3018 wk 6 lec
1/28
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
29 Terms
Chronic illness in Childhood and Adolescence
Refers to a condition that interferes with daily function:
For more than 3 months in a year
Causes hospitalisations of more than 1 month in a year
Considerations in Chronic illness for children
Social Determinants of Health
Income
Education
Employment
Working / life living conditions
Food security
Housing
Social considerations (e.g. friends, connections etc.)
Access to healthcare services
Common Chronic Conditions in Childhood
Most common = Asthma
T1DM
Childhood Cancers
Most common = Leukaemia
Conditions of birth
Congenital
Chromosomal
Genetic
Mental Health disorders
ADHD
Anxiety disorder
Eating disorders
→ Suicide is the #1 cause of death amongst individuals aged 15 - 24
+ Premature birth
Congenital birth defects
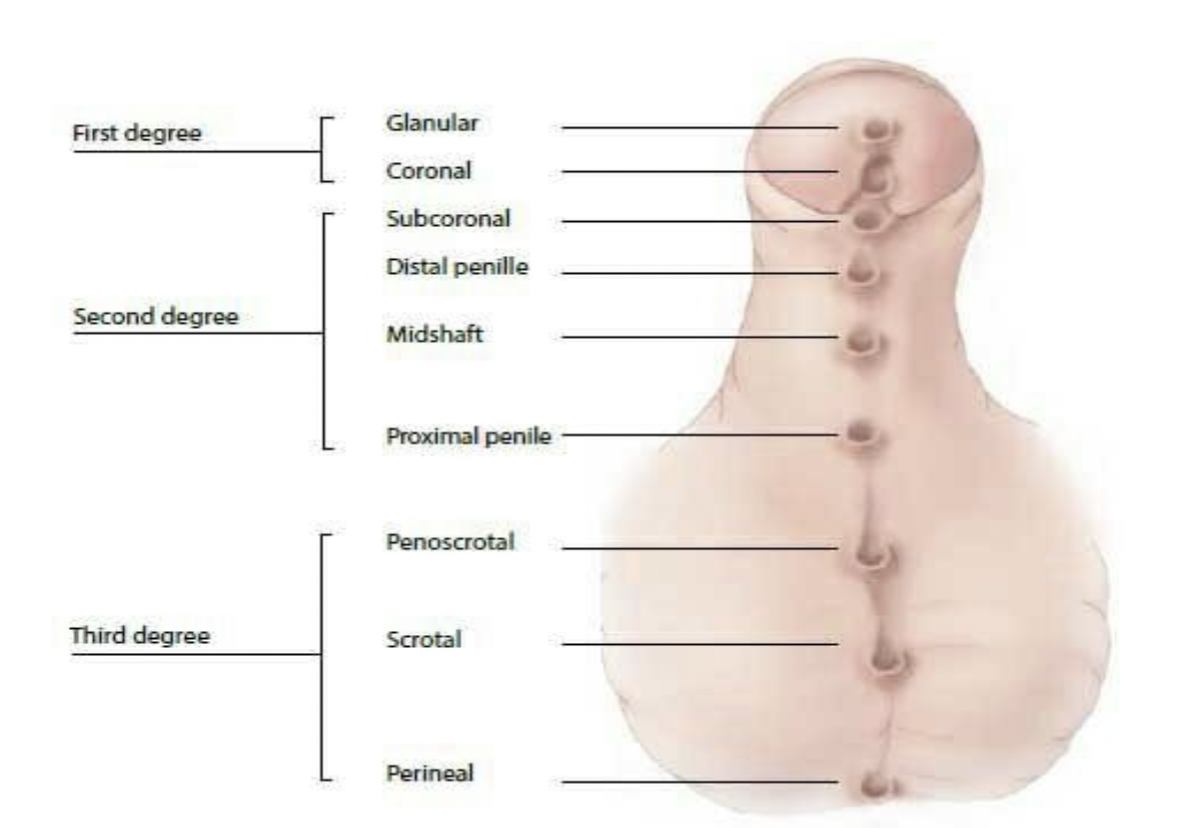
Hypospadias (refer to image)
penile birth defect - where the hole is at the bottom instead of the tip
Neural tube defects
brain, spinal cord, spine
Cleft lip or cleft palate
top lip doesn’t join together / palate has a slight cleft, or is not fully joined together
Chromosomal Birth Defects
1) Trisomy 21 (Down’s Syndrome)
2) Trisomy 13 (Patau Syndrome)
3) Trisomy 18 (Edward’s Syndrome)
Genetic Defects
Cystic Fibrosis - autosomal recessive genetic condition
Sickle Cell Anaemia
Spinal Muscular Atrophy
Childhood Disability
3 Dimensions of Disability
1) Impairment
eg. literal impairment, both functionally or structurally
2) Activity limitation
eg. Difficulty seeing, hearing, walking
3) Participation restriction
eg. restricted in ability to work, engage socially
Medical Model of Disability
Disability is a result of pathology and impairment
Disability is framed as a “problem”
Intervention focuses on treating the individual to be “normal” like society
Social Model of Disability
Disability disables people by FAILING to accomodate for their differences
Differences are socially accepted as “outliers” and “odd”
Leaves disabled individuals as segregated and excluded
Intervention focuses on changing social attitudes and behaviours towards disability
Intellectual and Developmental Disability
Main example = Autism
Significantly reduced ability to understand new or complex information
Reduced ability to learn and apply new skills
Reduced ability to cope independently
Greatly affects social development and personal development into adulthood
→ Social supportive factors can influence the child’s participation and feelings of inclusion in society
Complex Motor Disability
Primary problem is disorder of movement
Complexity comes with movement disorder + other associated exacerbating factors
eg. sensory deficits, learning problems etc.
Cerebral Palsy
A umbrella term for non-progressive neurological conditions that impact motor function
Stems from abnormalities or injury to the brain
Associated impairments under Cerebral Palsy include:
- Intellectual disability
- Epilepsy
- Visual and hearing impairment
Muscular Dystrophy
A broad term that describes the breakdown and cause of muscles to become very weak.
Progressive, irreversible muscle weakness
Muscles over time become replaced by fat deposits, weakening mobility and overall muscular function
Impact of Chronic illness and disability on Children
Spend 3x as many days ill and absent from school compared to those without chronic illness
All chronic conditions have the capacity to affect the development and growth of a child
Impacted emotional wellbeing
Affected social health and growth
Impacted education
May face barriers to quality healthcare
Impact of Chronic illness on Family
Uncertainty about their child’s future
Social isolation - reluctance to leave their child alone
Missed days from work to care
Financial losses
Physical challenges - stress related illnesses and self-neglect for child
Emotional challenges - loss and grief
Complex management of the family life
Impact towards marriage and family dynamics
Family responses after diagnosis
Go through a period of “normalisation” following a diagnosis
Positive normalisation:
Acknowledge condition
Accept potential changes to lifestyle that will occur
Focus on living with and normality
Active engagement in parenting and stabilising family
Development of a treatment regime that suits the family
Signs that the period of “normalisation” is challenging
Emphasis on their child as “different”
Changing parental style solely due to this difference
Illness is the focus of the family → becomes a root problem to many family issues
Treatment is treated as a burden to the family
Family and Child Centred Care
Forming partnerships between clinicians and families
Supportive and responsive to needs of family
Knowledge sharing and open communication
Coordinated care around the specific needs of the family and child
Shared decision making
Chronic illness in Adolescence
Adolescence = the time for achieving independence
Chronic illness can impact the capacity of an individual to successfully function and live independently
Impacts of Chronic illness on adolescent development
Physical
Puberty delay
Weight management
Physical signs of illness present → may impact mental health and self-perception
Psychosocial
Increased dependence on caregiver
Stigma
Social exclusion
Cognitive
Potentially impacted cognition
Learning difficulties due to multiple abscences during school
Family
Impacted family time
Financial challenges
Parental stress, frustration, concern
Impacts on the capacity for independence of Adolescence
Parental overprotection
Added treatment support needs - increased demand
Transition to Adult Healthcare
A milestone of becoming an adult in the healthcare world
What is transition in healthcare?
Purposeful, planned movement of adolescents with chronic medical conditions from child-centred to an adult oriented healthcare system
(generally 14yrs - 25yrs, depending on the appropriateness of starting transition)
It is gradual and designed for the child
Early intervention / prevention model
Supportive and empowering
Once transfer occurs, paediatric systems are still supportive and involved in the familiarising process
Challenges for clinicians during child transition
Letting go of the child
Timing - when is it most appropriate?
High lost of follow-up rate once in adult settings
Some adult clinicians may find it challenging and uncomfortable in managing young adults
Challenges for Adolescents
Different modes of care in adult healthcare
Timing of appointments with numerous different specialties
Language and specialist discussions
Interpretation of their transition being a means of rejection due to their age
Challenges for Parents and Carers
Abandonment
Fears of being perceived as “difficult” in advocating for their child
Anxiety and stress in navigating a more complex system
Principles of Transition Care******
1) Systematic and formal transition process
2) Early preparation
3) Identify and set a transition coordinator
4) Good communication between child, family, and clinicians
5) Individualised transition plan
6) Empower, encourage, and support
7) Follow up and evaluate (often lost)