drug induced cardio disorders
1/61
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
62 Terms
main drug induced cardio disorders
htn, arrhythmias, acute coronary syndrome, left ventricular systolic dysfunction + heart failure
mechanism of drug induced htn
drug works on multiple things: SNS activation, RAAS activation, Na retention, increased cardiac output, increased peripheral vascular resistance
risk factors for drug induced htn
hx of htn, decreased egfr (esp <60), metabolic syndrome, older age
which drug classes can cause drug induced htn
VEGF + tyrosine kinase inhibitors, calcineurin inhibitors, NSAIDs, corticosteroids, erythropoiesis-stimulating agents, OCPs, serotonin norepi receptor antagonists, stimulants, drugs of abuse
examples of VEGF + tyrosine kinase inhibtors
bevacizumab, sunitinib, sorafenib, ponatinib
what are VEGF + tyrosine kinase inhibitors used for
chemotherapy for renal, cell, thyroid, and other advanced solid tumors
tx for VEGF + tryrosine kinase inhibitor induced htn
ccbs, acei, k-sparing diuretics
calcineurin inhibitors
potent immunosuppressive drugs used to prevent post transplant rejection
adr is htn!
calcineurin inhibitor examples
cyclosporine, tacrolimus
tx for calcineurin inhibitor induced htn
thiazies (HCTZ)! → selectively block sodium chloride cotransporter (NCC) which may reduce htn
how to NSAIDs induce htn
prostaglandins regulate vascular tone → COX-2 inhibition decreases prostaglandin production → increases na+ + h2o retention → increased BP!
constricts the afferent arteriole → potential kidney damage!
black box warning of NSAIDs
increased risk of serious cardio thrombotic events, MIs, stroke
cox-2 inhibitors have lower gi risk but higher cardio risk!
how to corticosteroids cause htn
increases bp from na+ and h2o retention through mineralocorticoid receptor activity
in which pts is steroid induced htn common
cushing’s syndrome! and other pts taking for other reasons
corticosteroid with no mineralocorticoid
dexamethasone
what are erythropoiesis-stimulating agents used to treat
anemia, CKD, and pts receiving chemo
tx for erythropoiesis-stimulating agent induced htn
dose reduction or changing route from IV to IM
what is responsible for oral contraceptive induced htn
exogenous estrogen and progesterone!
OCP black box warning
endometrial cancer, breast cancer, may increase risk of blood clots, strokes, and heart attacks
what are serotonin norepi receptor antagonists used for
used for tx of GAD, MDD, OCD, PTSD, migraines, panic disorders
examples of serotonin norepi receptor antagonists
desvenlafaxine, venlafaxine, duloxetine
venlafaxine → increase bp by 9% w/ doses >300mg/d (monitor closely)
drugs of abuse that can cause htn
MDMA, PCP, methamphetamines, cocaine → all cause cns sympathetic excess/activation
chronic use → arterial stiffness + athersclerosis → htn
types of arrhythmias caused by drugs
bradyarrhythmia, supraventricular arrhythmia (afib, atrial flutter), qt prolongation, torsade de pointe
mechanisms of arrhythmias
structural abnormalities or electrical changes → affect action potential → cardiac arrhythmias
drug induced bradyarrhythmia
hr <60 bpm, caused by a depressant effect on sinus node automaticity
noncardiac drugs: phenytoin, TCAs, lithium, digoxin, acetylcholine inhibitors
cardiac drugs, bb, ccbs, proarrhythmic drugs
how do acetylcholinesterase inhibitors cause bradyarrhythmia
high ach levels increase parasympathetic tone in SA node → bradyarrhythmia
what are acetylcholinesterase inhibitors used to treat
mild to moderate alzheimer’s
examples of acetylcholinesterase inhibitors
donepezil, neostigmine, physostingmine, pyridostigmine
examples of antiarrhythmics
amiodarone, flecainide, ivabradine, propafenone
→ adverse effects correlates to total amiodarone exposure
which pt population is at higher risk of bradyarrhythmias d/t anti arrhythmics
elderly and those w/ hx of afib or mi
drug induced afib
most common type of arrhythmias but can have serious consequences (eg. stroke)
basically when atria beats irregularly
noncardiac drugs: antidepressants, antipsychotics, anesthetics
cardiac drugs: sympathetic activating agents, antiarrhythmics, diuretics
common afib risk factors
hf, htn, chd, cancer
how do sympathetic activating agents cause afib
sympathomimetic agents activate adrenergic receptors directly by increases norepi and epinephrine (catecholamines)
SNS activation can increase ca2+ dependent cardiac activity → trigger arrhythmias
examples of sympathetic activating agents
dopamine, dobutamine
how do loop and thiazide diuretics caused arrhythmias
cause hypokalemia!! → associated w increased risk of arrhythmias
examples of loop diuretics that cause arrhythmias
furosemide, bumetanide, torsemide, ethacrynic acid
examples of thiazide diuretics that cause arrhythmias
HCTZ, chlorthalidone, indapamide
how do positive inotropes cause arrhythmias
they strengthen contractions of the heart → arrhythmias!
examples of positive inotropes that cause arrhythmias
milrinone, dobutamine, dopamine
torsades de pointe
life threatening arrhythmia!, esp when QTc >500 ms
risk factors for torsades de pointe
qt interval (QTc) >500 ms
female, age >65, bradycardia, acute mi, electrolyte abnormalities, HFrEF, concomitant admin of ≥ 2 QT prolonging drugs
drugs that cause TdP
antiarrhythmics: disopyramide, procainamide, quinidine, sotalol
macrolides: azithromycin, clarithromycin, erythromycin
fluoroquinolones: ciprofloxacin, levofloxacin, moxifloxacin
antifungals: fluconazole, ketoconazole, pentamidine, voriconazole
antipsychotics: haloperidol, ziprasidone
antidepressants: citalopram, escitalopram
antiemetics: droperidol, granisetron, ondansetron
opioids: methadone
others: cocaine, cilostazol, donepezil
clinical presentation of acute coronary syndrome
chest pain, dyspnea, sudden/heavy sweating, racing heartbeat, lightheadedness/dizziness, fainting, unusual fatigue
types of acs
non st elevation: unstable angina, NSTEMI
st elevation: STEMI
drugs associated w/ CV risk factors
corticosteroids: htn, dyslipidemia, dm
cyclosporine, tacrolimus: htn, dyslipidemia
NSAIDs/cox2 inhibitors: htn (minimal)
erythropoietin: htn
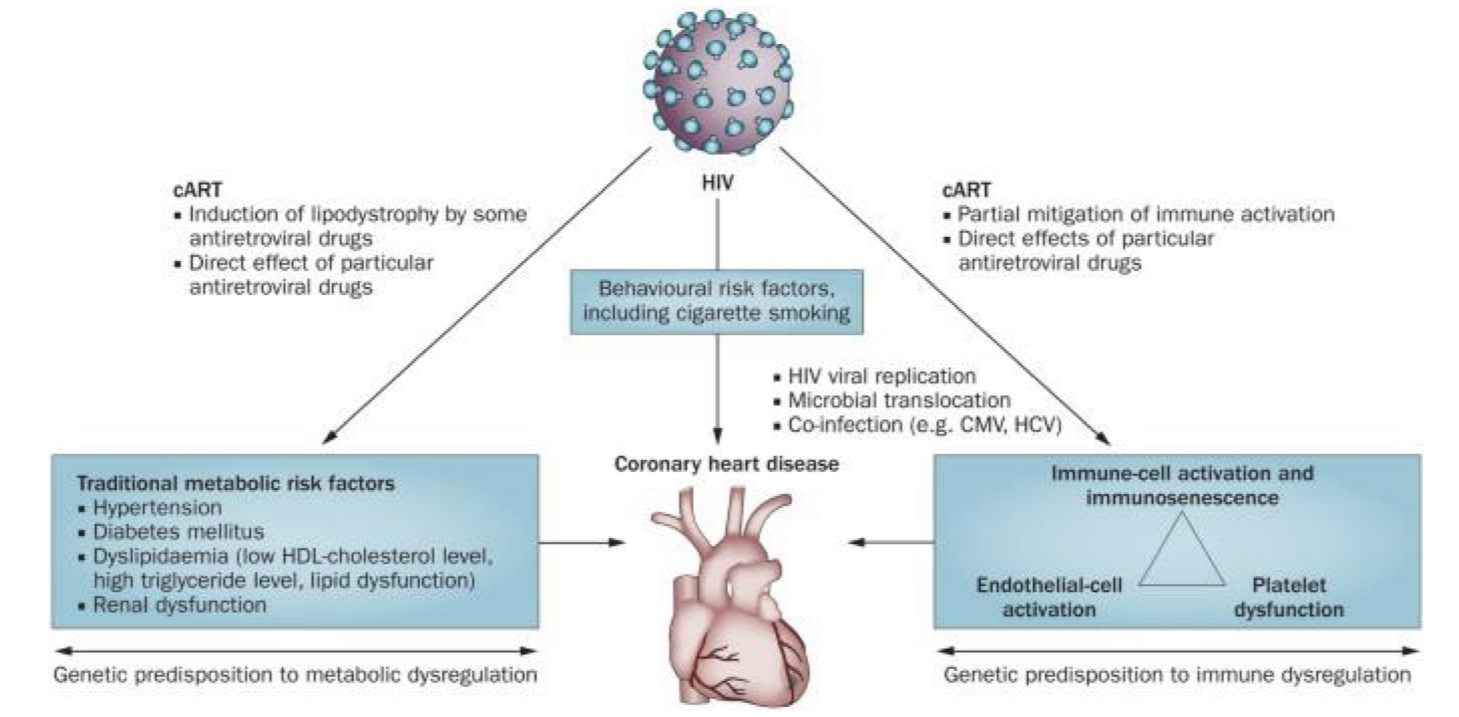
HAART: dyslipidemia
all can cause MACE (major adverse cardio events, eg. mi, fatal cad, stroke, death)
main drugs associated w/ MACE
NSAIDs, combined ocps, highly ctive antiretroviral therapy (HAART), erythropoietin
what is HAART used for
management + tx of HIV
how do erythropoiesis-stimulating agents cause acs
increase blood viscosity + platelet activation
Hb increase of >1g/dl over 2 wks may increase risk
make sure to use lowest dose possible for essential therapy
left ventricular systolic dysfxn (LVSD)
left ventricular complication that can lead to hf
heart failure
chronic condition when heart cannot pump adequate blood to organs
clinical presentation of LVSD and HF
sob, swelling of feet + legs, fatigue, difficulty sleeping at night
drug induced LVSD
cytotoxic agents (anthracyclines, trastuzumab)
antipsychotics (clozapine)
TCAs
anthracycline examples
daunorubicin, doxorubicin, idarubicin
how does anthracyclines cause LVSD
irreversible cardiotoxicity (decreased systolic fxn and global longitudinal strain, increased diastolic dysfxn) → cytoplasmic vacuolization, cardiac fibrosis, myofibril loss
what is the lifetime dose and what should you consider in anthracycline induced LVSD
450-500 mg/m²
consider cardioprotection w/ dexrazoxane
how does trastuzumab cause LVSD
humanized mab that targets HER-2 receptor for BCA → reversible cardiotoxicity
what is the lifetime dose and what should you consider in trastuzumab induced LVSD
no lifetime dose
drug cessation
clozapine induced LVSD
associated w/ cardiomyopathy + myocarditis
more common during rapid drug titration!
drugs that exacerbate HF
NSAIDs, cox-2 inhibitors, corticosteroids, thiazolidinediones, negative inotropes
thiazolidinedione induced HF
used for dm tx! (pioglitazone, rosiglitazone)
increases fluid reabsorption in the distal nephron and vascular permeability in adipose tissue
black box warning for thiazolidinediones
cause/exacerbate congestive HF
negative inotrope induced HF
weakens contractions + slows hr
bb: slow hr + should not be initiated during acute hf exacerbation
non dhp ccbs: more negative inotrope effects than dhp ccbs
generally avoid in pt w/ systolic hf even if it is for tx of angina/htn