16. Non Bio treatments for AN
1/19
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
20 Terms
What are the principles of the cognitive approach?
The cognitive approach suggests that behaviour is a result of information processing and mental processes.
All the information we receive from the environment is processed by the brain and this processing leads us to our beliefs, feelings and behaviours.
How does the cognitive approach explain mental health conditions like AN?
According to the cognitive approach mental health disorders are as a result of faulty cognitive processes.
This means the way we process information and beliefs we then hold as a result are faulty, disordered or dysfunctional.
What is CBT-E and how is it different to traditional CBT?
Enhanced cognitive behavioural therapy (CBT-E) is used as a main form of therapy for patients with AN.
The main aim is to rectify the thoughts and behaviours associated with disordered eating and body dysmorphia.
Diagram of CBT-E
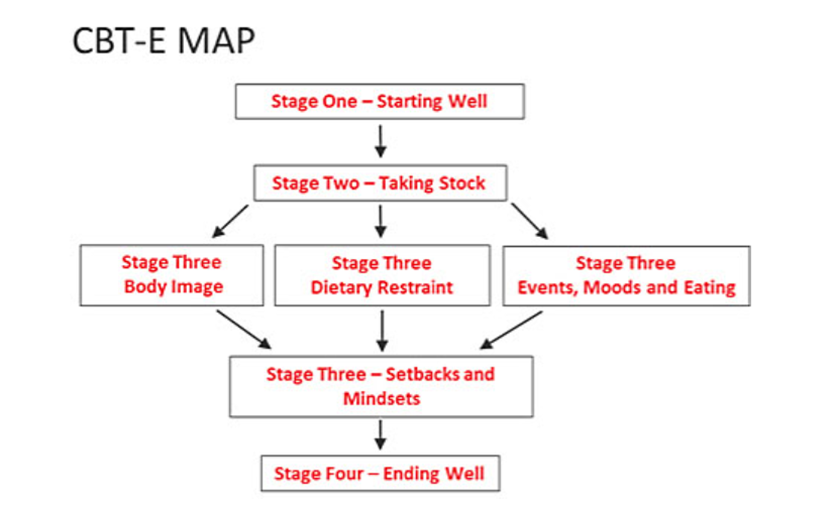
What is stage 1 - Starting well?
This stage of treatment takes about 4 weeks with 2 sessions held per week to encourage rapid change in the client’s behaviour.
2 important procedures are implemented in this phase - ‘weekly weighing’ with the therapist, and ‘regular eating’.
Clients are educated about the disorder and they will also learn about the treatment programme so that they know what to expect.
It is important during this 1st stage that the patient is positive about the treatment and motivated to progress because the therapy will only be effective if they are willing to make the necessary changes.
Establishes positive relationships between patient and therapist.
One of the key focuses is that making sure that the diet improves overall health.
What is stage 2 - Taking stock?
This stage is quite brief consisting usually of two appointments, 1 week apart.
The therapist and client will meet to discuss the progress being made in stage 1 and ‘taking stock’ of how the patient is currently.
Good progress can be praised to boost motivation , while poor progress can be discussed to uncover possible reasons for why things aren’t going well.
What is stage 3?
Body image
Dietary restraint
Events, moods and eating
Setbacks and mindsets
This is the main stage of the treatment where clients will usually have 8 appointments once a week to tackle the factors that are involved in the maintenance of the eating disorder.
This will involve dealing with the clients body image, their dietary rules, and any event-related changes in eating.
Dealing with body image will usually look at certain behaviours likely to lead to body dissatisfaction such as constant body checking, as well as the triggers that make them ‘feel fat’.
Dietary rules are explored to consider the impact that rigid restrictive rules are having on the client’s quality of life, and any foods that they currently avoid are gradually introduced to the diet.
It is also important that external events that impact on major changes in eating are considered and tackled at this stage in treatment.
Everything to do with their mindset and behaviour are tackled at stage 3.
What is stage 4 - Ending well?
Clients are encouraged to look to the future and consider factors that need to be managed to prevent relapse.
Usually clients will have 3 appointments about 2 weeks apart at this stage.
The therapist and patient will draw up an agreed plan that is personalised for their specific circumstances.
Clients are also encouraged to consider their own mindset so that they do not see any relapse as ‘failure’, and instead think of it as a 'lapse’ that they can address.
A post-treatment review appointment will then be made about 5 months later where the client will be able to discuss any setbacks or issues.
How does Pike et al (2003) support the effectiveness of CBT-E for AN?
Pike (2003) compared the effectiveness of CBT and nutritional counselling as outpatient treatments given to patients with AN following hospitalisation.
In the 33 patients followed by the researchers, the relapse rates of those receiving CBT was considerably lower - 22% than those receiving nutritional counselling - 73%.
How does Byrne et al (2011) support the effectiveness of CBT-E for AN?
Byrne (2011) considered the effectiveness of CBT-E in treating patients with the full range of eating disorders in an outpatient clinic in Australia.
They found that two thirds of patients in the treatment group showed significant improvement in symptoms both in relation to eating behaviour and also other general psychopathology.
What is a strength of CBT-E in terms of being evidence based and transdiagnostic?
CBT-E is grounded in research and targets the underlying cognitive and behavioural processes common to all eating disorders, making it broadly applicable.
What is a limitation of CBT-E in terms of engagement challenges?
Patients with AN often resist weight restoration, which can lead to poor adherence or early dropout.
What is a strength of CBT-E in terms of structured and individualised?
It follows a clear framework but can be tailored to each patient’s needs, whether adolescent or adult, and adapted for outpatient or inpatient care.
What is a limitation of CBT-E in terms of limited evidence for adults?
While effective for adolescents, research shows mixed results for adults, with no clear superiority over other treatments.
What is a strength of CBT-E in terms of positive clinical outcomes?
Studies show significant improvements in weight restoration and reduction of eating disorder symptoms, often with medium to large effect sizes.
What is a weakness of CBT-E in terms of being resource intensive?
Requires highly trained therapists and strict adherence to the protocol, which can limit availability in routine practice.
What is a strength of CBT-E in terms of focus on relapse prevention?
CBT-E doesn’t just aim for weight gain, it addresses thought patterns and behaviours that maintain the disorder, reducing the risk of relapse.
What is a limitation of CBT-E in terms of relapse risk still remains?
Even after successful treatment, relapse rates are high (9-52%) meaning ongoing support is often necessary.
What is a strength of CBT-E in terms of flexible delivery?
Can be delivered face to face, in intensive programs, or remotely making it accessible in different clinical contexts.
What is a weakness of CBT-E in terms of not universally effective?
Severe cases or those with minimal early weight gain may respond poorly, highlighting the need for alternative or combined approaches.