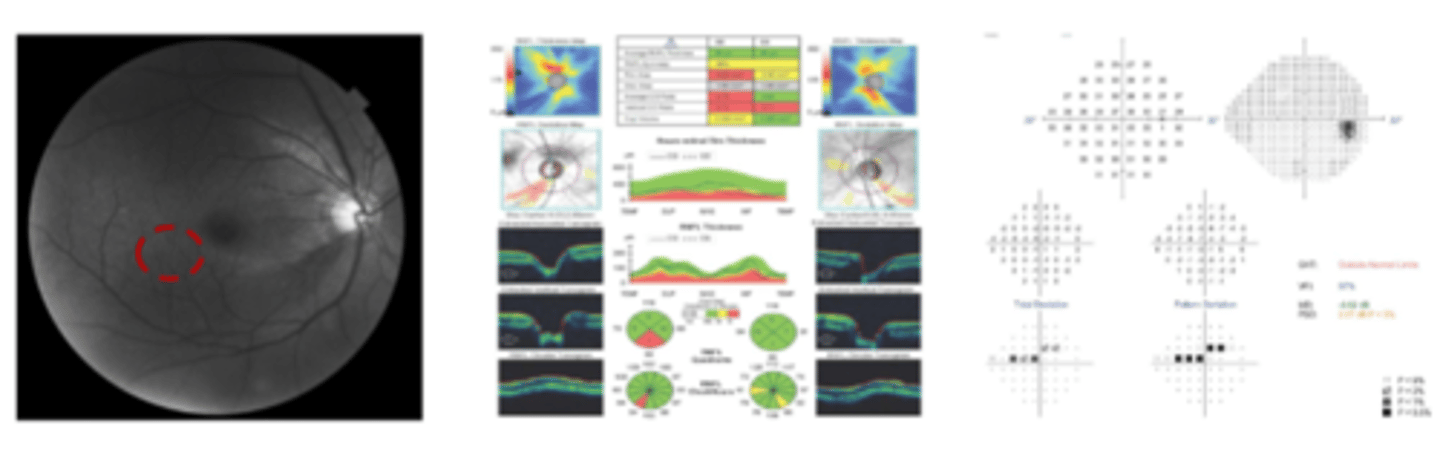
4 Visual Fields
1/70
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
71 Terms
Does damage to the superior or inferior optic disc cross the horizontal raphe?
no, superior and inferior retina do not overlap or cross the horizontal raphe
What is the best way to render an VF unreliable?
lots of false positives
What reliability indices results are you looking for?
Fixation errors <33%
False positive errors <20%
False negative errors <33%
What is a sure-fire sign the VF is unreliable?
pattern standard deviation is worse than total
What should you do if the mean deviation is positive?
look at number of false positives
Why do high false negatives not negate the results of a VF?
high false negatives are seen in severe disease with decrease in overall sensitivity
What is the average dB number for central VF?
30dB
What is the average dB number for peripheral VF?
20dB
What is the dB total deviation plot called on an octopus?
comparison
how does octopus perimetry refer to likelihood for the total deviation (instead of percentages)?
probabilities
What are the pattern deviation plots called on an octopus?
corrected comparison + corrected probabilities
What 4 things cause a generalized decrease in VF sensitivity?
1. small pupils
2. corneal opacities
3. cataracts
4. RE
What does the pattern deviation plot do?
filters out general depressions in the total deviation plot to highlight focal depressions
What does the PSD represent?
the regularity of the hill of vision
What does a low value on PSD mean?
close match between shape of normal hill of vision and shape of patients visual field
"how smooth the hill of vision is"
What is considered statistically significant VF loss?
cluster of 3 or more points that are flagged <5%, with at least one point at the <1% level
What is the minimum VF criterial for diagnosing glaucomatous damage?
meet one of the following:
1. GHT ONL on ≥2 fields
2. cluster of 3 or more non-edge points in a location typical for glaucoma, all of which are <5% and one or more at <1% on 2 consecutive VF
3. PSD <5% of normal on 2 consecutive fields
What parameters aid in staging glaucoma based on VF?
1. # of abnormal points on pattern deviation plot
2. distance of VF loss from fixation
3. depth of VF defect
What criteria must be met to diagnose mild glaucoma off a VF?
ALL MUST BE TRUE:
1. MD better than -6
2. less than 25% of points are depressed below the 5% level and fewer than 10 points are depressed below the 1% level
3. all points in central 5º must have sensitivity ≥15dB
What criteria must be met to diagnose moderate glaucoma off a VF?
only ONE must be true:
1. MD -6 to -12
2. 25-50% of point flagged below 5% level and <25% of points depressed below 1% level
3. one hemifield has a central 5ºn point <15dB but none of those central points have a sensitivity of 0dB
What criteria must be met to diagnose advanced/severe glaucoma off a VF?
only ONE must be true:
1. MD worse than -12
2. >50% of points depressed below 5% or >25% depressed below 1%
3. one point in central 5º is 0dB OR two hemifieds contain a point with sensitivity <15dB within central 5º
What basic defect is seen in early and middle stage glaucoma?
focal defect in hill of vision (rest of vision normal)
What is the role of VF testing in glaucoma?
1. determine the presence of absence of functional loss to differentiate glaucoma from suspect or physiological cupping
2. quantify the degree of functional loss in glaucoma patients to set target IOP
3. assess effectiveness of IOP lowering strategy
4. determine the rate of VF progression to identify patients in need of aggressive IOP control
What challenged are seen in VF testing?
1. subjective testing therefore variability between test (need multiple tests before determining loss is real)
2. some patients unable to perform
3. VF loss not limited to glaucoma, must rule out other causes
What are the common VF loss patterns seen in glaucoma?
1. paracentral defect
2. nasal step
3. arcuate scotoma
What does a paracentral defect look like?
What does a nasal step defect look like?

What causes a paracentral defect?
if NRR thinning starts IT
What type of nasal step is most common? Why?
superior nasal step because IT rim defects are common
How does a nasal step become an advancing nasal step?
as wedge defect expands temporary, the VF near fixation is lost
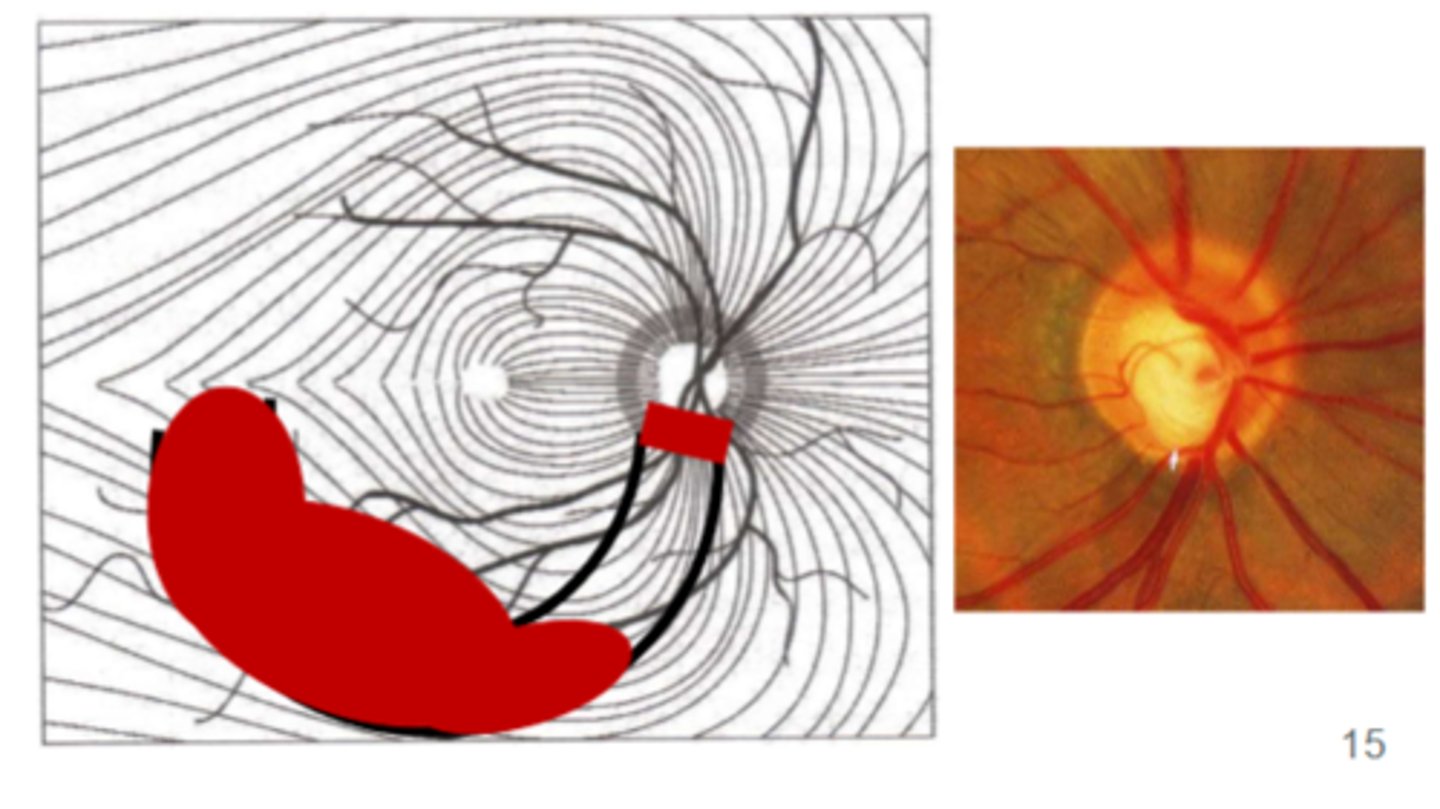
What happens as NRR thinning expands temporally?
begin to lose more RGC closer to fixation (nasal fixation on VF)
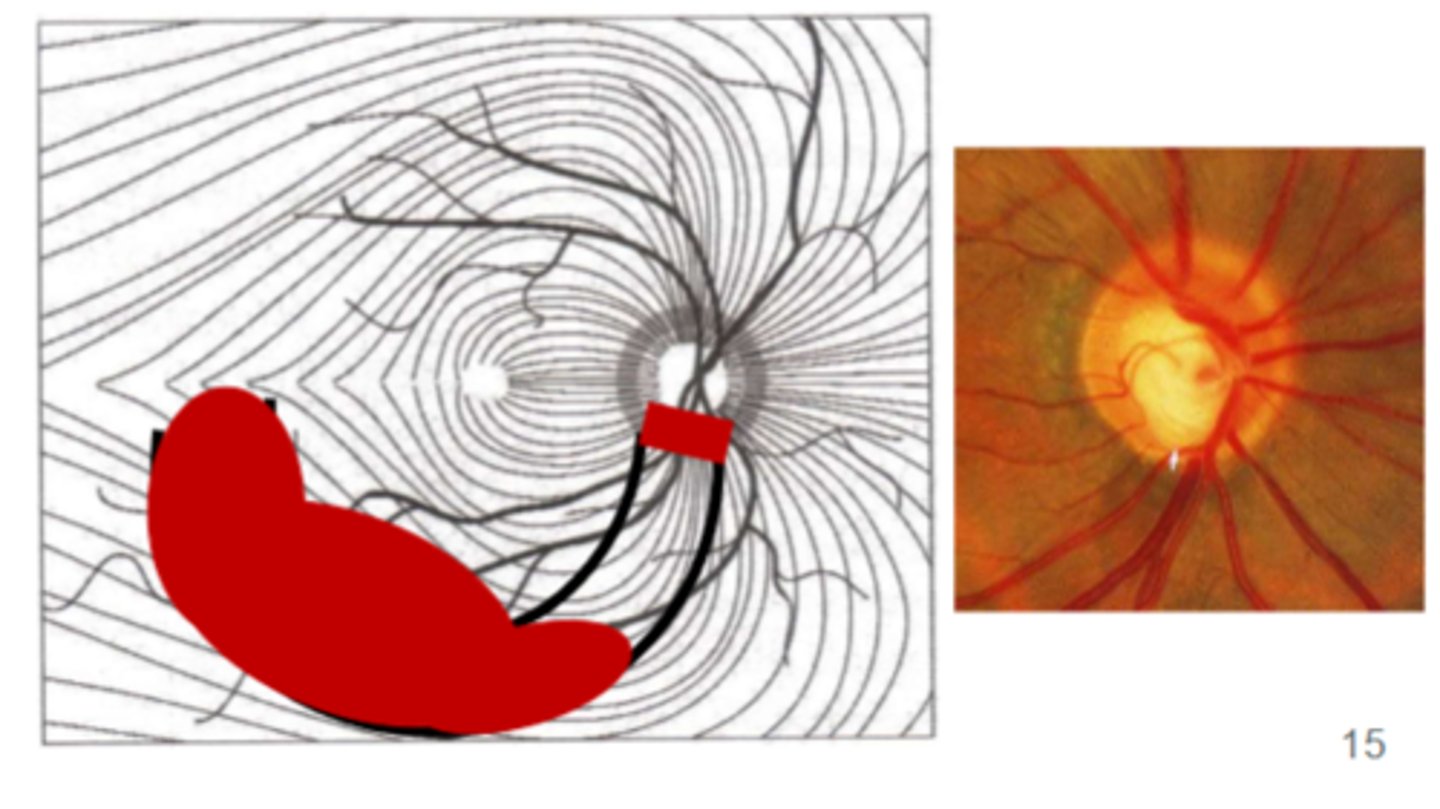
What happens as NRR thinning deepens?
more GCs along NFL bundle dies, getting closer and closer to disc --> eventual arcuate scotoma

What's another name for an arcuate scotoma? And what does it look like?
Bjerrum scotoma

What does the VF look like in end-stage glaucoma?
central island of vision only
image - double arcuate scotoma

What trial lens do you use for Humphrey VF?
distance rx + 3.00 add
cyl lenses ≥1.25D of cyl, otherwise SE
Yuhas says "...correct for cyl only if cyl is dominant or close to in the prescription..."
What trial lens do you use for Octopus 600 VF?
wear habitual correction or use distance trial lenses (no near add)
no cyl lenses so cannot run w/o habitual if cyl ≥1.25D
What is the preferred VF pattern for non-glaucomatous loss?
30-2
What is the preferred VF pattern for moderate glaucoma?
24-2
How many degrees are the points of the 24-2 separated by?
6°
What's the difference between the 24-2 and 24-2C?
24-2C, 10 extra points near fixation added to 24-2
What is the preferred VF pattern for severe glaucoma?
10-2
How many degrees are the points of the 10-2 separated by?
2°
What is the 10-2 equivalent on the octopus?
M-pattern
When do you use the 10-2 in glaucoma?
1. severe glaucoma
2. early glaucoma if patient have GCA loss, I or IT RNFL/NRR thinning
3. NTG glaucoma with central island of vision
What is the octopus equivalent of SITA standard?
dynamic
What is the octopus equivalent of SITA fast?
TOP
What does the SITA standard algorithm do?
uses a 4dB staircase followed by a 2dB staircase
crosses threshold twice
How does the SITA fast algorithm compare to SITA standard?
crosses threshold once rather than twice
How long does SITA standard take?
5-7 mins
How long does SITA fast take?
3-5 mins
What does the GPA do?
tracks vision overtime
What VF tests can you use GPA for?
24-2 or 30-2 only
What is needed for GPA?
2 baseline tests
What does a half triangle mean on GPA event analysis?
test point has significantly worsened on two consecutive tests compare to baseline
What does possible progression mean on GPA event analysis?
≥3 test points have significantly worsened on 2 consecutive tests compared to baseline
What does likely progression mean on GPA event analysis?
≥3 test point has significantly worsened on three consecutive tests compare to baseline
What does full triangle mean on GPA event analysis?
test points have significantly worsened on three consecutive tests compare to baseline
Which is a reliable marker of progression, possible progression or likely progression?
likely progression
What does the VFI do?
represents the entire VF as a % of normal (another way to describe the mean deviation
What rate of change of the VFI indicated progression of disease and requires aggressive treatment?
anything >2%
What should you do the VFI if you start a new therapy?
restart the baseline
What is the normal rate of change of VFI due to aging?
1%/year
What VFI value indicated disability?
30%
What MD value indicates disability?
-22 dB
What are the common false results of VF?
1. trial lens scotoma (most common with 30-2)
2. abnormal GHT not caused by glaucoma
3. considering result of each eye separately
When should you/how often should you run VF tests?
-3 tests per year in first 2 years of diagnosis (eur glaucoma society)
-2 tests within first 6 months and 2 more tests within next 18 months (world glaucoma association)
How often do low to high risk glaucoma suspects need perimetry?
low - every yr
medium to high - every 6 months
How does medical insurance limit VF testing?
limits VF testing to every 3 months
When should you run a 10-2 for mild to moderate glaucoma?
1. after establishing baseline of 24-2
2. IT NRR thinning or NFL loss
3. thinning on GCA
4. flagged points adjacent to fixation on 24-2
5. NTG
How does frequency doubling technology (FDT) work?
stimulates magnocellualr RGC pathway by using a high temporal flicker frequency
How does SWAP work?
stimulates S-cones