Dermatopathology and Wound Healing (EXAM 1- MOD)
1/108
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
109 Terms
What are the basic functions of the skin?
Physical barrier against bacteria, virus, & other organisms
Regulates body temp
Prevents dehydration
What are the layers of the skin?
Epidermis, Dermis, Hypodermis/Subcutis
The epidermis protects from….?
Smoke, UV rays, Viruses and Bacteria, and Dryness
The dermis contains…?
blood vessels that produce skin with oxygen and nutrients (most structures located here)
what does the Hypodermis store and control?
stores fat, controls body temp
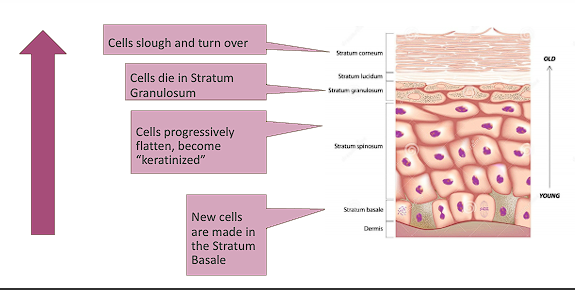
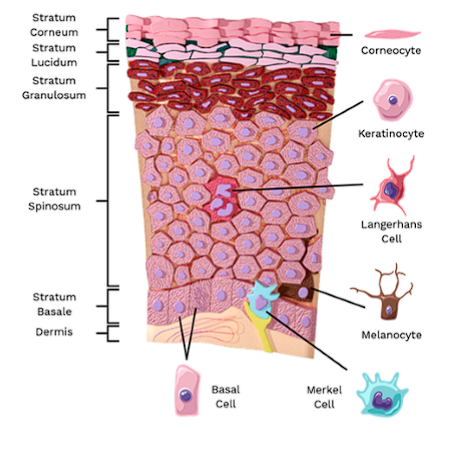
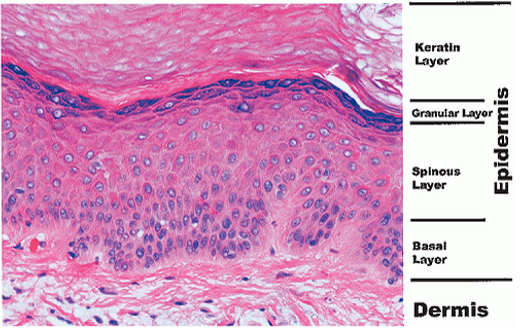
what are the layers of the epidermis? (superficial to deep)
Stratum Corneum → Stratum lucidum →Stratum granulosum → Stratum Spinosum → Stratum Basale (Come Lets Get Some Beer)
Where does cell division in the epidermis layer occur?
Stratum Basale (Basal layer)
what makes up most of the single layer of cuboidal cells in the Basal layer?
Immature keratinocytes and basal cells
Basal cells are the _______ of the skin
stem cells
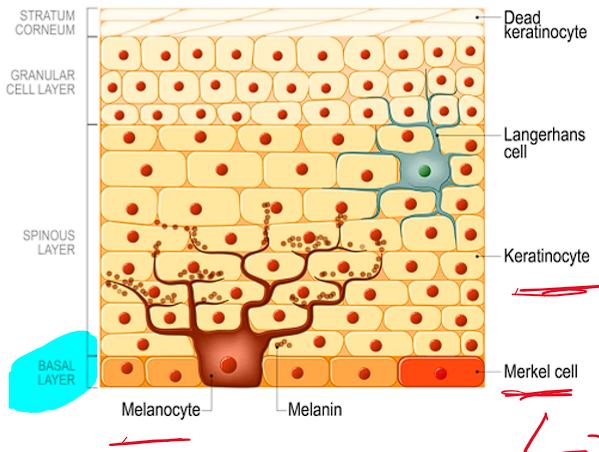
What are the major cell types within the basal layer?
Keratinocytes, Melanocytes, and Merkel cells ( Babe Keep Making Meatloaf)
Describe keratinocytes
Tough, fibrous cells
90% of epidermal cells
Form protective water barrier.
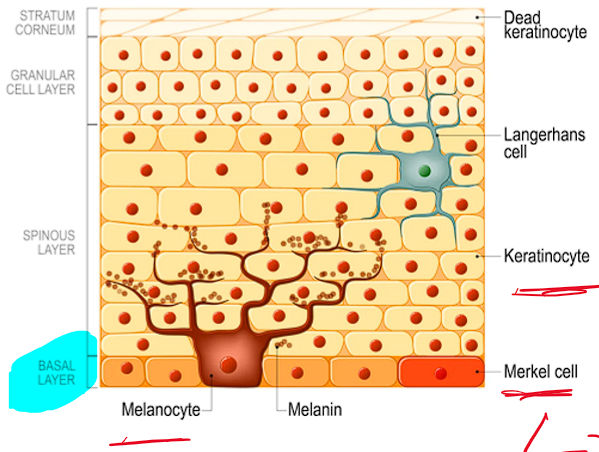
Describe Melanocytes
Produce melanin
Protect from UV rays
Responsible for skin color
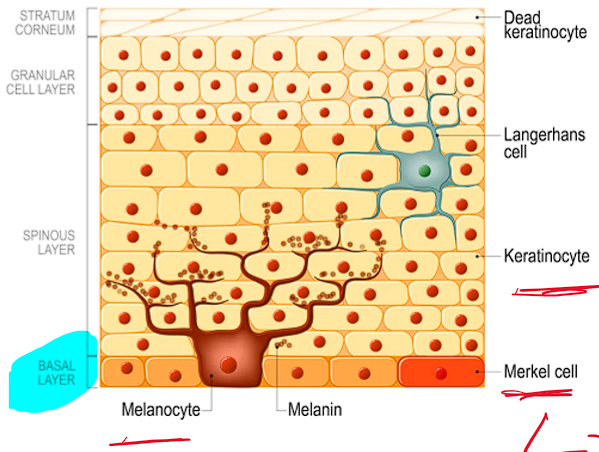
Describe Merkel cells
Epidermal sensory cells that help detect light tough sensation
The stratum spinosum (spinous layer) have mostly what type of cells?
Keratinocytes
The “prickle cell layer” is consider the…?
stratum spinosum
what cells are the first line of immunologic defense in the epidermis? and where is located?
Langerhans cells
located in stratum spinosum

Describe the function of Langerhans cells
Monitor the environment
Capture invaders and break them down
Attach antigens to the cell surface and present them to T cells to trigger immune response
What is the thickness layer of the epidermis?
Stratum Spinosum (Spinous layer)
In the stratum spinosum keratinocytes start producing ?
Keratin
The cells in the spinous layer appear to be what? and why?
“Spiny”
Due to desmosome connections and keratin filaments, which provide strength and help resist adhesive forces
There are 3-5 layers of flattened keratinocytes in which layer of the epidermis?
Stratum granulosum (granular layer)
What is formed in the stratum granulosum?
keratohyalin and lamellar granules
keratohyalin and lamellar granules help do what in the granular layer?
Form waterproof barrier
Solidify the keratin matrix
prevent nutrients from getting to more superficial cells
What disintegrates in the upper layers of the granular layer?
Organelles and Nucleus
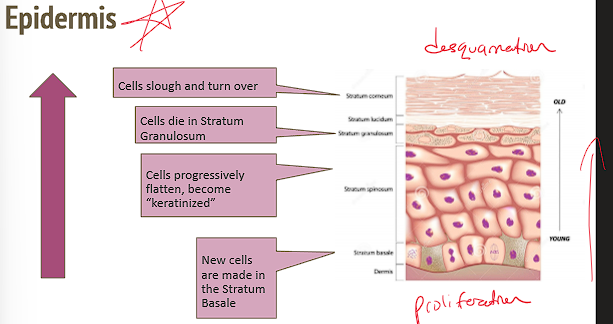
In the Granular layer cells are….
dying
Which layer of the epidermis does constant shedding and replacement occur?
Stratum corneum (cornified layer)

Which layer of the epidermis is considered the “Major physical barrier?”
stratum corneum
There are 10 to 30 layers of cells as flattened plates or “squames” in this layer of the epidermis. What layer is it?
Stratum corneum (cornified layer)
Dead/ “acellular” outer layer is considered which layer of the epidermis?
Cornified layer
Complete cell turnover in the cornified layer takes how long in young people and elderly people?
28-30 days in young people
As long as 50 days in elderly people
describe the process of proliferation to desquamation through the epidermis.
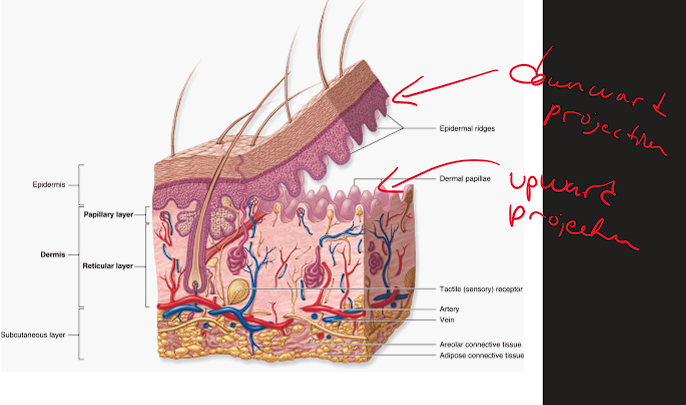
The Dermal-Epidermal Junction (DEJ) is also known as the….?
Basement Membrane Zone
What does the DEJ contribute to ?
structural integrity and the skin’s barrier function between the epidermis and dermis
How does the DEJ contribute to structural integrity?
Rete ridges (epidermal ridge)- downward projection of the epidermis
Dermal papillae - upward projection of the dermis
This alternating pattern increases surface area which:
Forms a strong connection from dermis to epidermis
Allows for efficient exchange of nutrients and waste
What are considered flat skin lesions?
Macules and Patches
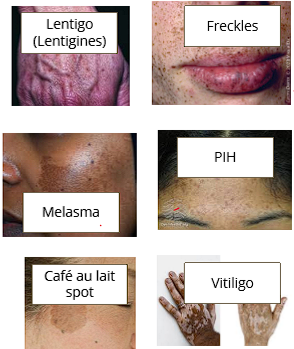
Describe a Macule
A flat (NON PALPABLE), hypo/hyperpigmented lesion
<1cm
what are some examples of a macule?
Freckle
lentigo
post inflammatory hyperpigmentation (PIH)
some nevi (moles)
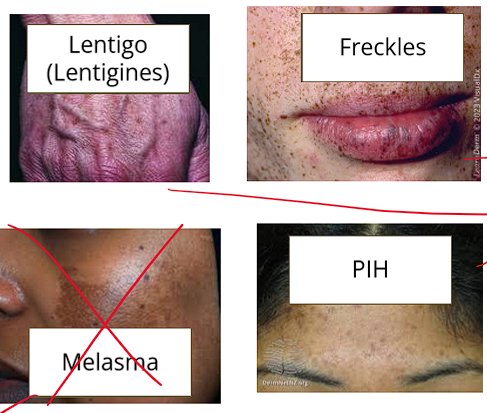
Describe a Patch
Flat (NON PALPABLE), hypo/hyperpigmented area
>1cm
What are some examples of a patch?
vitiligo
cafe au lait spot
tinea versicolor
melasma

What are considered raised skin lesions?
Papules, plaques, and nodules

Describe Papules
Elevated, PALPABLE
<1cm
what are some examples of papules?
Some acne
Warts
Many viral rashes
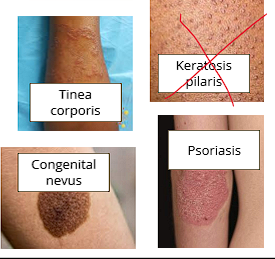
Keratosis pilaris
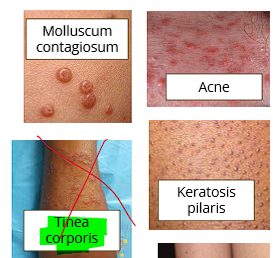
what are plaques
Elevated, Palpable
>1 cm
What are some examples of Plaques?
Psoriasis
Dermatitis
Tinea Corporis
Some congenital nevi
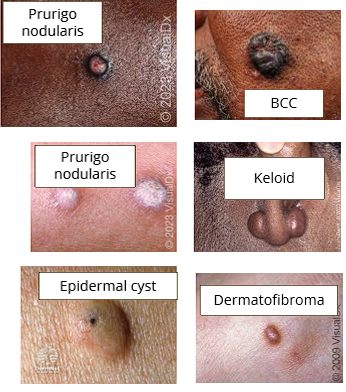
What are Nodules?
Solid, rounded lesion
Diameter is roughly equal to thickness
Firm lesions that extends deeper into the skin
What are some examples of nodules?
Epidermal cysts
Basal cell carcinoma
Keloid
Dermatofibroma
Prurigo nodularis
What are vesicles?
Fluid filled
Small blisters (<1cm)
What are some examples of vesicles?
Chicken pox
Herpetic lesion
Poison Ivy
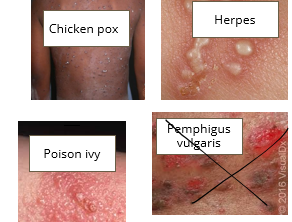
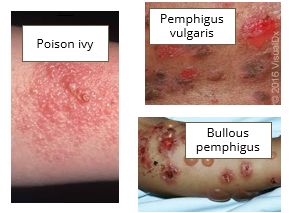
What are Bullae?
Fluid filled
Large Blisters (>1cm)
What are some examples of Bullae?
Poison ivy
Bullous disorders
What are Pustule?
Vesicle or bulla that contains purulent fluid (pus)
What are examples of pustule?
Acne pustule
Folliculitis
Furuncles
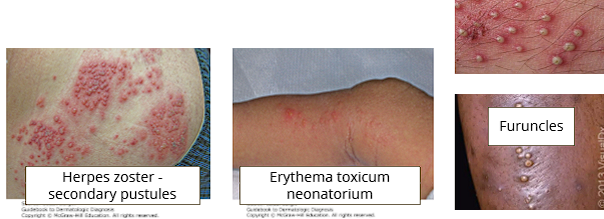
what are considered fluid filled skin lesions?
Vesicles, Bullae, and Pustule
What are the 9 major patterns of skin inflammation?
a. Psoriasiform dermatitis
b. Interface dermatitis
c. Vesiculobullous
d. Vasculitis
e. Spongiotic
f. Panniculitis
g. Nodular
h. Folliculitis
i. Perivascular
What is the representative disease for Psoriasiform Dermatitis?
Psoriasis

Describe the Epidemiology/ Etiology of Psoriasis
Unknown etiology ( genetic and environment component) affects 1-2% of population
Describe the pathogenesis of Psoriasiform Dermatitis
The cell cycle moves far too fast; too many new keratinocytes are produced in the basal layer, and they’re pushed to the surface without having proper chance to mature
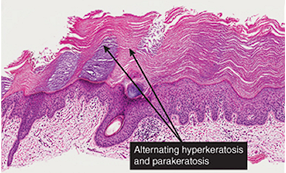
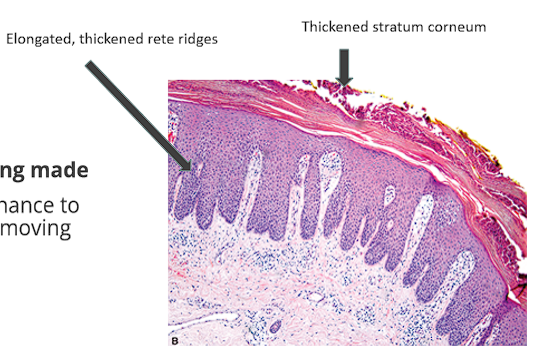
Describe the histopathology of Psoriasiform Dermatitis
Rapid epidermal cell turnover→ Marked epidermal thickening of the stratum corneum (Hyperkeratosis- skin producing cells faster than it can shed them)
Rete ridges are significantly and evenly elongated
Cornified layer exhibits (Parakeratosis- immaturity of those piled-up cells)
Accumulation of acute inflammatory cells (neutrophils) within the epidermis
What are the clinical manifestations of Psoriasiform dermatitis?
Chronic persistent, relapsing, scaling skin condition
Sharply marginated (clear border) , red plaques with silvery scales
can see associated arthritis
EX: lichen simplex chonicus, seborrheic dermatitis

What is the representative disease for Interface dermatitis?
Lichen Planus

What is the epidemiology/etiology of Interface dermatitis?
Poorly understood, can be related to medications
What is the pathogenesis of interface dermatitis?
An inflammatory process where infiltrating immune cells directly attack and damage the keratinocytes resting along the DEJ
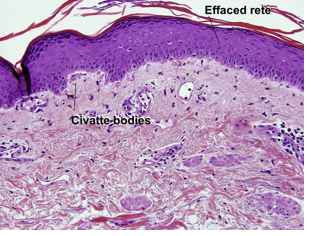
What is the Histopathology of interface dermatitis?
Dense infiltrate of lymphocytes (mostly T Lymphocytes) along the DEJ
Keratinocytes under attack clump tg → form Colloid/Civatte bodies (dense eosinophilic globules)
Chronic inflammation causes hyperkeratosis and flattening of rete ridges, “Sawtooth” rete ridges in established lesions.
what are the clinical manifestations of interface dermatitis?
Itchy rash with distinct violaceous papules with angulated borders and flat tops or “Pruritic, polygonal, purple papules”
Flexor surfaces of extremities, genital area
Whitish streaks on lesiona are also seen on mucosa (Wickham Striae)
EX: Lupus, erythema multiforme, fixed drug reaction
What is the representative disease for Vesiculobullous Dermatitis?
Bullous Pemphigoid
What is the Epidemiology/Etiology for Vesiculobullous Dermatitis?
Blistering autoimmune disease that typically occurs in elderly patients
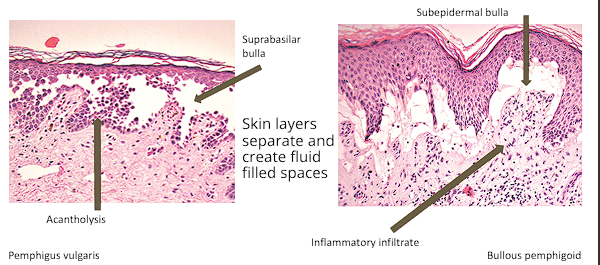
What is the pathogenesis for Vesiculobullous Dermatitis?
Autoantibodies target components of the skin’s basement membrane causing separation of the skin layers and fluid filled space
What is the Histopathology for Vesiculobullous Dermatitis?
Subepidermal bullae (blisters forms beneath epidermis) or Intraepidermal bullae (blister forms within epidermis)
Some related VD diseases may have acantholysis (separation of keratinocytes) or hyperkeratosis
Inflammatory infiltrate within dermis and around blister can vary, commonly including Eosinophils, neutrophils and lymphocytes
what are the clinical manifestations for Vesiculobullous Dermatitis?
Begins itching (hive like) and then a tense blister develops
Most commonly on extremities and trunk
When it breaks, leaves erosion, then hyperpigmentation after blister goes away
EX: pemphigus, dermatitis herpetiformis, HSV, hand-foot-mouth disease
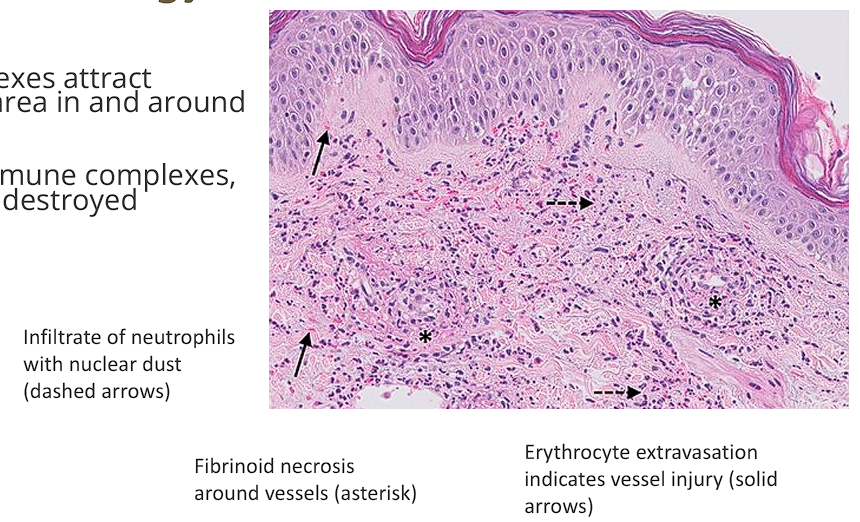
What is the representative disease for Vasculitis?
Leukocytoclastic Vasculitis (LCV)
What is the epidemiology/etiology of Vasculitis?
Can occur at any age
Triggered by infections (especially Staph and Strep), cancers, or medications
What is the pathogenesis of Vasculitis?
immune complexes (antibodies bound to exogenous antigens) deposit in vessel walls
Neutrophils destroy vessels and surrounding tissue
What is the Histopathology of Vasculitis?
Neutrophil infiltration around vessels
Leukocytoclasia- accumulation of necrotic neutrophil nuclei and debris
Fibrinoid necrosis - Fibrin protein deposition within and around vessel walls
RBC extravasation (leakage of blood)
What are the clinical manifestations of vasiculitis?
inflammatory disorder of small blood vessels
Palpable purpura
Lesions may ulcerate or become necrotic
Arthralgia, myalgia, malaise, involvement of GI tract and other abdominal organs
EX: IgA Vasculitis, Connective tissue diseases, ANCA-associated vasculitides
What is the Representative disease of Spongiotic Dermatitis?
Allergic Contact Dermatitis
What is the Epidemiology/Etiology of Spongiotic Dermatitis?
Very Common, thousands of known antigens
Delayed hypersensitivity reaction
Immune mediated reaction to a substance that touched the skin
What is the histopathology of Spongiotic Dermatitis?
Spongiosis (intracellular edema of epidermis)
Separation of Keratinocytes
minimal perceptible microscopic changes→ severe blisters w/ fluid filled spaces
Perivascular inflammation of superficial dermis
Infiltrate of lymphocytes and eosinophils
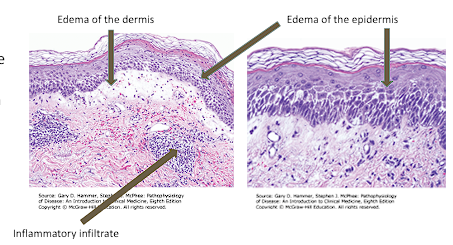
What is the pathogenesis of Spongiotic Dermatitis?
Epidermal edema causes separation between keratinocytes
What are the clinical manifestations of Spongiotic Dermatitis?
Pruritic eruption
Erythematous papules
Vesicles and Bullae at contact site
EX: Drug eruptions, Atopic dermatitis (eczema)
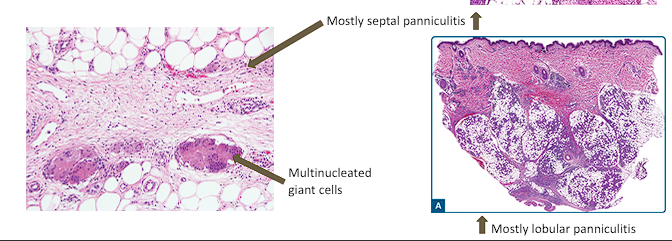
What is the representative disease for Pannicultis?
Erythema Nodosum
What is the Epidemiology /Etiology for Panniculitis?
More common in females (3:1)
Associated with infections, IBD, medications
What is the histopathology for Panniculitis?
Inflammation of the subcutaneous fat
Septal thickening/fibrosis in some cases of septal inflammation
Foamy histiocytes and multinucleated giant cells due to necrosis within fat
What are the clinical manifestations of Panniculitis?
Tender red nodules→ anterior lower legs
Bruise like patches
Fever and arthralgias possible
EX: Erythema Induratum, Nodular vasculitis, Lupus
What is the representative disease for Nodular dermatitis?
Cutaneous sarcoidosis
What is the Epidemiology/Etiology for Nodular dermatitis?
High incidence in black population in US, Women >Men
Poorly understood
Genetic and environmental components
What is the Histopathology for Nodular dermatitis?
Dense infiltrates of inflammatory cells in dermis
Macrophages and lymphocytes (sometimes eosinophils and neutrophils) compose nodules
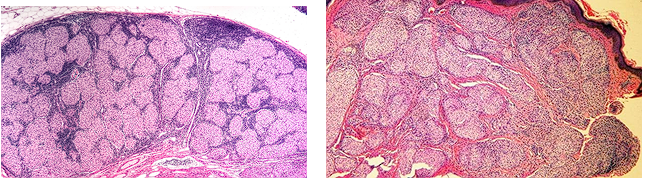
What is the pathogenesis of Nodular dermatitis?
Large, well defined collections of immune cells group tg to form nodules within the dermis
What are the clinical manifestations of Nodular dermatitis?
Red-brown nodules
Common on face
Painful, itchy, or ulcerated lesions\
“great imitator”, can occur within tattoos and scars
EX: Prurigo nodularis
What is the representative disease for Folliculitis?
Acne
What is the epidemiology/ etiology of folliculitis?
Any age possible, very common in adolescents
Excess sebum production
Hyperkeratinization (clogging of hair follicles)
Bacterial colonization (Cutibacterium acnes)
inflammation
What is the histopathology of folliculitis?
Inflamed hair follicle
Follicle becomes plugged with keratin, sebum, and/or debris
Neutrophilic infiltrate → can form intraepidermal pustules
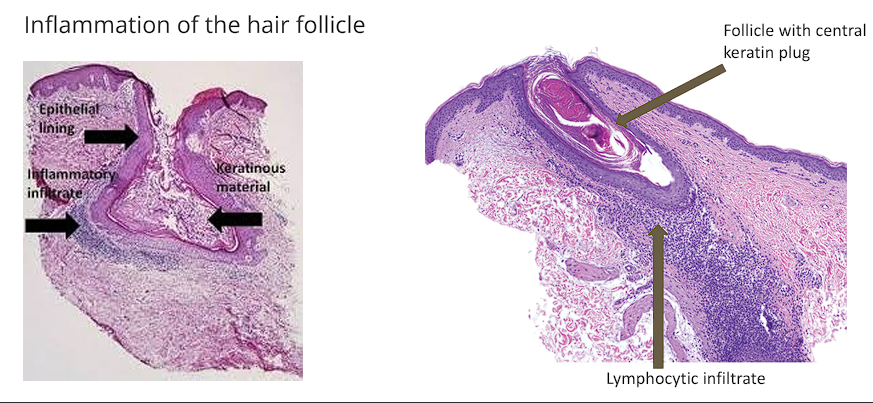
What is the pathogenesis of folliculitis?
Follicle becomes plugged
Follicular wall ruptures
Contents spill into dermis causing inflammation
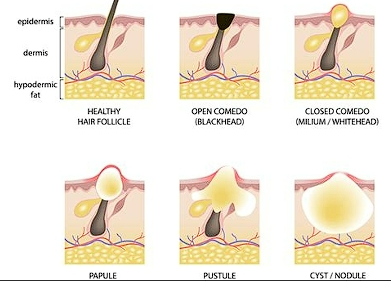
What are the Clinical manifestations of folliculitis?
Follicle based comedones, inflammatory papules, and pustules

What is the representative disease for Perivascular dermatitis?
Urticaria
What is the epidemiology/Etiology for Perivascular dermatitis?
Affects 15-25% of population, all ages
Many causes
What is the histopathology for Perivascular dermatitis?
Mast cell degranulation→ release histamine pro-inflammatory cytokines
Causes vasodilation and extravasation of fluid in the dermis
Minimal to no epidermal changes
What is the pathogenesis for Perivascular dermatitis?
Inflammatory reaction clustered around superficial and/or deep dermal blood vessels
What are the clinical manifestations for Perivascular dermatitis?
Transient papules or plaques, often called hives/wheals
Possible angioedema/anaphylaxis
EX: Insect bite reactions, angioedema

Actinic Keratosis (AK), Basal cell carcinoma (BCC), Squamous cell carcinoma (SCC), and Malignant melanoma (MM) are considered __________ lesions.
Neoplastic lesions
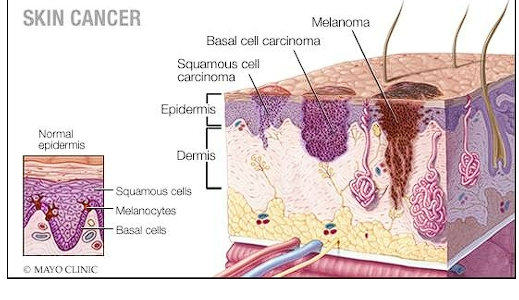
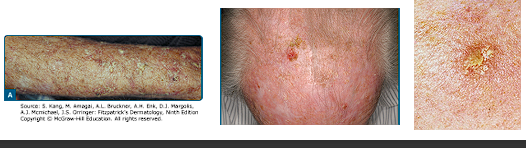
Describe Actinic keratosis and It’s histology
Precancerous lesion
Caused by sun exposure
Rough scaly lesion
Can progress to Squamous cell carcinoma
Histology:
Dysplastic keratinocytes
Parakeratosis: retention of nuclei in the stratum corneum
Thickened stratum corneum