS A BRAIN INJURY, don't take it lightly!
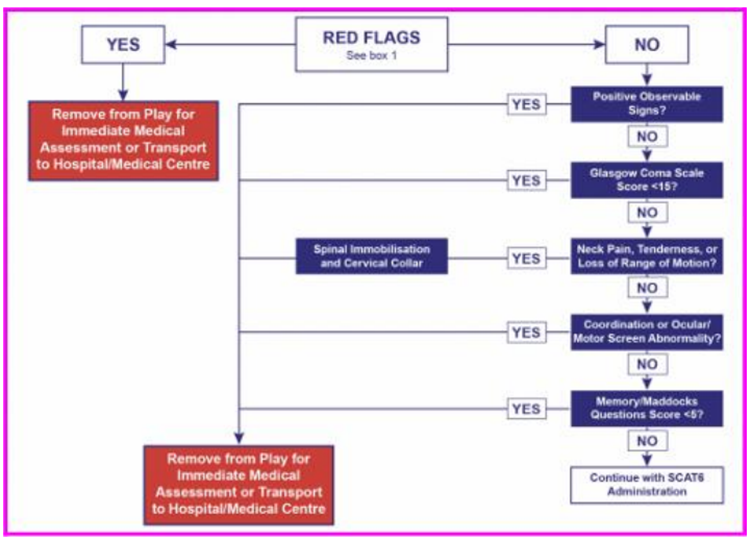
How can the SCAT6 assist with concussion identification? What age group and population? What does it include? Determines if?
Sport Concussion Assessment Tool (SCAT) 6 for evaluating athletes aged 13 years and older
list of steps that compiles objective and subjective findings
determines if the person had a concussion and which functions are impacted
Are there red flags?
If yes: Remove from play for immediate medical assessment or transport to hospital/medical Centre
If no: Continue to next question
Positive observable signs?
If yes: Remove from play for immediate medical assessment or transport to hospital/medical Centre
If no: Continue to next question
Glasgow coma scale score < 15?
If yes: Remove from play for immediate medical assessment or transport to hospital/medical Centre
If no: Continue to next question
Neck pain, tenderness, or loss of ROM?
If yes: Spinal immobilization and cervical collar AND remove from play for immediate medical assessment or transport to hospital/medical Centre
If no: Continue to next question
Coordination or ocular/motor screen abnormalities?
If yes: Remove from play for immediate medical assessment or transport to hospital/medical Centre
If no: Continue to next question
Memory/Maddocks questions score <5?
If yes: Remove from play for immediate medical assessment or transport to hospital/medical Centre
If no: Continue with SCAT6 Administration
What is Chronic Traumatic Encephalopathy CTE?
Commonly seen in what populations?
S/S? These can lead to what?
CTE: progressive neurodegenerative disorder caused by repeated head trauma, such as concussions or sub concussive hits
commonly seen in athletes (football, boxing), military personnel, and others exposed to repetitive brain injuries--> Like Tua
some athletes have committed suicide by shooting their heart and not their brain so that their brains could be studied
s/s: memory problems, changes in emotion and personality → depression
Be able to recognize the signs and symptoms of concussion and CTE. Discuss issues of return to play and return to learn or work.
Physical Symptoms Concussion
Potential Longer Term Symptoms of Concussion
Emotional Symptoms of Concussion
Cognitive Symptoms of Concussion
physical symptoms concussion
headaches & dizziness
difficulty w/balance
N/V
fatigue
difficulty w/sleeping
double or blurred vision
sensitivity to light/sound
slurred speech
glassy-eyed stare
potential longer-term symptoms of concussion
loss of libido
loss of menstruation
growth problems (children)
fatigue, exercise intolerance
weight gain
changes in BP and/or HR
muscle weakness
chronic headaches or dizziness
muscle spasticity
early dementia/chronic traumatic encephalopathy (brain disorder)
emotional symptoms of concussion
irritability
restlessness
anxiety
depression
mood swings
aggression
decreased tolerance for stress
change in personality/behavior
cognitive symptoms of concussion
difficulty w/memory
confusion
slowed processing of information
Feeling 'foggy'
difficulty w/concentration
decreased performance
WHOOP WHOOP
deterioration of motor skills, memory (could indicate bleed)
Identify the neurological sequelae following a traumatic brain injury.
Neuromuscular Impairments
Cognitive Impairments
Neurobehavioral Impairments
Communication Impairments
Swallowing
Dysautonomia
Disordered Sleep
Post traumatic seizures
Secondary Impairments and Medical Complications
Which one of them is getting the pt up important?
We want to do ROM, but not _______.
neuromuscular impairments: paresis, impaired coordination and postural control, abnormal tone, abnormal gait, tremor and chorea (less common)
cognitive impairments: arousal, concentration, memory, learning, executive functions (planning, cognitive flexibility, response inhibition)
neurobehavioral impairments: agitation/aggression, disinhibition, apathy, mental inflexibility, impulsiveness, irritability
communication impairments: disorganized oral or written communication, imprecise language, word retrieval difficulties, socially inappropriate language, difficulties in distracting environments, reading social cues
swallowing: nutritional needs and aspiration risk
dysautonomia: overactive sympathetic response-> increased HR, RR, and BP, diaphoresis, decerebrate/decorticate posturing, hypertonia, and teeth grinding
disordered sleep: insomnia, hypersomnia, and sleep apnea (think of their circadian rhythm and natural light)
post traumatic seizures: phenytoin (anticonvulsant)
secondary impairments and medical conditions: due to the high potential of prolonged immobility and collateral injury:
Identify the changes in consciousness with traumatic brain injury.
Coma
Unresponsive wakefulness
Minimally conscious state
What are the 5 levels of consciousness?
coma (different from a medically induced coma): no evidence of awareness
unresponsive wakefulness (vegetative state): there is a sleep-wake cycle; eyes may be open, they might have reflexive squeezing, but they are not responsive
minimally conscious state
5 levels of consciousness
1) alert: responds readily, may be confused
2) lethargic: drowsy
3) obtunded: difficult to arouse, cannot make complete sentences, repeated stimulation
4) stuporous: no verbal response, may moan, responds to pain by moving
5) comatose: no evidence of awareness
What is amnesia? Post traumatic amnesia?
not being able to recall an event (the shorter it lasts, the better the prognosis)
post-traumatic amnesia: length of time between the injury and the time at which the patient is able to consistently remember ongoing events’
the period after a brain injury until the patient can consistently remember ongoing events again.
after brain injury, the person is not yet reliably remembering what is happening right now / from moment to moment
What is the difference between declarative and procedural memory? Implicit Learning?
declarative memory: the ability to recall facts and events from past experiences (remembering a pt's name or the steps of an exercise)
procedural memory: the ability to remember how to perform a task, often referred to as muscle memory; involves practicing previously learned skills
implicit learning: a form on non-cognitive learning that occurs without conscious awareness, like adapting to movement patterns without explicit instruction
What is the Glasgow Coma Scale and how is the score used in treatment?
How does the scoring work and what is the ranges for severe, moderate, and mild?
Sections:
Eye Opening
Spontaneous — 4
To speech — 3
To pain — 2
No response — 1
Best Motor Response
Follows motor commands — 6
Localizes — 5
Withdraws — 4
Abnormal flexion — 3
Extensor response — 2
No response — 1
Verbal Response
Oriented — 5
Confused conversation — 4
Inappropriate words — 3
Incomprehensible sounds — 2
No response — 1
the higher the score, the better the outcome
8 or less (severe)
9 to 12 (moderate)
13 to 15 (mild)
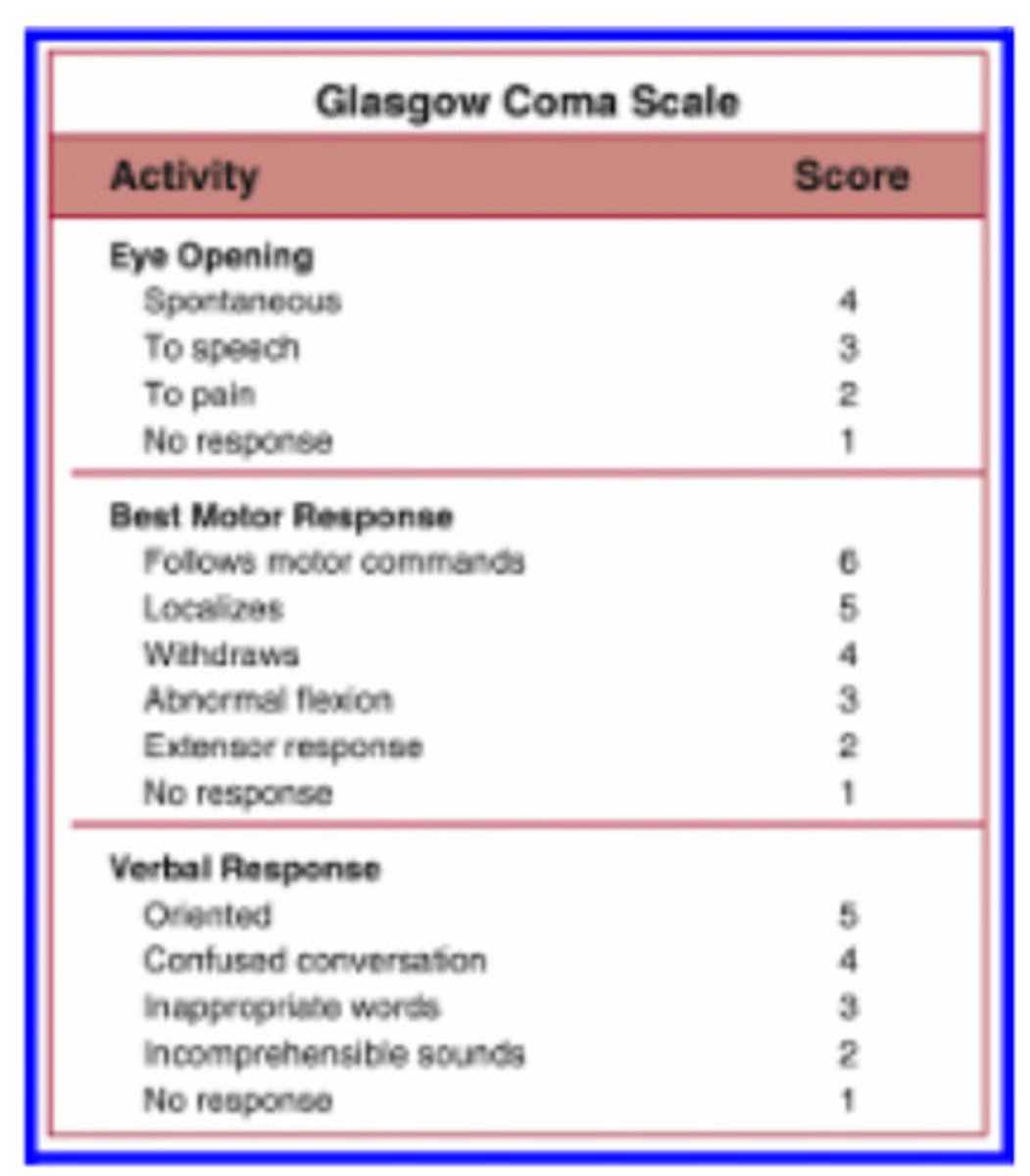
Be familiar with the Rancho Los Amigos Cognitive Functioning Scale. How might it guide therapeutic interactions and the treatment environment?
Set realistic what?
How can communication be modified?
Tailor treatment activities: For lower levels 1 - 3, Mid levels 4 - 6, Higher levels 7 - 8)
people are not textbooks, but knowing the level they fall in this scale can help you be realistic with your treatment and make activities meaningful for the pt
set realistic goals (a Level III won't be able to follow complex commands)
modify communication: use simple cues for lower levels (I-III) and encourage problem-solving in higher levels (VII-VIII)
tailor treatment activities
lower levels (I-III): sensory stimulation, positioning, passive ROM
mid levels (IV-VI): structured tasks, simple functional activities, redirection for agitation
higher levels (VII-VIII): community reintegration, memory aids
optimize the environment: reduce distractions for confused pts (IV-V), introduce real-world challenges for more advanced levels (VII-VIII)
I. No Response
Patient appears to be in a deep sleep and is completely unresponsive to any stimuli.
II. Generalized Response
Patient reacts inconsistently and nonpurposefully to stimuli in a nonspecific manner. Responses are limited and often the same regardless of stimulus presented. Responses may be physiological changes, gross body movements, and/or vocalization.
III. Localized Response
Patient reacts specifically but inconsistently to stimuli. Responses are directly related to the type of stimulus presented. May follow simple commands such as closing eyes or squeezing hand in an inconsistent, delayed manner.
IV. Confused-Agitated
Patient is in a heightened state of activity. Behavior is bizarre and nonpurposeful relative to immediate environment. Does not discriminate among persons or objects; is unable to cooperate directly with treatment efforts. Verbalizations frequently are incoherent and/or inappropriate to the environment; confabulation may be present. Gross attention to environment is very brief; selective attention is often nonexistent. Patient lacks short- and long-term recall.
V. Confused-Inappropriate
Patient is able to respond to simple commands fairly consistently. However, with increased complexity of commands or lack of any external structure, responses are nonpurposeful, random, or fragmented. Demonstrates gross attention to the environment but is highly distractible and lacks ability to focus attention on a specific task. With structure, may be able to converse on a social automatic level for short periods of time. Verbalization is often inappropriate and confabulatory. Memory is severely impaired; often shows inappropriate use of objects; may perform previously learned tasks with structure but is unable to learn new information.
VI. Confused-Appropriate
Patient shows goal-directed behavior but is dependent on external input or direction. Follows simple directions consistently and shows carryover for relearned tasks such as self-care. Responses may be incorrect due to memory problems, but they are appropriate to the situation. Past memories show more depth and detail than recent memory.
VII. Automatic-Appropriate
Patient appears appropriate and oriented within the hospital and home settings; goes through daily routine automatically, but frequently robot-like. Patient shows minimal to no confusion and has shallow recall of activities. Shows carryover for new learning but at a decreased rate. With structure is able to initiate social or recreational activities; judgment remains impaired.
VIII. Purposeful-Appropriate
Patient is able to recall and integrate past and recent events and is aware of and responsive to environment. Shows carryover for new learning and needs no supervision once activities are learned. May continue to show a decreased ability relative to premorbid abilities, abstract reasoning, tolerance for stress, and judgment in emergencies or unusual circumstances
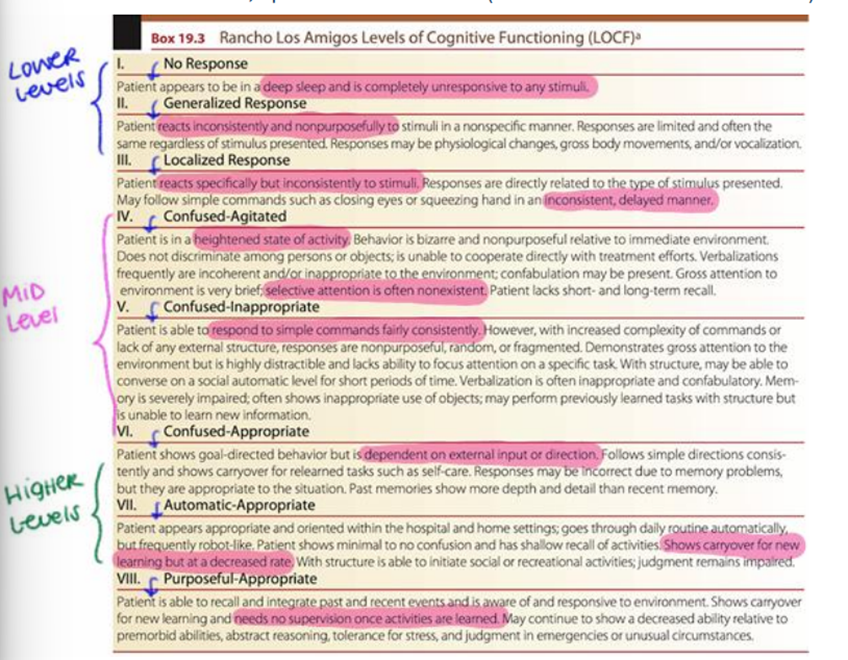
Describe the medical management following a TBI.
When does medical management start? What is included in that management?
Medical interventions include what?
Why would they use sugar or salt?
What team approach is ideal?
medical management starts at the scene: maintain blood flow and oxygen to the brain, stabilize the pt, treat other injuries, avoid elevation of intracranial pressure (pt positioned with head at 30°)
medical interventions: medications, osmotherapy, hypothermia (aka target temperature management), surgical decompression
sugar or salt pull the fluid out of the brain (reduce risk of brain swelling)
interdisciplinary team approach
What is heterotopic ossification and its relationship with TBI and SCI?
What should you be careful about when doing as it can promote HO?
Commonly occurs after (2)? For each, what area does it occur in?
abnormal formation of bone in soft tissues
careful with aggressive stretching! (could promote HO)
-commonly occurs after TBI and SCI
*TBI-related HO: often affects hips, shoulder, elbow
*SCI-related HO: commonly occurs around the hips, shoulder, knee
What are the signs and symptoms of HO? How is it treated?
What medications are used?
What therapy is done?
If its severe and functionally limiting then what can be done?
What therapy can be done to prevent recurrence in some cases?
S/S: pain, decreased ROM, swelling and warmth around the area, joint stiffness
tx & management:
medications: NSAIDs to decrease inflammation, bisphosphonates to slow bone growth
physical therapy: ROM exercises to maintain mobility but avoid aggressive stretching
surgical removal: if severe and functionally limited
radiation therapy: in some cases, used to prevent recurrence
Outline the components of a physical therapy examination for a patient with TBI. Tip: Many of the same treatment procedures are utilized for a patient with TBI or stroke.
Perform a through what? What should you make sure to include?
Find out about the pts (4)?
For a good prognosis what is ideal? What might lead to a bad prognosis?
Assess systems includes?
Assess function includes?
perform thorough history including history of injury, PMHx, results of CT scan/MRI
find out about living situation, PLOF, work/school life, family
good prognosis-> active individual, younger age, no comorbidities
bad prognosis-> diffuse axonal injury (global TBI), decorticate/decerebrate positioning
assess systems:
cognition/ability to follow commands
spasticity/tone
muscle function
coordination
sensation
vital signs
skin integrity
ROM
respiratory function
CNs
assess function:
bed mobility
ambulation
transfers
balance
stairs
wheelchair mobility
Based on a case scenario, prescribe a physical therapy plan of care for a patient with TBI.
What scale can help?
What is the aerobic exercise recommendation for TBI? (Intensity, duration, frequency)
When can they start to do aerobic exercise after a CVA/TBI? They have to be medically ______, if not then?
What is the strength exercise recommendation for TBI? (Intensity, duration, frequency)
What is the Flexibility exercise recommendation for TBI? (Intensity, duration, frequency)
Rancho Los Amigos can help with this!
aerobic exercise recommendation for TBI
intensity: 40-70% of VO2 peak
duration: 20-60 minutes per session
frequency: 3-5 times/wk
can start 8 to 21 days after CVA/TBI if medically stable
if unstable, PT contraindicated
strength exercise recommendation for TBI
intensity: 3 sets of 8-12 reps
duration: 1-2 sets
frequency: 2-3 days/wk
flexibility exercise recommendation for TBI
intensity: to tolerance
duration: 30-60 second hold, 3 times for each muscle/joint
frequency: 2 days/wk (before or after aerobic/strength)
How can spasticity be managed in a patient with a TBI?
Stretching need to be? Hold for how long?
Why WB joint approximation?
Strengthen what muscles
Positioning techniques include what? This prevents?
E stim used for?
Avoid spasticity triggers like?
What should be used t the hands and feet and should you do closed chain exercises and machines or free weights and open chain exercise?
prolonged, slow stretching (hold for 30-60 sec)
WB joint approximation for muscle recruitment
strengthen antagonists (opposite muscles)
positioning techniques: prevents contractures (side-lying, weight-bearing postures)
E-stim (NMES, TENS): stim the muscle opposite of the spastic muscle= reciprocal inhibition
avoiding spasticity triggers (fatigue, stress, infections)
use straps for hands and feet, closed chain exercises and machines instead of free weights and open chain (from lab)
What is serial casting?
When is the cast changed? with each change what is increased? What should you make sure to check? If a cast is not appropriate then what can be used?
non-invasive method used to gradually increase joint mobility and reduce spasticity by applying a series of progressive casts--> a prolonged stretch
the cast is changed every few days (2-5), increasing the stretch incrementally (CHECK FOR SKIN INTEGRITY!)
could use a splint instead if casting is not appropriate
How would you modify the treatment environment to promote positive outcomes for a patient with TBI?
use care NOT to overstimulate (monitor the pt's response)
Be able to apply PNF principles to TBI rehabilitation.
bed mobility
sitting balance
gait training
upper limb recovery
bed mobility: D1 flexion/extension to facilitate rolling
sitting balance: rhythmic stabilization for core control
gait training: D1/D2 LE patterns to improve step initiation & weight shifting
upper limb recovery: slow reversals in D1 flexion/extension for reaching tasks
How can neuroplasticity be promoted in a patient who sustained a TBI?
INTENSITY AND SALIENCE (IMPORTANCE) MATTERS!