Lecture 24: Mechanisms of Bone Healing
1/52
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
53 Terms
What are the cells making up bone composition and what is their function?
osteoprogenitor cells
osteoblasts: produce bone
osteoclasts: remove bone
osteocytes: resident support
bone lining: control & differentiation
What percent of bone ECM is organic & water and what percent is inorganic?
organic and water: 35%
inorganic 65%
What makes up the organic & water portion of bone ECM?
type I collagen: 90%
osteocalcin, osteonectin, proteoglycans, glycosaminoglycans, lipids
What makes up the inorganic portion of bone ECM?
mostly hydroxyapatite
What is direct (primary) fracture healing?
osteonal reconstruction:
requires rigid internal fixation (less than 2% strain)
minimal or no fracture gap
What is indirect (secondary) fracture healing?
intermediate callus formation:
direct bone formation (intramembranous)
endochondral ossification
What is strain in fracture healing?
fracture gap length - change in length/original length (described as percentage)
What percent of strain in fracture healing is caused by granulation tissue, cartilage, and bone (osteoblasts)?
granulation tissue: 100%
cartilage: 10%
bone: 2%
What are the two types of direct healing?
contact healing: gaps less than 300 microns
gap healing: gaps less than 1 mm
In contact healing, osteons (cutting cones) cross fracture planes - one fragment to the other. How is gap healing different?
• Blood vessels and connective tissue form
• Osteoblasts deposit perpendicular lamellar bone in gap
• Cutting cones traverse fracture plane
• Lamellar bone becomes longitudinally oriented
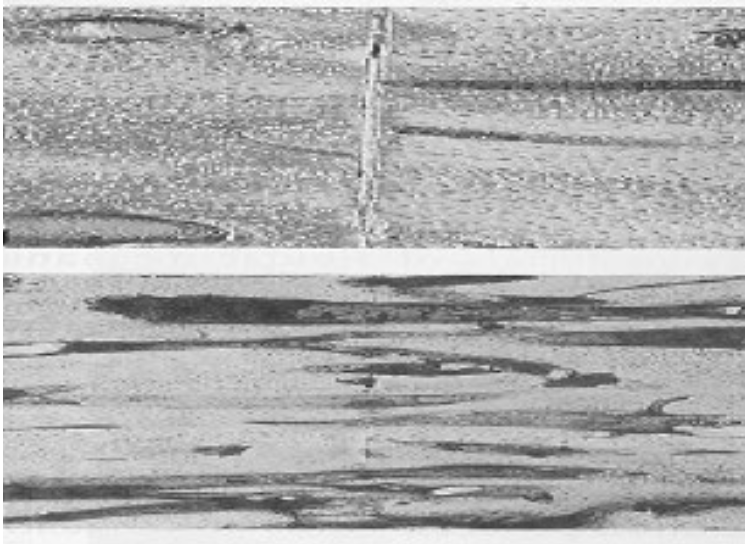
What type of direct healing is this?
contact
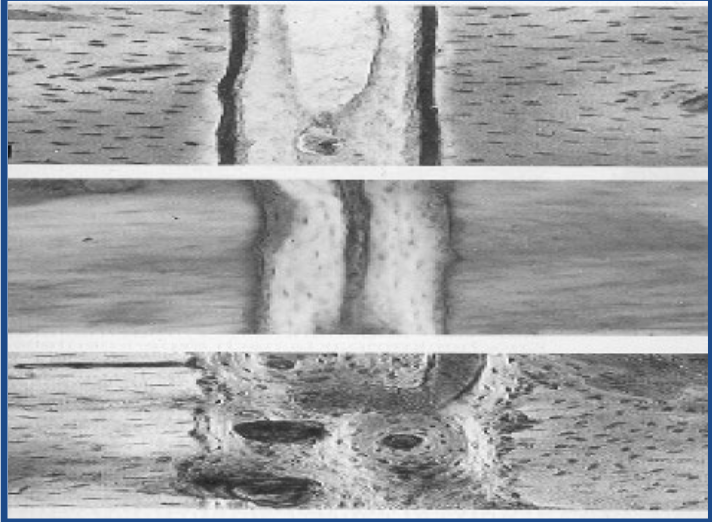
What type of direct healing is this?
gap healing
What are the three requirements for direct (primary) healing?
rigid fixation (decrease inter-fragmentary strain)
adequate reduction (only possible with simple fractures)
sufficient blood supply
What type of fracture healing is the most common and is enhanced by motion?
indirect (secondary) healing
What is required for indirect fracture healing?
callus formation
What inhibits indirect healing?
rigid stabilization
What are the 4 general phases of fracture healing?
1. Hematoma formation (inflammation) phase
2. Soft callus formation (proliferative) phase
3. Hard callus formation (maturing or modeling) phase
4. Remodeling phase
What are the four specific stages of fracture healing?
1. Hematoma formation/inflammation: Release of inflammatory cells and mediators, Bone Morphogenetic protein (BMP) (Other *TGF-β proteins)
2. Intramembranous bone formation
3. Chondrogenesis
4. Endochondral ossification: Very similar to metaphyseal growth plate, *Transforming Growth Factor β
What type of fracture healing is faster?
indirect bone healing
What type of fracture healing uses bone plates and what type uses less rigid fixation like pins/wires?
bone plate = direct
pins/wires = indirect
What is fracture nonunion?
all evidence of osteogenic activity at fracture site has ceased → fracture union NOT possible w/o surgical intervention
What are the two Weber-Cech fracture classifications?
viable (vascular)
nonviable (avascular)
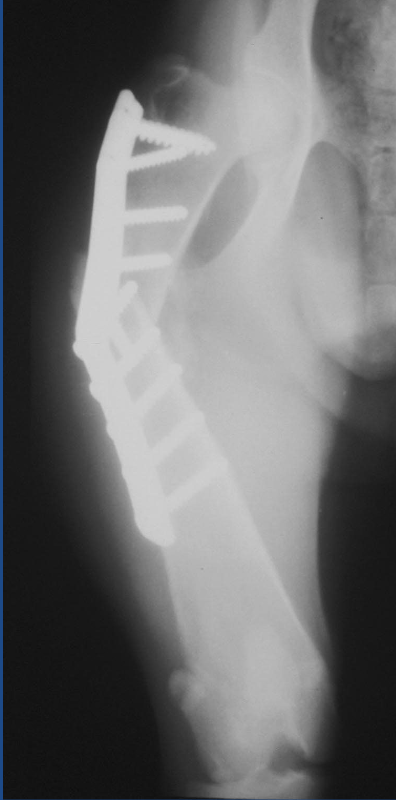
What is a viable- hypertrophic nonunion fracture?
abundant callus but NOT bridging the fracture site (“elephant foot”)
What causes viable- hypertrophic nonunion fractures?
inadequate stabilization
premature weight-bearing
too much activity of patient
What type of fracture is this?
hypertrophic nonunion
What is a viable- mildly hypertrophic nonunion fracture?
mild callus but NOT bridging the fracture site (“horses foot”)
What causes a viable- mildly hypertrophic nonunion fracture?
inadequate stabilization usually due to implant failure
ex. plate breaks, screw pulls out
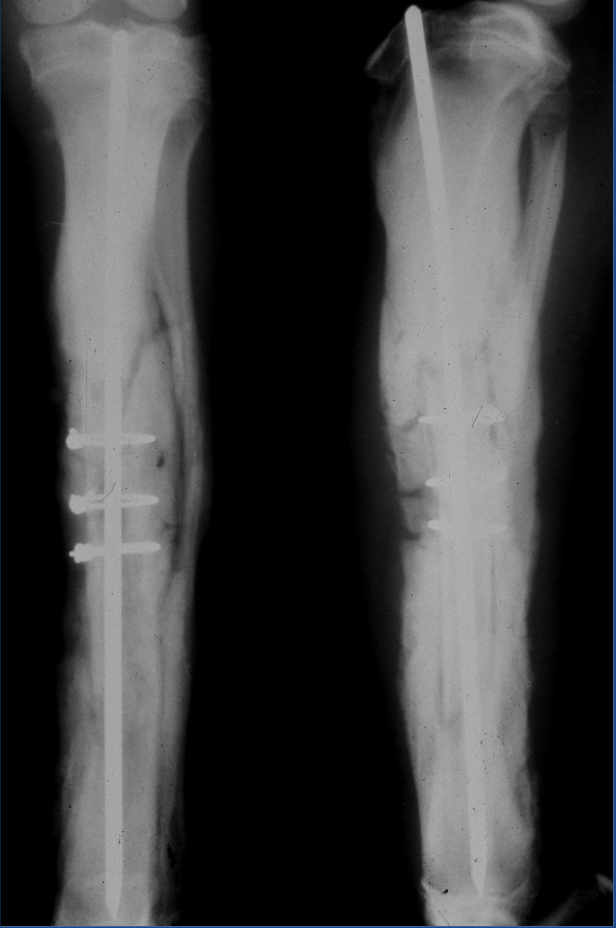
What is a viable- oligotrophic fracture?
no callus - just fibrous tissue and blood vessels joining ends
see rounding of fracture edges, resorption of bone and shortening of fragments
What causes a viable- oligotrophic fracture?
displacement of fracture fragments or inadequately apposed fragments

What type of nonunion case is this?
oligotrophic
What type of nonunion case is this?
mildly hypertrophic
What is a nonviable- dystrophic nonunion fracture?
intermediate fragments of fracture heal to one main fragment and not the other
What causes a nonviable- dystrophic nonunion fracture?
• Poor blood supply on non-healing side
• Instability on avascular side
• More common in older animals w/ poorer blood supply
What is a nonviable- necrotic nonunion fracture?
fragments have no blood supply and cannot heal to any of main fragments
the classical ‘sequestrum’
avascularity of fragment can lead to implant loosening
What causes a nonviable- necrotic nonunion fracture?
poor blood supply
infection at the fracture site - but does not have to be an infection
What is a nonviable- defect nonunion fracture?
large defect - even if ends have blood supply, they cannot bridge bone
What causes a nonviable- defect nonunion fracture?
massive loss of bone at fracture site
What is a nonviable- atrophic nonunion fracture?
end result of other 3 nonviable nonunions - uncommon, most difficult cases to treat
What are the causes of nonunion fractures?
• Infection
• Ischemia
• Distraction of bone ends
• Excessive compression of bone ends
• Interposition of soft tissue at fracture
• Improper implant fixation
• Systemic factors
What are the clinical signs of nonunion fractures?
• Pain at the fracture site
• Lameness: usually non-wt-bearing (NWB)
• Disuse atrophy of limb
• Movement felt at fracture site
What are the radiographic signs of nonunion fractures?
• Fracture gap
• No activity at fracture ends
• Obliteration of marrow cavity
• Osteopenia of surrounding bone
• If callus even present: Does not bridge fracture gap!
How are nonunion fractures treated?
rigid stabilization of fracture
enhancing blood supply (bone grafting)
treat underlying cause of nonunion: infection, fracture gaps, possible metabolic disorders
What are the causes of malunions?
• Untreated fracture
• Improperly treated fracture
• Premature excessive wt-bearing on fracture
What are the clinical results of malunion?
• Angular limb deformities
• Limb shortening
• Gait abnormalities
• Degenerative joint disease
What supplies 80-85% of a bone’s blood supply?
nutrient artery
__________ blood supply supplies early periosteal callus after injury.
extraosseous
What are the three general types of graft transplanting
• Autogenous- within same individual
• Allograft- different individuals, same species
• Xenograft- different individuals, different species
What are the O’s of grafting?
• Osteogenesis- osteoblasts that survive transfer (Very few survive)
• Osteoconduction- graft acts as scaffold in which new bone is laid down
• Osteoinduction- graft induces cells to promote new bone (BMP)
• Osteopromotion- material that enhances regeneration of bone (Platelet-Rich Plasma)
Where does a cancellous bone graft come from?
trabecular bone
Describe the physiology of cancellous bone grafts.
• Bone graft separated from its blood supply
• Few cells survive- osteogenic cells
• Mesenchymal stem cells are induced to form bone cell lines (Inductive Proteins (BMPs))
• Deposition new bone from osteoprogenitor cells
• Resorption of necrotic bone
What are the indications for bone grafts?
• Any orthopedic fracture or arthrodesis
• Infected fractures
• Delayed / nonunions
• Bone loss- cysts, fractures
• Limb- sparing for bone tumors
What are the most common bone graft donor sites?
ilial wing
proximal tibia & humerus
distal femur
What steps are important when harvesting a cancellous bone graft?
asepsis
prepare surgical donor site in advance
separate sx instruments
minimize grafts air exposure
keep in blood-soaked sponges
debride graft are and do not create fracture