Case 4: Ivan Netter
1/22
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
23 Terms
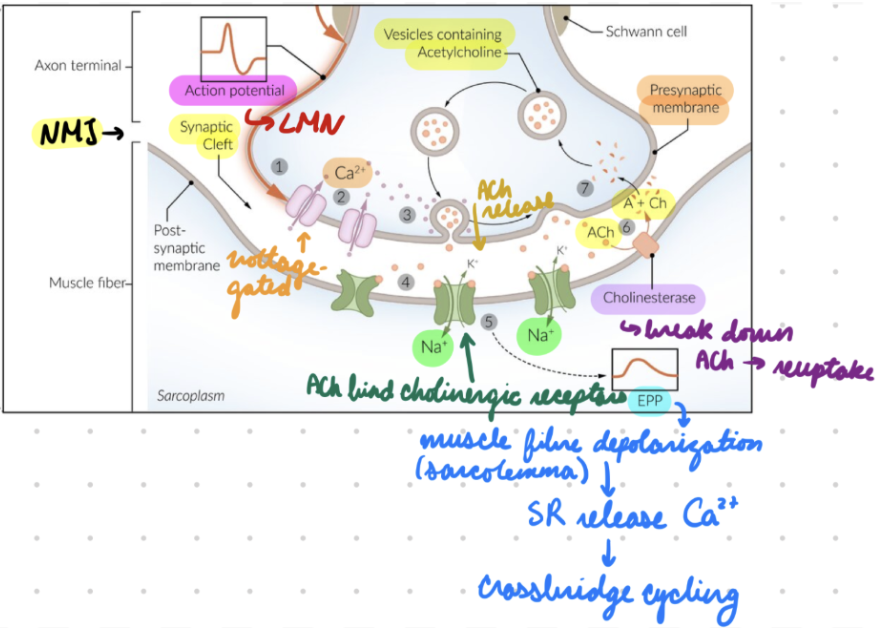
Neuromuscular Junction (NMJ): Description
Synapse between LMN + skeletal muscle
Involved in excitation-contraction coupling
NMJ: LMN
Presynaptic neuron
Receive AP from axon = Presynapatic membrane depolarize = Open voltage-gated Ca2+ channels
Ca2+ influx into presynaptic terminal = Vesicles containing ACh fuse with presynaptic membrane = Release ACh into synaptic cleft
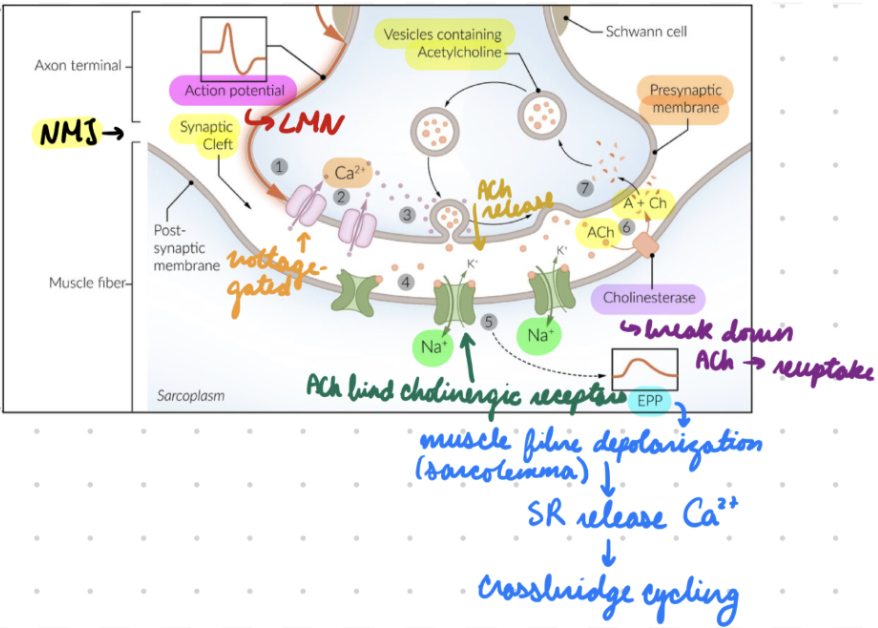
NMJ: Skeletal Muscle
ACh bind cholinergic nicotinic receptors on postsynaptic membrane (muscle motor end plate) = Na+ enter muscle
Muscle sarcolemma depolarize = End-plate potential (EPP) → T-tubules
Voltage-sensitive dihydropyridine receptors (DHPR) in T-tubules + ryanodine receptors in SR open = Release Ca2+ from SR into sarcoplasm (intracellular)
Tropomyosin unbind myosin-binding site on actin = Crossbridge cycling + muscle contraction
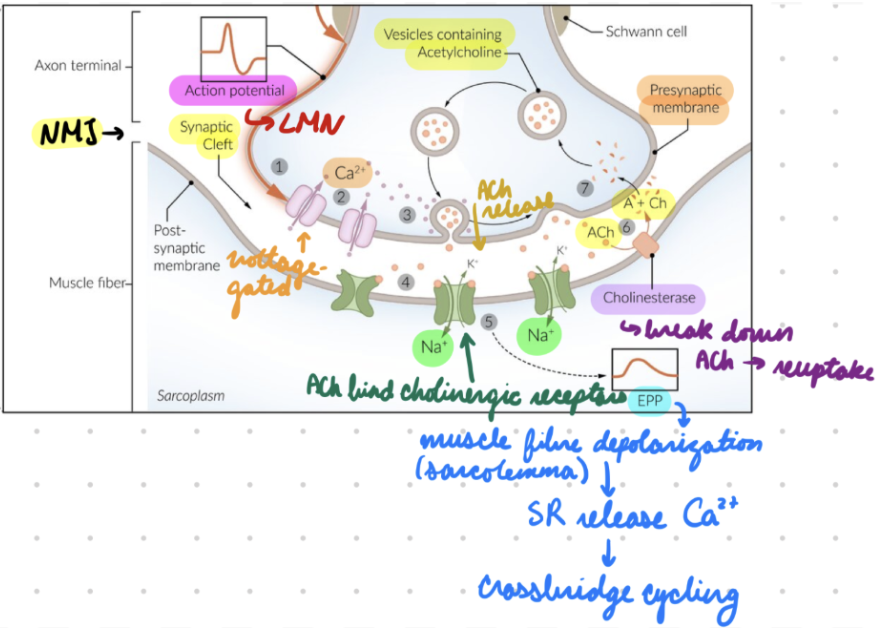
NMJ: Synaptic Cleft
Acetylcholinesterase (AChE) breaks down ACh → Acetate + choline
Choline reuptake into presynaptic membrane = Resynthesize ACh
NMJ Disorders: Etiology
Autoimmune: Myasthenia gravis
Paraneoplastic: Lambert-Eaton myasthenic syndrome (LEMS)
Autoimmune condition = Abs against presynaptic Ca2+ channels = Inhibit ACh release
From small cell lung cancer
Toxic:
Botulism
Cholinergic poisoning (organophosphates)
Tick paralysis
Snake venom
NMJ Disorders: Clinical Presentation
Muscle weakness: Lack of strength
Muscle fatigue: Inability to continue after multiple repetitions
Neuromuscular weakness: Impaired motor function (strength or ROM)
Paresis: Mild-moderate
Paralysis: Severe or complete
NMJ Disorders: Management
Autoimmune + Paraneoplastic: Immunosuppressants
Corticosteroids (prednisone)
Steroid-sparing immunosuppressants (MTX, axathioprine)
Biologics (rituximab)
Toxic:
Respiratory support
Remove source
Administer antitoxin
Myasthenia Gravis (MG): Description
Autoimmune NMJ disorder → Muscle weakness
Ocular: Affects only extraocular + eyelid muscles
Generalized: Affects all skeletal muscles
MG: Epidemiology
More common in women
Risk factors…
Other autoimmune conditions
Thymoma (tumor in anterior mediastinum)
Thymic hyperplasia
Allogenic stem cell transplantation
MG: Etiology
Autoantibodies against postsynaptic ACh receptors (AChR) or receptor-associated proteins (muscle-specific tyrosine kinase = AChR formation)
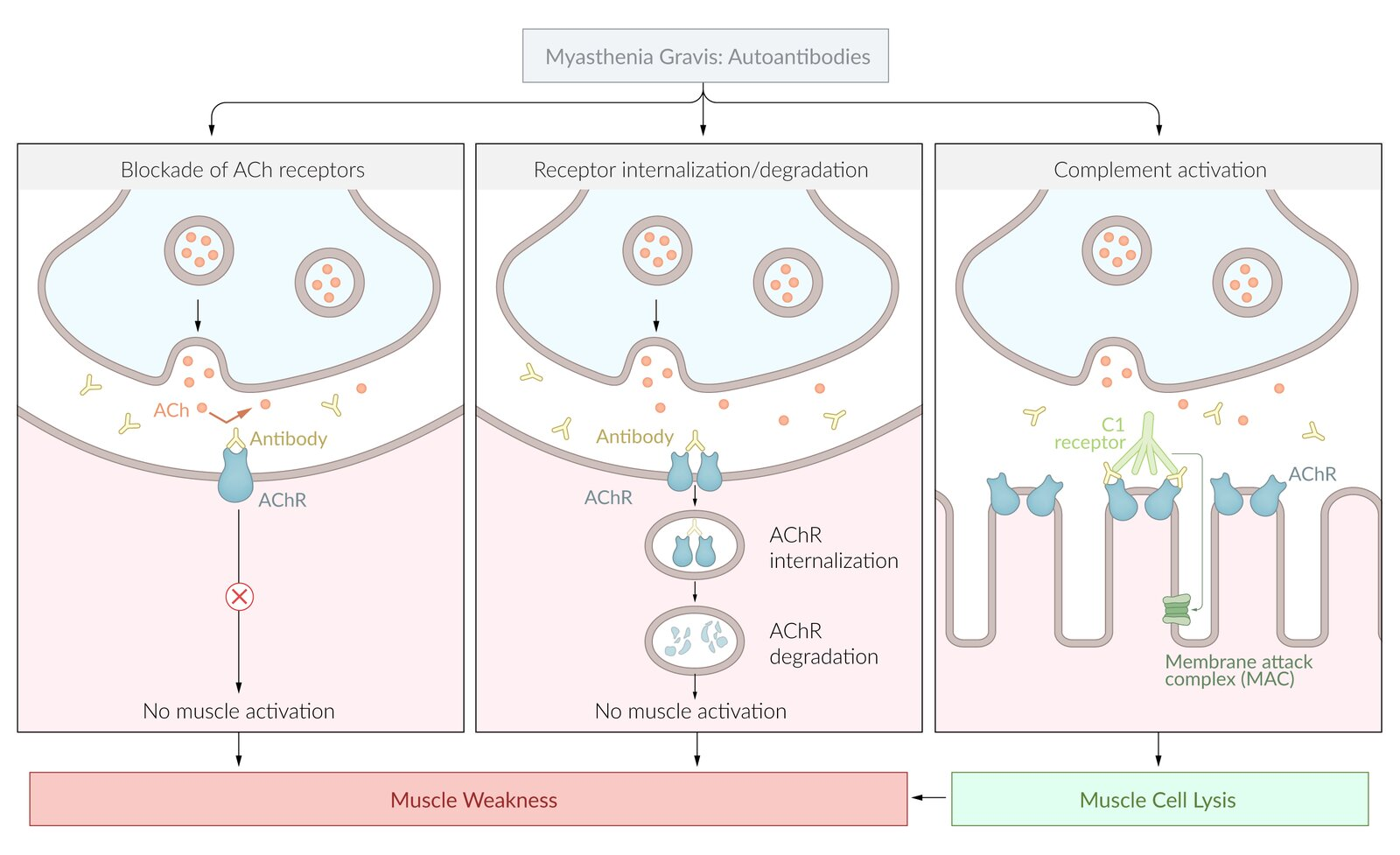
MG: Pathophysiology
Autoantibodies target postsynaptic AChR on muscle cells =
Competitive AChR inhibition
AChR internalization/degradation
Complement activation
Impair signal transduction at NMJ (AChR inhibition + internalization) OR muscle cell lysis (complement) = Skeletal muscle weakness + fatigue
Thymus: Muscle-like (myoid) cells express AChR = T cells target AChR = Produce AChR autoantibodies
MG: Clinical Presentation
Muscle fatigue + weakness
Worse with use
Improves with rest
Eye muscles
Diplopia
Blurred vision
Ptosis: Drooping eyelids
Bulbar (face + neck) muscles
Dysarthria (impaired speech)
Dysphagia
Proximal muscles
Difficulty standing + climbing stairs
Difficulty brushing hair
Respiratory muscles
Dyspnea
Resp failure
MG: Investigations
Physical exam
Lab tests
EMG study
Chest CT
Tensilon/Edrophonium test
MG Investigations: Physical Exam
Normal deep tendon reflexes
Plantar responses
Down going
Ocular Tests:
Ice-Pack Test: Ice pack on affected eyelid for 5 mins = Improve ptosis
Curtain Sign: Lifting more ptotic eyelid = Worsens ptosis in contralateral eyelid
Cogan Lid Twitch Sign: Eyelid twitching after 10-20 sec downward gaze
Simpson Test: Looking up for > 1 min = Eyelid fatigue
MG Investigations: Lab Tests
Anti-AchR abs
Anti-MuSK abs: Negative anti-AChR abs
MG Investigations: EMG Study
Negative anti-AChR abs
Decremental response on repetitive stimulation
MG Investigations: Chest CT
Assess thymoma or thymic hyperplasia
MG Investigations: Tensilon/Edrophonium Test
Process:
Administer rapid-acting short-duration AChE inhibitor
Assess symptoms improvement
Not performed
MG: Treatment
Pharmacological
Surgery
MG Treatment: Pharmacological
AChE inhibitor
MOA: Inhibit ACh breakdown = Increase ACh action at NMJ = Improve muscle contraction + strength
First-Line: Pyridostigmine
Immunosuppressants
Indication: Pyridostigmine inadequacy/intolerance
Ex: Glucocorticoids, azathioprine
MG Treatment: Surgery
Thymectomy
Indications:
Thymoma
Immunotherapy unsuccessful/intolerance
MG: Complications
Myasthenic Crisis: Acute symptom exacerbation → Resp failure
MG: DDX
Lambert-Eaton myasthenic syndrome (LEMS)