Module 5 (Respiratory System )
1/27
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
28 Terms
Describe the structure and function of the respiratory system and its components.
The functions of the reparatory system is the breath, gas exchange, smell and regulate blood pH.
It is divided into the upper and lower respiratory tract.
What consist of the Upper respiratory tract
Nasal cavity
Pharynx
Larynx
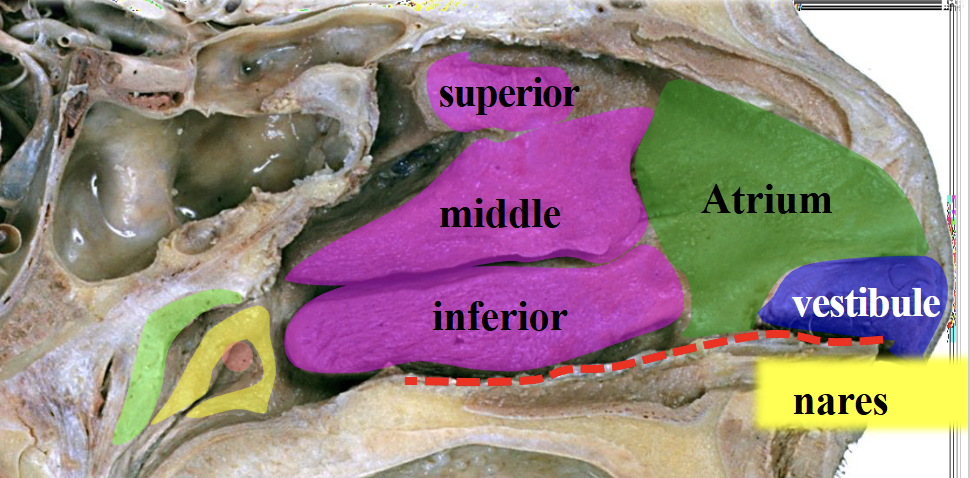
Nasal cavity (Structure and function)
On the lateral wall of the nasal cavity there is the nasal conchae (superior, middle, inferior) that increases surface area and creates turbulence allowing the air to stay in the cavity for longer
Divided by the Nasal septum (cartilage at the front and bone at the back) separating the nose into the left and right nasal cavity
Function
Filters air
Warms inhaled air
Humidifies air
Traps particles in mucus
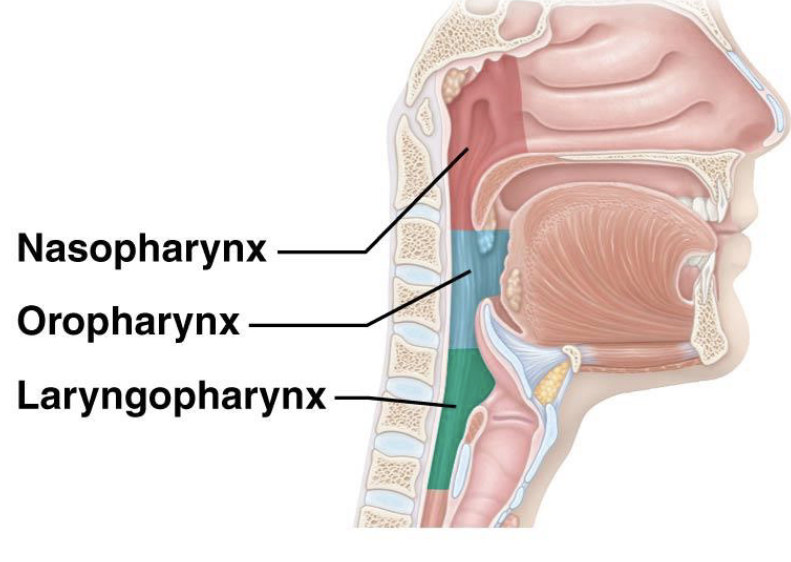
Pharynx (Structure and function)
A muscular tube behind the nasal and oral cavities divided into:
Nasopharynx (Pseudostratified ciliated columnar - Filters, warms, and humidifies air)
Oropharynx (Nonkeratinized stratified squamous - Protects against abrasion from food)
Laryngopharynx (Nonkeratinized stratified squamous - Protects against abrasion from food)
Function
Passageway for air
Assists swallowing
Protects respiratory tract
Walls lined with mucosa
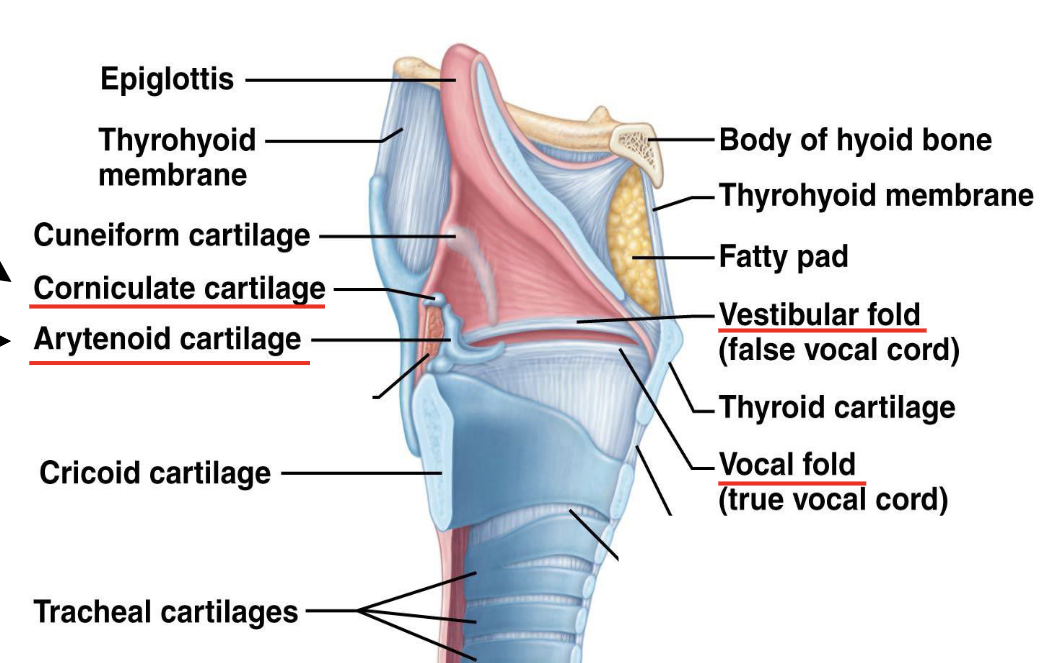
Larynx (Structure and function)
Structure
Cartilaginous structure connecting pharynx to trachea
What connects the pharynx and the trachea
Function
Maintains open airway
Produces sound (voice)
Prevents food entering airway during swallowing
What consist of the Lower Respiratory Tract
Trachea
Bronchi and Bronchioles
Alveoli
Trachea
Structure
Flexible and slightly rigid tube within the mediastinum
Bifurcates (splits in two) into the primary bronchi
Functions:
Conducts air to and from the lungs.
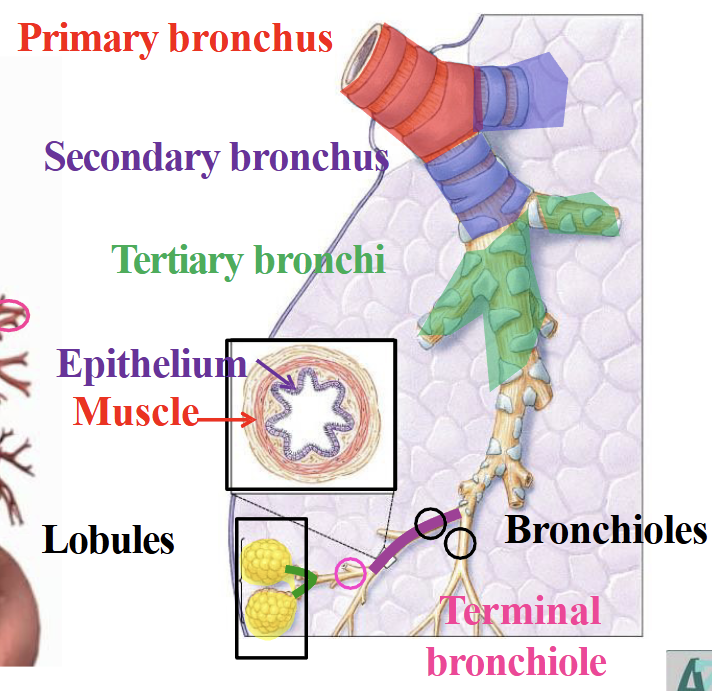
Bronchi and Bronchioles
Bronchi - continues to bifurcate from primary to secondary and then to tertiary bronchi
Bronchioles - From tertiary it turns into bronchioles (smaller branches of bronchi), then terminal, respiratory and finally alveolar ducts.
Function
Conduct air throughout lungs
Alveoli
Structure
Tiny air sacs
Functional units of the lungs
Made of:
Type I and Type II alveolar cells
Function
Site of gas exchange
O₂ diffuses into blood
CO₂ diffuses out of blood
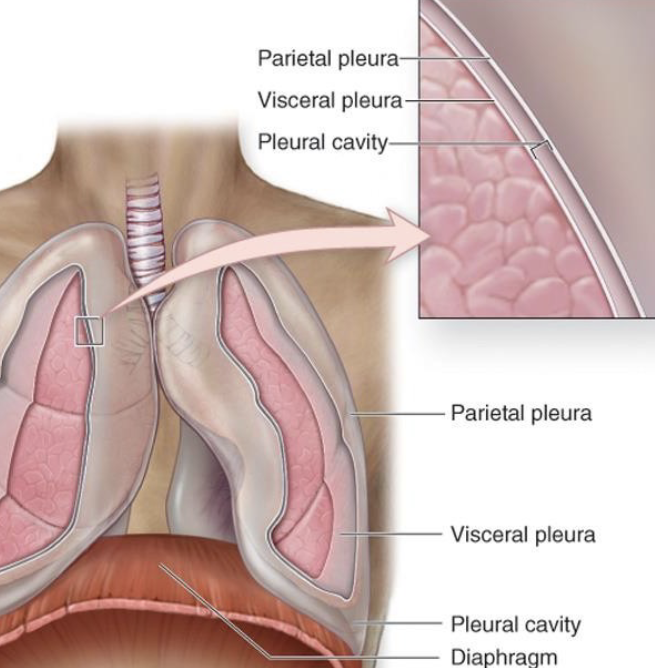
Pleura and Pleural cavities
Structure
Visceral pleura - inner layer, covers lungs
Parietal pleura - outer layer, lines thoracic wall
NOTE: both pleura’s are the same one layer just wrapper around like an elastic band
Between them is the pleural cavity containing pleural fluid.
Function
Reduces friction during breathing
Maintains negative pressure to keep lungs expanded
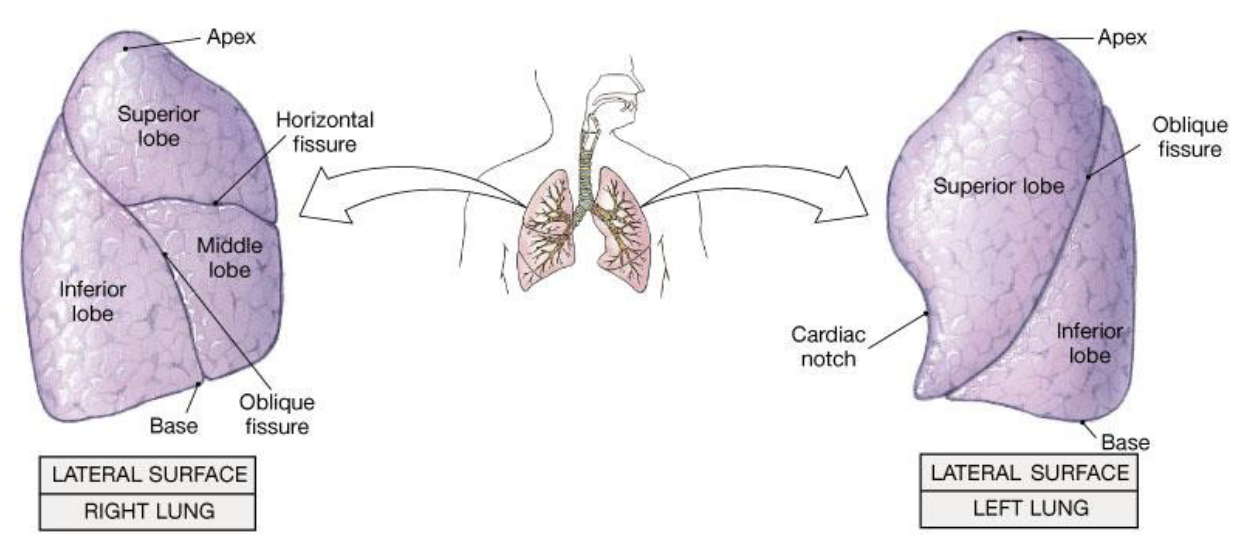
Lungs lobes and fissures
Right lung has 3 lobes (Superior, Middle, Inferior), separated by the horizontal and oblique fissure
Left lung has 2 lobes (Superior, Inferior), separated by the oblique fissure
Intercostal Muscles
Function
External intercostals assist inspiration
Internal intercostals assist forced expiration
Diaphragm
Function
Primary muscle of inspiration.
Contracts → thoracic cavity volume increases, air enters the lungs
Alveolar Pressure Changes (Inhalation + Exhalation)
Inhalation: Diaphragm contracts, flattening, increasing the lung volume thus reducing the pressure making the air move in
Exhalation: Diaphragm and intercostals relax causing the lungs to recoil back elastically, decreased volume moving the air out
Quiet breathing
Two types:
Diaphragmatic (deep) breathing
Inhale: diaphragm contracts → thoracic cavity expands
Exhale: diaphragm relaxes (passive)
Costal (shallow) breathing
Inhale: external intercostals contract as well as the diaphragm → ribs rise → thoracic cavity expands
Exhale: muscles relax (passive)
Fast-forced breathing
Inhalation:
Engages both the external intercostal muscles (elevate the rib cage) and diaphragm (make the lungs bigger)
Exhalation:
Internal intercostals (lower rib cage) and Abdominal muscles contract to reduce thoracic volume
Negative Pressure System (Interpleural Pressure)
Lungs want to recoil inward and the chest want to spring outward, creating a slight vacuum
Always less than atmospheric pressure
Air moves into the lungs when intrapulmonary pressure falls below atmospheric pressure. Air moves out when intrapulmonary pressure rises above atmospheric pressure.
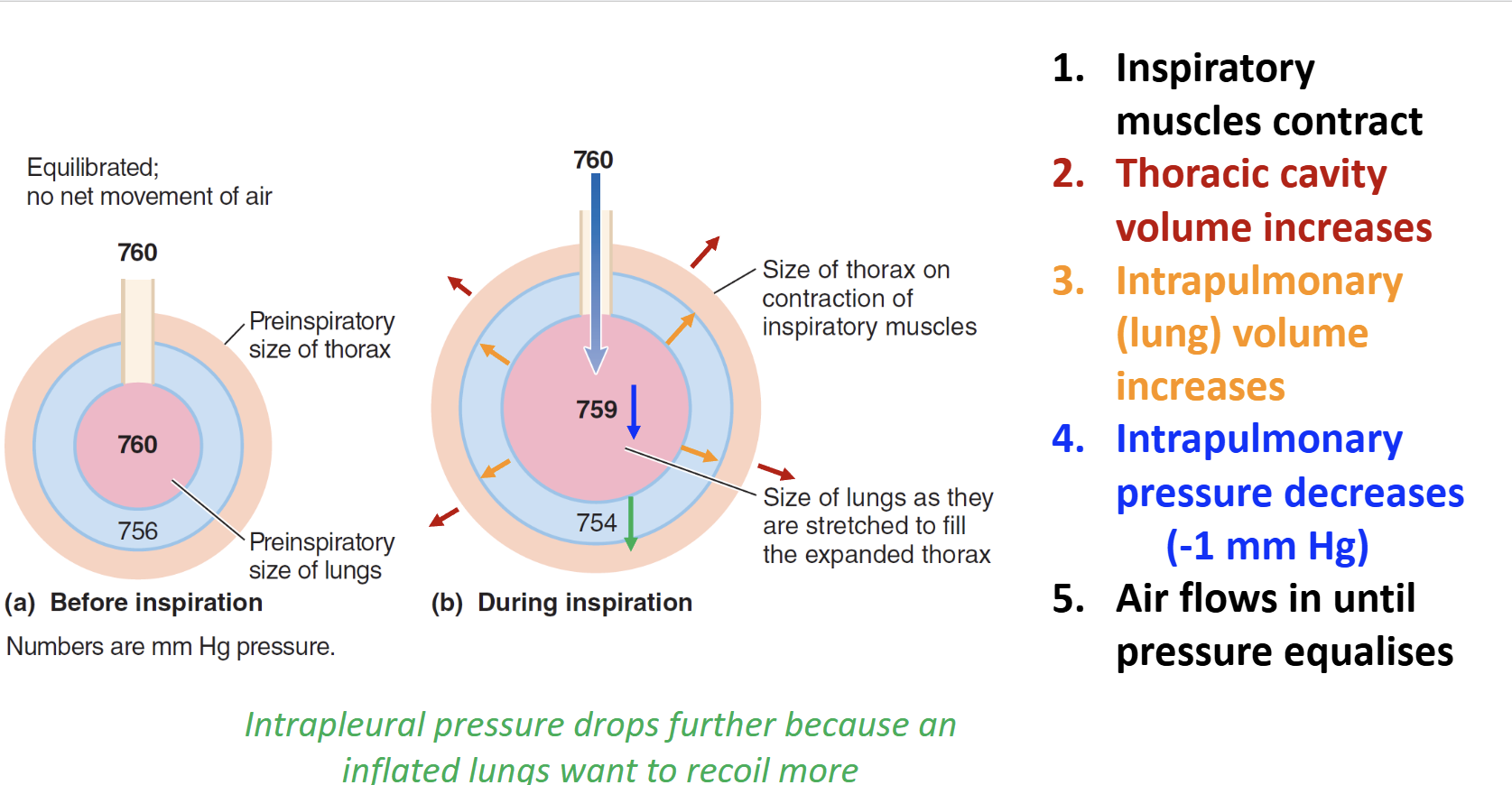
Volume and Pressure changes during inspiration and expiration?
Inspiration:
Thoracic volume ↑
Lung volume ↑
Intrapulmonary pressure ↓
Air flows in
Expiration:
Thoracic volume ↓
Lung volume ↓
Intrapulmonary pressure ↑
Air flows out
Note: Intrapleural pressure may drop further if the lungs are inflated even more, increasing more air intake.
What factors affect inspiration and expiration?
Airway resistance
Increased by bronchoconstriction/dilation, mucus, or fluid
Makes breathing more difficult
Alveolar surface tension
Tends to collapse alveoli as water pulls attracts it to one another
Surfactant reduces surface tension and makes inflation easier
Lung compliance
How easy you can stretch the lungs
High compliance = easier breathing
Low compliance = harder breathing
Elastic recoil
Natural tendency of lungs to recoil after inflation
Helps passive expiration
What is Partial Pressure
Mixture of gasses in the air, each gas creates its own share of pressure.
PO2 or PCO2
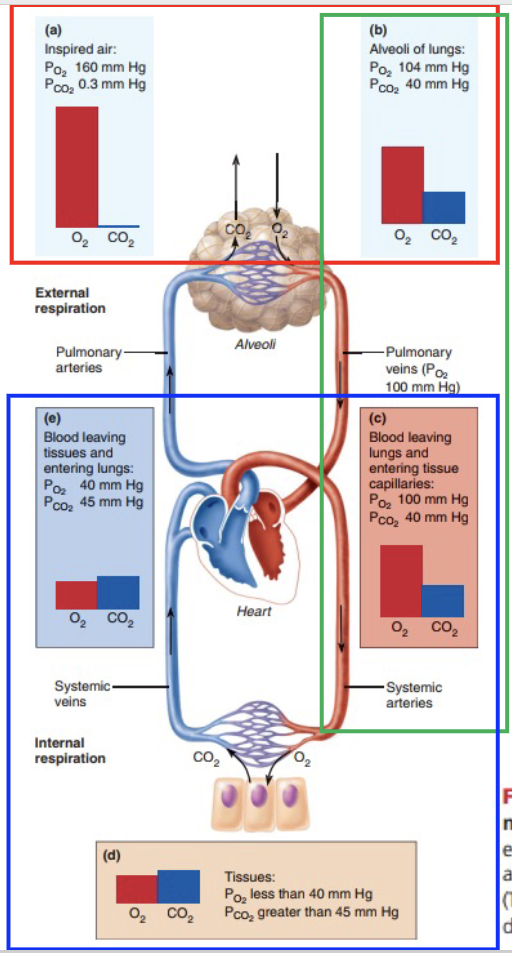
How does PO₂ change throughout the respiratory system and body?
160 → 104 (Air → Alveoli)
The air is mixed with the residual air already in lungs as well as being diluted by water particles
104 → 100 (Alveoli → Blood)
O₂ diffuses into blood
Blood becomes oxygenated
100 → 40 (Blood → Tissues)
Cells continuously use O₂ for respiration
O₂ diffuses from blood into tissues (doesn’t completely empty out)
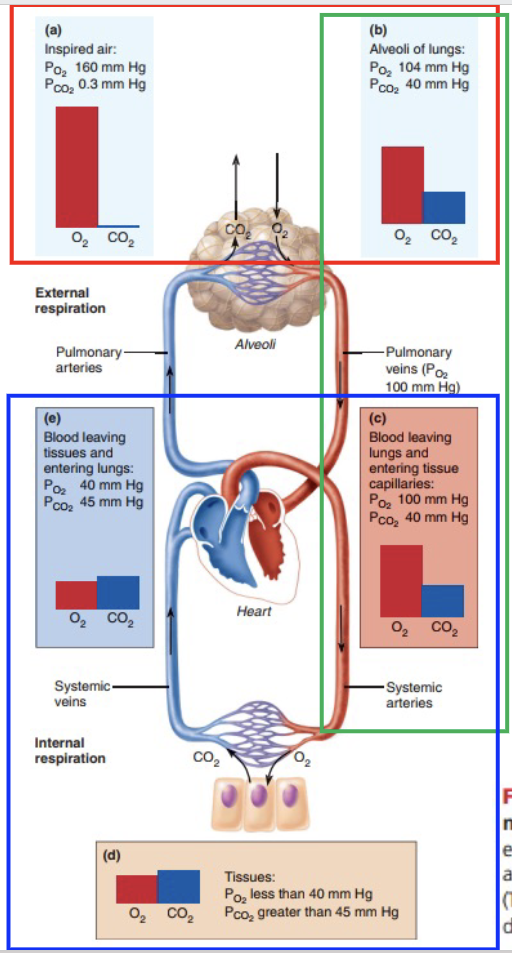
How does PCO₂ change throughout the respiratory system and body?
0.3 → 40 (Air → Alveoli)
CO₂ from blood enters alveoli
40 → 40 (Alveoli → Blood )
40 is left in order to maintain this acid-base balance
40 → 45 (Blood → Tissues)
Cells produce CO₂ during cellular respiration
45 → 40 (Blood → Alveoli)
CO₂ diffuses into alveoli and is exhaled
How are oxygen and carbon dioxide carried in the blood?
Oxygen
98.5% bound to hemoglobin (Hb)
1.5% dissolved in plasma
Carbon Dioxide
70% as bicarbonate ions (HCO₃⁻)
23% bound to hemoglobin
7% dissolved in plasma
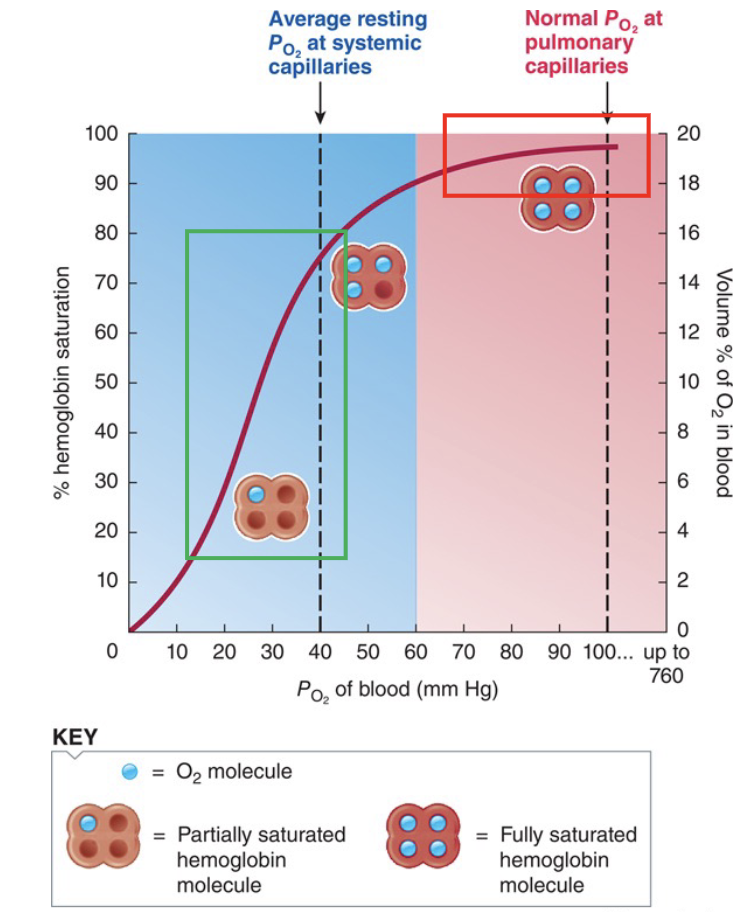
What are the plateau and steep regions of the oxyhemoglobin dissociation curve?
Plateau region (lungs): Large changes in PO₂ cause small changes in Hb saturation (acts as a safety feature to ensure oxygen is received throughout the body) → Hb binds O₂ strongly and remains highly saturated.
Steep region (tissues): Small decreases in PO₂ cause large decreases in Hb saturation → Hb releases O₂ easily.
Link to CO₂:
↑ CO₂ (and H⁺) in tissues reduces Hb's affinity for O₂, making O₂ unload even more easily where it is needed. This results in the CO₂ then being picked up by Hb, while the O₂ is unloaded
Ventilation
Movement of air in and out of the body
Arterial partial pressure of Oxygen
Located in the carotid and aortic bodies.
Detect ↓ PaO₂, ↑ PaCO₂, and ↓ pH.
Important when blood O₂ levels become low.
Many neural tissue becomes less active except for this, peripheral chemoreceptors becomes more active with less oxygen
Stimulates the medullar for increased ventilation.
A lifesaving mechanism
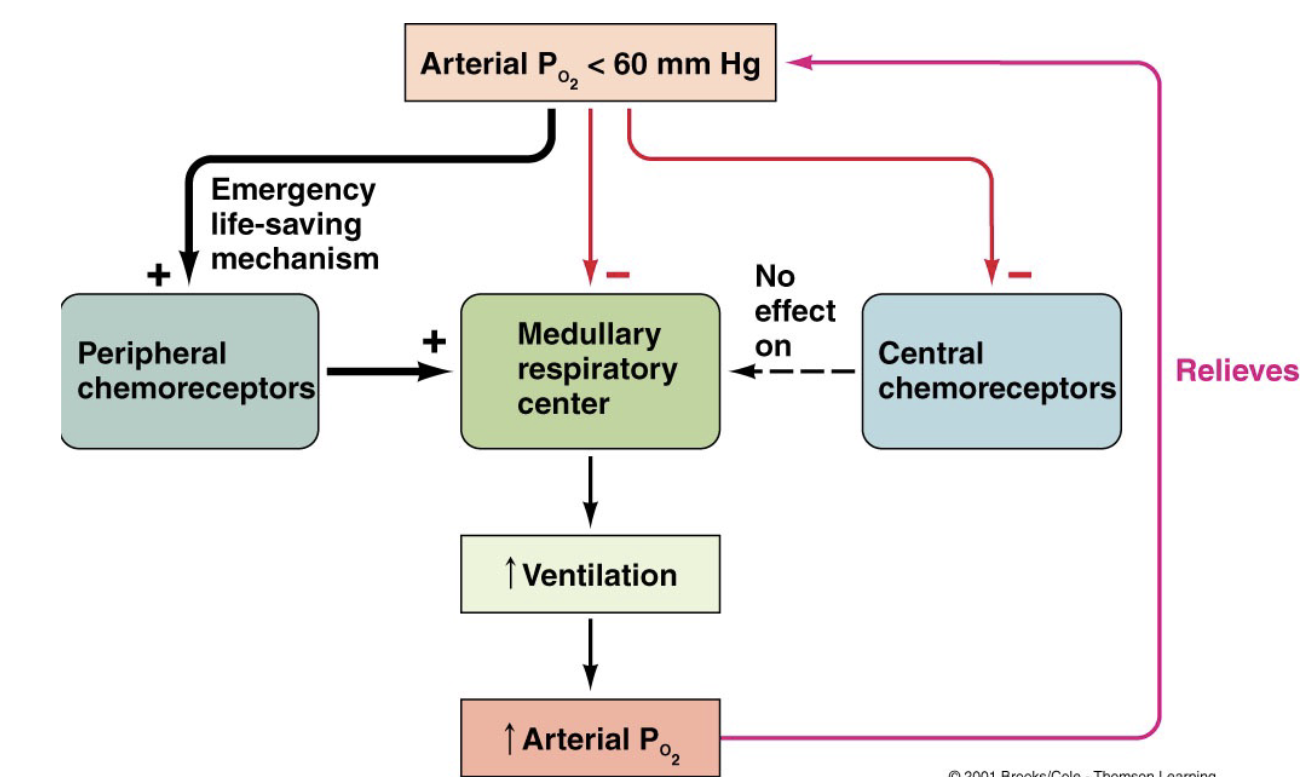
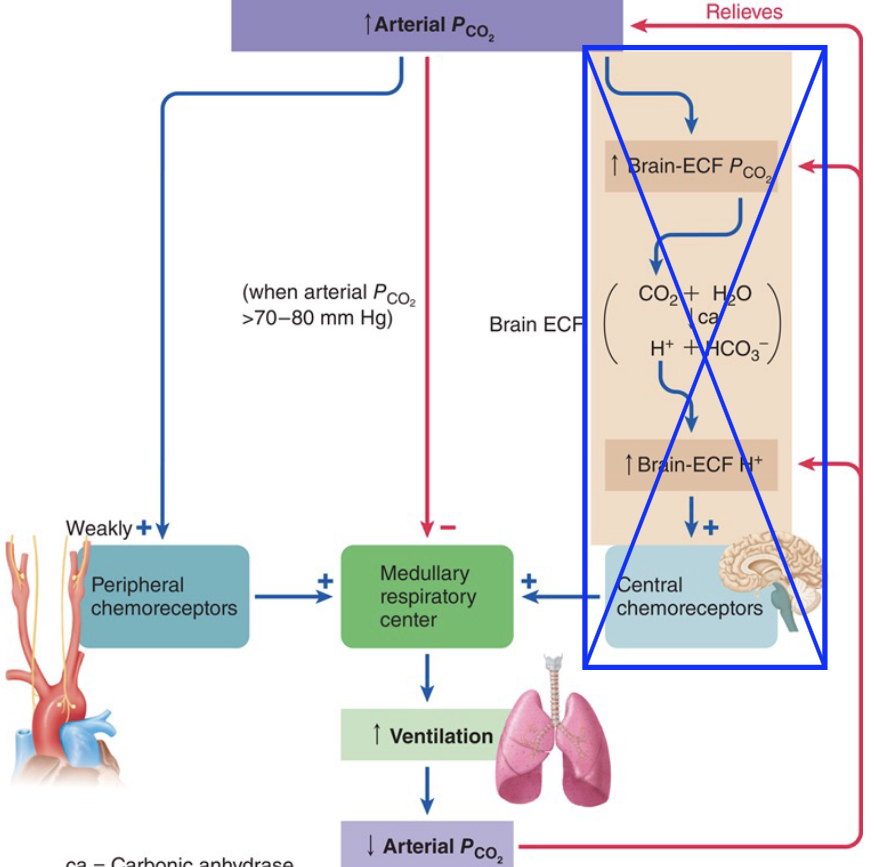
Arterial partial pressure of Carbon Dioxide
Located in the medulla (brainstem).
Detect ↑ PaCO₂ indirectly through ↑ H⁺ in the CSF.
When CO₂ rises → ventilation increases through the central chemoreceptors (detected through the low pH).
Main regulator of normal breathing.
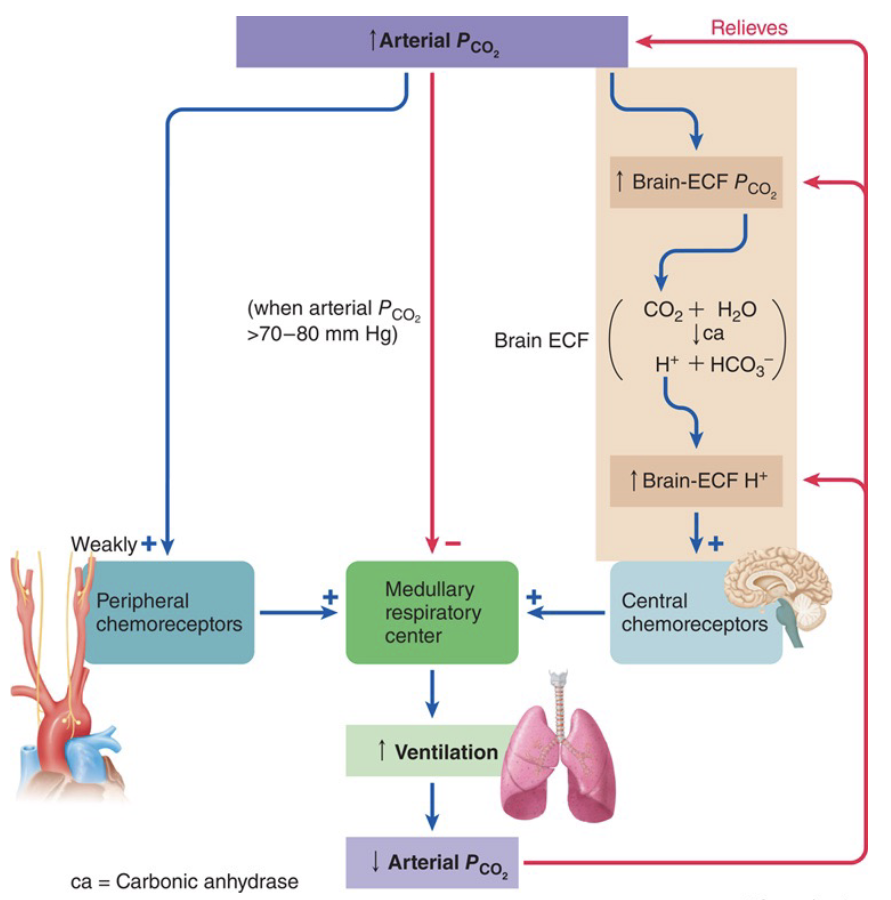
Changes in arterial pH
Blood H⁺ increases
Peripheral chemoreceptors detect the increased H⁺ (low pH) directly
Ventilation increases, removing CO2
Caused by increase in CO2