Quiz 2- Principles of Endodontic Access + Working Length and Apical Stop
1/79
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
80 Terms
What are the 4 goals of access?
Locate all canals
Straight-line access to canals
Removal of chamber roof and coronal pulp tissue
Conservation of tooth structure
What is “straight line” access?
Unimpeded access of the instruments in the canals to the apical one third of the canal or the first curve

What effect does opening the orifice in a straight line access have on the file?
Less stress on file
What dictates the shape of access?
Pulp chamber anatomy
Your access should be as small as possible, but
As large as necessary
What are the consequences of having an access that is too small?
Difficulty locating canals
Missed canals
Difficulty achieving straight-line access
What are the consequences of having an access that is too big?
Unnecessary removal of tooth structure
Why is it necessary to remove pulp material from the pulp horns/ crowns?
To prevent coronal discoloration
What is outline form?
The recommended shape of the access: it should be a projection of internal tooth anatomy onto external root structure
What may change over time with calcification of the chamber?
Outline form
What is convenience form?
Modification of ideal outline form to facilitate instrument placement and manipulation
Why it is pertinent to remove caries prior to access?
Prevent contamination of root canal system
Access restorability
Provide sound tooth structure for temporization / restoration
The toilet of the cavity should be kept clean. How can you prevent debris from blocking the canal?
By frequently irrigating
The first step to opening the access is to study the
Pre-operative radiographs and determine the depth of access from it
When opening the access, you may/may not remove restorations, but it is important to
Remove all caries
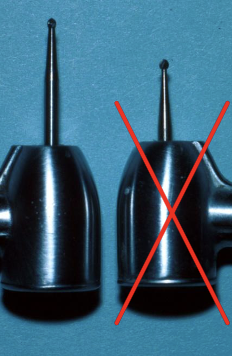
What bur is used for access opening?
701 in high-speed handpiece (may use slow speed when closer to chamber)
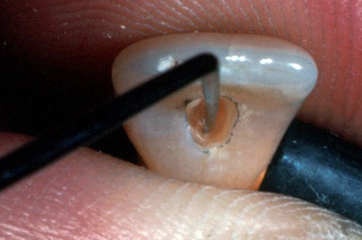
What should you use to detect the chamber / canal oriface?
DG- 16 endo explorer
Tactile sensation can help during access because you can
Re-evaluate as needed
In calcified cases, for access opening, it may be helpful to
Expose radiograph if needed

Which tooth has 1 canal?
Maxillary anterior teeth
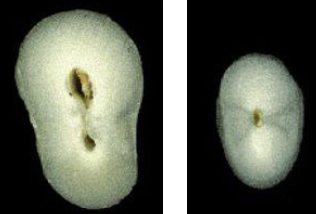
Which tooth has a 30% chance of having 2 canals?
Mandibular canine
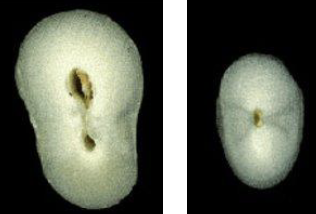
30% of mandibular canines may have 2 canals, of the 30%, what percent have 2 canals that join?
20%
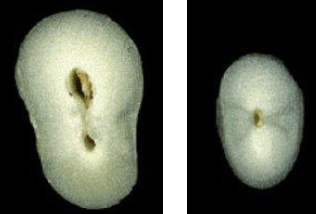
30% of mandibular canines may have 2 canals, of the 30%, what percent have 2 canals that separate?
10%

What is the root shape of central incisors?
Usually straight

What is the root shape of lateral incisors?
Usually apical curvature to distal or palatal
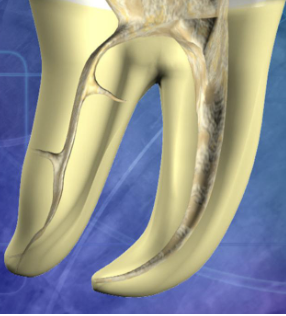
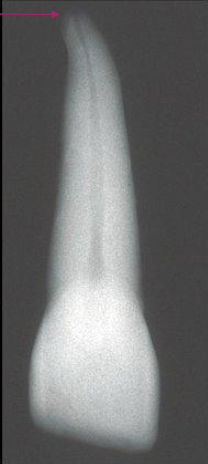
What is the root shape of canines?
Long root, usually apical curvature
Why might it be difficult to radiographically interpret canine apices?
Due to a small root tip
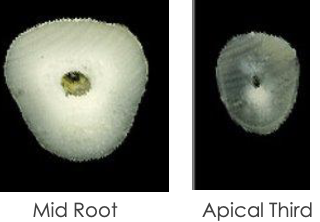
What is the canal shape of a maxillary central incisor?
Usually round
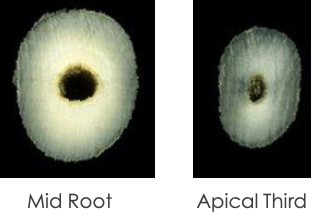
What is the canal shape of a maxillary lateral incisor?
Usually oval / round

What is the anatomical variation in this lateral incisor?
Lingual developmental or palato-radicular groove


What is the anatomical variation in this lateral incisor?
Dens invaginatus

What is the anatomical variation in this lateral incisor?
Talon cusp
When creating your access in maxillary central incisors, what should you observe in your radiograph?
Anatomy, shape, and location of canal
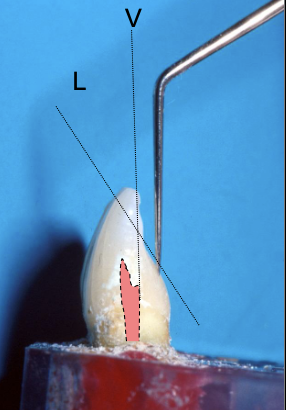
The access outline is determined by the “incisal limit.” What does this mean?
The use of the incisal edge as the coronal reference point for measuring working length and initiating access cavities, particularly for mandibular incisors

Your access outline should be triangular in shape and 3mm×2mm in size. Why do you need to make an outline?
To have a strategically designed cavity prep designed to provide straight-line access to root canals


Which burs are slow speed latch? What do they do?
GG #4, #3, #2: help with smoothing the opening

This bur is used to cut the cavo-surface outline
#701

This bur is used to extend the access prep into the pulp chamber down the long axis of the tooth
Sx #2

After extending the access prep into the pulp chamber. Use this instrument to explore the pulp chamber and check for pulp horns
G2 explorer

If you need to remove a lingual shoulder, you can use this instrument to smooth out the access opening
GG 2,3,4 and Hedstrom File
Biomechanical instrumentation refers to
Instrumentation and access + canal enlargement
Chemomechanical instrumentation refers to
Disinfection of canal and access
What you take out of the tooth is more important than
What you put in
What are the goals of biomechanical and chemomechanical preparation?
Reduce # of viable bacteria
Remove all tissues and debris
Avoid irritation of PA tissues
Keep instruments and irrigants inside tooth
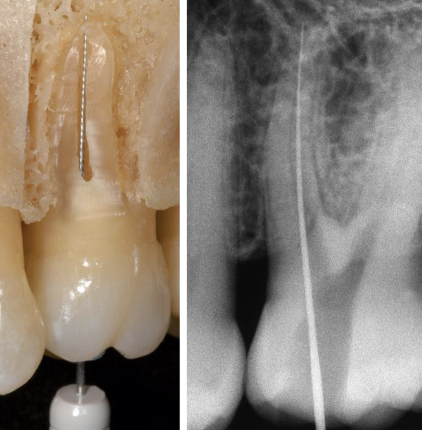
Correct working length is critical to meet the goals of biomechanical and chemomechanic preparation. What is working length?
From the coronal to the apical extent of the root canal system
This material is used to disinfect the canal system (kill microbes)
Sodium hypochlorite (NaOCl) - bleach
This material is used to remove the smear layer of dential debris that accumulate on the canal walls
17% EDTA (ethylenediaminetetraacetic acid)
For the purposes of our lab course, what will you be using instead of bleach?
Water in 10mL with side vented needles
What is a precaution to take with bleach when using it in clinic?
It stains
Apical patency is technique where
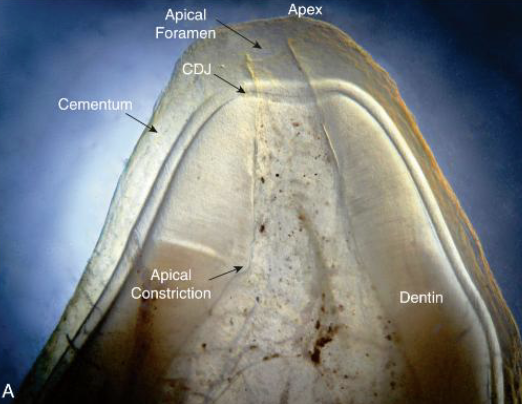
The apical portion of the canal is maintained free of debris by recapitulation (using smaller endo files to remove debris) with a small file through the apical foramen
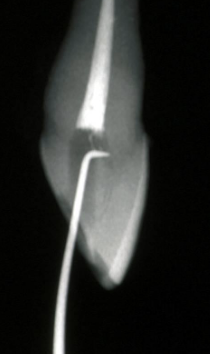
Working length is the distance from
A coronal reference point to the point at which canal preparation and obturation should terminate
This is the largest file used to the full working length of the completely preparaed root canal
Master apical file (MAF)
When should the the apex terminate?
0.5-1mm from radiographic apex
For the working length, if there is difficulty viewing the file, you can use
A 15K file or larger
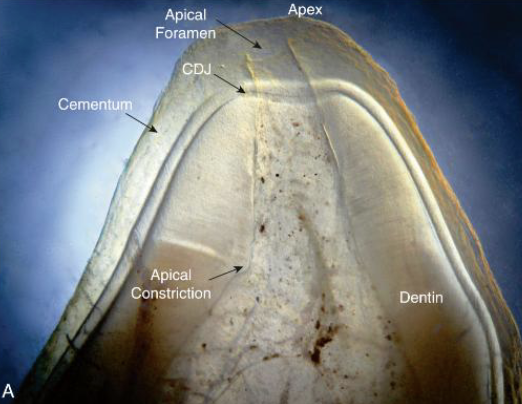
_______ thickens with age. This is why apical constriction occurs within this area
Dentin; dentinal area
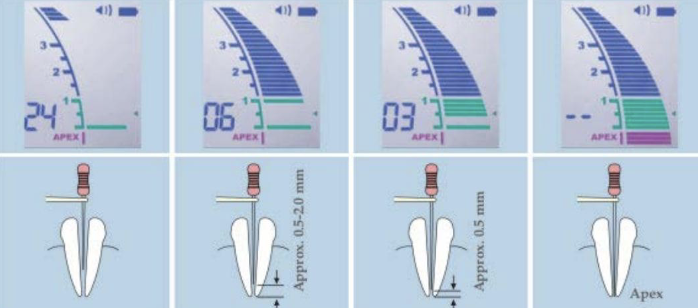
To determine working length, this helps clinically along with radiographic WL
Combination of apex locator measurements + radiographic WL
As you reach apical constriction, use your tactile sensation for working length determination
“Feel” an increase in resistance
What is an advantage of using tactile sensation for working length determination?
Saves time
No radiation exposure
What is a disadvantage of using tactile sensation for working length determination?
Not always accurate- this is very important!
How can you use a paper point to determine working length?
Moisture or blood present on apical part of paper point tells you where the canal ends
What is an advantage of using paper points for working length determination?
Useful in teeth with open apices or as an adjunct to other methods
What is a disadvantage of using paper points for working length determination?
Not always accurate
Working length is important. These can affect treatment outcome
Apical termination of instrumentation and obturation
Obturation within 0-2mm of apical termination has a ____ % success rate
94%!
Obturation within >2 mm of apical termination has a ____ % success rate
68%

Obturation past the apex has a ____ % success rate
76%
For every 1mm loss in working length, there is ______ % decrease in success
14%
Root canals are ____ % more successful when you fill up to (but not past!) the apex
29%
Your apical stop size is
The size of the smallest K-file that cannot be pushed (without force) beyond working length
This is the apical stop size BEFORE instrumentation
Initial apical stop size
This is the apical stop size AFTER instrumentation
Final apical stop size
What are some reasons why the initial and final apical stop size might differ?
Overinstrumentation
Debris packed apically
Inaccurate assessment
The initial and final apical stop size must be physically checked using tactile sensation. What happens if you fail to check?
Common cause of overfilling
First to bind is
The smallest file that feels resistance when twisting at working length
Often the first to bind is the same size as
The initial apical stop size
The first file to bind will determine the “ideal” final apical size used to
Enlarge the apex of canal to adequately debride the canal walls
The final apical size will be 3 sizes larger than the first file to bind when handfiling.
If your first file to bind is #20K file, 3 sizes larger would be size #35 (#25, #30, #35)
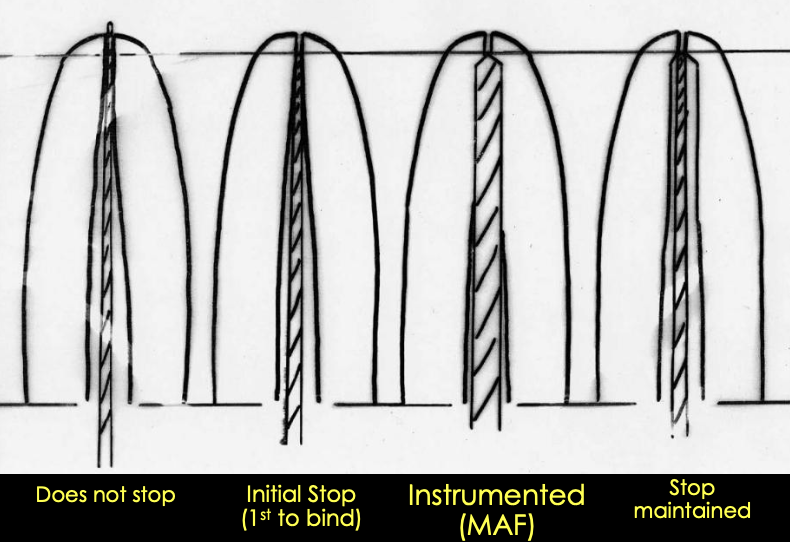
What are the steps for maintaining the apical stop?
Initial stop (1st to bind)
Instrumented MAF
Stop maintained
What is a consideration if you have a calcified canal?
You may need to start with a smaller K file (size 15)
How can you create a repeatable reference?
Make sure the reference point is touching the stopper (incisal edge or cusp)