HTHSCI 2H03 - Week #4: Pharmacology of the Endocrine System (pituitary, thyroid, adrenal) & Pharmacotherapy Management of Diabetes Mellitus
1/67
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
68 Terms
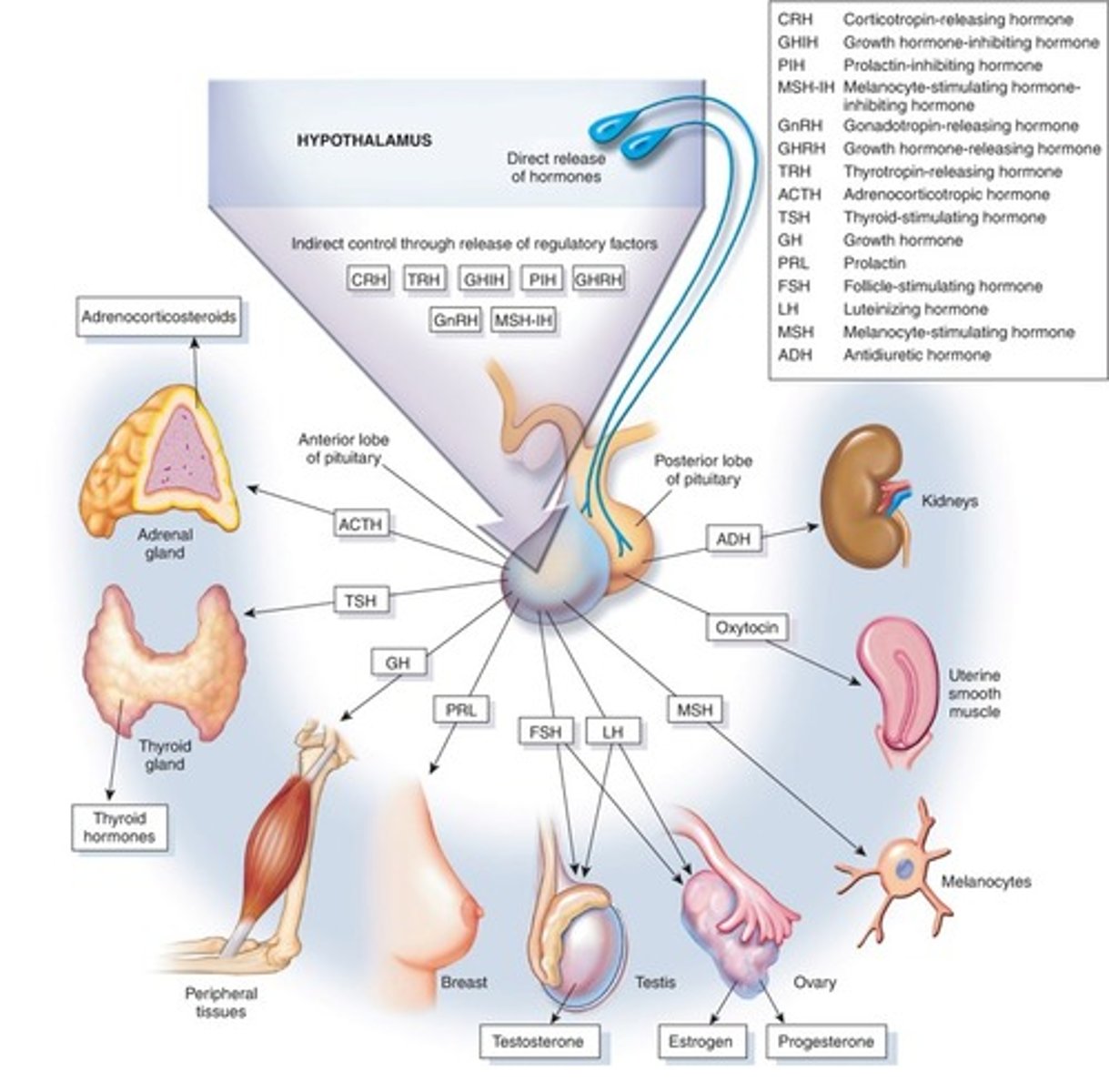
Hypothalamus vs. Pituitary Gland
- The hypothalamus and pituitary gland regulate the function of numerous endocrine glands.
Hypothalamus
- Secretes hormones that regulate the function of the anterior pituitary.
- Controls the posterior pituitary through neuronal signaling.
Hypothalamus Functions Diagram
Pituitary Endocrine Disorders
- Occur as a result of tumour formation, congenital defect, surgery, radiation therapy, infection, hemorrhage or other injury.
- Many hormones are produced by the pituitary; only a few are used clinically.
Growth Hormone (Somatotropin)
- Anterior pituitary hormone that stimulates growth & metabolism.
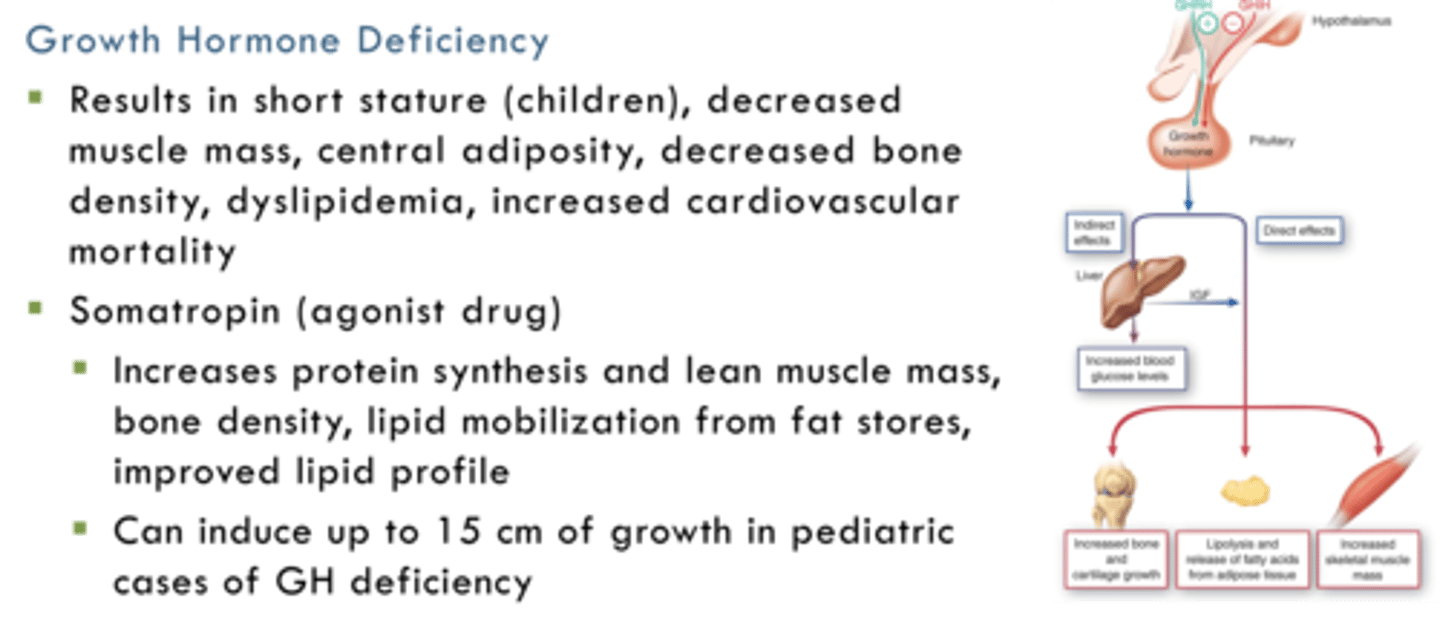
Growth Hormone Deficiency
- Results in short stature (children), decreased muscle mass, central adiposity, decreased bone density, dyslipidemia, increased cardiovascular mortality.
Somatropin (agonist drug):
- Increases protein synthesis and lean muscle mass, bone density, lipid mobilization from fat stores, improved lipid profile.
- Can induce up to 15 cm of growth in pediatric cases of GH deficiency.
Growth Hormone Deficiency Diagram
Antidiuretic Hormone
- Stored and released by posterior pituitary in response to increased serum osmolality.
- ADH acts on the kidneys to increase water resorption.
Acromegaly
- Associated with benign pituitary tumours (pituitary adenoma) causing excessive growth hormone production and secretion.
- Headache, visual disturbances.
- Enlarged heart, hands, feet, tongue, skull, nose, and lips, deep voice, sleep disorders.
- Fatigue, excessive sweating, arthritis.
- Usually treated with surgery, medication and/or radiation therapy.
Octreotide - Growth Hormone Antagonist
- Pharmacologically related to somatostatin (GHIH) and inhibits the secretion of growth hormone and reduces tumor size.
Pegvisomant - Growth Hormone Receptor Antagonist
- Blocks binding of somatotropin at growth hormone receptors in target tissues.
Growth Hormone Antagonists
- Appropriate for individuals with inadequate response to surgery and/or radiation therapy, or who are not a suitable candidate for surgery.
Antidiuretic Hormone (ADH)
- Also known as vasopressin (endogenous ligand/hormone).
- Deficiency causes diabetes insipidus; rare condition resulting in dilute urine and constant thirst.
Desmopressin - ADH
- Agonist drug.
- Available as a nasal spray, SC, IV and PO; prolonged duration of action.
- Does not exert the same effects on blood pressure as vasopressin (a potent vasoconstrictor).
- Blood pressure, body weight (twice a week), fluid intake and urine output must be monitored.
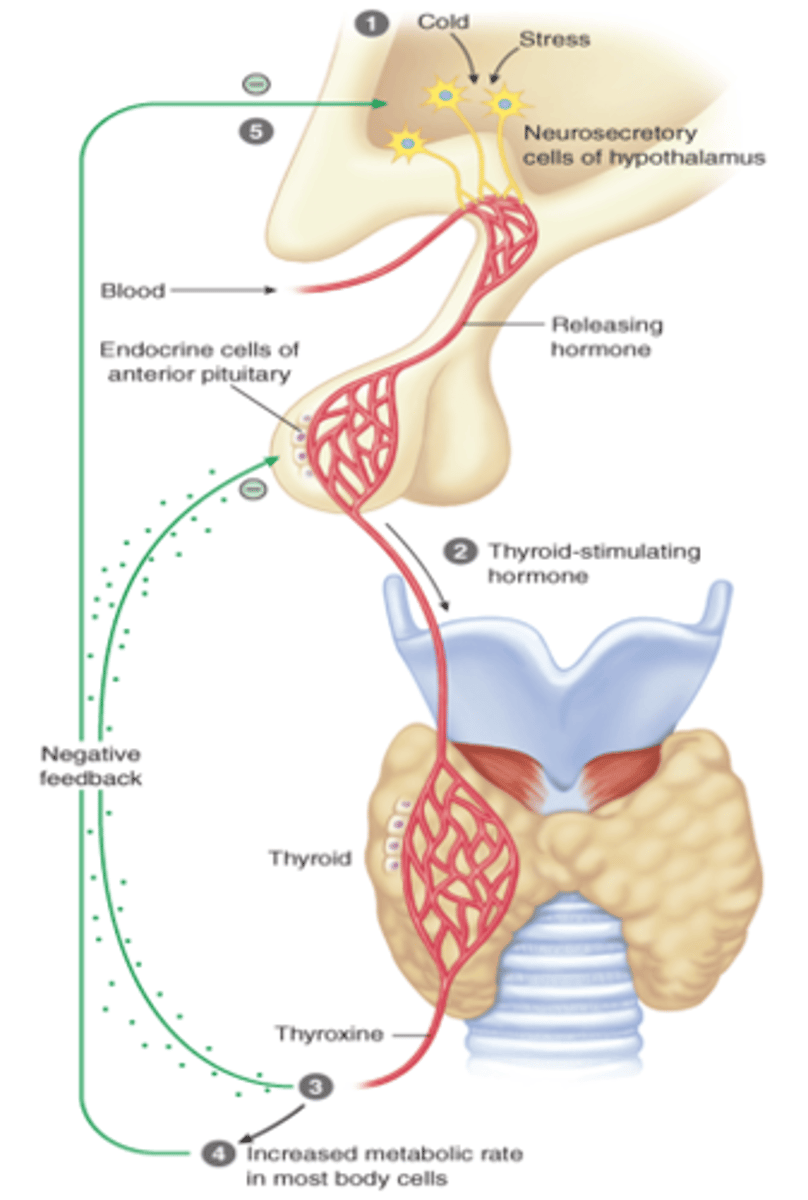
Thyroid Hormone/Gland
- The hypothalamus produces thyrotropin-releasing hormone (TRH) which stimulates the anterior pituitary to produce thyroid stimulating hormone (TSH).
- Thyroid stimulating hormone induces the thyroid to produce and secrete triiodothyronine (T3 ~10%) and thyroxine (T4 ~90%).
- T4 is converted to T3 in target tissues.
- Thyroid hormones regulate basal metabolic rate and impact the function of almost all major organ systems.
Thyroid Gland Diagram
Primary Hypothyroidism
- Inactive thyroid gland commonly caused by an autoimmune disease "Hashimoto's thyroiditis"; women (especially of menopausal age) are at increased risk.
- Low serum T4, elevated TSH, increased antithyroid antibody.
Secondary & Tertiary Hypothyroidism
- Low TSH from anterior pituitary gland or TRH from hypothalamus.
Hypothyroidism
- Drug induced hypothyroidism e.g. lithium.
- Gestational hypothyroidism associated with low IQ in children; monitor TSH levels in 1st trimester of pregnancy.
Hyperthyroidism vs. Hypothyroidism
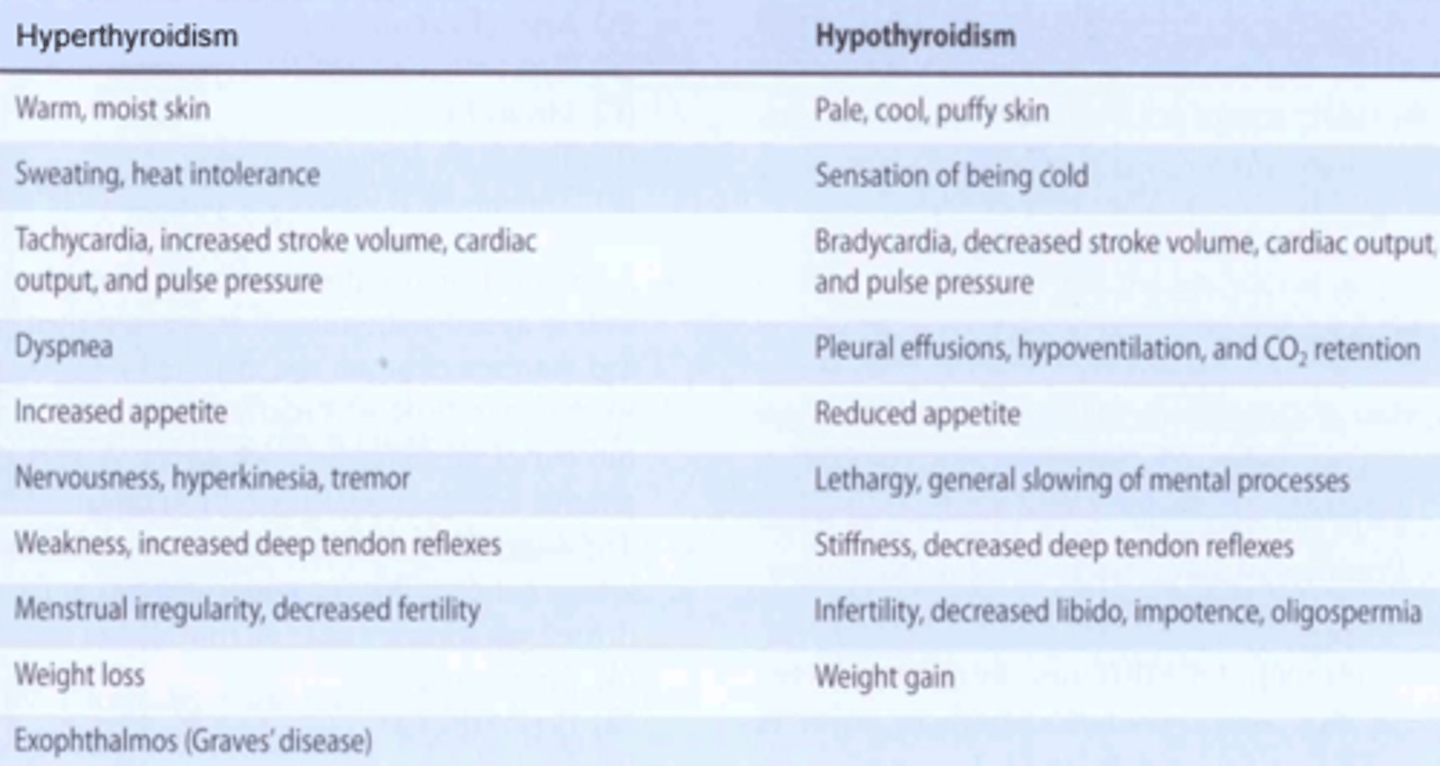
Levothyroxine (Synthroid)
- Synthetic form of thyroxine T4, administered once daily PO.
- Reverses the effects of hypothyroidism: Increased metabolism, weight loss, improved tolerance to environmental temperature, increased activity levels, increased pulse rate.
Regular monitoring of serum TSH levels required:
- Narrow therapeutic index; increased cardiovascular demand.
- Some adverse effects: sweating, insomnia, rapid pulse, dyspnea, irritability, fever and weight loss.
- Numerous drug-drug interactions.
Primary Hyperthyroidism
- Grave's disease; autoimmune disorder - body develops antibodies (thyroid stimulating immunoglobulins) that activate the TSH receptor; women also at increased risk.
- TSH levels will be low, despite high thyroid hormone levels.
Secondary Hyperthyroidism
- Increased TSH secretion from anterior pituitary resulting in increased T4 production and release.
Methimazole & Propylthiouracil (PTU)
- Hyperthyroidism.
- Thioamides that inhibit synthesis of thyroid hormone.
- PTU also disrupts conversion of T4 to T3 in target tissues, so faster onset.
- PO administration; regular monitoring of serum TSH levels required.
- While therapeutic effect of methimazole can take 3 - 4 weeks; convenience in daily dosing; avoids hepatotoxicity and leukopenia (associated with PTU).
Radioactive Iodine
- Hyperthyroidism.
- Single dose to permanently destroys follicular cells in overactive thyroid gland; commonly used in cases of thyroid cancer.
Treatments for Hyperthyroidism
- Surgery can be used to reduce thyroid size in patients with breathing or swallowing problems (due to goiter), uptake of radioactive iodine is low, or malignancy is suspected.
- Drug therapy is often used prior to surgery to reduce the risk of thyrotoxicosis and to decrease vascularity of the gland.
- Other medications (beta adrenergic antagonists, and calcium channel blockers) are used as adjunctive agents to treat some of the symptoms (tremor, anxiety, palpitations, increased heart rate).
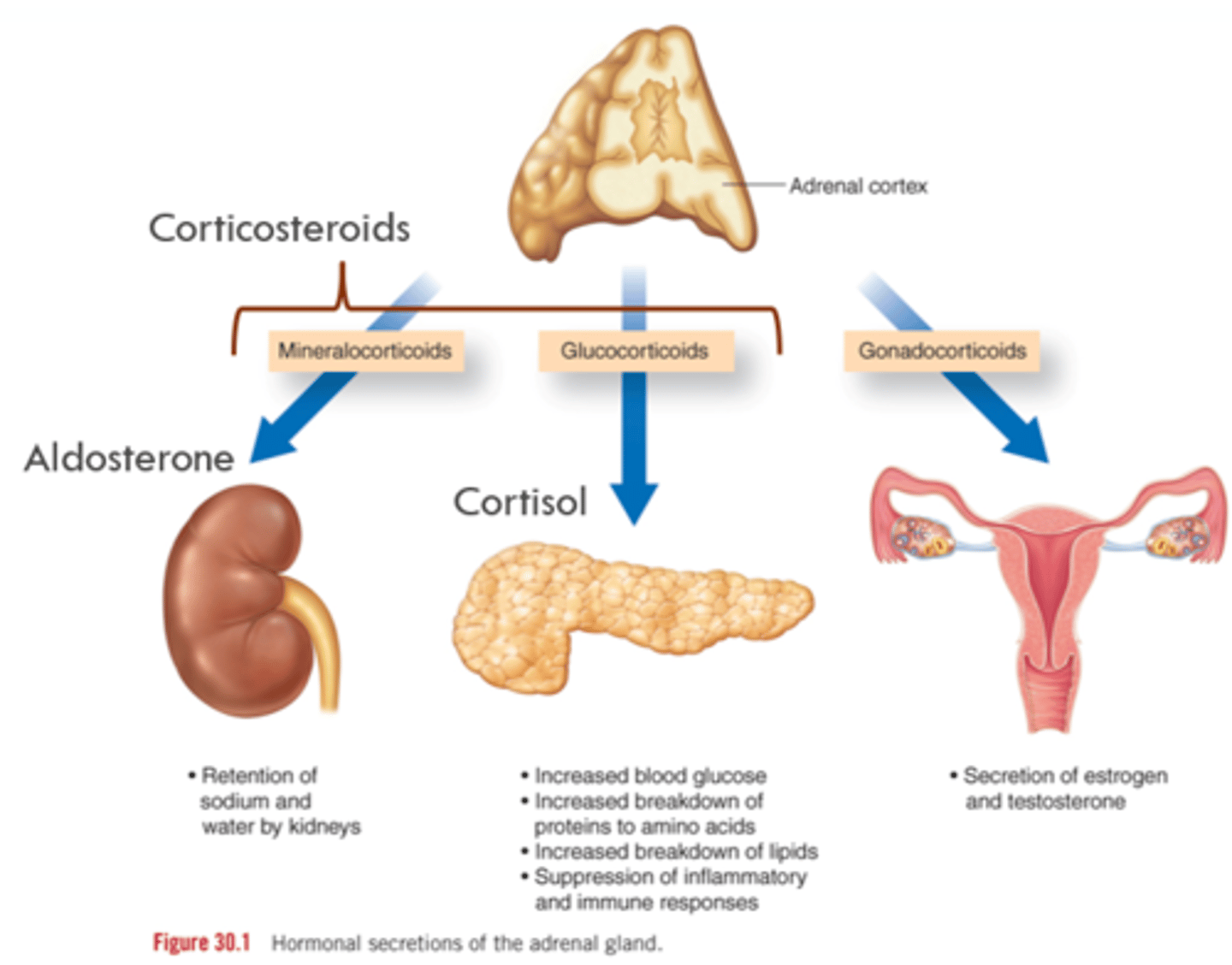
Physiology of Adrenal Glands
HPA Axis of Adrenal Glands
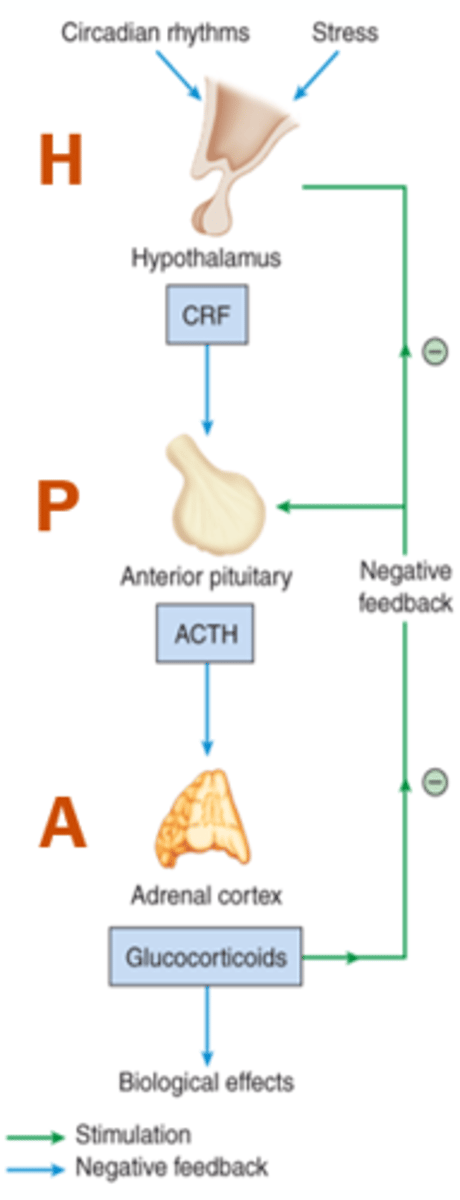
Glucocorticoids (Cortisol)
- Increase blood glucose levels.
- Increase breakdown of lipids and proteins.
- Suppress immune and inflammatory responses, stabilize mast cells.
- Increase vascular smooth muscle sensitivity to NE and angiotensin II.
- Affect mood and CNS excitability.
- Decrease bone density.
- Bronchodilation.
Mineralocorticoids (Aldosterone)
- Regulate plasma volume by conserving sodium and water and promoting potassium excretion by the kidney.
Primary Adrenal Insufficiency (Addison's Disease)
- Hyposecretion of corticosteroids due to autoimmune destruction of both adrenal glands.
- High ACTH, low cortisol, low aldosterone.
Secondary Adrenal Insufficiency
- Inadequate secretion of ACTH from the anterior pituitary OR;
- Chronic, long-term corticosteroid therapy leading to adrenal atrophy.
Symptoms of Adrenal Insufficiency
- Hypoglycemia, fatigue, muscle weakness, hypotension, anorexia, diarrhea, dehydration, decreased plasma sodium levels.
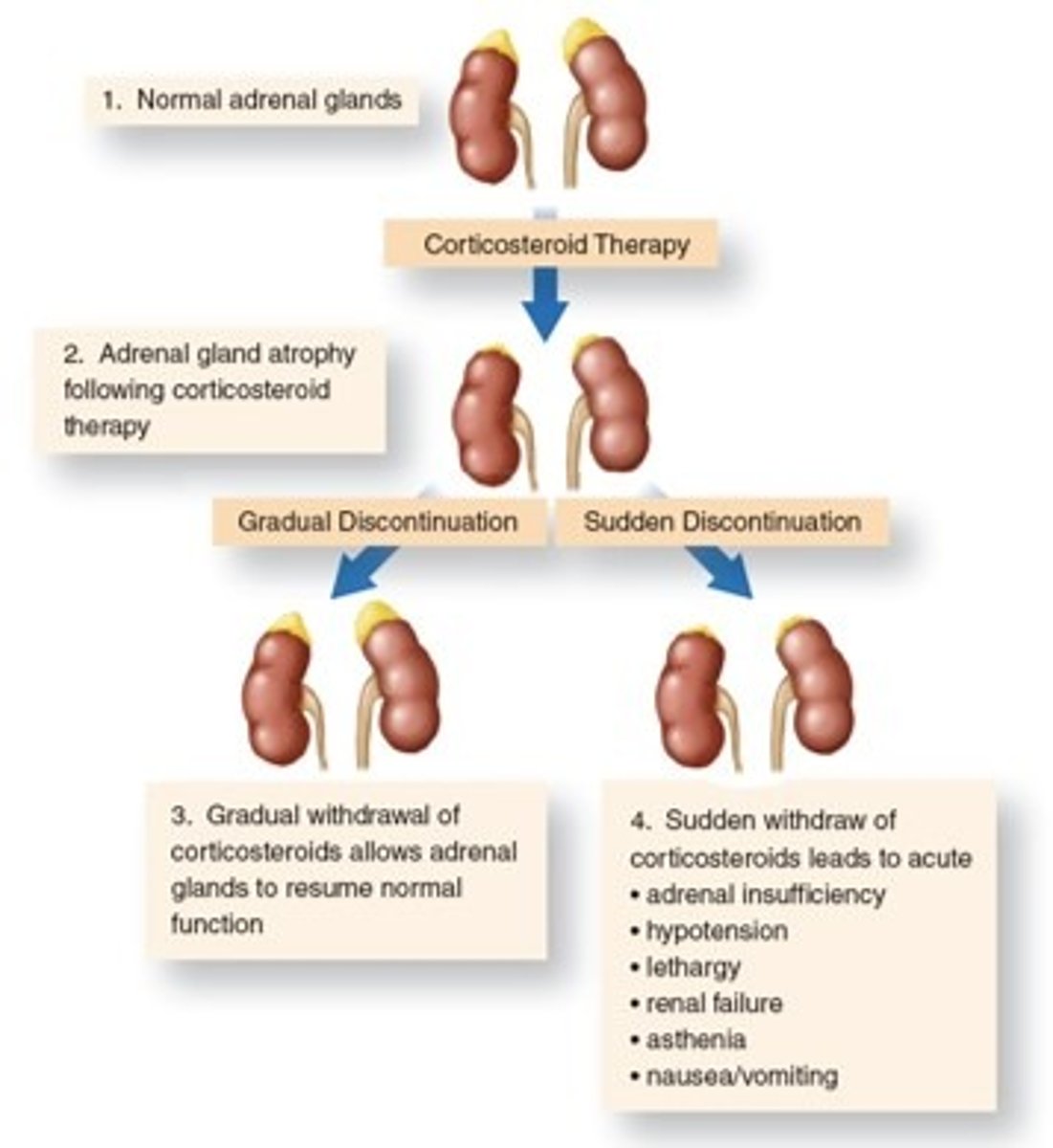
Secondary Adrenocortical Insufficiency
- In cases of high dose, chronic, systemic corticosteroid therapy, the drug should be withdrawn slowly, over the course of several months, to allow recovery of normal adrenal function.
- Acute insufficiency requires IV hydrocortisone/dexamethasone therapy to prevent hypovolemic shock and death.
- Mineralocorticoid replacement with fludrocortisone may also be required.
Secondary Adrenocortical Insufficiency Diagram
Non-Adrenal Disorders
- Corticosteroids/Glucocorticoids are potent anti-inflammatory and immunosuppressive drugs prescribed for many non-adrenal conditions.
Non-Adrenal Disorders Examples
Corticosteroid/Glucocorticoid Drugs
- Well absorbed & distributed; highly bound to plasma proteins.
- Metabolized by liver; excreted by kidneys.
- Crosses placenta, enters breast milk.
- Exert dose, duration & route dependent adverse effects which include osteoporosis, mood changes, edema, hypertension, fluid retention, hyperglycemia, hyperlipidemia, F&E imbalances, myopathies.
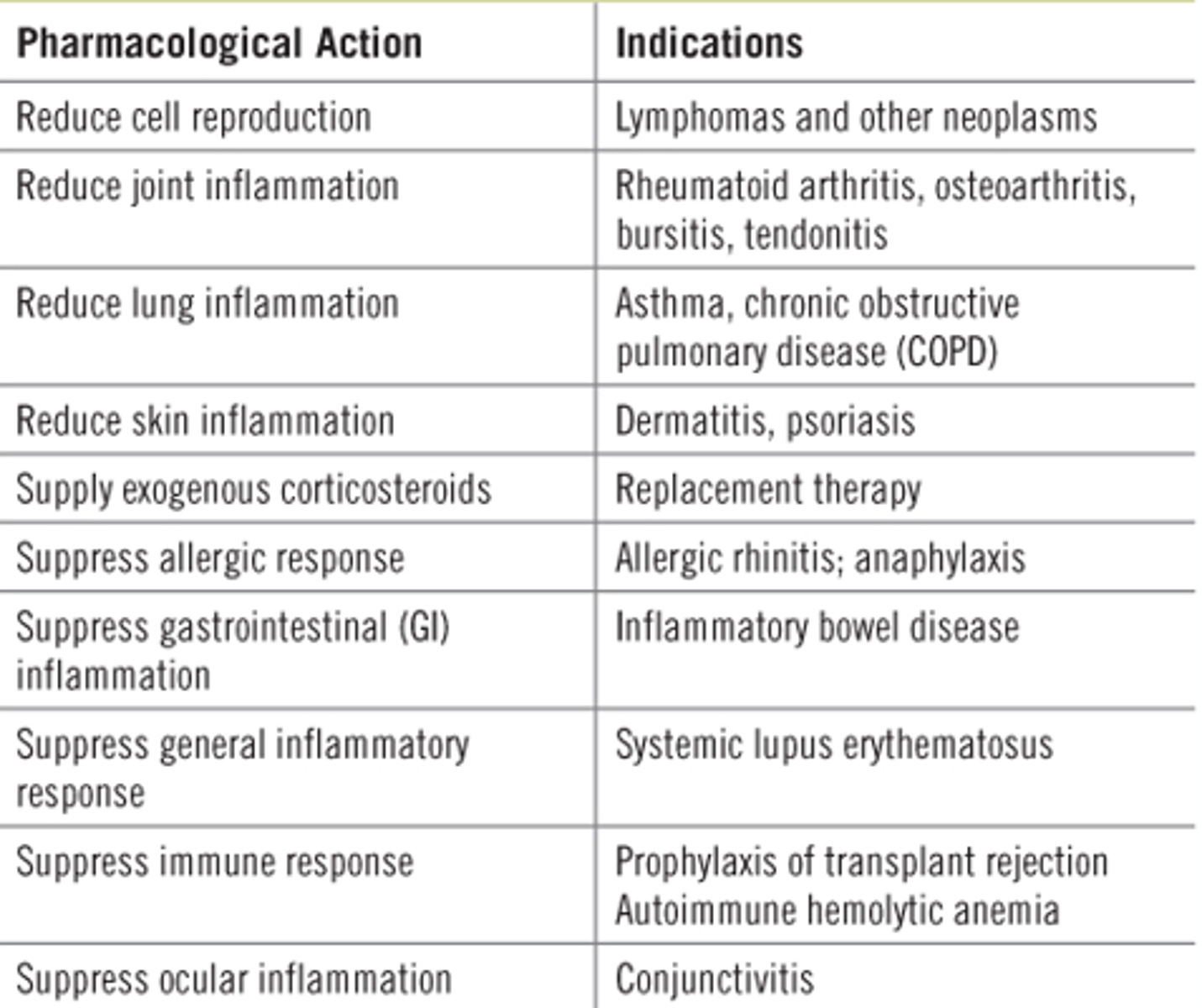
Actions and Indicators for Corticosteroids
Cushing's Syndrome
- Metabolic disorder caused by excess secretion of corticosteroids due to excess amounts of ACTH (aka Cushing's Disease).
- Prolonged, high dose, systemic glucocorticoid or corticosteroid drug therapy.
Cushing's Syndrome Presentation
- Redistribution of body fat to face, shoulders, trunk and abdomen.
- Increased risk of infection and decreased wound healing.
- Mood and personality changes.
- Adrenal atrophy and osteoporosis.
Cushing's Syndrome Treatment
- Surgery; if associated with adrenal or ectopic tumour.
- Slow and gradual reduction in glucocorticoid/corticosteroid dose.
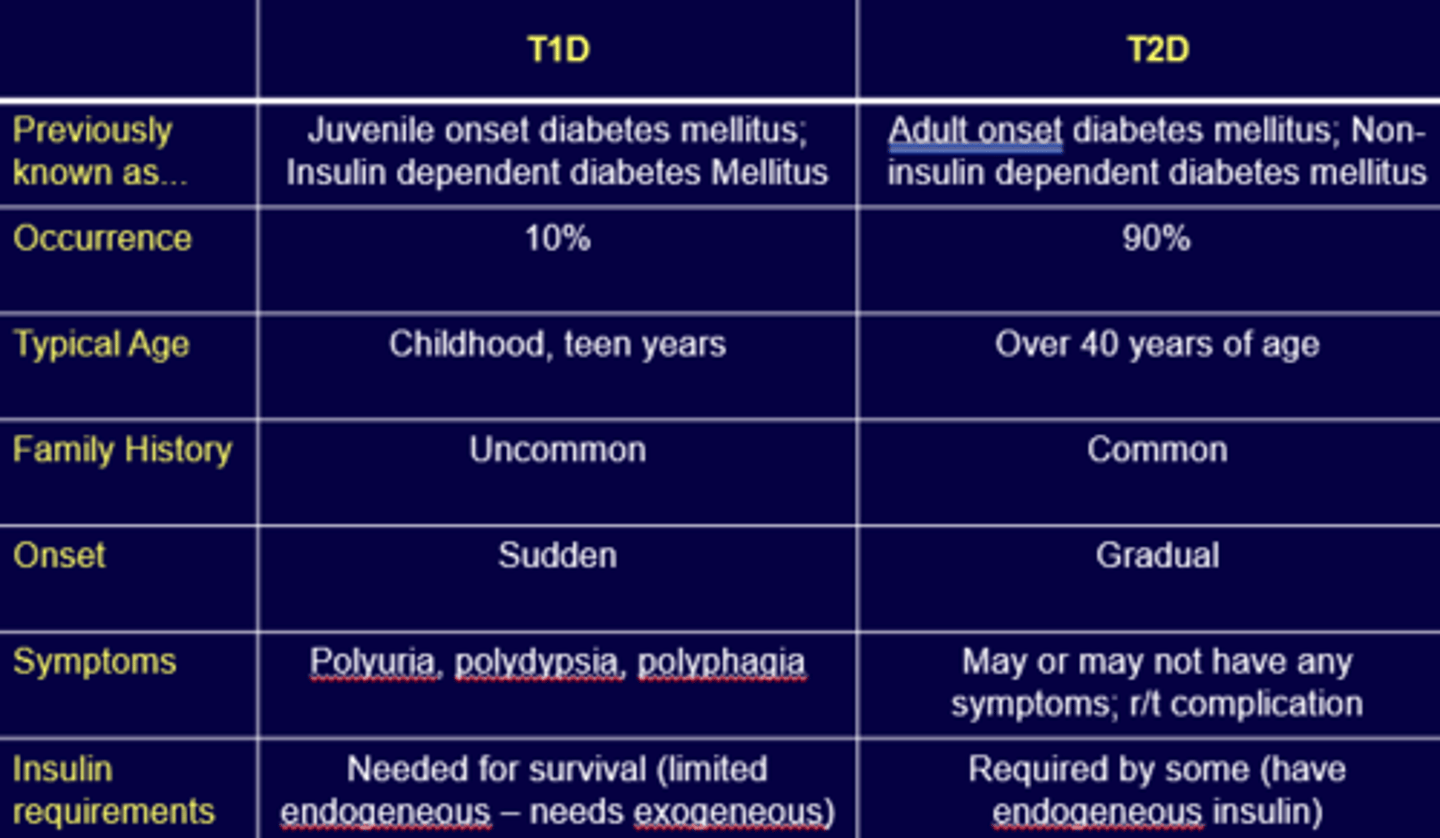
Differences Between T1D & T2D
People who Discovered Insulin (1923)
- Sir Fredrick Banting.
- J.J.R. Macleod.
- Charles Best.
- James Collip.
Pharmacotherapy for T1D
- Insulin (exogenous).
- Type of insulin: Depends on insulin delivery system.
Best practices include:
–Multiple daily injections (MDI) – need 2 types.
–Continuous Subcutaneous Insulin Infusions (CSII) (ex. pumps, artificial pancreas).
- Mimic endogenous insulin secretion; basal and bolus to manage blood glucose levels.
*Inhaled insulin not yet available.
*Watch for basal (cloudy) and bolus (clear) insulin.
T1D - BASAL
- 'Background' insulin that addresses hepatic glucose production.
T1D - BOLUS
- Secreted in response to energy intake and glucose.
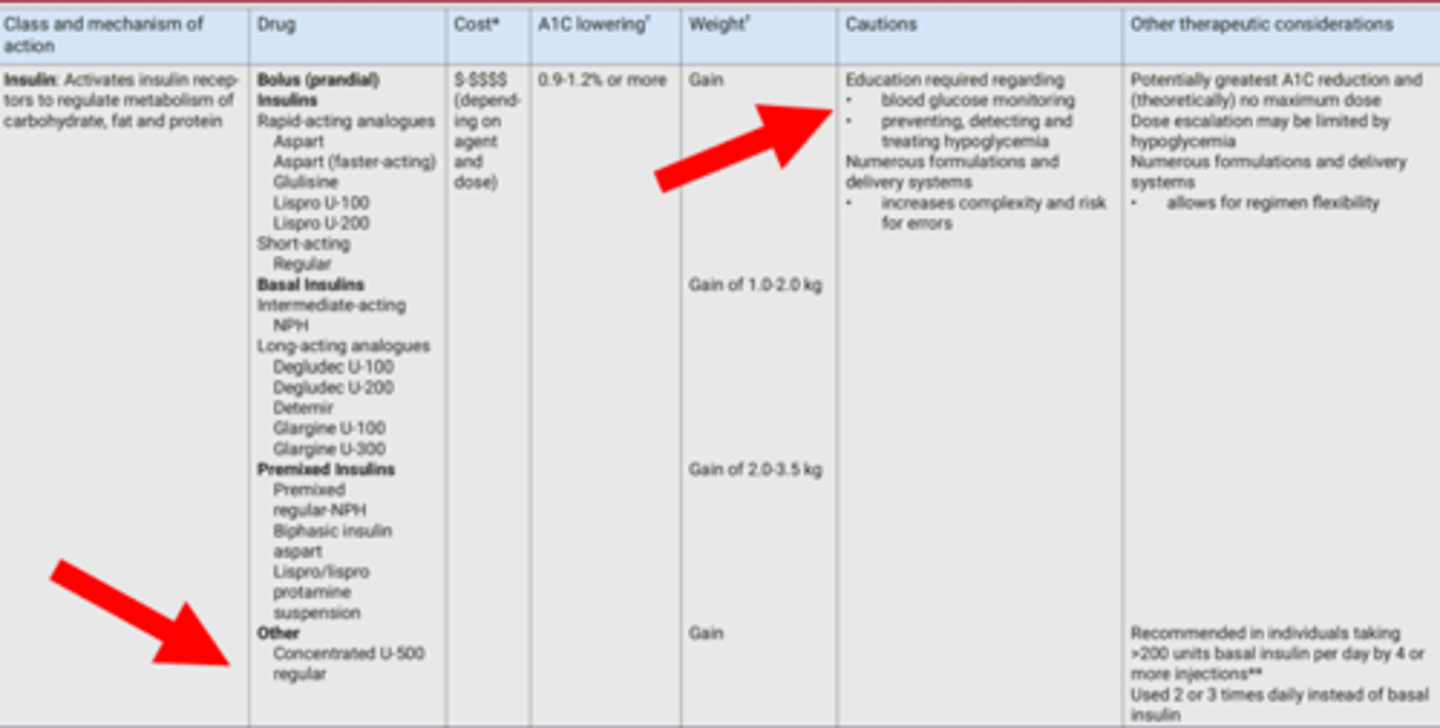
About Insulin
Insulin Considerations
- Basal-bolus (prandial) insulin regimens (MDI) or CSII are best insulin regimens for T1DM.
- Insulin regimens should be tailored to the individual.
- All individuals with T1DM should be counselled about the risk, prevention and treatment of hypoglycemia.
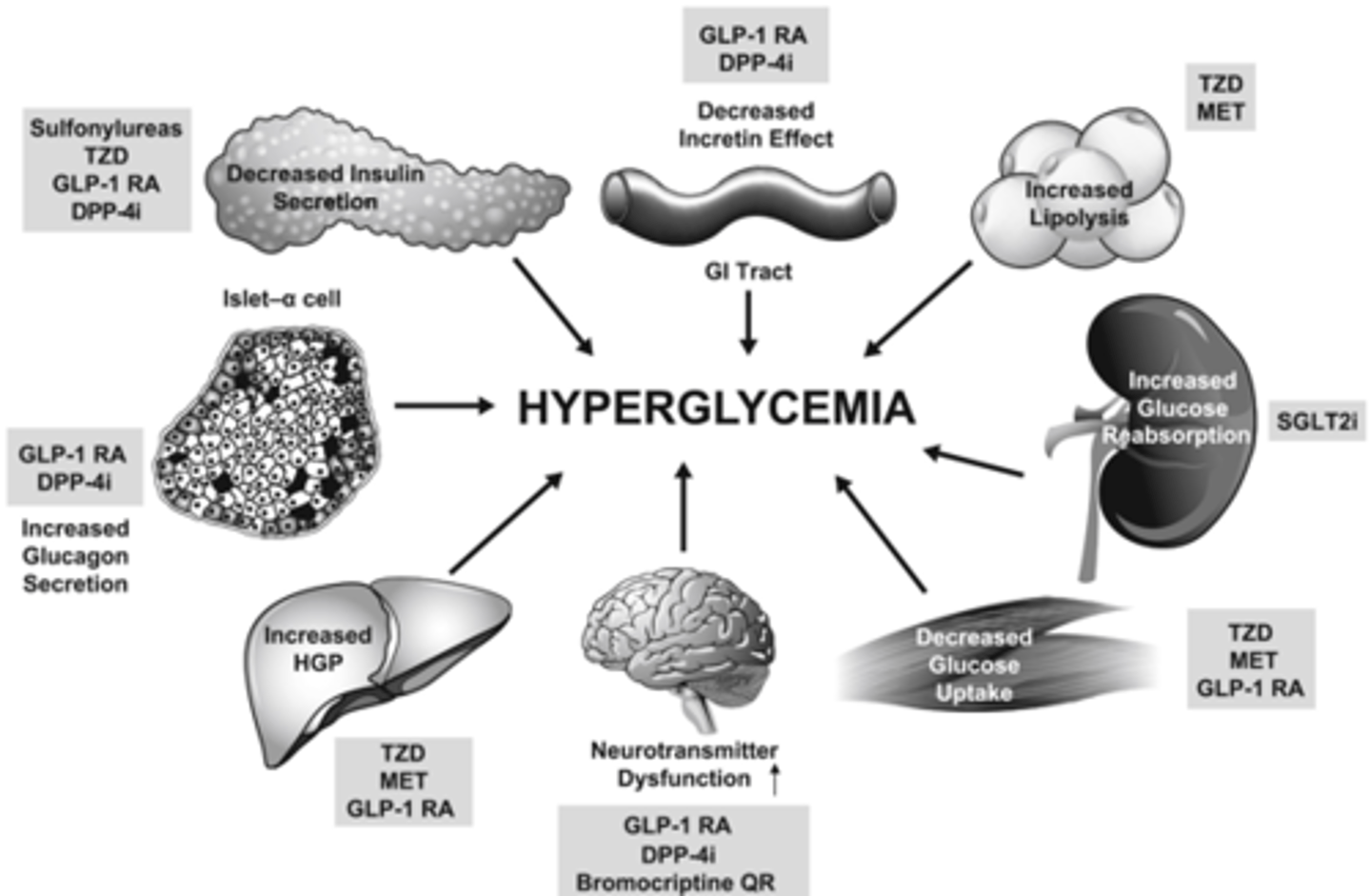
Hyperglycemia - T2D
Insulin/GLP1 Fixed-Ratio Combinations

Biguanide Considerations

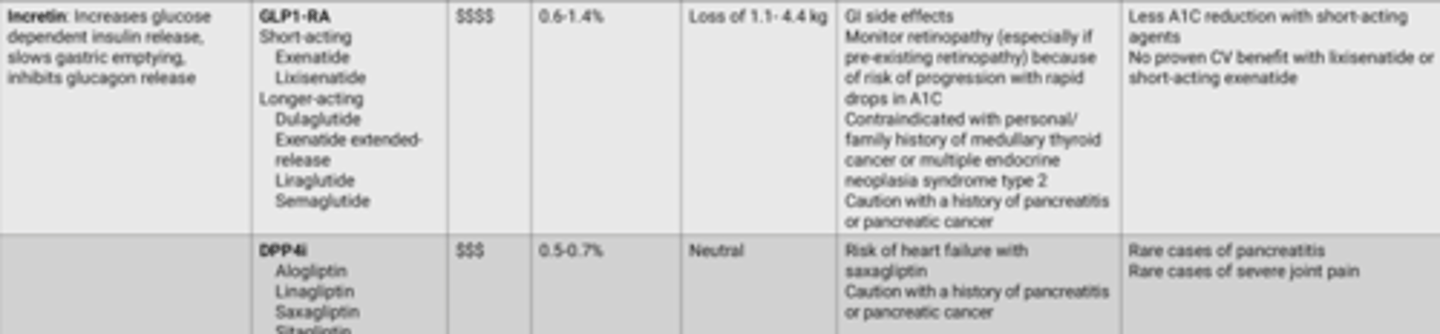
Incretin Considerations
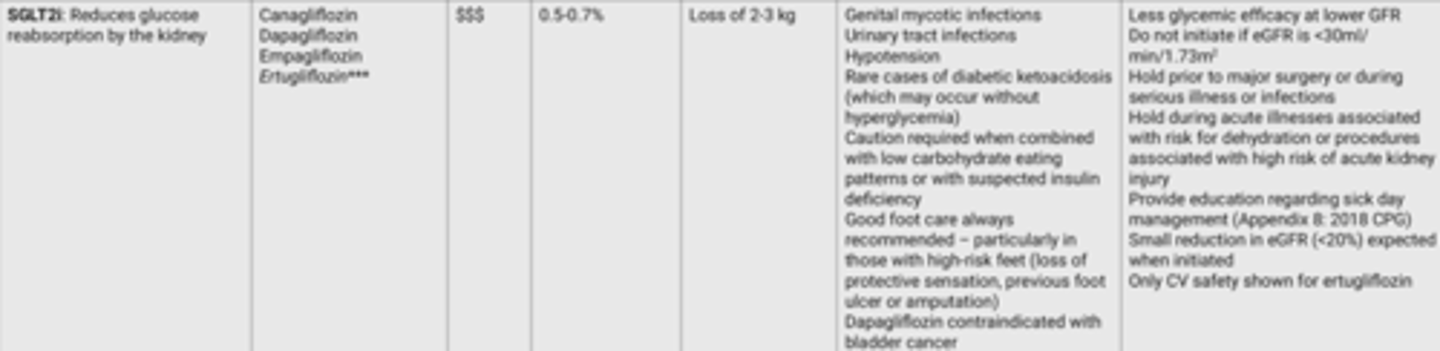
SGLT2i Considerations
Alpha-Glucosidase Inhibitor Considerations

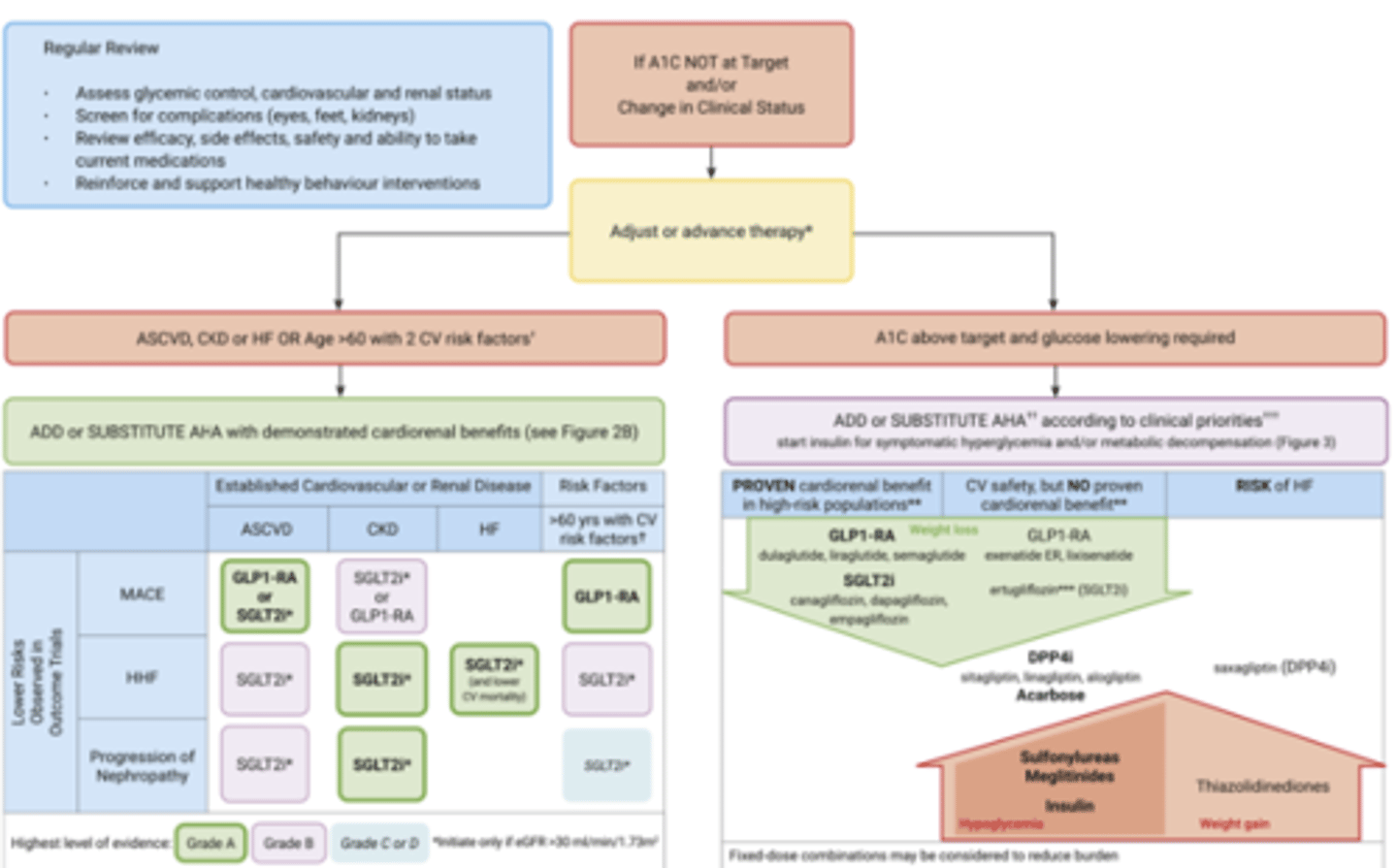
Pharmacologic Glycemic Management of Type 2 Diabetes in Adults
Insulin Secretagogue Considerations

Meglitinides Considerations

Thiazolidinedione Considerations

Pharmacotherapy for T2D
- Oral vs. Injectable (does not mean insulin).
- Classes address different action mechanisms.
- Combination therapy address multiple pathophysiological defects.
- Efficacy of a drug = old… A1C.
- Effectiveness of a drug = weight, A1C, hypo, CV risk.
- Patient centred = adherence, cost, SE.
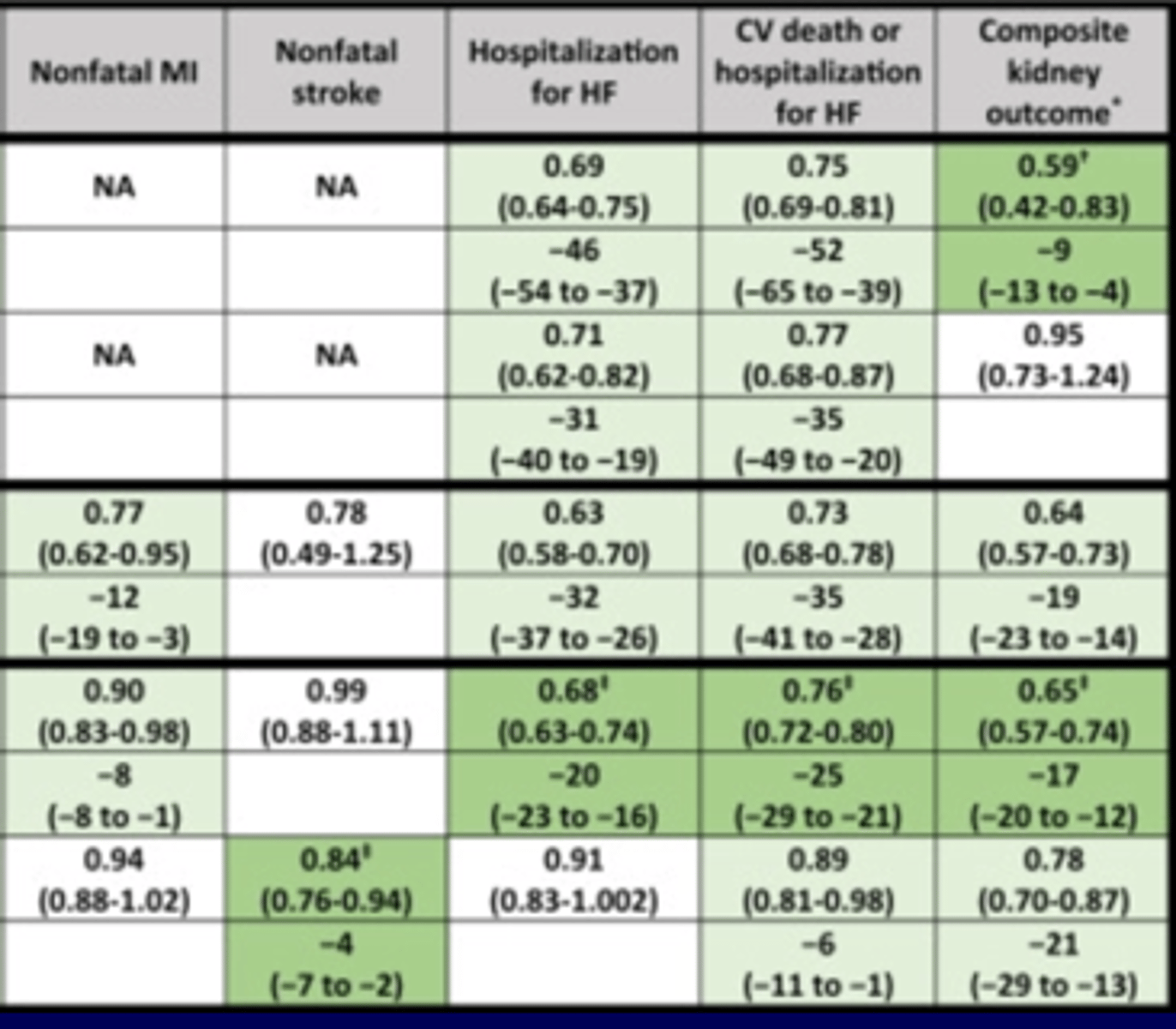
T2D - Study Populations with Heart Failure, Chronic Kidney Disease, or Type 2 Diabetes #1
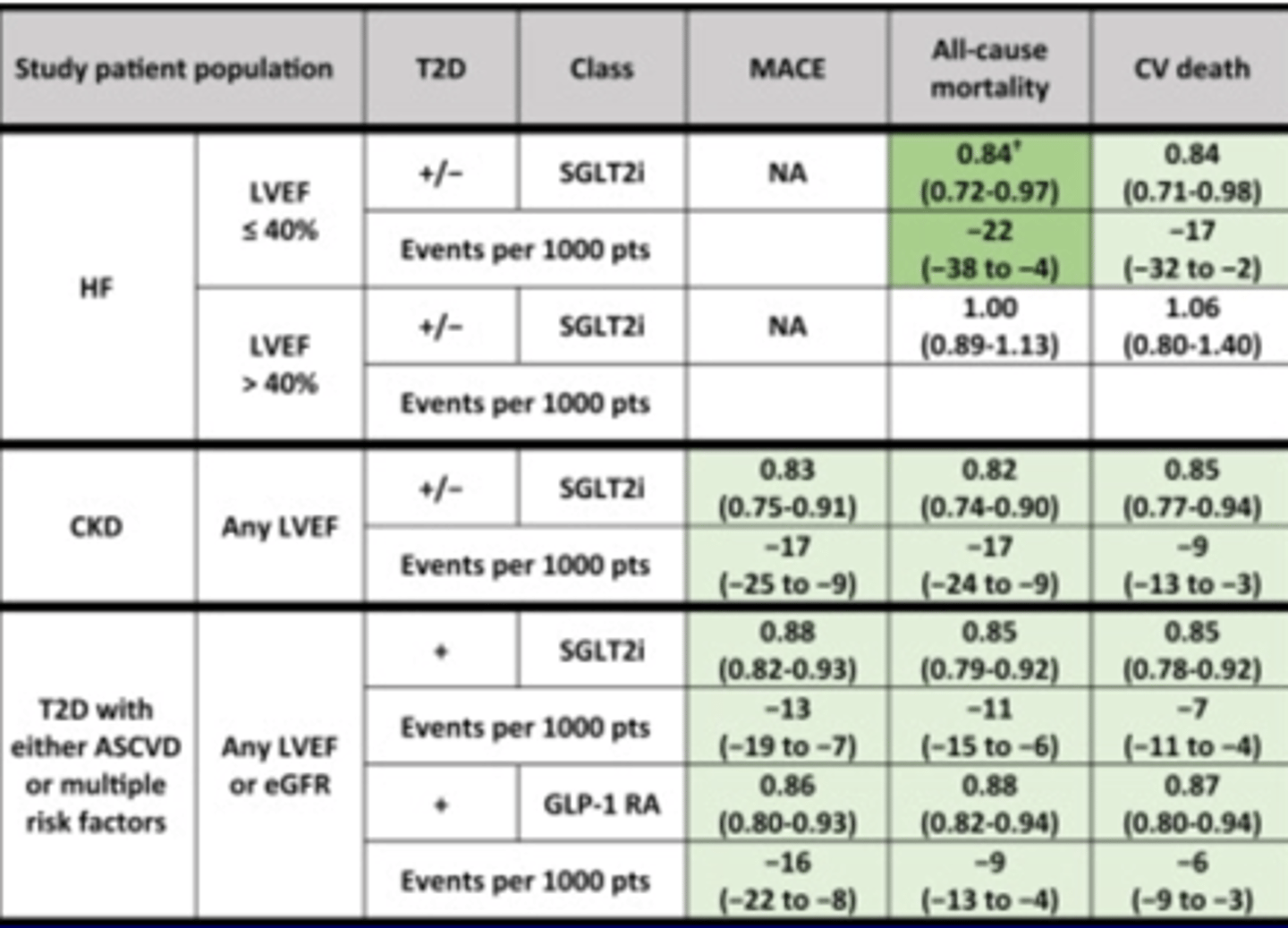
T2D - Study Populations with Heart Failure, Chronic Kidney Disease, or Type 2 Diabetes #2
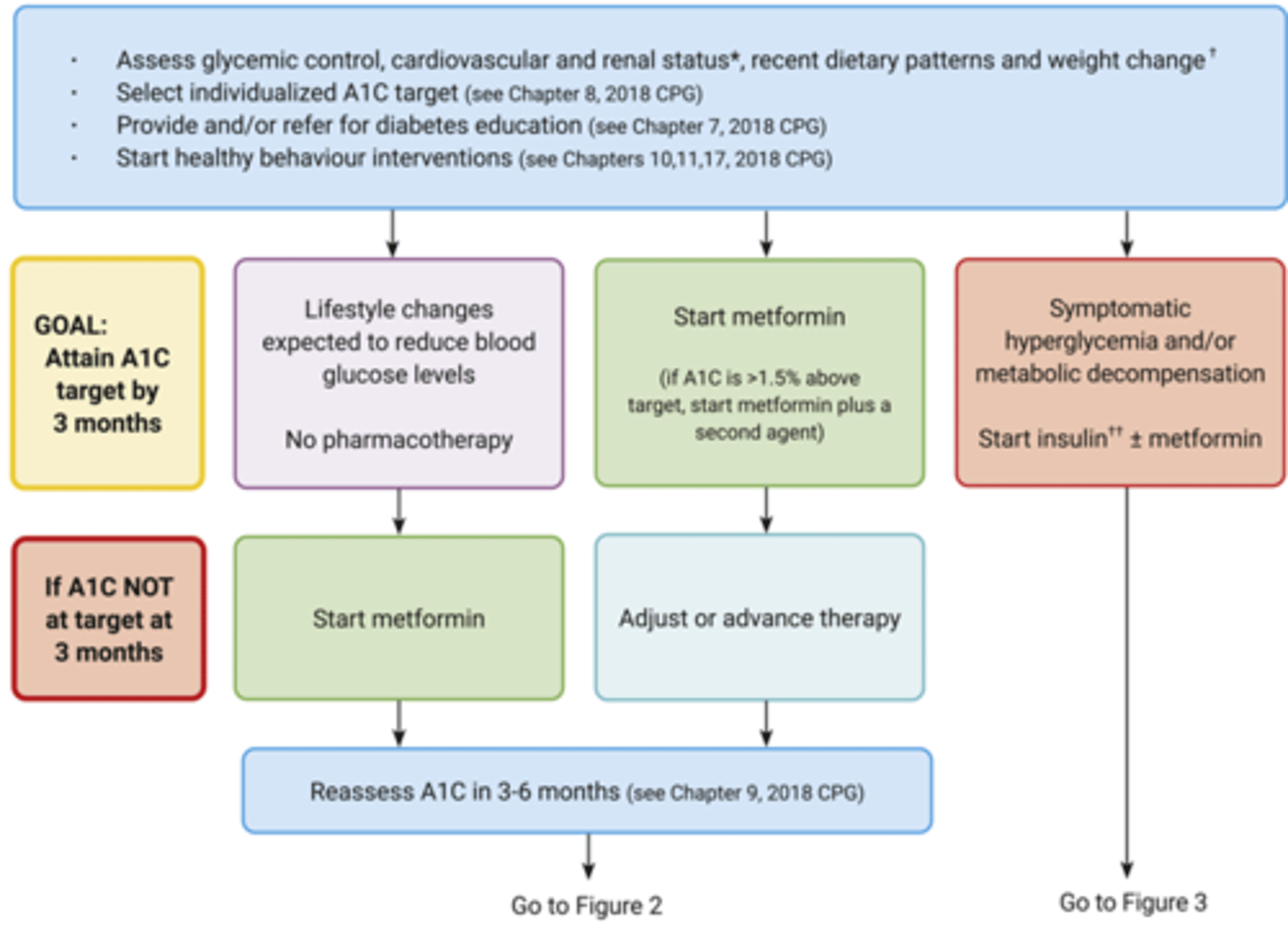
T2D - At Diagnosis
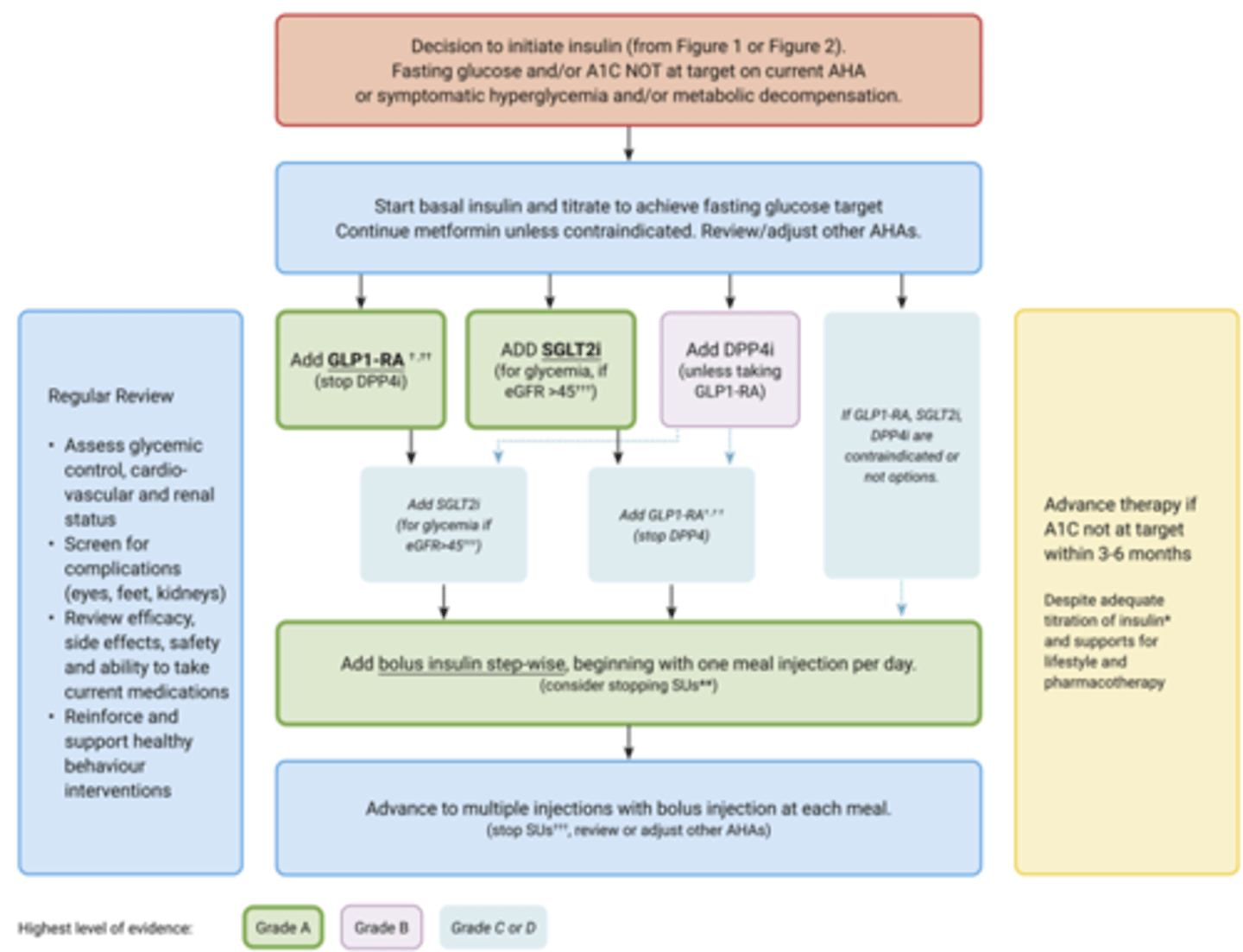
T2D - Ongoing Insulin Management
T2D - Require Insulin
Cardiovascular Risk Factor's
- Smoking (tobacco use).
- Hypertension (untreated BP greater than or equal to 140/9; or current antihypertensive therapy).
- Dyslipidemia (Untreated LDL > 3.4 mmol/L OR HDL-C < 1.0 mmol/L (men) and < 1.3 mmol/L (women) OR triglyceride > 2.3 mmol/L; Current lipid-lowering therapy).
- Central obesity.
T2D Patient Considerations
- Degree of hyperglycemia.
- Risk of hypoglycemia.
- Overweight or obese.
- Comorbidities (renal, hepatic issues).
- Preferences (medication adherence)
- Access to treatment.
- BG lowering efficacy and durability.
- Risk of inducing hypoglycemia.
- Effect on weight.
- Contraindications and/or side effects.
- Cost/coverage.
Glycemic Management in Adults with Type 1 Diabetes