ceutics drug disposition
1/91
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
92 Terms
which things are absorbed in the stomach
weak acids and alcohol
which type of drugs are likely to have an instantaneous effect
lipophilic drugs
(ex: anasthesia)
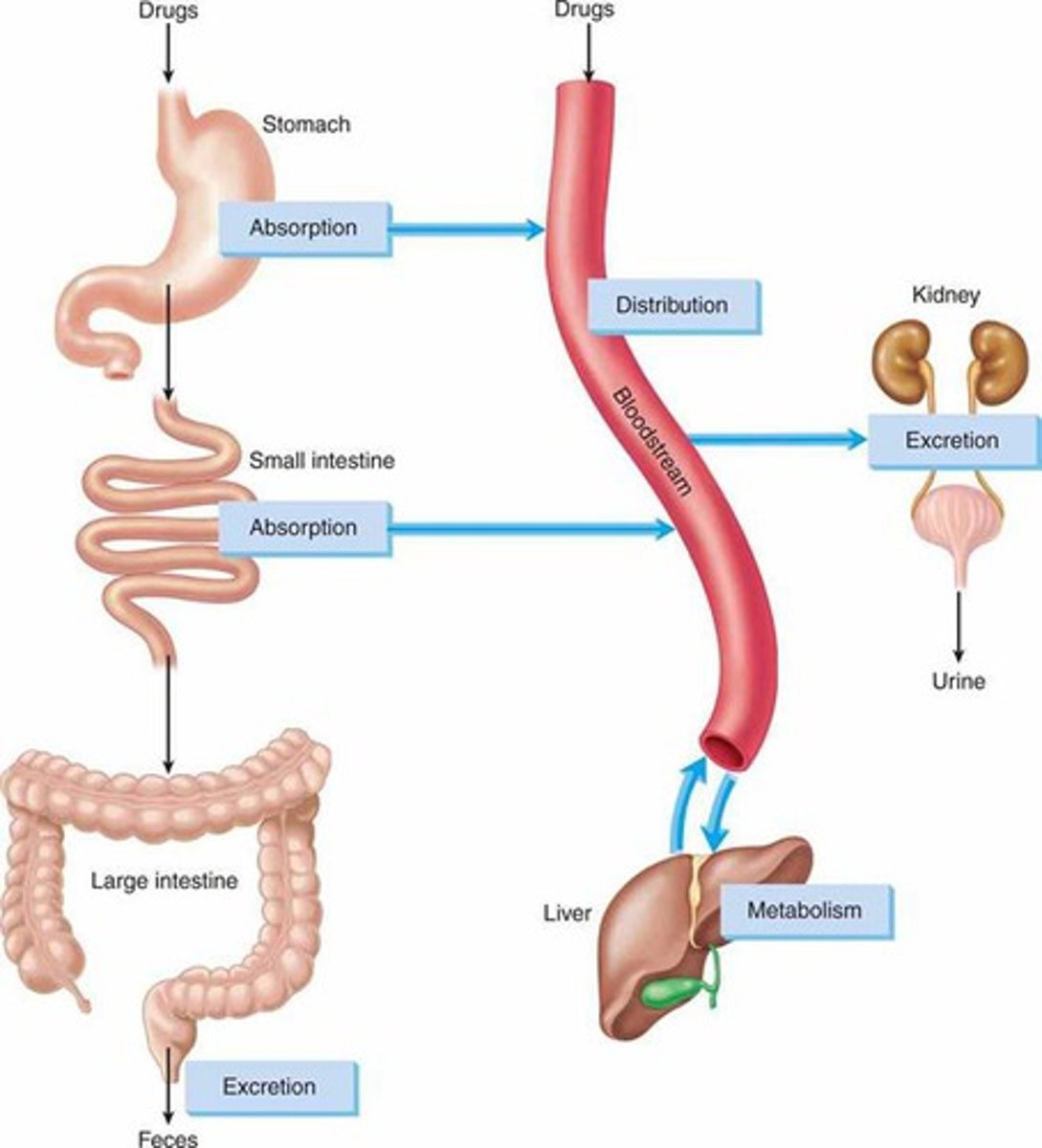
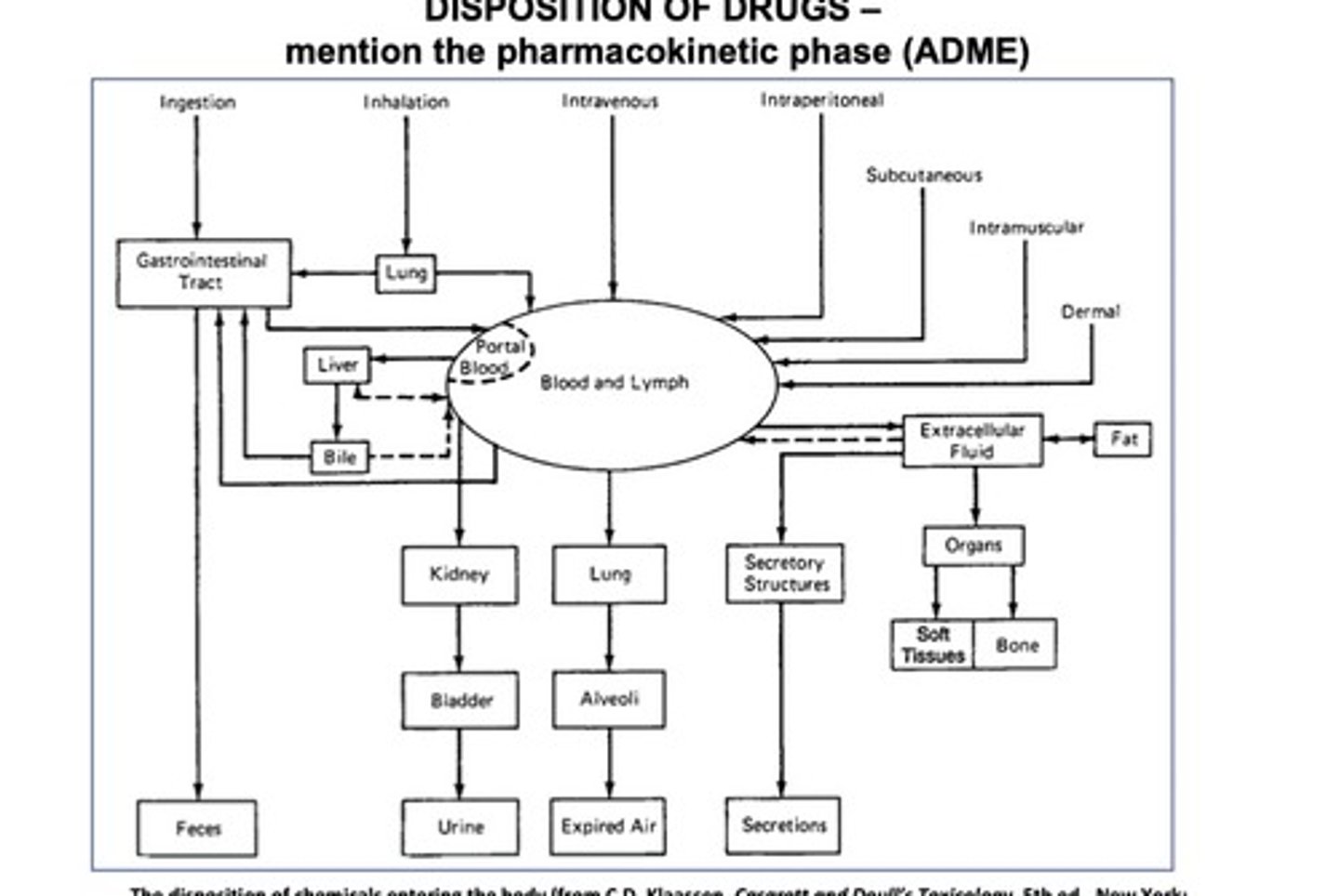
describe the pathway an oral drug travels from ingestion to excretion
ingested
-> stomach (weak acids and alcohol absorbed)
-> intestines
-> liver portal circulation (metabolism)
-> some escapes to target, rest is excreted
in general, what determines the magnitude of the effect of a drug?
concentration of drug at the site of action aka dose (1st order kinetics= higher concentration then higher effect)
t/f: a higher dose is linked to greater magnitude of effect and faster onset
false. usually greater magnitude but does not mean faster onset. onset depends on how fast absorbed, not how much there is
pharmacokinetics vs pharmacodynamics
Pharmacokinetics: What the BODY does on the drugm (ADME)
Pharmacodynamics: What the DRUG does on the body (effect of drug on target cells)
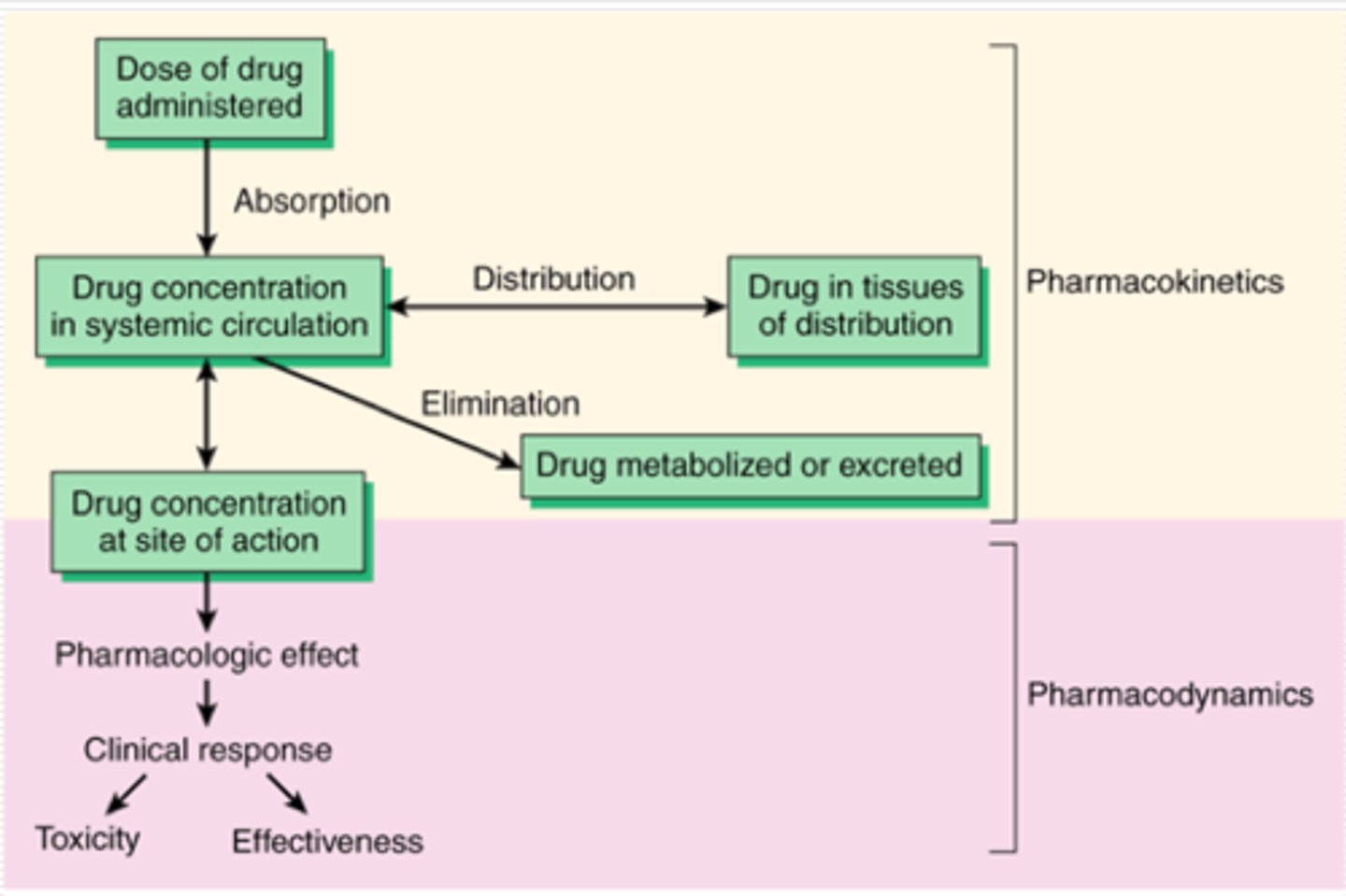
ADME is the study of pharmaco________
kinetics
the effect of a drug on target cells is known as pharmaco_________
dynamics
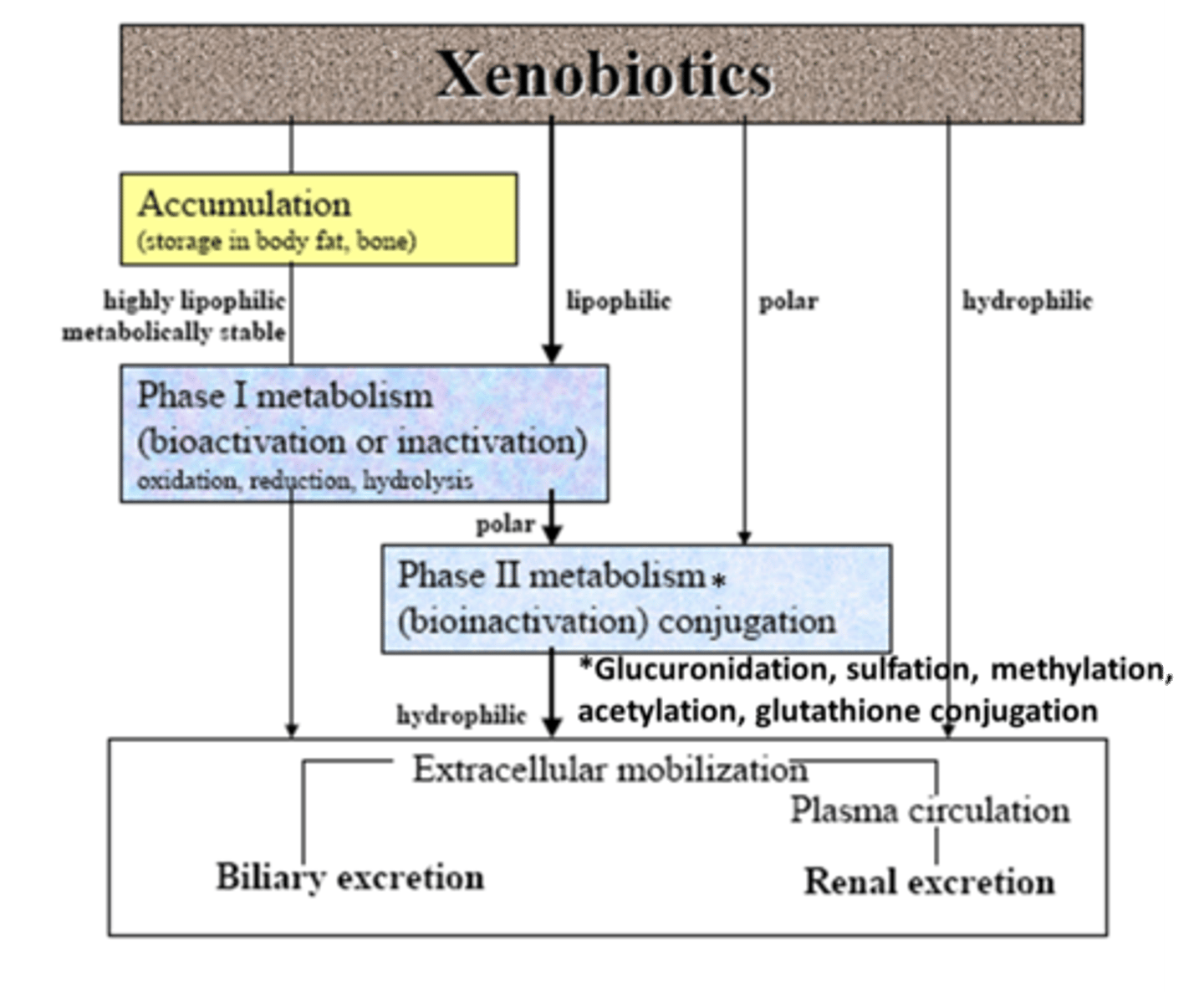
xenobiotic
foreign substance taken into the body (not endogenous)
- note: some endogenous compounds may also act as xenobiotics (ex: T3 and T4/ thyroxine)
t/f: while xenobiotics are not endogenous compounds, some endogenous compounds may act as xenobiotics
true. ex: thyroxine
how are doses established
trial and error in phase 2
- dose, intervals, and route randomly selected and pt is evaluated
t/f: the magnitude of response of a drug is proportional to the concentration of the drug at the site of administration
false. site of action
2 types of concentration gradients measured in PK
site of ________
site of _______
1. site of administration= absorption. drug is in blood or lymph
2. site of action= tissue cells/ post absorption, blood delivers to target and diffuses to target
t/f: if drug enters blood but complement blows it up or enzyme destroys it, we have high absorption at the site of action
false. high absorption at site of administration but low at site of action (post absorption issue)
what explains why many drugs have side effects
drugs must move from site of administration to site of action. drug will end up distributing to other tissues unintentionally leading to side effects
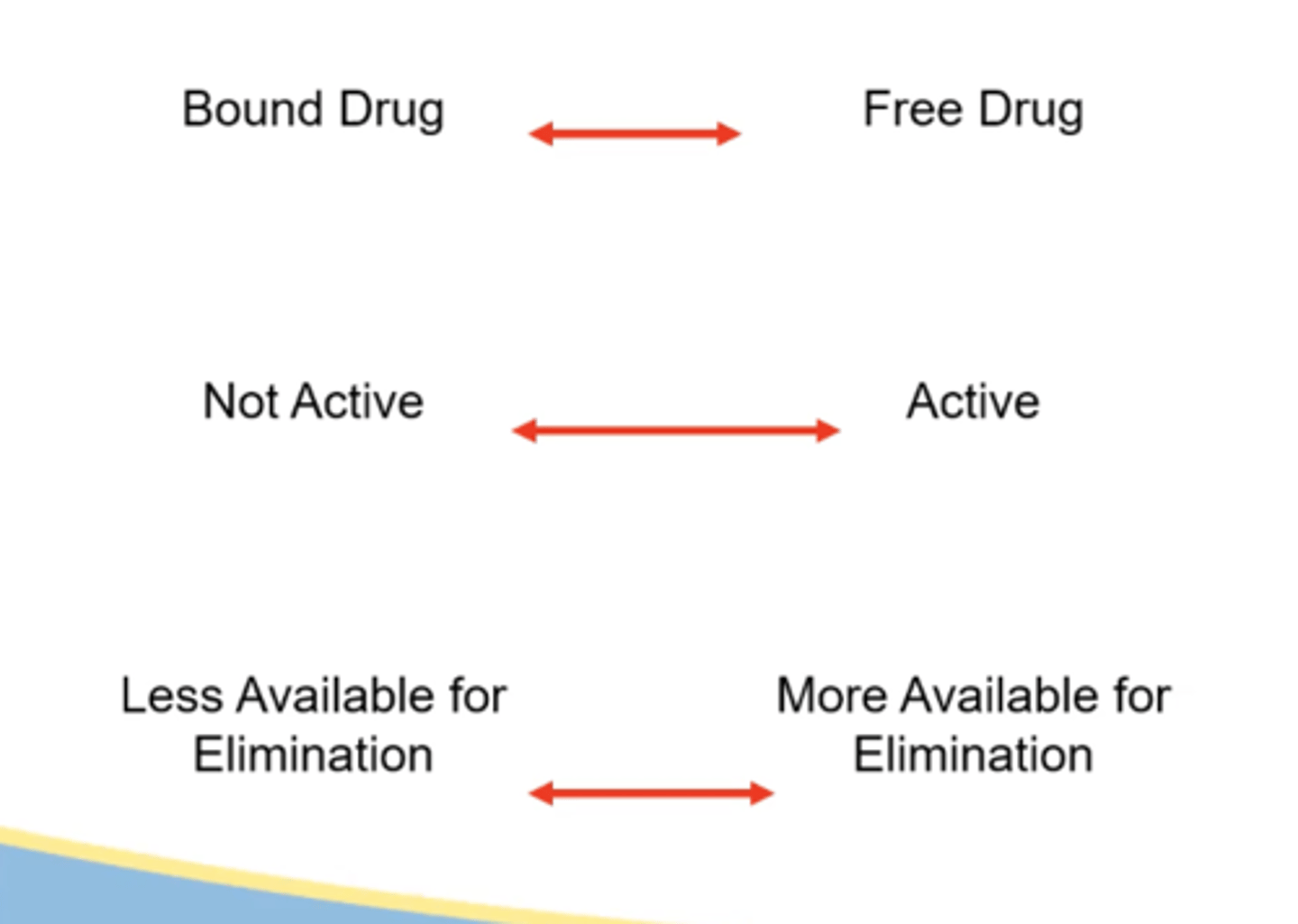
when drugs that have escaped metabolism are bound to plasma protein, they are related to
a. onset
b. duration
c. intensity
b. duration
why do we not consider metabolized drugs bound to albumin in the ct curve
bc they have no effect. they are inactive and waiting for elimination. but know that they do bind to albumin and take up space
what can happen to a free drug (unbound to albumin) in the plasma (4)
1. exerts effect at site of action (ex: receptor)
2. become sequestered in other tissues (trapped w no effect. ex: fat)
3. become metabolized (liver, lung, GI)
4. may be eliminated directly (kidney, air, sweat, feces)
in which 4 ways can drugs be eliminated
1. feces (via GI)
2. urine (via kidney)
3. expired air (via lungs)
4. secretions (via sweat/sebum)
magnitude of therapeutic response is proportional to concentration of drug at _____________
site of action
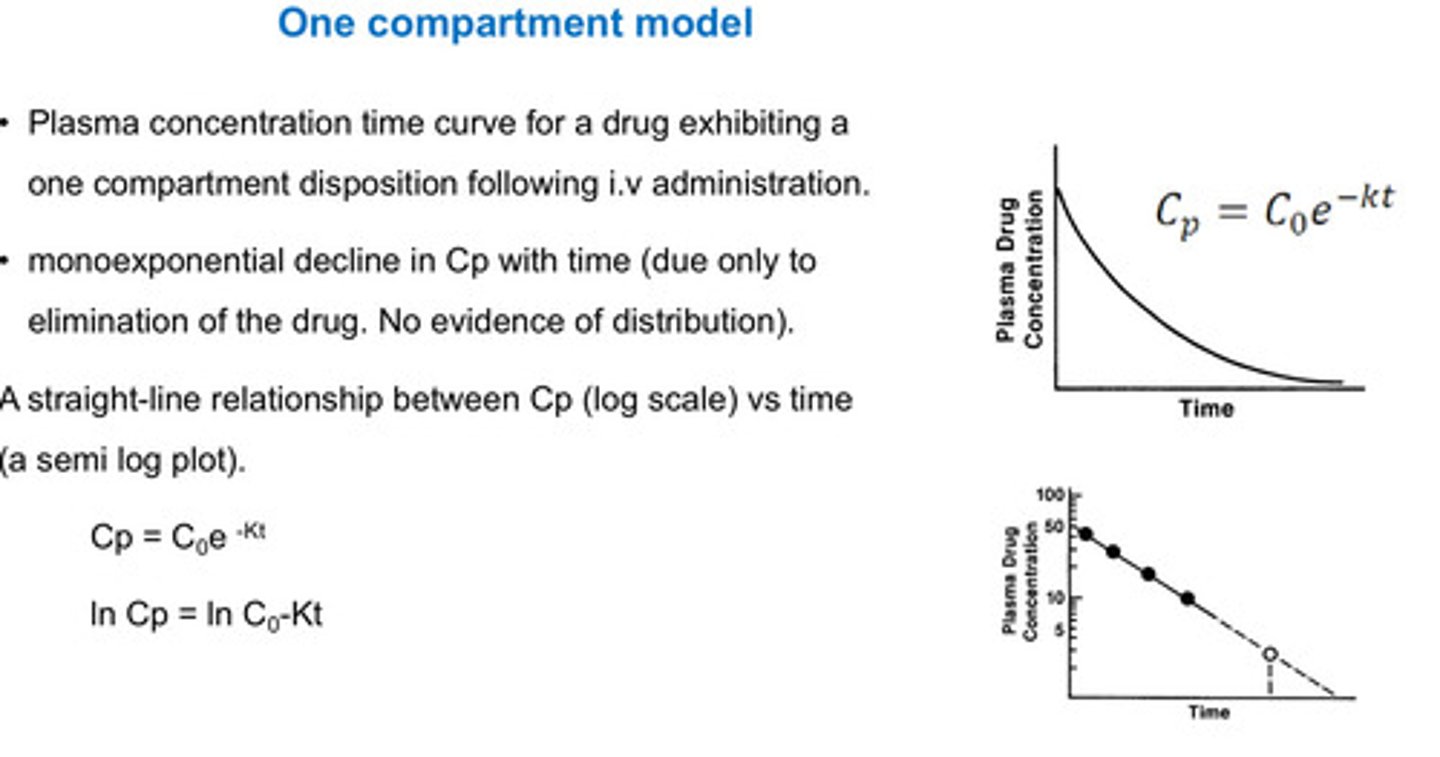
concentration vs time curve
y axis:
x axis:
up/down shifts:
left/right shifts:
y axis: blood concentration
x axis: time
up/down shifts: intensity of response
left/ right: time/half life
what methods are used to collect data for a concentration time curve
blood, spinal fluid, synovial fluid, biopsy, urine, feces, expired air
blood vs plasma vs serum
blood: has RBC, WBC, platelets, proteins
serum: plasma + clotting factors
plasma: no clotting factors
t/f: when blood is collected, drug molecules are in the water portion of blood
true. not talking about drugs bound to RBCs or anything like that. refer to drugs in the plasma
t/f: it is impossible to determine the total amount of drug present in the body or at the target site by direct methods
true. even if we take blood sample, we do not know total body concentration of drug. some of drug is in blood, at target, sequestered, not absorbed, etc
in concentration vs time curve,
what does positive slope mean?
negative slope?
positive slope means as time increases, concentration increases= absorption exceeds elimination
negative slope means as time increases, concentration decreases= elimination exceeds absorption
in concentration vs time curve,
what does a peak/horizontal line mean?
elimination and absorption are equal
explain why a change in plasma concentration reflects a change in tissue concentration
bc drug in plasma is in equilibrium w drug in tissue (as plasma concentration changes, drug will redistribute)
- less in blood means less will get into tissue
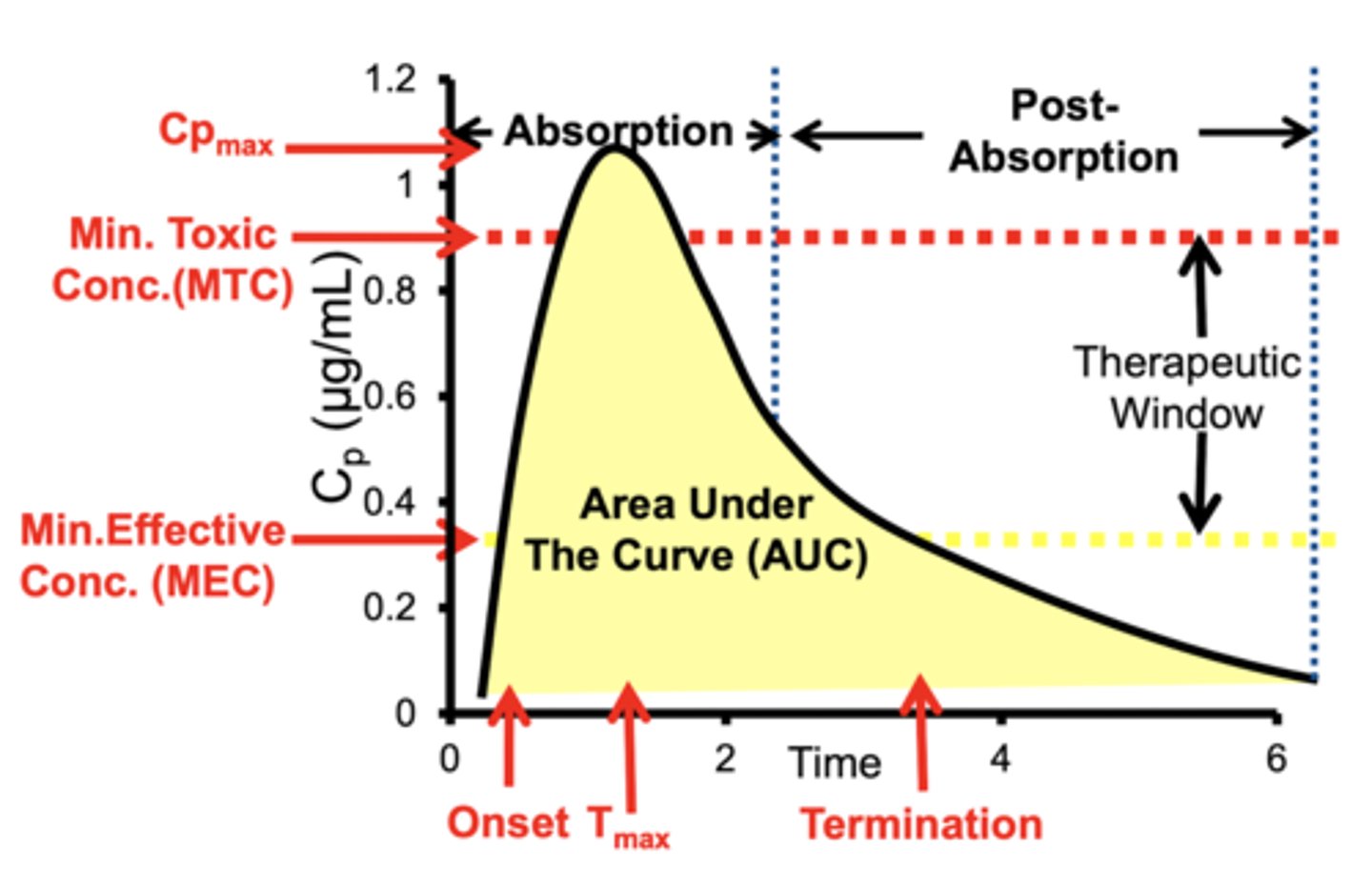
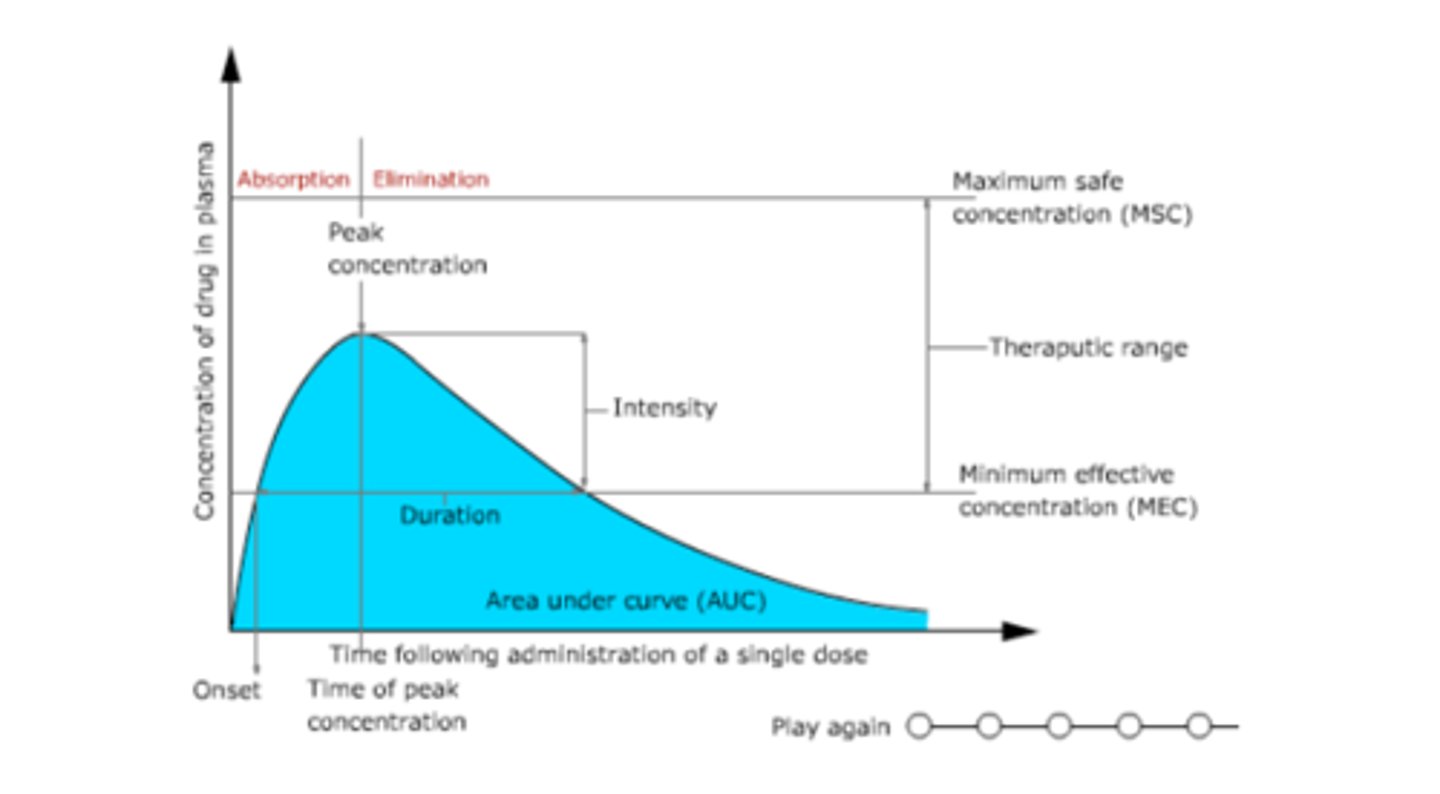
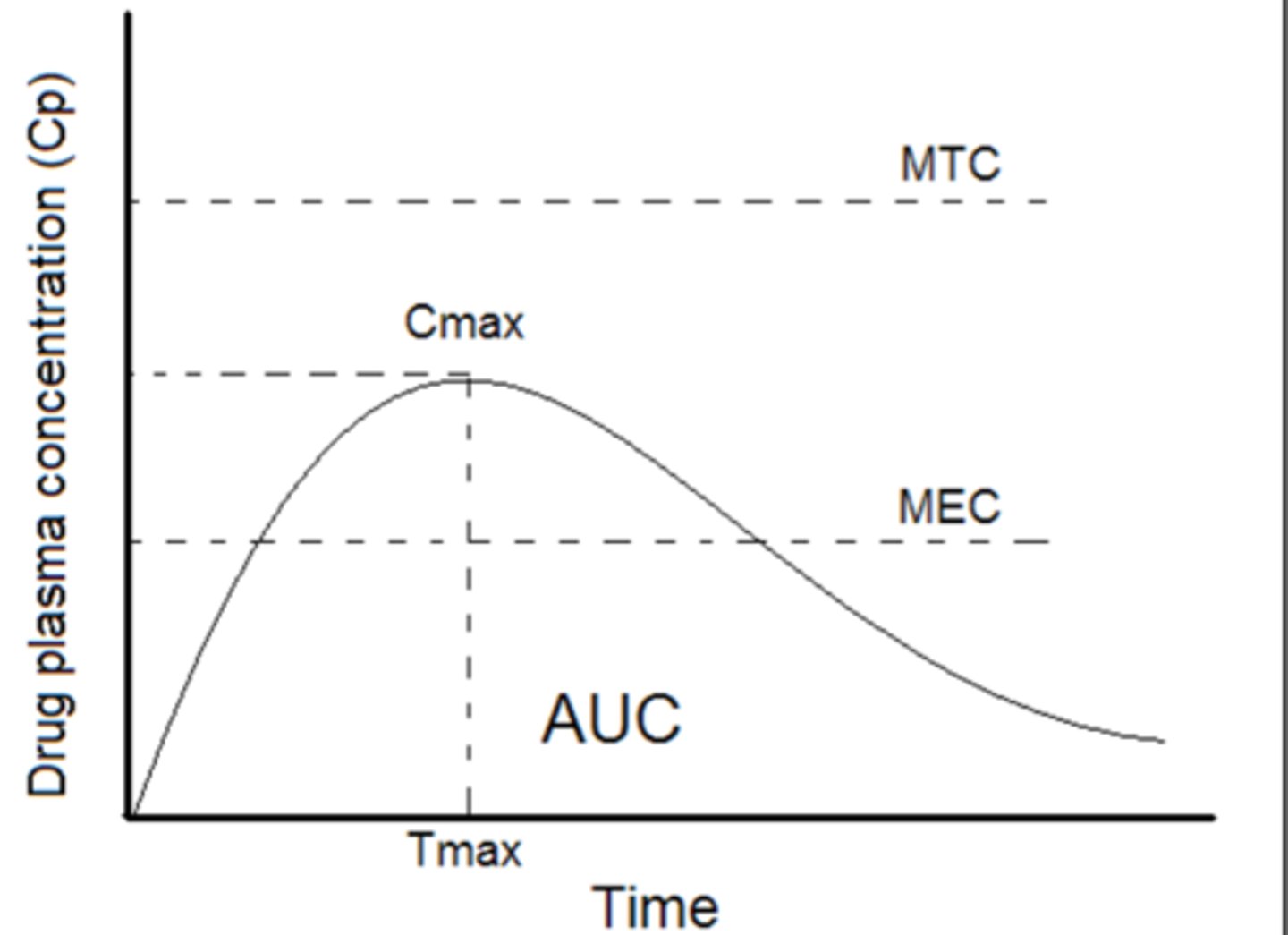
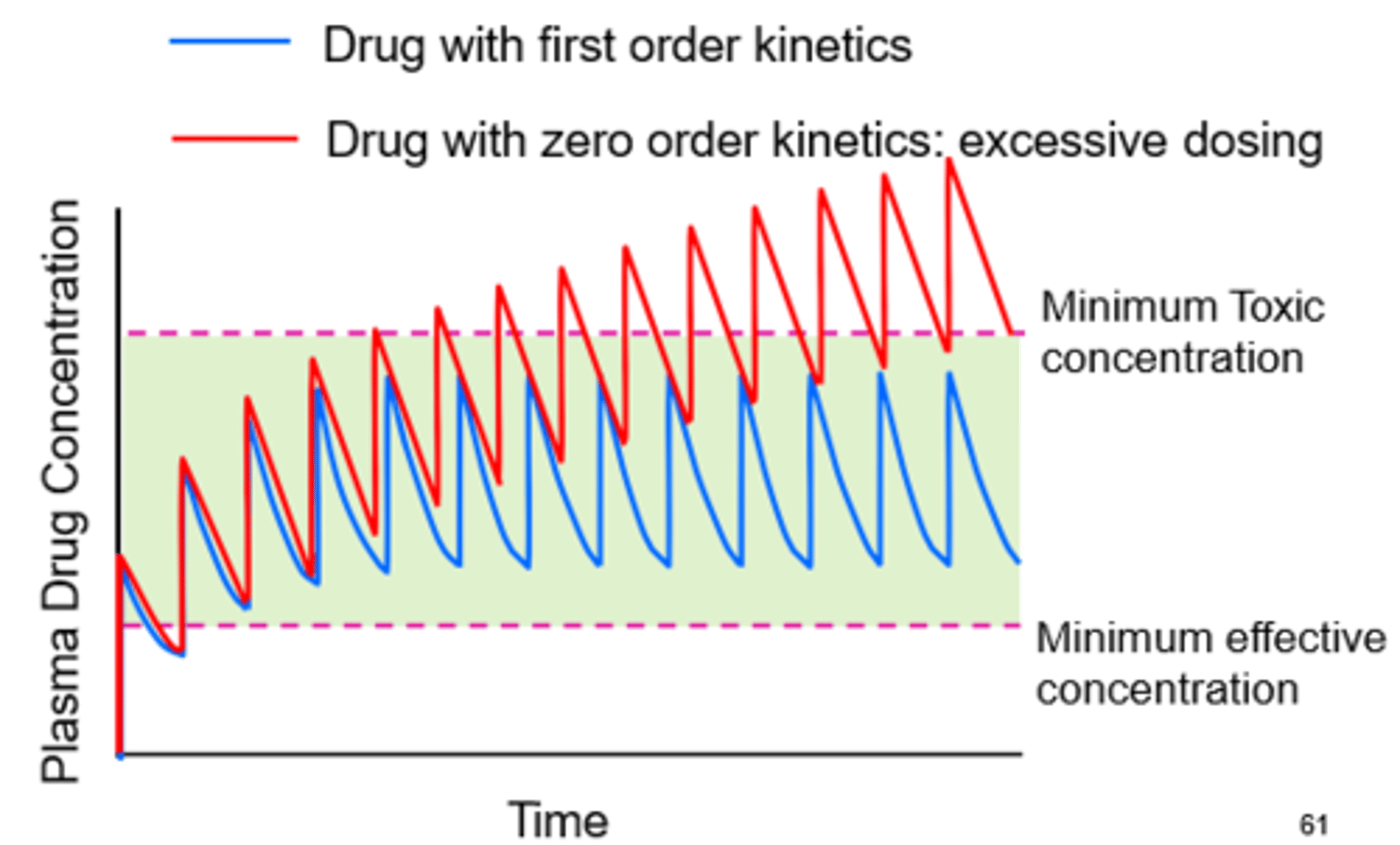
MEC
Minimum effective concentration - the plasma drug level below which therapeutic effects will not occur.
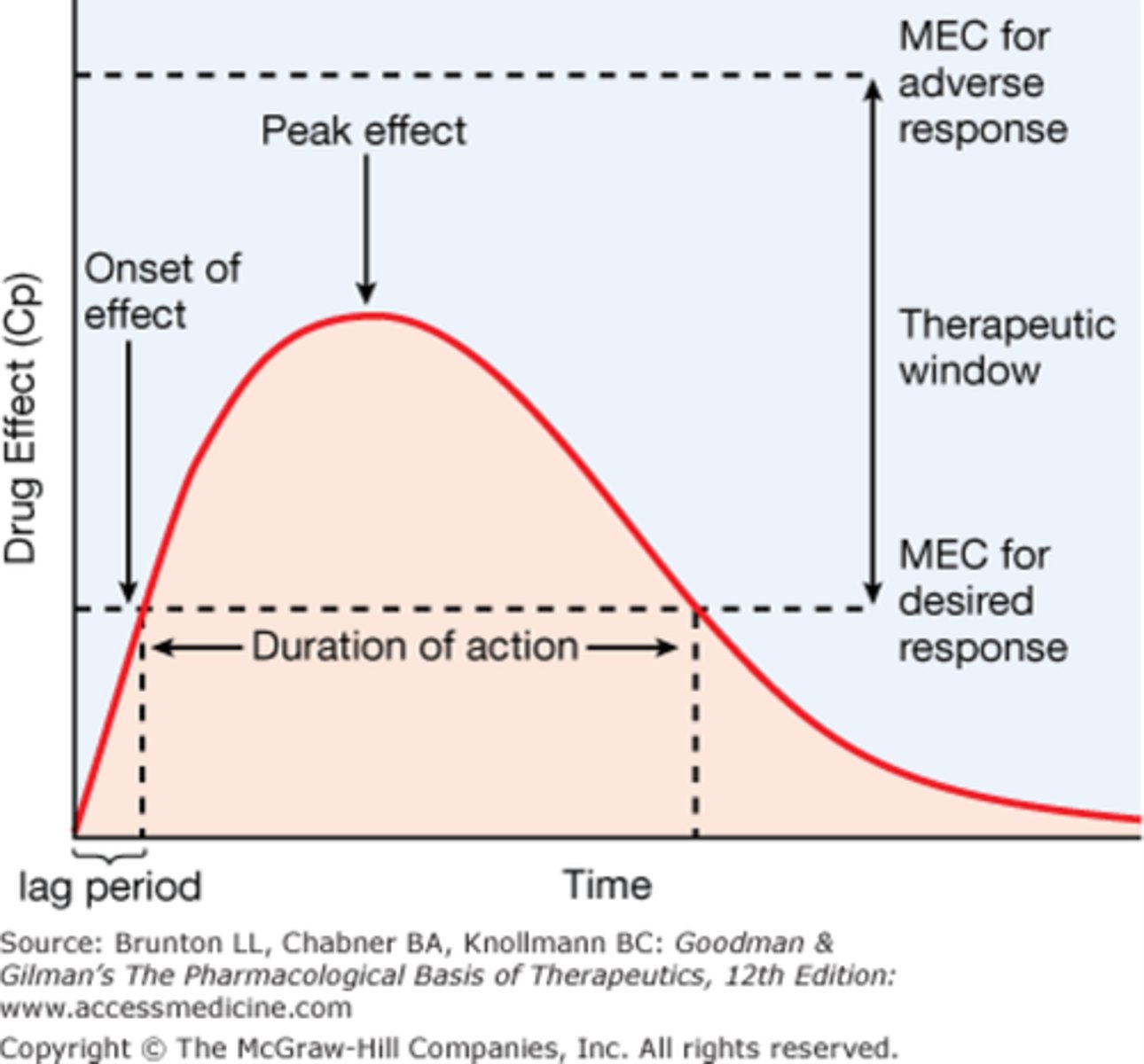
MTC
Minimum toxic concentration; the lowest concentration at which a toxic effect is achieved.
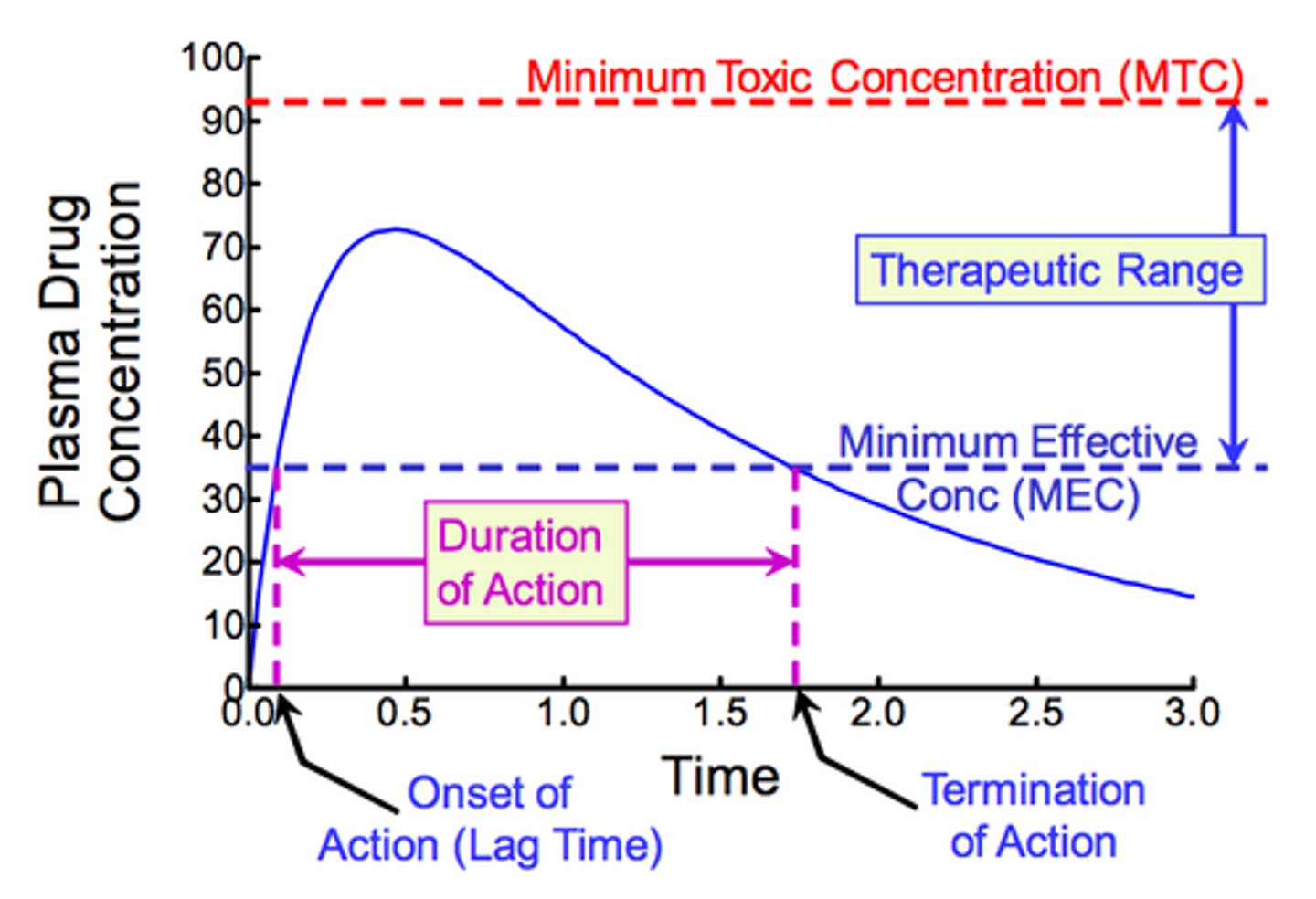
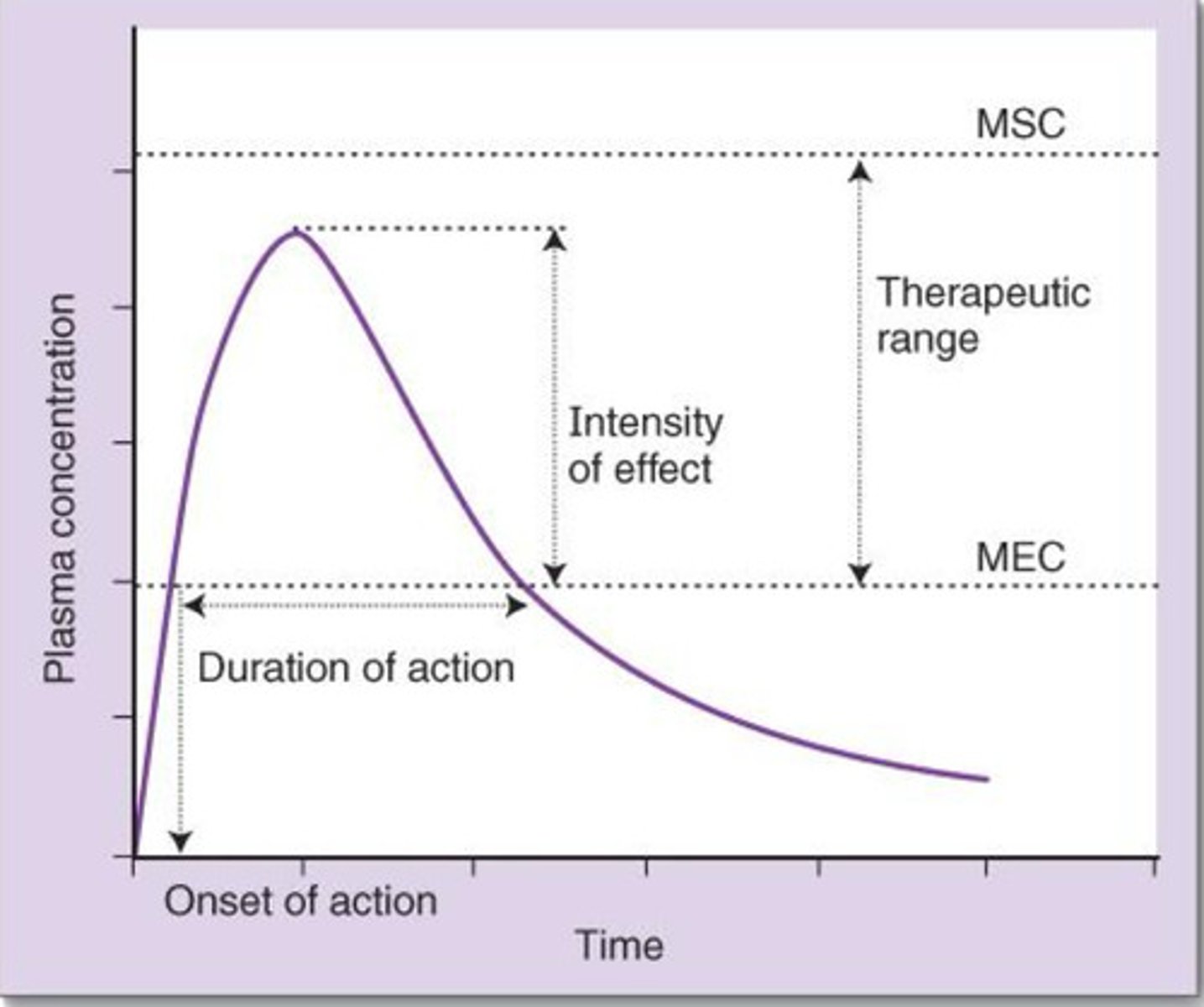
how can you establish the duration of action of a drug looking at a concentration vs time graph
the duration of time the drug remains above MEC
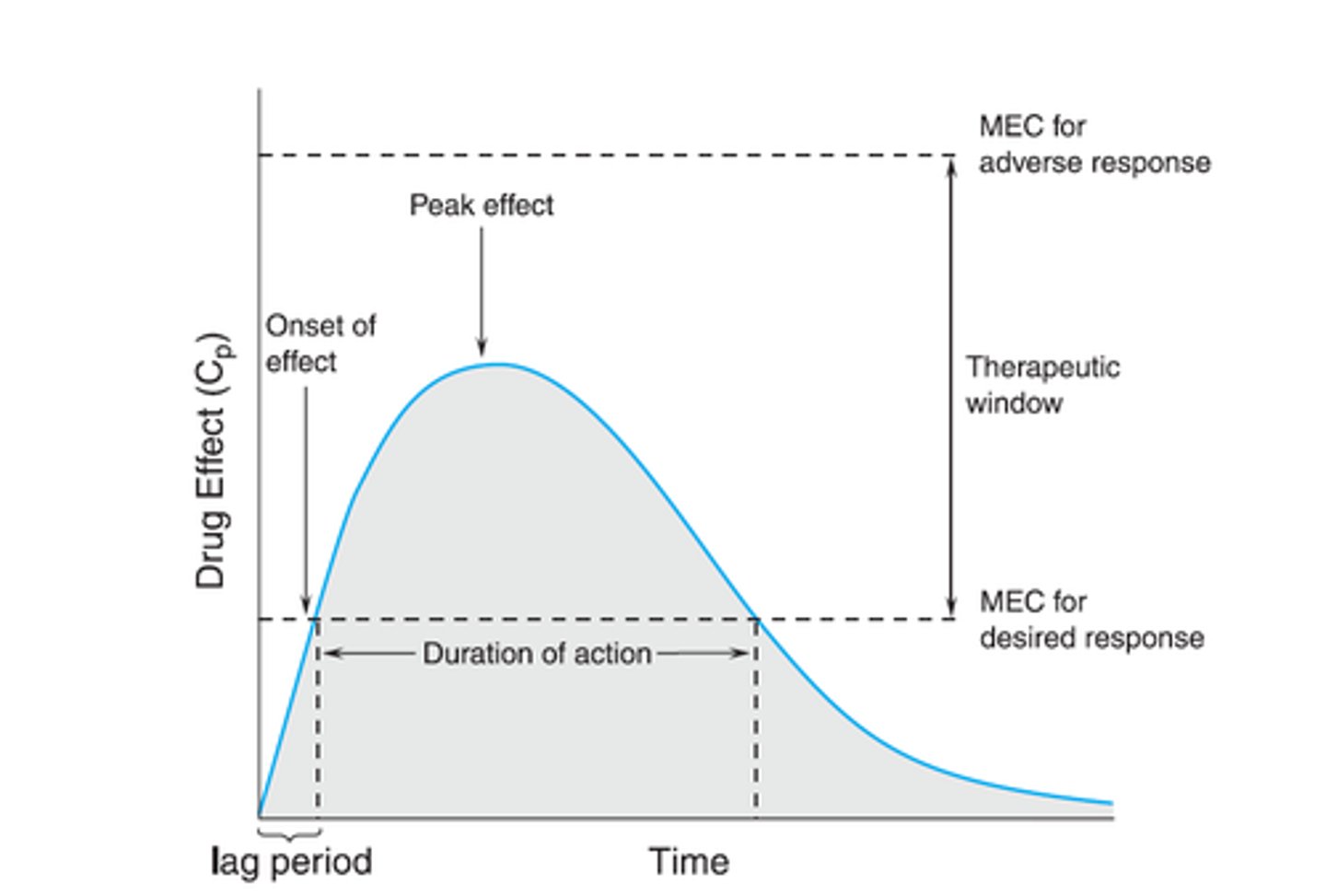
how can you establish the onset of action of a drug looking at a concentration vs time graph
how long it takes drug to reach the MEC level
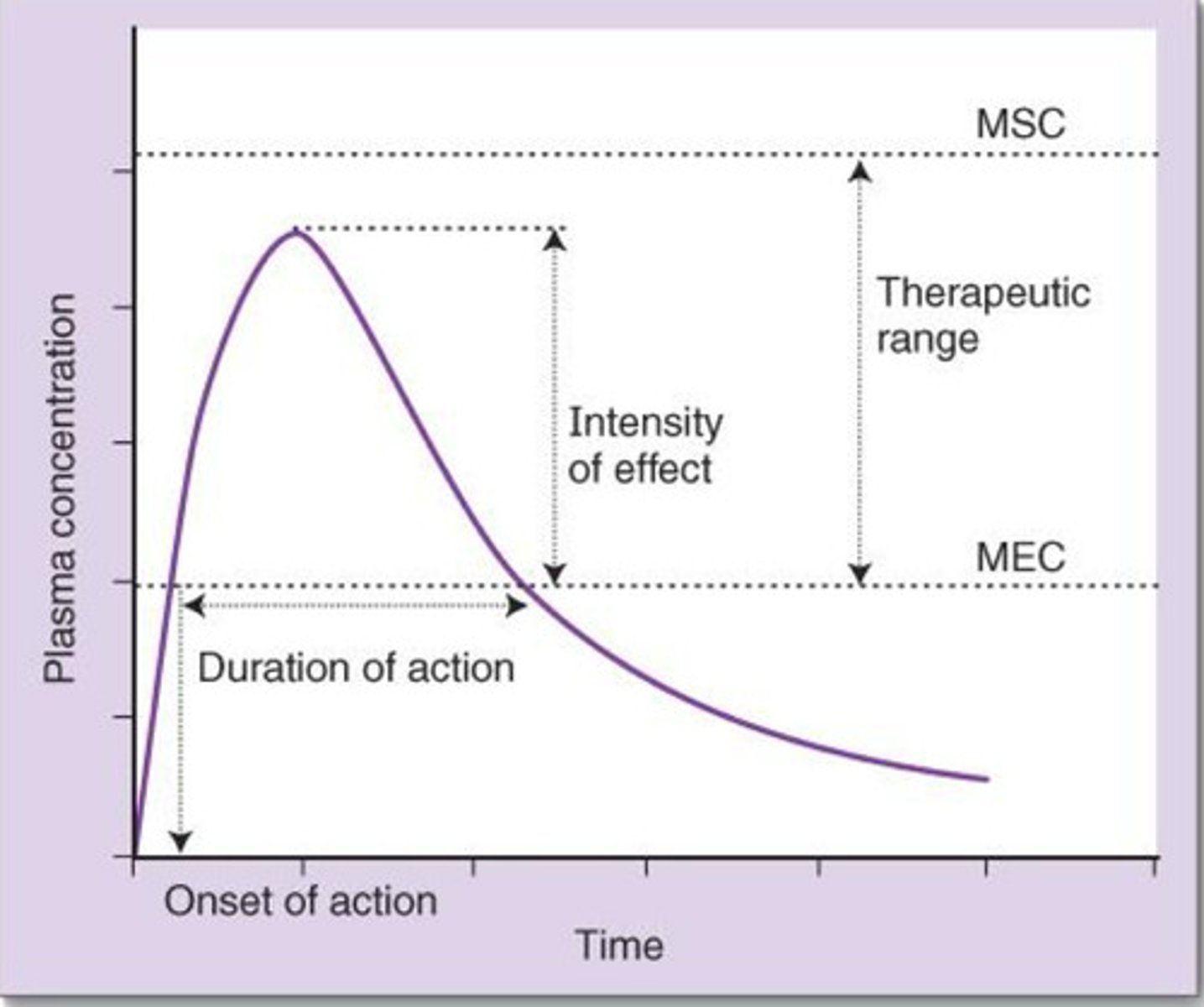
t/f: the MEC may not be the therapeutic response we want to achieve
true. MEC is just the beginning of therapeutic response. the peak from MEC is the intensity and determines max effect (proportional to plasma concentration)
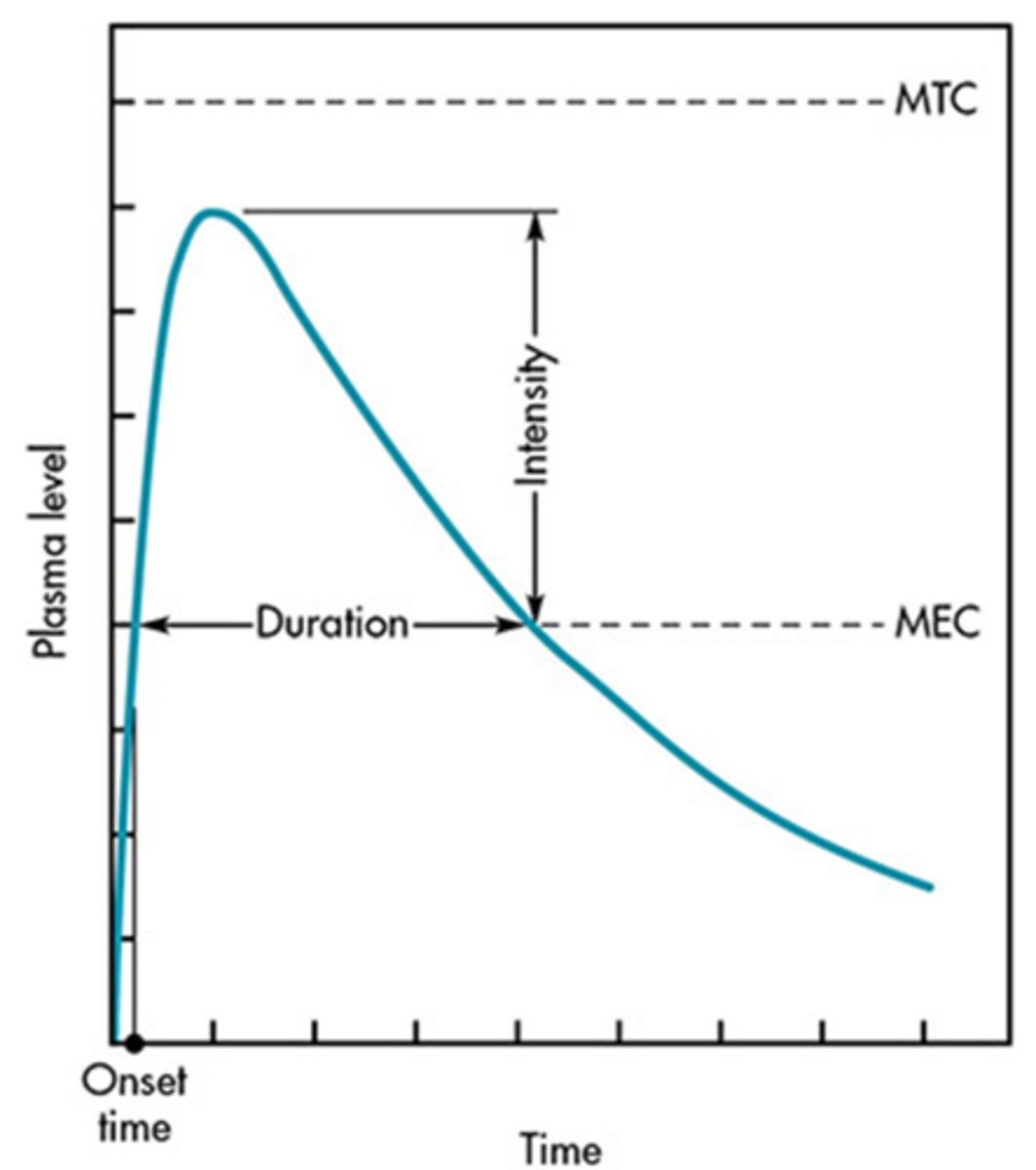
intensity of a drugs response is proportional to ____________
plasma concentration
t/f: the duration of action is the time from onset to full elimination
false. its the time spent in MEC. once its below MEC it is not considered in duration
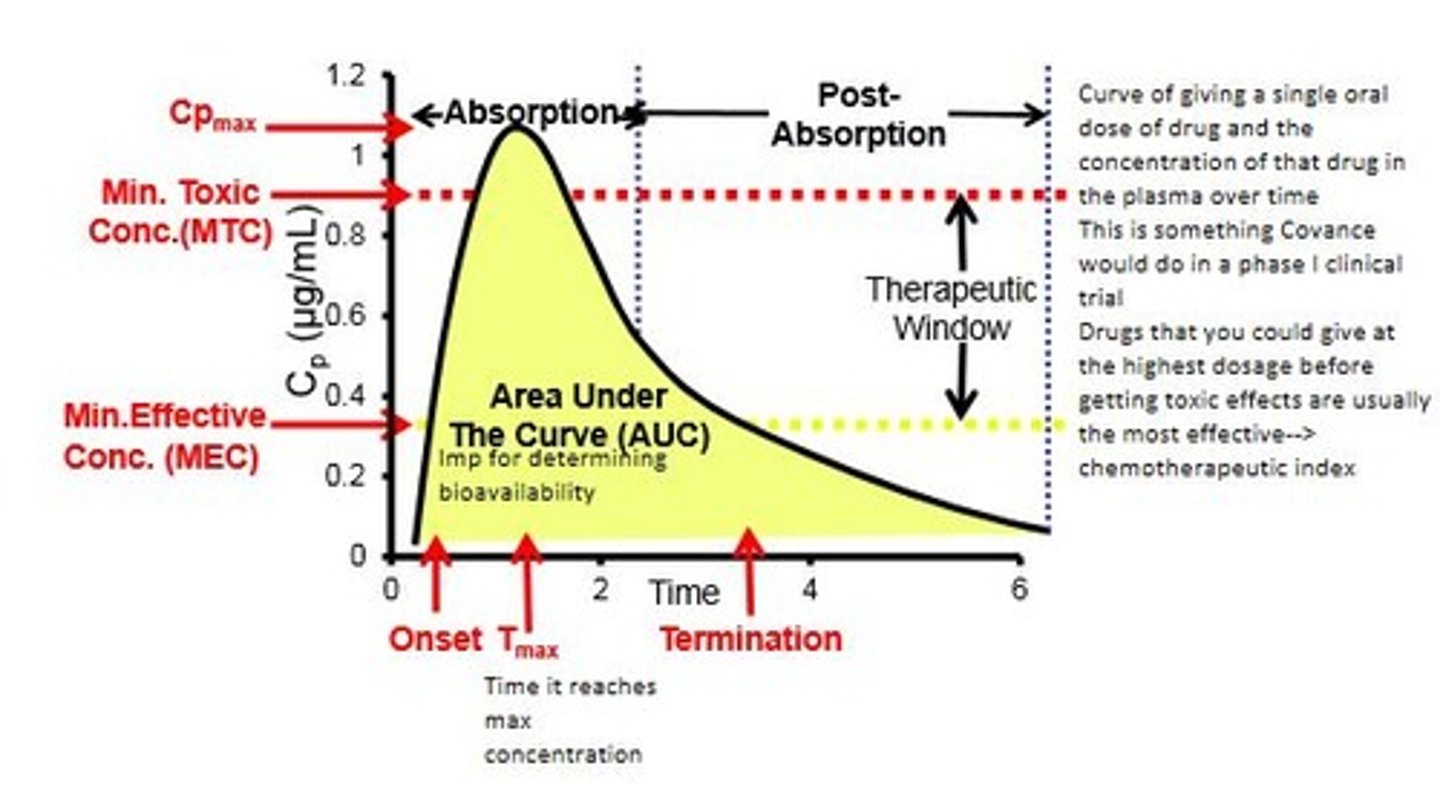
AUC
area under the curve; represents the amount of drug absorbed systemically
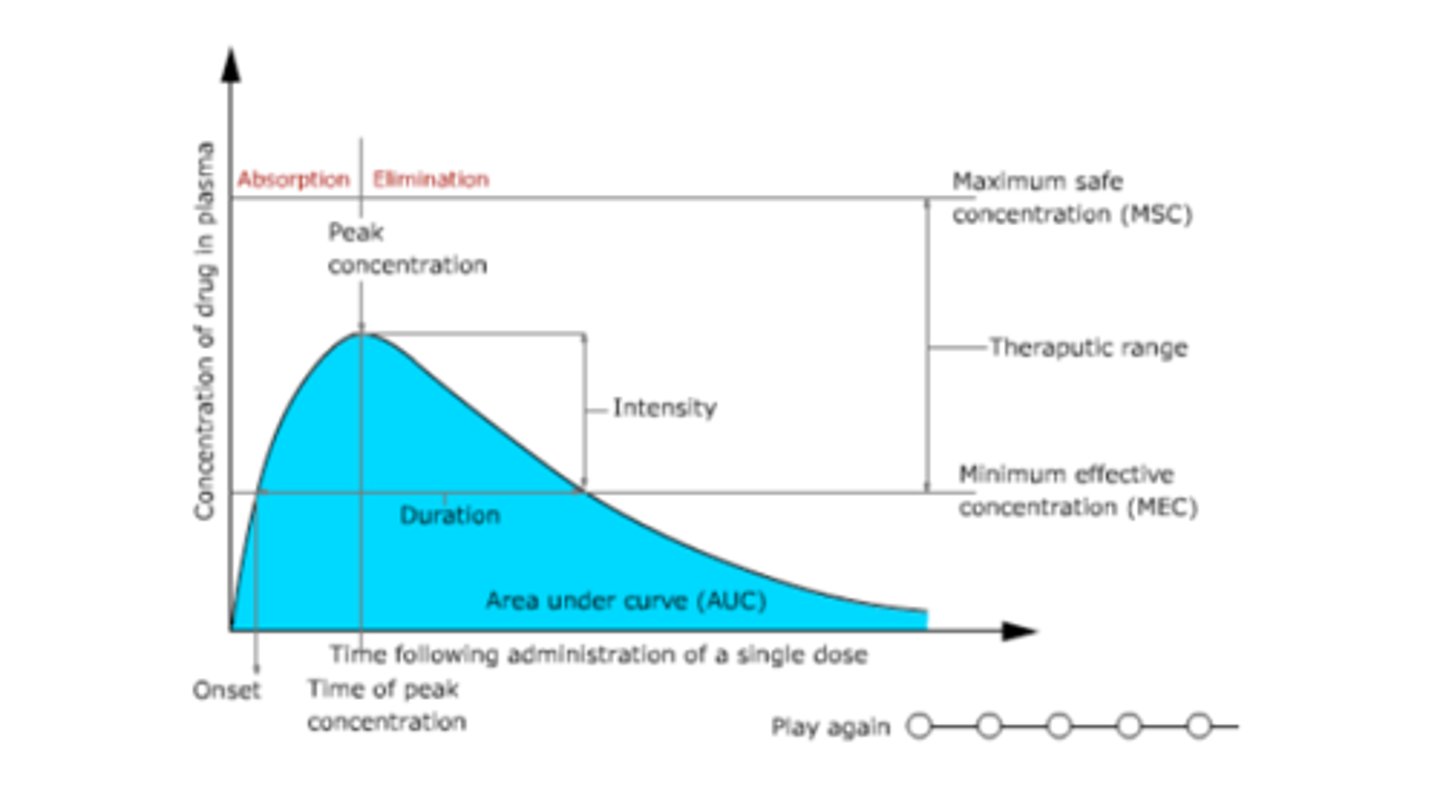
given a ct curve, what represents the amount of a drug that is absorbed in the body
AUC
an IM injection would shift the CT curve _______ (compared to oral)
left
(less time needed for same amount of absorption== going straight into blood)
(not up/down bc same amount is still absorbed)
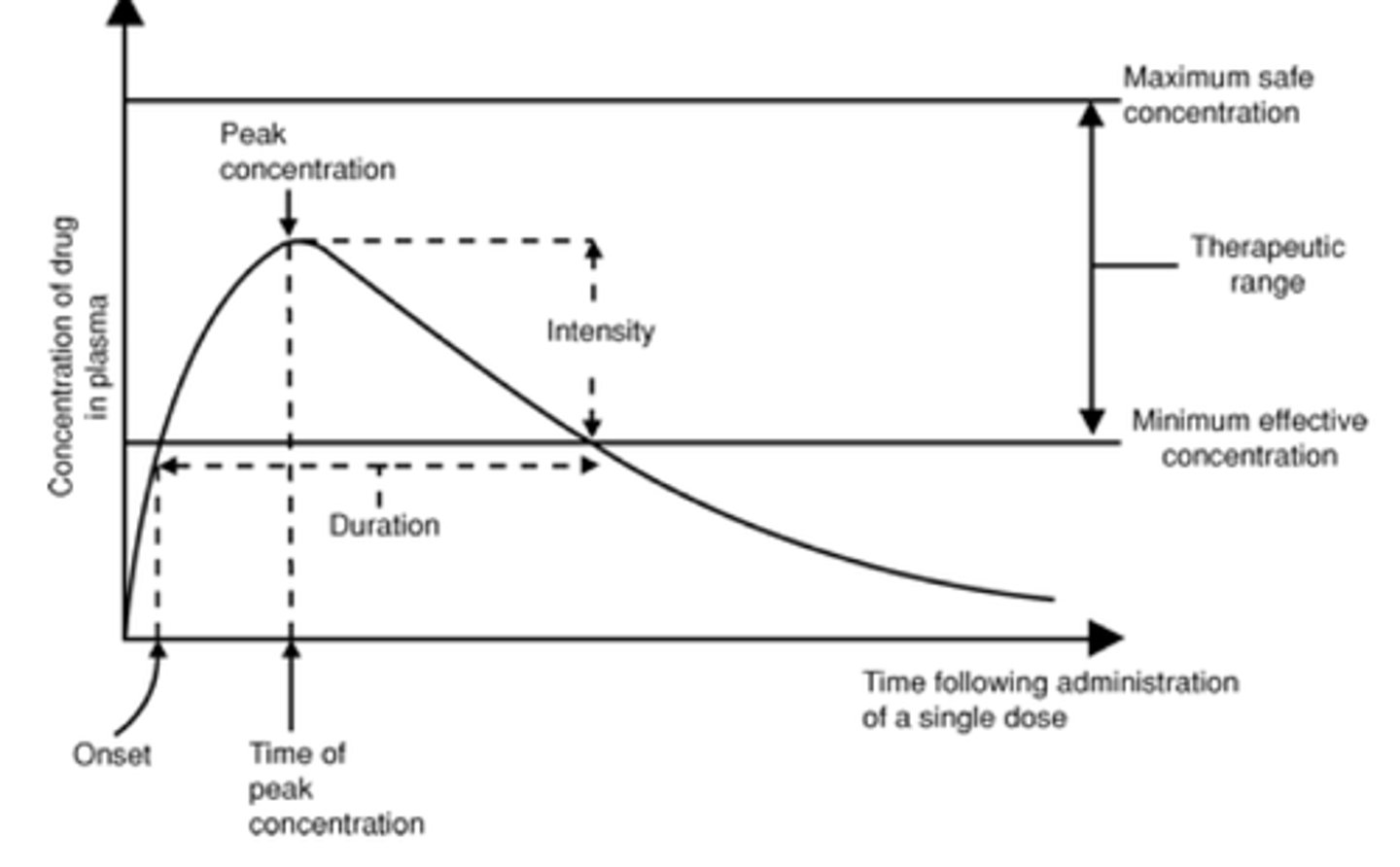
peak time and peak absorption in a ct curve
peak time (Tmax): time it takes to reach max concentration
- marker of rate of drug absorption
peak absorption (Cmax): the max concentration
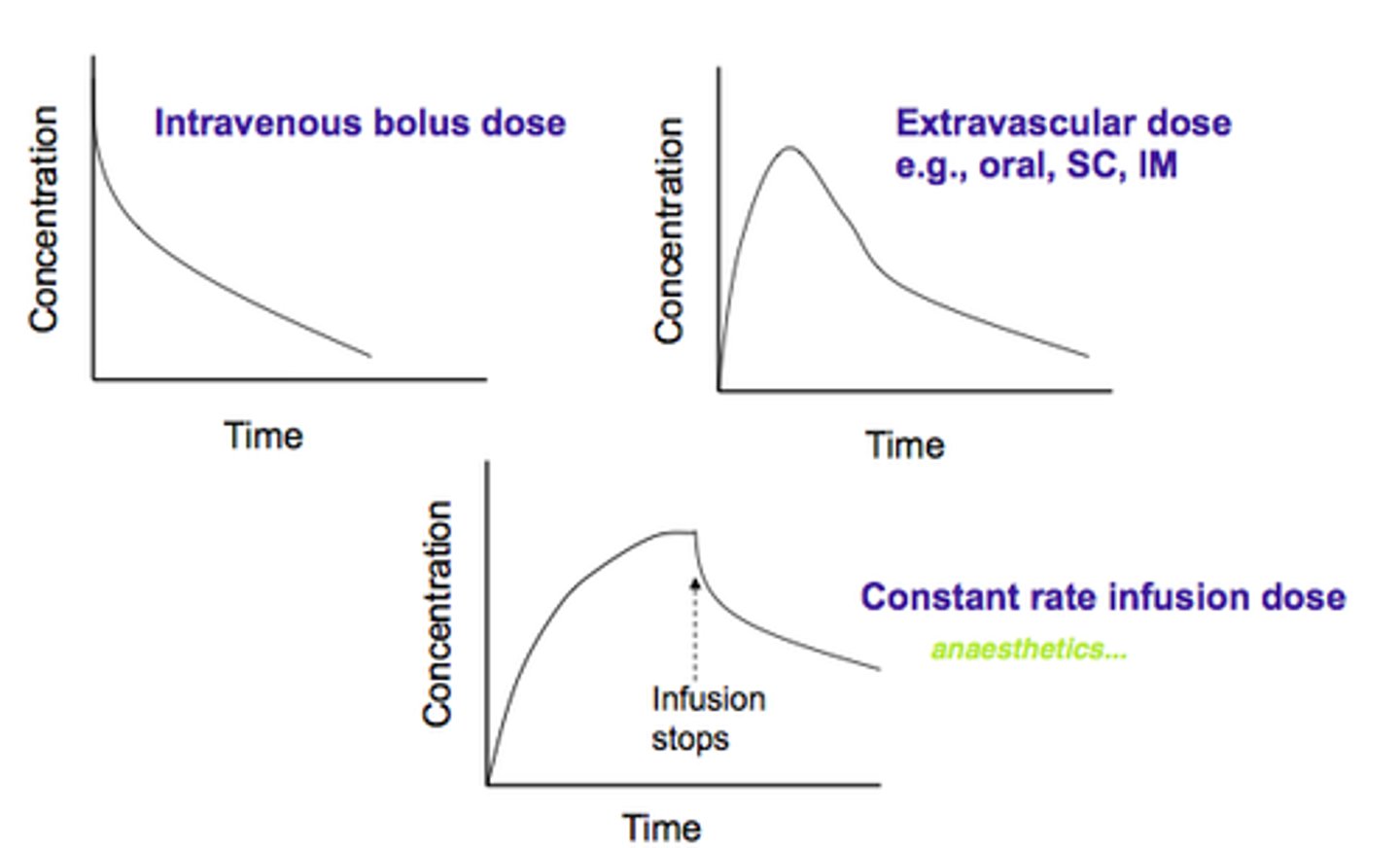
a ct curve starts high and has a negative slope until it gradually becomes horizontal. this is indicative of
a. IM
b. IV bolus
c. IV constant infusion
d. oral
b. IV bolus
bc its going straight to blood. it does not need to be absorbed
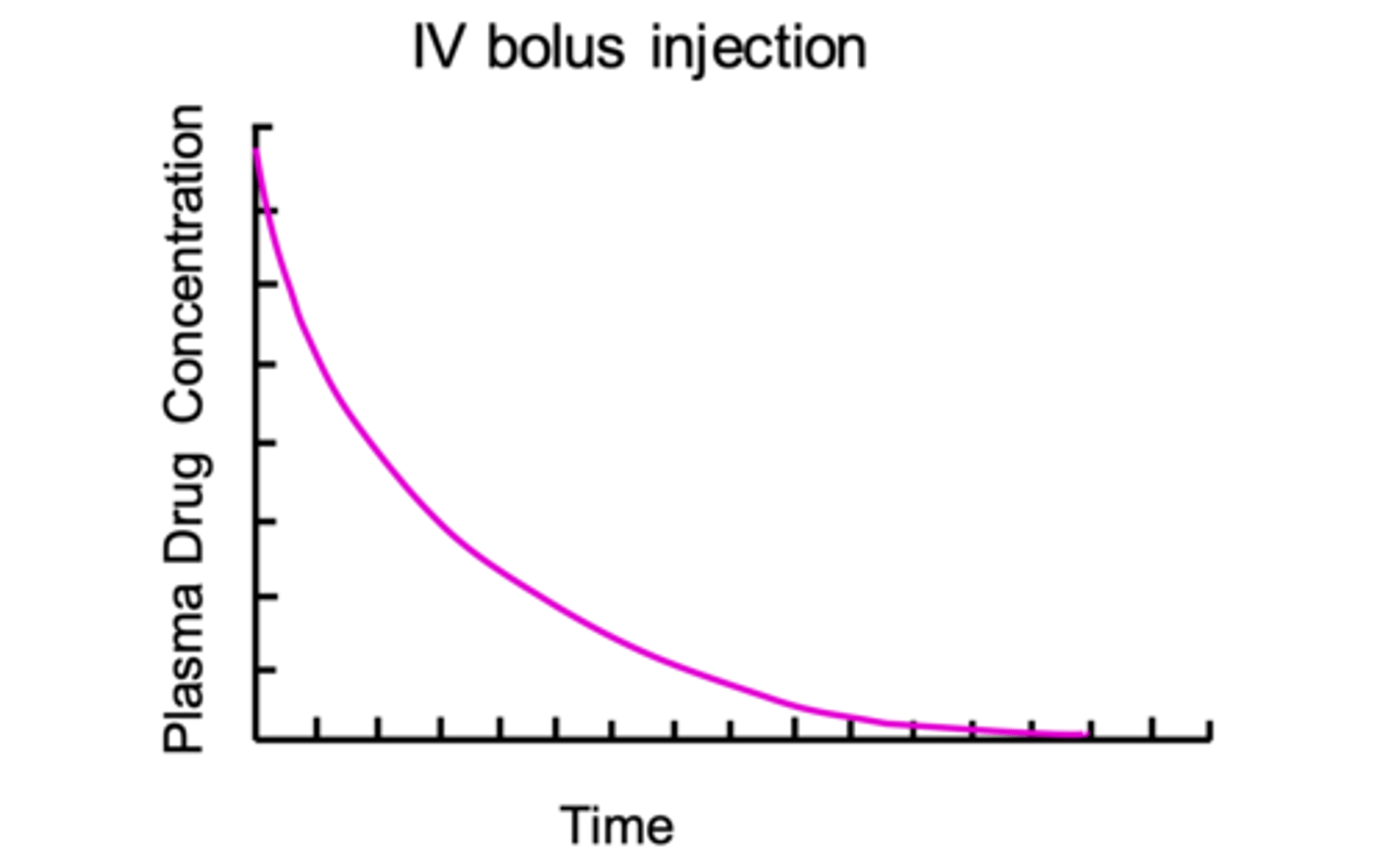
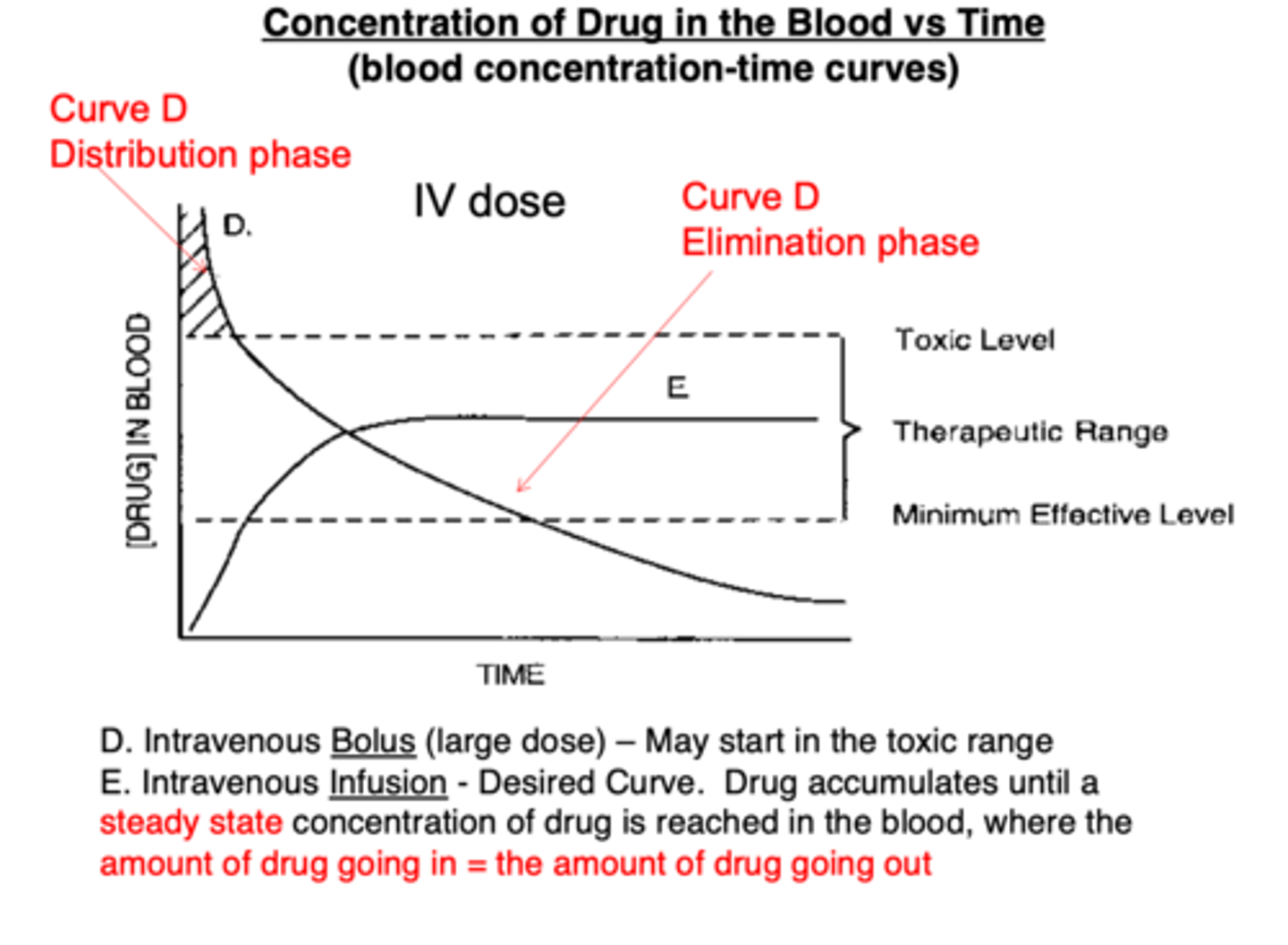
IV bolus vs constant infusion concentration time curve
IV bolus: will start off high and gradually lower
constant IV: will start at 0, increase, then plateau to maintain constant concentration level
what would shift a curve downwards?
a. greater absorption
b. greater elimination
c. more drug administered
d. drug given orally instead of IM
b. greater elimination
a downward shift == lower drug levels in plasma. greater elimination (via metabolism or excretion) would reduce the drug concentration, shifting the curve downward
since the response to a drug is related to the concentration of drug at target site, it is also related to ___________
plasma concentration (bc of equilibirum)
2 types of plasma concentration vs effect curves
graded= increment in physiologic or biochemical response as dose or concentration is increased
quantal= percent of the population under study that has a response as the dose is increased
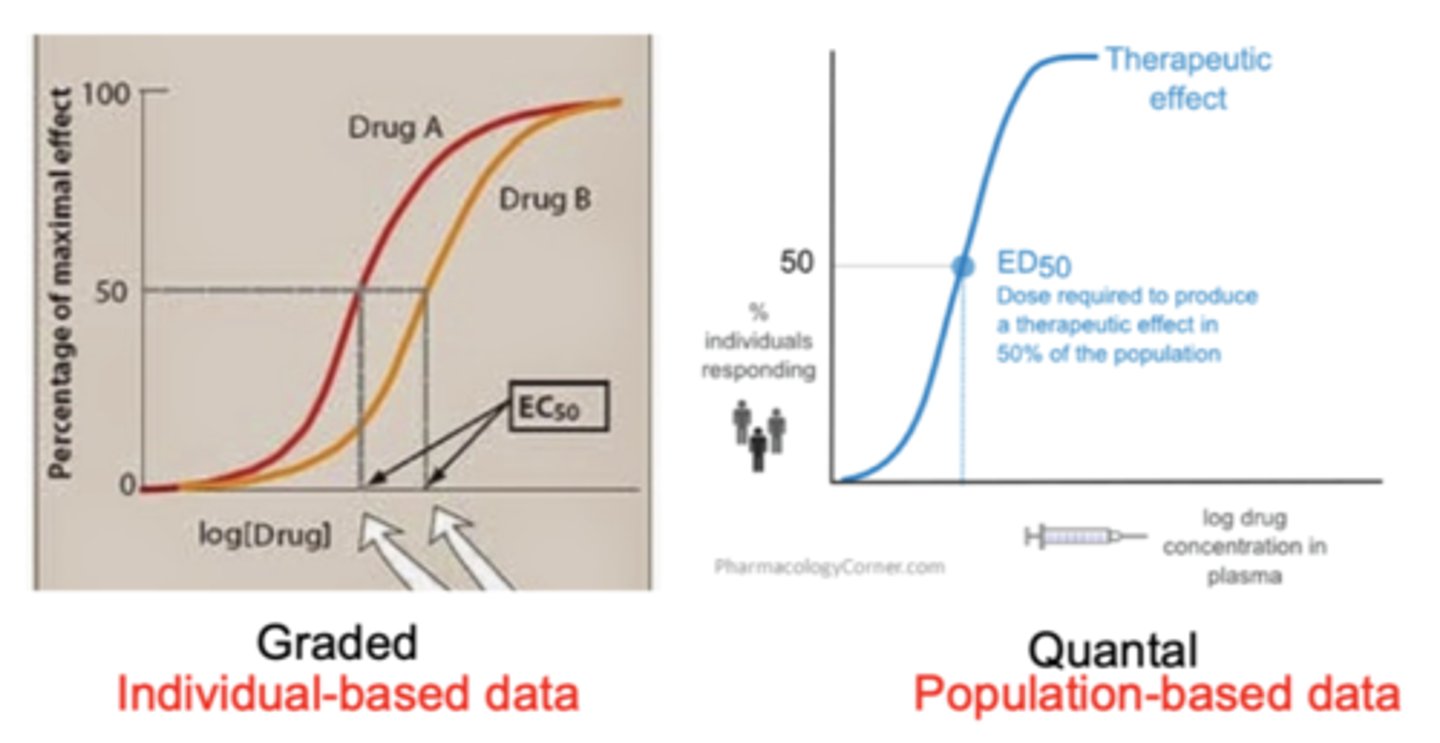
which type of response is this:
response to drug is proportional to concentration and is usually reversible
a. graded response
b. quantal response
a. graded
a reduction in blood pressure with antihypertensives would be an example of
a. graded response
b. quantal response
a. graded response
t/f: a graded response is usually reversible if the concentration of the drug is lowered
true
which type of response is this:
response to drug is only elicited when drug concentration is higher than a certain critical concentration
a. graded response
b. quantal response
quantal
which response is known as an all or none response
a. graded response
b. quantal response
b. quantal
t/f: a drug exhibiting a quantal response may be irreversible
true
examples of quantal responses
death, hypotensive toxicity of antihypertensive agents
a graph displaying plasma concentration vs percent of population with effect is
a. graded response
b. quantal response
b. quantal
(there either is or isnt an effect. a graded response has magnitude of effect)
t/f: in the concentration effect curve, the plateau that we see in terms of effect is the therapeutic effect we are looking for
false. may or may not be therapeutic effect. may have too much toxicity, especially as concentration increases and plateau remains
(minor/major toxicity is actually what drags the effectiveness line down)
t/f: whether you give 1x, 10x, or 100x of a drug dose, then concentration time curve shape will be identical if its same route of administration
true. shape of curve and half life is identical.
BUT maximum concentration will be different (y asymp increases)
t/f: whether you give 1x, 10x, or 100x of a drug dose, then concentration effect curve shape will be identical if its same route of administration
false. effect is higher with higher concentration
[but compare to concentration time curve, where the curve IS the same shape, just different y asymp]
what is the negative slope of a concentration time curve also known as
half life (or elimination rate)
t/f: when compared to 1x of a drug, a 100x drug concentration will have a longer half life
false. half life is the same bc first order kinetics depends on % of concentration, not a certain amount
the rate of drug eliminated from the kidney is
a. lower at 1000x
b. higher at 1000x
c. same at 1000x
c. same
(rate of drug eliminated is the same but the AMOUNT of drug molecules is higher)
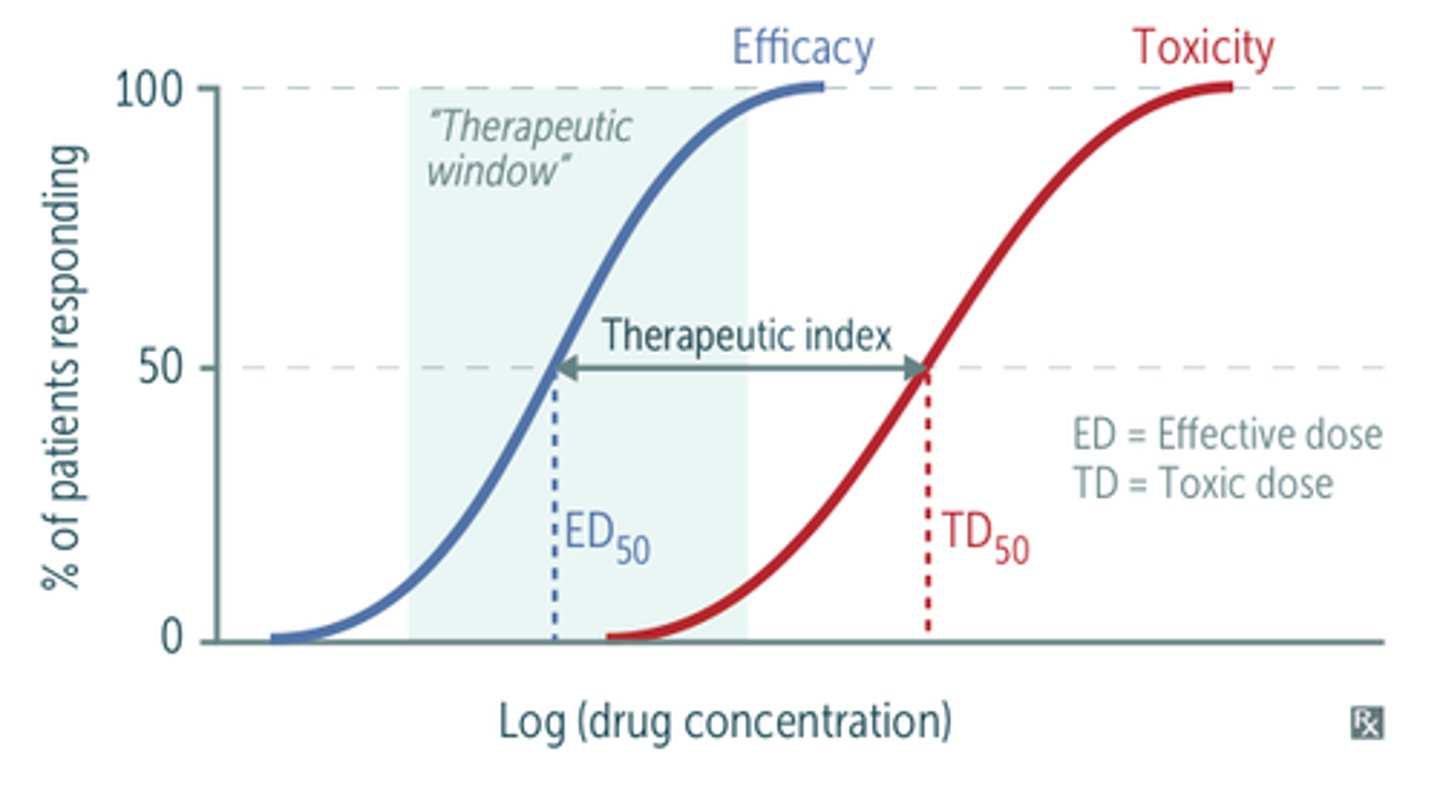
ratio of the dose needed to produce a TOXIC effect and the dose needed to elicit DESIRED therapeutic response is known as the _______________
therapeutic index (TI)
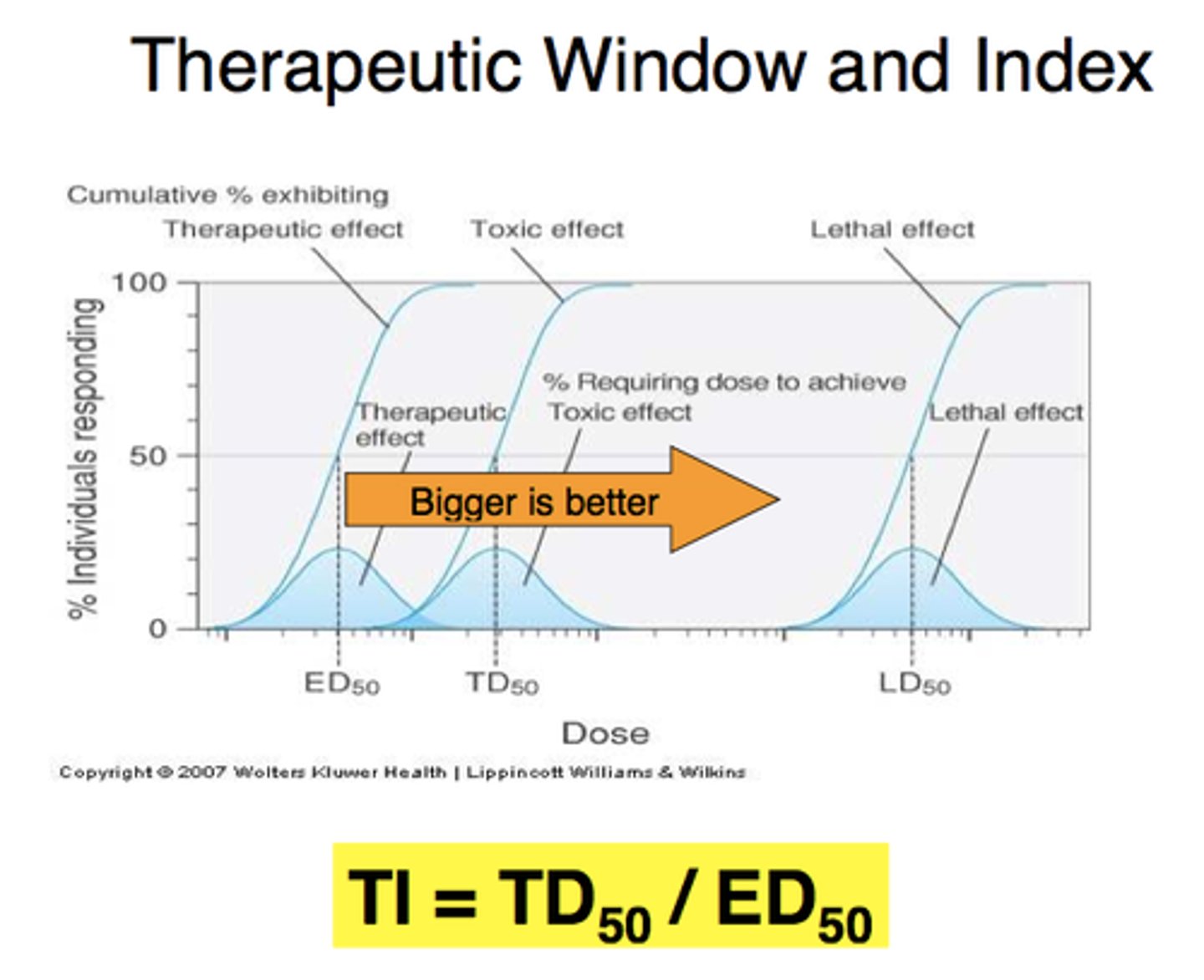
t/f: a large TI indicates higher safety
true. large TI (therapeutic index) means large margin between therapeutic and toxic line
t/f: when applying the vertical line test to a quantal graded response curve, if the line does NOT bisect BOTH the desired therapeutic effect and the adverse effects, then there is a larger therapeutic index compared to if they do bisect
true. if they do bisect then therapeutic effect and adverse effects are overlapping= narrow TI
when may response-time curves be more useful than concentration-time curves
when concentrations dont correlate with response
ex: topical creams. we dont know the concentration of a topical on the skin, so response-time curves may be more beneficial
also: anticancer drugs, anticoagulants, digoxin
cases where plasma concentration does NOT correlate with response (overall summary)
- active metabolites (prodrug)
- chirality-structural activity responses
- tolerance and acquired resistance
- single dose therapy (once it returns to homeostasis, concentration doesnt matter)
- duration vs intensity of therapy
- time delays
drug x is more active when given orally than when given IV. what can this indicate?
drug x is a prodrug w active metabolites. therefore the first pass effect is needed for the drug to be active. IV bypasses this
t/f: if a drug has an active metabolite, it is likely that plasma concentration does not correlate with response
true. if the metabolite is active then we need to measure the concentration of the metabolite as well (not just og drug) to determine response
(ex: amitriptyline and its desmethyl metabolite)
t/f: the R and S enantiomers of a drug do not usually differ in PK and PD
false. enantiomers usually differ. this is why plasma concentration of the total drug may not correlate w response [need to distinguish how much of isomer is in plasma]
explain why plasma concentration of drugs w enantiomers (chirality SAR) does not correlate with response
plasma concentration will show both the R and S form but maybe only 1 is giving effect. so concentration of total drug does not correlate to effect. more specific assays must be done
what does it mean by "less negative elimination slope"
eliminated more slowly/ will be in body longer
__________ is the diminished response to same dosage of a drug, either developed slowly or acutely
tolerance
tolerance vs acquired resistance
tolerance: diminished response to same dosage of a drug, either developed slowly or acutely
- never complete tolerance
acquired resistance: diminished sensitivity of cells (bacteria/ cancer) to a drug
- could have total resistance
t/f: while the degree of tolerance varies but is never complete, acquired resistance may be totally resistant
true. bc bacteria and cancer cells can adapt to be completely resistant (more independant compared to pure physiology)
mechanisms of tolerance
1. decreased concentration of drug at target (we cant rlly measure this)
2. increased clearance rate (greater GFR, metabolism, induction)
3. pharmacokinetic adaptations (maybe not absorbed bc of food or interactions)
4. downregulation of receptors
downregulation
Decrease in receptor number in response to high concentration of drug
- may lead to tolerance to drug
t/f: plasma concentration does not correlate with response in single dose therapy
true. single dose therapy is used to return body to homeostasis. correlation may exist between effect and peak plasma concentration but no correlation beyond peak
if the target for a drug is H. pylori in the stomach, which choice would lead to higher success
a. slow absorption
b. fast absorption
a. slow absorption
we want the drug to stay in the stomach rather than getting absorbed. if its absorbed, then its in blood/lymph and wont be working on the target (h. pylori)
explain why methotrexate is a case where plasma concentration does not correlate with response
what is its response related to?
what does methotrexate do?
response relates more closely to the DURATION of dosing rather than the dose/concentration
methotrexate is an antimetabolite that inhibits the enzyme dihydrofolate reductase. inhibiting for short time is ok but long time= irreversible damage in all dividing cells
why may there be a time delay even if the drug is fully absorbed
must reach equilibrium at the site of action as well. not just site of absorption
(ex: max cardiac action of digoxin isnt seen until an hour after IV bolus)
IV bolus vs constant infusion
IV Bolus: A large dose is given all at once, leading to a rapid peak in drug concentration, which then declines over time
Constant Infusion: A drug is administered at a steady rate, maintaining a stable plasma concentration over time. Useful for drugs with a narrow therapeutic window or when continuous effect is needed.
why does warfarin take a couple of days to have its full effect
warfarin is a vitK antagonist that works by reducing the number of coag factors that the liver makes. warfarin wont work immediately bc we still have coag proteins initially. we need time for those proteins to decrease
t/f: sometimes a fluctuating concentration of antibiotics is more desirable than steady concentrations
true
(depends on bacteria. also dont want to disrupt fluora too much)
ex: ceftazidime doesnt have concentration-dependant killing
ex: gentamicin DOES depend on concentration. larger infrequent doses are more effective than small
if ceftazidime doesnt have concentration-dependant killing, how will the dose-response curve look? what type of kinetics is this?
horizontal line. ZERO ORDER KINETICS. response is constant regardless of concentration
(higher concentration will NOT correlate to amount of bacteria killed)
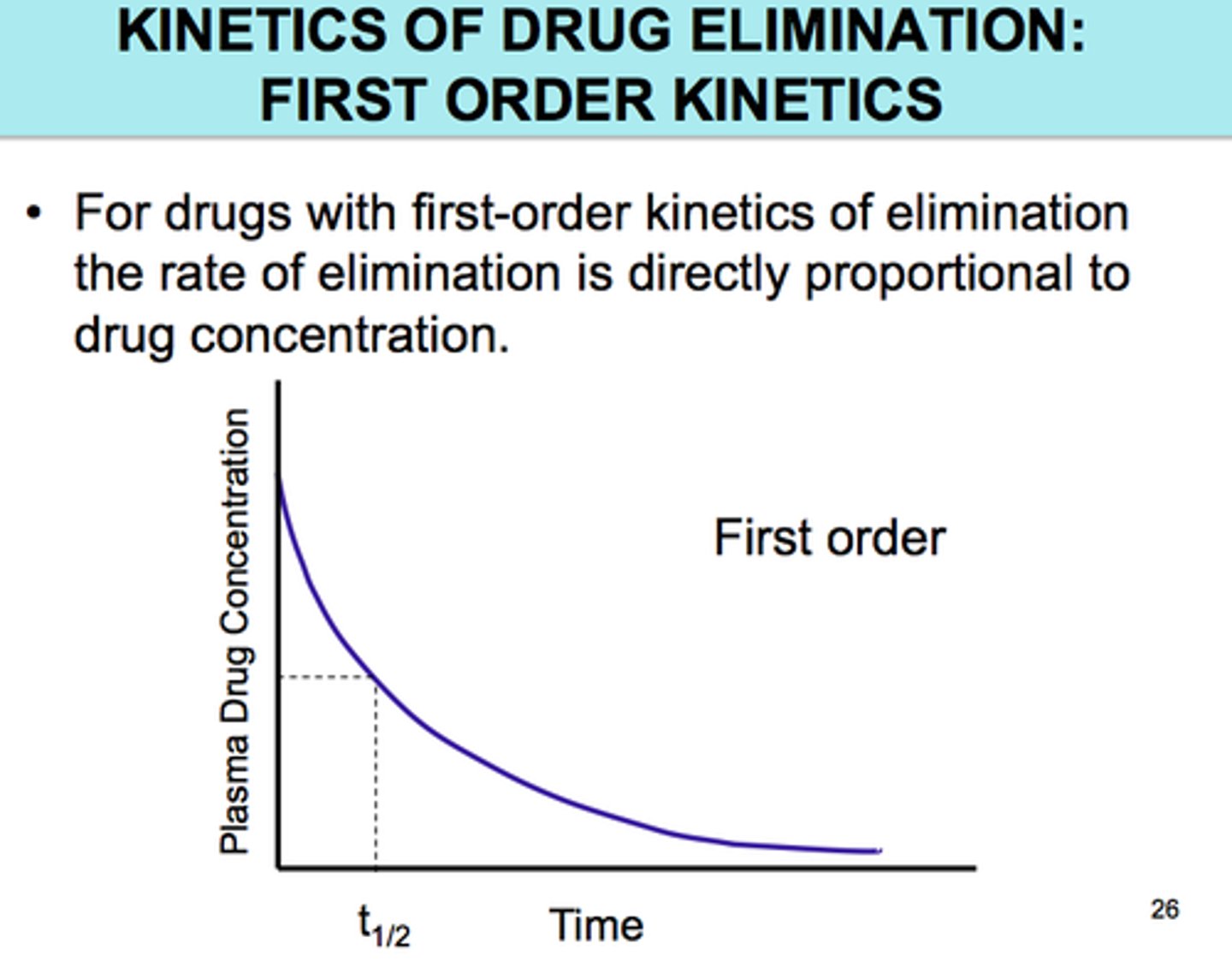
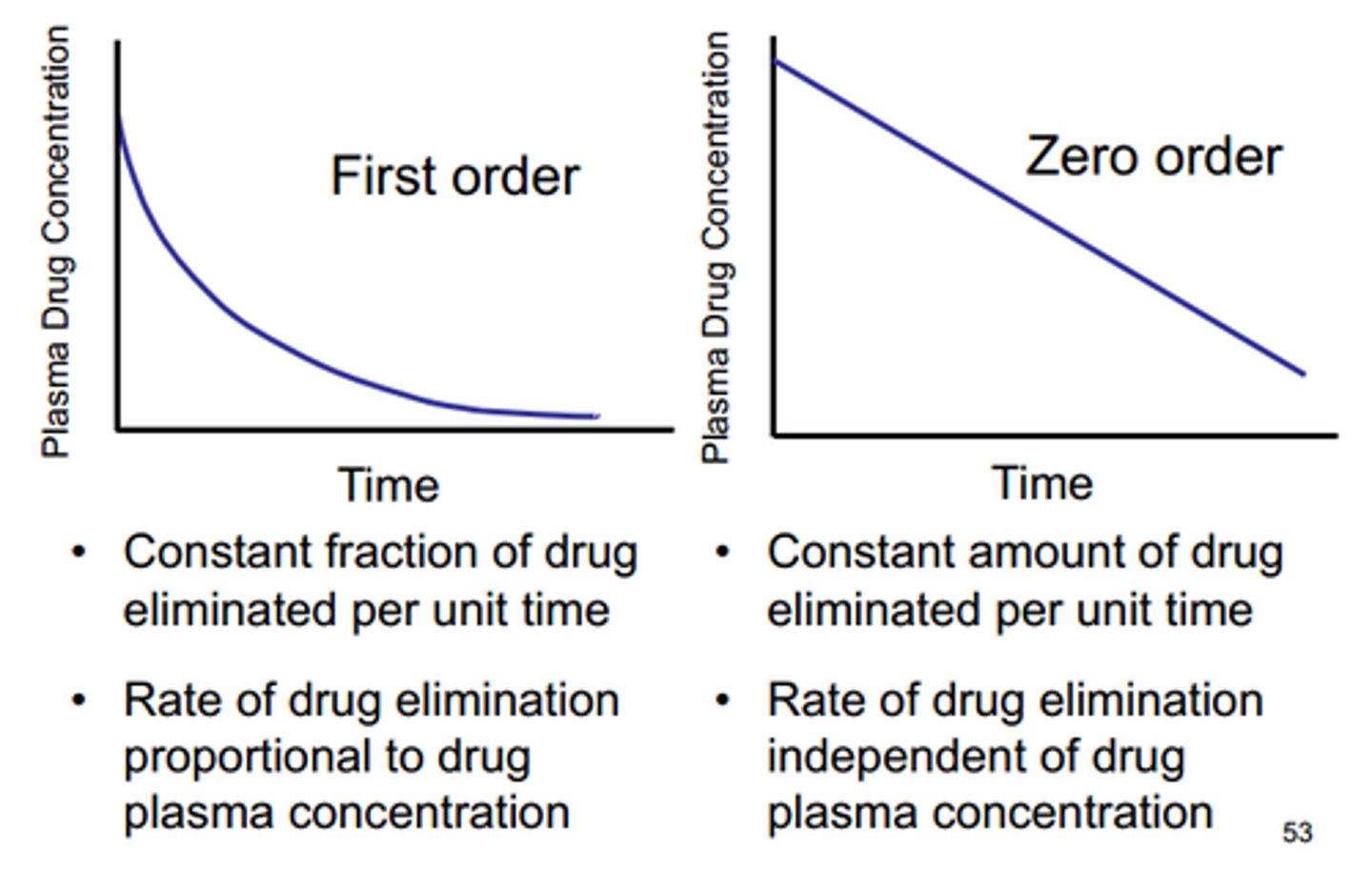
zero vs first order kinetics
zero order - constant amount of drug is removed per unit of time [if you have 50 or 100 drugs, it's still removing only 10 per hour]
first order - MAJORITY. constant % of drug is removed per unit of time. [ if 20% is removed every hour, then having more drug means more gets cleared per hour]
![<p>zero order - constant amount of drug is removed per unit of time [if you have 50 or 100 drugs, it's still removing only 10 per hour]</p><p>first order - MAJORITY. constant % of drug is removed per unit of time. [ if 20% is removed every hour, then having more drug means more gets cleared per hour]</p>](https://knowt-user-attachments.s3.amazonaws.com/0caacdd4-b3b6-4549-96ea-d2a6902512c4.jpg)
most kinetic processes in the body follow _____ order kinetics
first
first order kinetics equation
before integration and after? linear form?
rate of process = dc/dt= -K[C]
(change in concentration)/ (change in time)= -(rate constant)(concentration of drug at that time)
C= C0 e^(-Kt)
linear:
log C= log C0 - Kt/2.303
![<p>rate of process = dc/dt= -K[C]</p><p>(change in concentration)/ (change in time)= -(rate constant)(concentration of drug at that time)</p><p>C= C0 e^(-Kt)</p><p>linear:</p><p>log C= log C0 - Kt/2.303</p>](https://knowt-user-attachments.s3.amazonaws.com/63c16305-6893-4cca-af98-3917dee8caeb.jpg)
linear first order kinetics equation. what is the slope? y-int?
log C= log C0 - Kt/2.303
slope: -K/ 2.303
intercept: C0 aka initial concentration
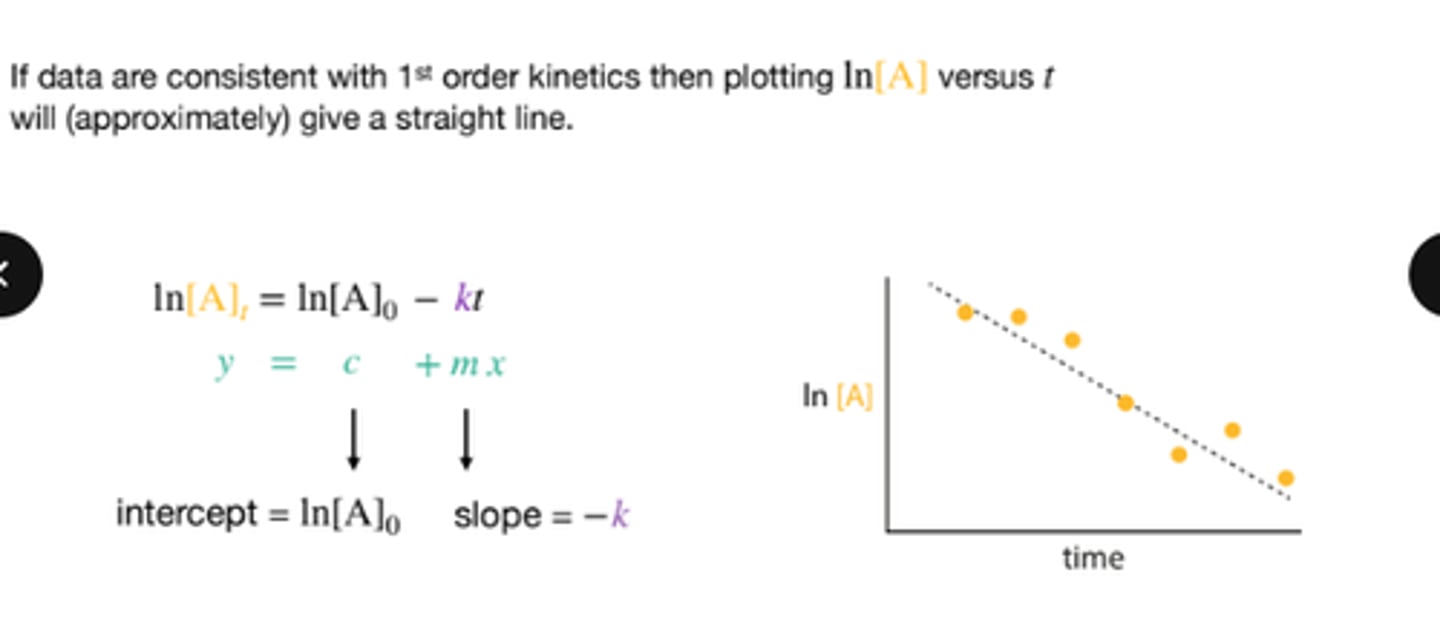
in a linear first order kinetics graph, what does the y intercept represent
initial concentration of drug at time zero
how does the elimination rate change in first-order vs. zero-order kinetics as drug concentration increases?
first: higher elimination rate bc depends on initial concentration
zero: constant elimination rate bc does not depend on initial concentration
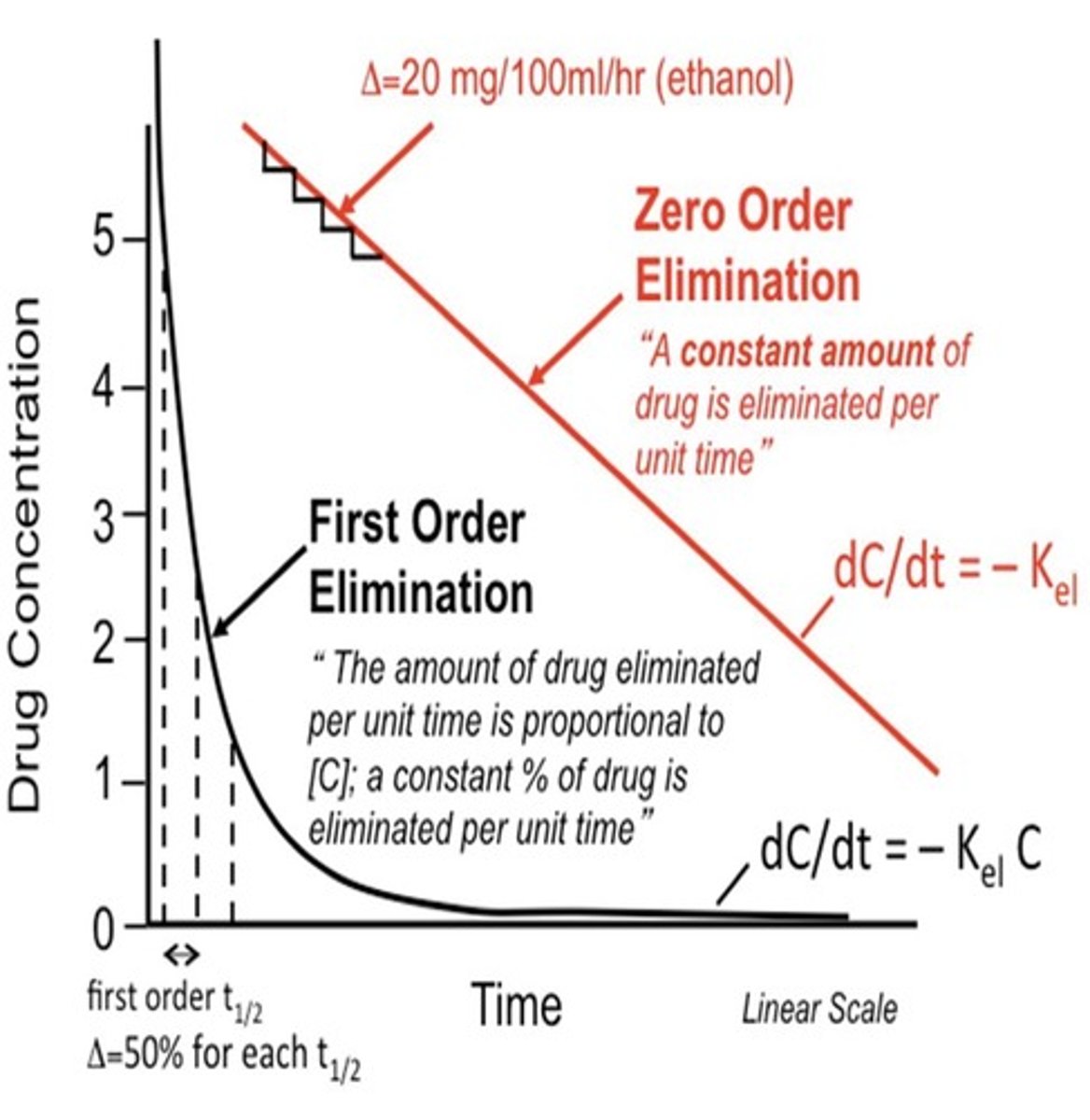
how does half-life change in first-order vs. zero-order kinetics?
first: half-life is constant (bc a constant fraction is eliminated per unit time)
zero: half-life is not constant and increases as drug concentration increases bc elimination pathways are saturated
t/f: a semi log plot makes a zero order kinetics equation appear as a straight line
false. first order
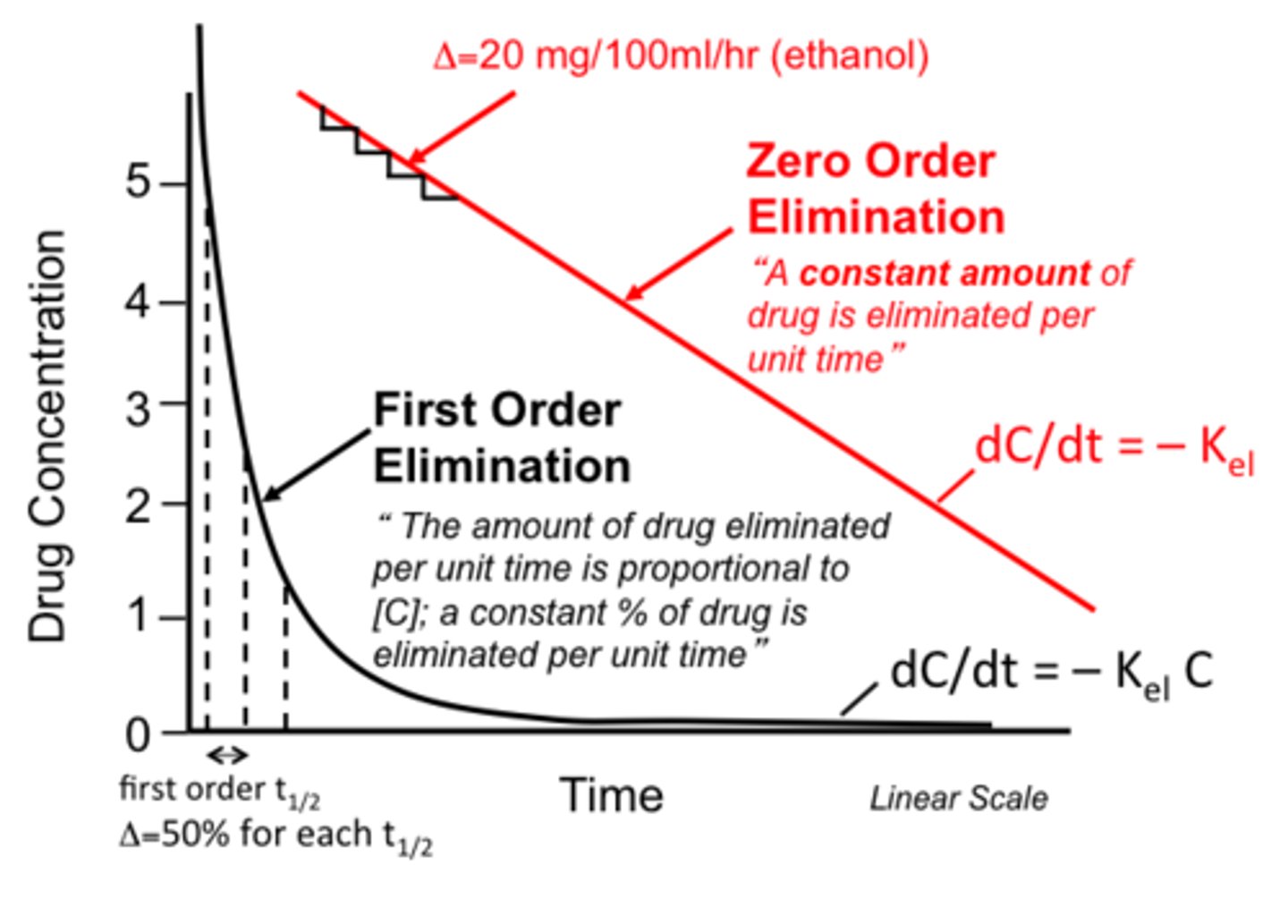
what does the concentration vs. time graph look like for first-order vs. zero-order elimination?
first: exponential decline (curved downward) but can be linearized via logs
zero: straight-line decline (constant slope)
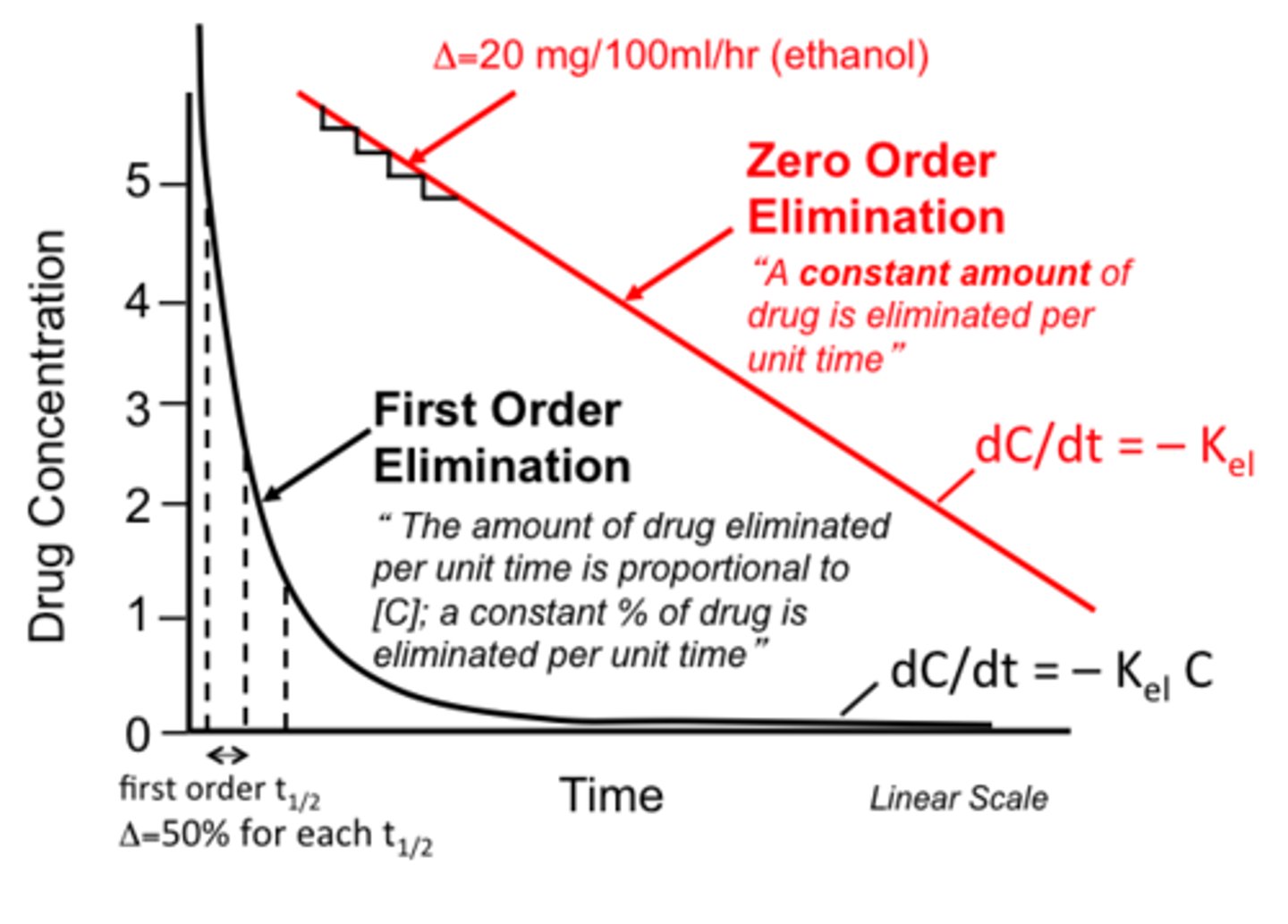
which type of kinetics (first or zero order) is more likely to result in drug toxicity? why?
zero bc elimination rate is fixed (does not depend on concentration so excess drug keeps accumulating)
what does the slope of a semi log plot of concentration vs time represent
rate of elimination (negative slope)