Blood Pressure Disorders
1/127
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
128 Terms
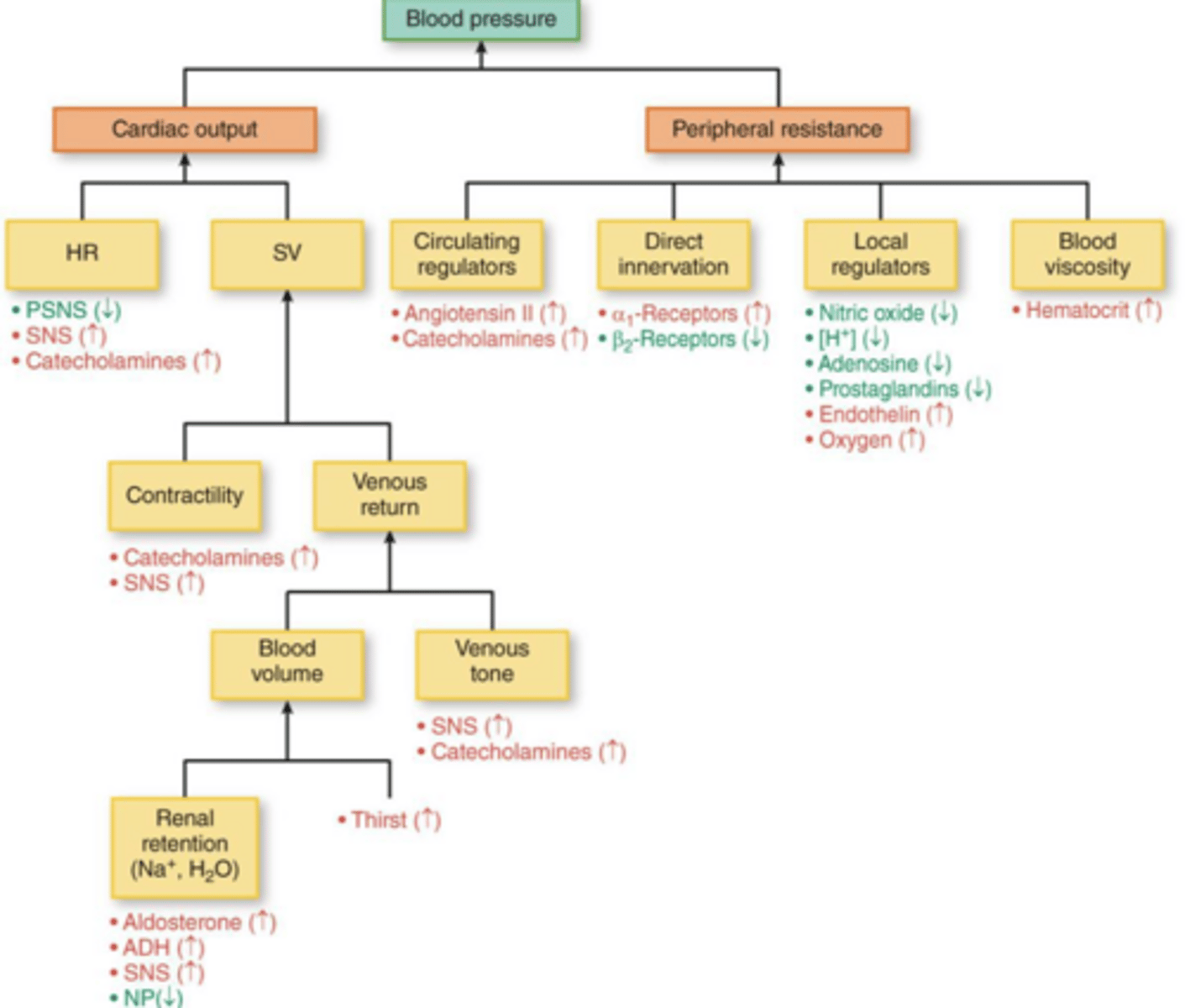
What are the two primary components that determine blood pressure?
Cardiac output (CO) and total peripheral resistance (TPR).
Define Systolic Blood Pressure (SBP).
The peak aortic pressure during the ejection of blood from the left ventricle into the aorta.
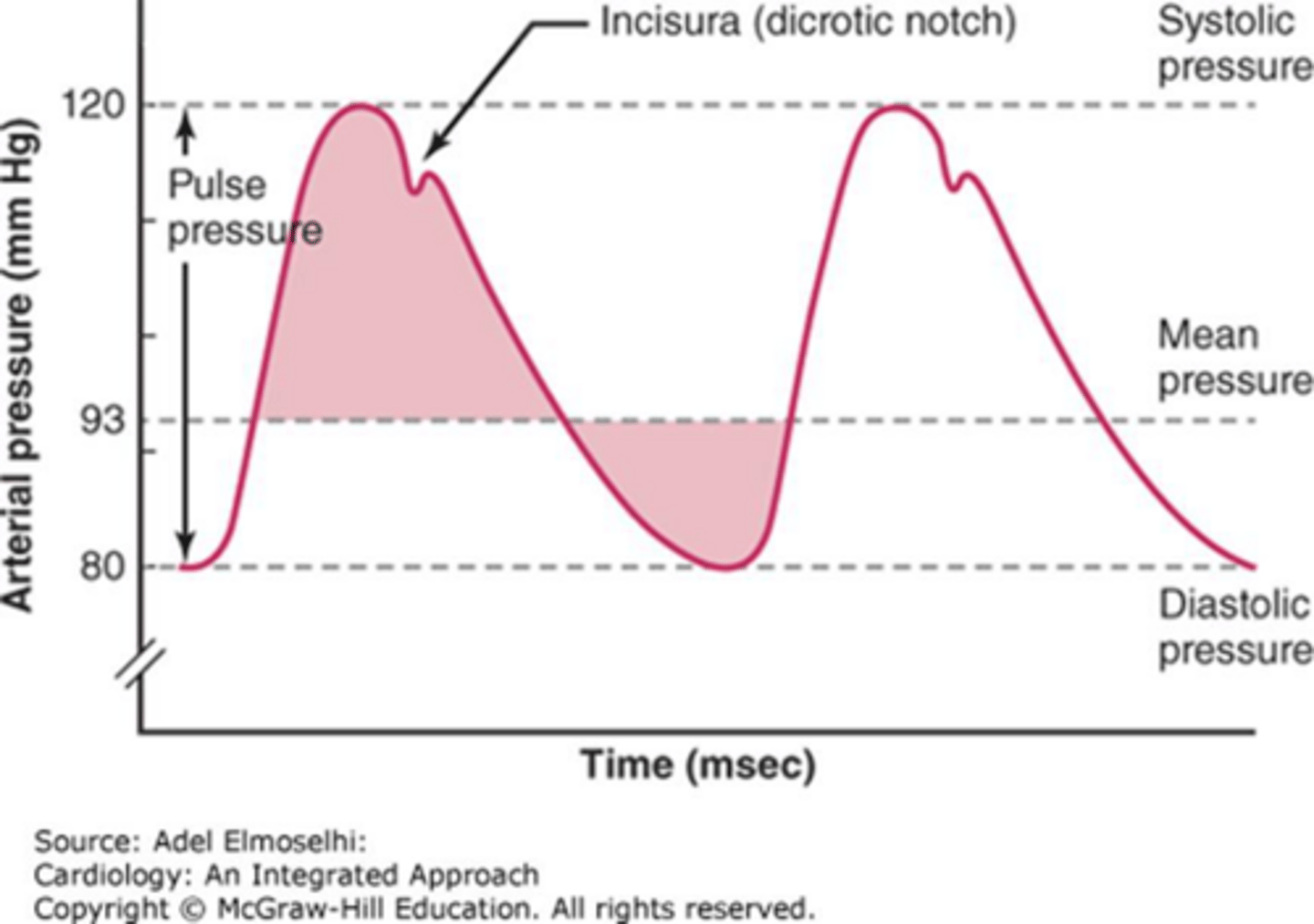
Define Diastolic Blood Pressure (DBP).
The minimum aortic pressure during the relaxation phase of the ventricles.
What is Mean Arterial Pressure (MAP)?
The average pressure throughout the cardiac cycle.
What are the primary short-term blood pressure control mechanisms?
CNS receptors, baroreceptors (carotid sinus and aortic arch), and chemoreceptors.
What is the primary long-term blood pressure control mechanism?
Renal-body fluid feedback (pressure natriuresis/diuresis).
According to 2017 ACC/AHA guidelines, what is the blood pressure range for 'Elevated' hypertension?
Systolic 120-129 mmHg AND Diastolic < 80 mmHg.
According to 2017 ACC/AHA guidelines, what is the blood pressure range for Stage 1 Hypertension?
Systolic 130-139 mmHg OR Diastolic 80-89 mmHg.
According to 2017 ACC/AHA guidelines, what is the blood pressure range for Stage 2 Hypertension?
Systolic 140+ mmHg OR Diastolic 90+ mmHg.
What blood pressure reading defines a Hypertensive Crisis?
Systolic 180+ mmHg and/or Diastolic 120+ mmHg.
What are the basic requirements for accurate office blood pressure measurement?
Patient at rest for 5 minutes, not talking, chair with back support, feet on floor, arm supported, and appropriate cuff size/position.
What is the USPSTF recommendation for blood pressure screening in adults?
Annual screening for all adults 18 years and older using office blood pressure measurement.
What are the two main categories of hypertension based on etiology?
Primary (essential) hypertension and secondary hypertension.
What is the clinical significance of uncontrolled hypertension?
It significantly increases the risk of cardiovascular disease, including heart disease and stroke.
What are the two main pillars of hypertension treatment?
Lifestyle modifications and pharmacologic therapy.
What demographic groups have the highest prevalence of hypertension in the U.S.?
Males, older adults, Black adults, and those living in rural areas.
What is the difference between orthostatic hypotension and vasovagal hypotension?
Orthostatic hypotension involves a drop in BP upon standing; vasovagal hypotension is a reflex-mediated response often triggered by specific stimuli.
What is the definition of blood pressure in terms of vascular physics?
The force exerted by blood against the wall of a blood vessel, depending mainly on blood volume and vascular compliance (tone).
Why should an abnormal blood pressure reading be repeated?
To confirm the reading and rule out errors caused by variables like patient position, technique, or temporary stress.
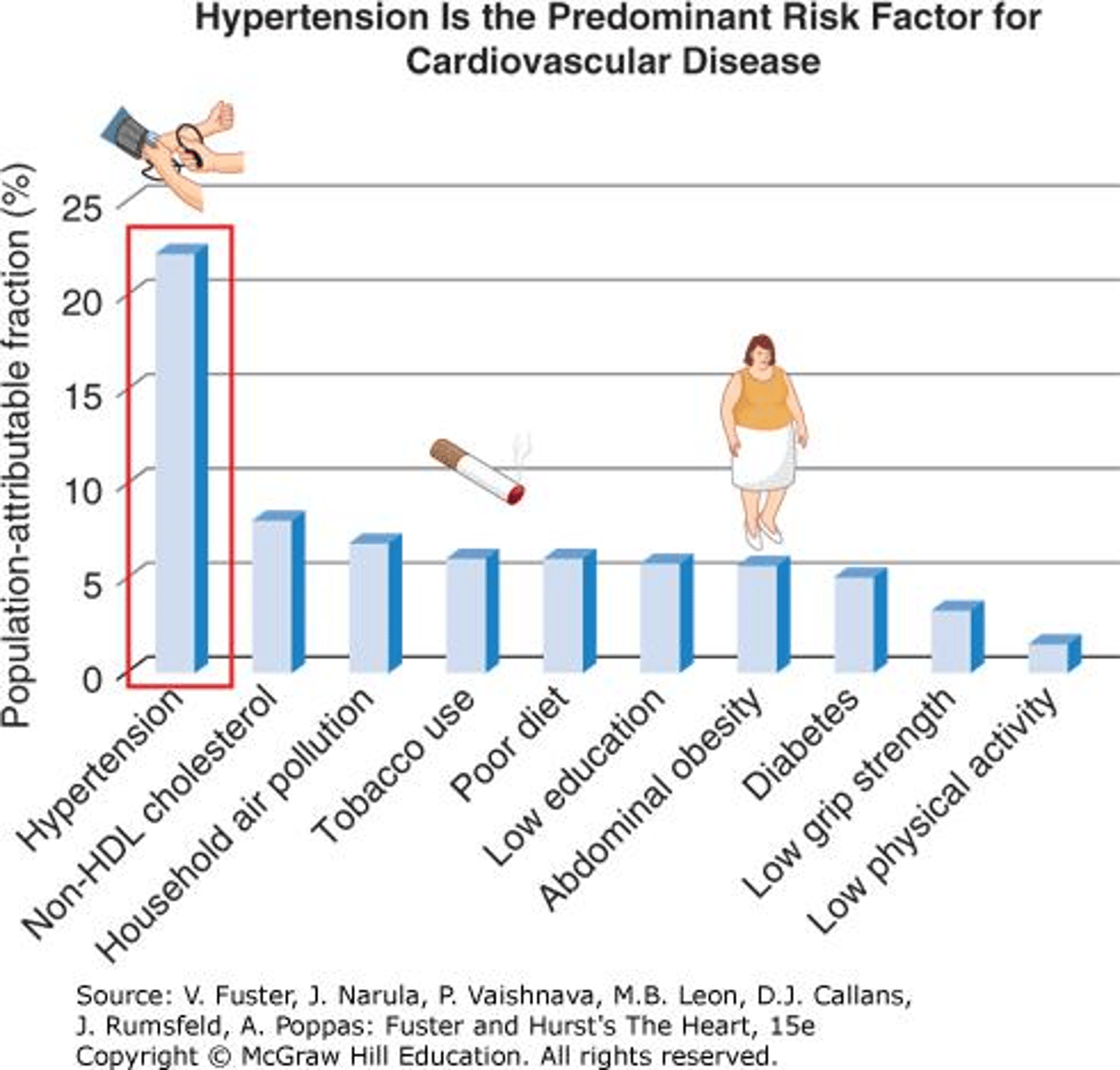
What is the relationship between cardiovascular disease risk and blood pressure?
Cardiovascular disease risk is directly related to blood pressure levels.
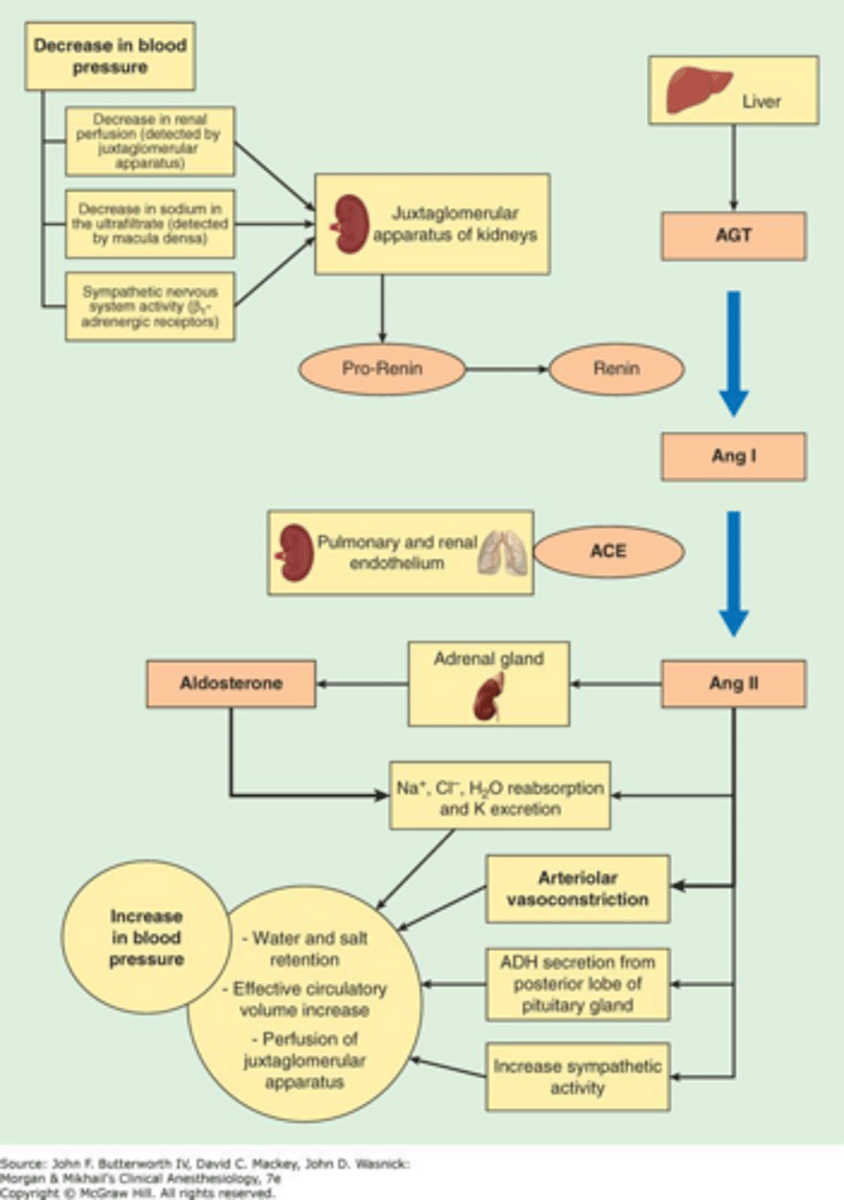
What is the role of the renin-angiotensin-aldosterone system (RAAS) in BP regulation?
It is a key hormonal system that regulates blood pressure, fluid balance, and systemic vascular resistance.
What are the common clinical complications of uncontrolled hypertension?
End-organ damage, including heart disease, stroke, and other cardiovascular complications.
What is the recommended age to begin routine blood pressure screening in children?
Age 3 and older at annual preventive visits.
What is the primary goal of managing hypertensive emergencies?
Immediate management to prevent further end-organ damage and stabilize the patient.
What is the importance of patient counseling in long-term hypertension management?
It emphasizes medication adherence, lifestyle modifications, and monitoring strategies to ensure long-term control.
What is the general clinical definition of hypertension?
Meeting hypertension criteria on two separate occasions.
List four non-modifiable risk factors for hypertension.
Older age, male sex, race, and genetic variants.
List four modifiable risk factors for hypertension.
Obesity, sedentary lifestyle, smoking, and high sodium intake.
What are the two primary physiological drivers of increased systemic vascular resistance (SVR)?
Changes in the arteriolar bed and abnormally increased tone in the autonomic nervous system originating in the vasomotor system.
What are the three primary stimuli for renin secretion by the kidney?
Decreased NaCl transport at the macula densa, decreased pressure/stretch of the renal afferent arteriole, and sympathetic stimulation of beta-1 adrenoreceptors.
How does the Renin-Angiotensin-Aldosterone System (RAAS) increase blood pressure?
Renin leads to Angiotensin II (vasoconstriction) and Aldosterone (sodium and water retention), which increases blood volume and cardiac output.
What is the recommended stepwise approach to diagnosing hypertension?
Step 1: Confirm elevated BP (≥130/80); Step 2: Rule out measurement error; Step 3: Confirm with out-of-office readings (home or ambulatory monitoring).
What is the difference between White Coat Hypertension and Masked Hypertension?
White Coat HTN is elevated BP in the office but normal at home; Masked HTN is normal BP in the office but elevated at home.
What clinical features should raise suspicion for secondary hypertension?
Onset at an early age (<30), abrupt onset, exacerbation of previously controlled HTN, drug-resistant HTN, severe elevations, or associated symptoms.
What are three major complications of untreated or undertreated hypertension?
Congestive heart failure, stroke (cerebrovascular accident), and hypertensive nephropathy.
What physical exam finding suggests coarctation of the aorta?
Radial-femoral pulse delay.
Which symptoms are associated with Pheochromocytoma in the context of secondary HTN?
Sweating, palpitations, and headaches.
What is the ACC/AHA blood pressure goal for a patient with increased CV risk?
< 130/80 mmHg.
What is the ACC/AHA blood pressure goal for a patient over 65 years old?
< 130 SBP.
What does a radial-femoral delay indicate during a physical exam?
Coarctation of the aorta.
What are the three stimuli for the inhibition of renin secretion?
Increased NaCl transport, increased stretch within the renal afferent arteriole, and beta-1 adrenoreceptor blockade.
What is the primary function of Angiotensin II in the RAAS pathway?
It causes vasoconstriction of the arterioles.
What is the primary function of Aldosterone in the RAAS pathway?
It increases sodium retention, which leads to water retention and increased blood volume.
What is the significance of Labile Hypertension?
It is characterized by variability of systolic blood pressure; treatment can be challenging and it may be associated with anxiety or increased catecholamines.
What diagnostic labs are typically included in an initial hypertension workup?
CBC, BMP (electrolytes/kidney function), lipid panel, and urinalysis.
When is an ECHO indicated in a hypertension workup?
If there are clinical signs or symptoms of cardiac disease.
What are the two main causes of increased blood volume in hypertension?
Renal dysfunction or hormonal dysfunction.
What is the relationship between sodium intake and potassium intake regarding hypertension risk?
High sodium intake and low potassium intake are both risk factors for hypertension.
What are the specific requirements for an accurate office blood pressure measurement?
Correct cuff size, patient seated and rested for 5 minutes, no talking, and feet flat on the floor.
What is the single greatest risk factor for cardiovascular disease (CVD)?
Hypertension.
What is the recommended blood pressure goal for patients with increased cardiovascular risk?
< 130/80 mmHg
Which patient population benefits the most from tighter blood pressure control (e.g., < 120/80)?
Patients at risk for stroke.
What are the two primary physiological targets for hypertension treatment?
Systemic vascular resistance and volume management.
What is the primary mechanism of action of ACE inhibitors?
They inhibit the formation of angiotensin II and stimulate the synthesis of vasodilating prostaglandins.
Why are ACE inhibitors preferred for patients with diabetes?
They provide renal protection.
What is the most common side effect associated with ACE inhibitors?
Chronic cough.
What are the critical contraindications for both ACE inhibitors and ARBs?
Pregnancy (or planning pregnancy) and concurrent use with each other.
What monitoring is required after initiating an ACE inhibitor or ARB?
Follow-up in 2-4 weeks to check serum creatinine and potassium levels.
Which ARB is known for having the longest half-life?
Telmisartan.
Why is Aliskiren typically reserved for patients who cannot tolerate ACE inhibitors or ARBs?
ACE inhibitors and ARBs provide superior kidney protection and have better clinical evidence for preventing T2DM nephropathy.
What is the primary difference between dihydropyridine and non-dihydropyridine calcium channel blockers?
Dihydropyridines act predominantly on the peripheral vascular system, while non-dihydropyridines have SA and AV node depressant effects.
Which class of calcium channel blockers is preferred for the treatment of hypertension?
Dihydropyridine CCBs.
What is a common side effect of dihydropyridine CCBs and how can it be minimized?
Peripheral edema; it can be minimized by combining the CCB with an ACE inhibitor or ARB.
Why should beta-blockers be used with caution when combined with non-dihydropyridine CCBs?
Both classes can cause SA/AV node depression, leading to excessive bradycardia or heart block.
What is the mechanism of action of thiazide diuretics?
They decrease plasma volume and peripheral vascular resistance by inhibiting sodium and chloride resorption in the distal convoluted tubule.
Which thiazide diuretic is considered more potent and longer-acting than hydrochlorothiazide?
Chlorthalidone.
What electrolyte disturbance should be monitored when using thiazide diuretics?
Hypokalemia and other electrolyte imbalances; also, note that they can elevate uric acid levels.
What is the primary clinical use of loop diuretics in the context of cardiovascular disease?
Fluid management (e.g., in CHF) rather than primary blood pressure control.
What is the mechanism of action of loop diuretics?
Inhibition of Na, K, and Cl reabsorption in the thick ascending loop of Henle.
Which patient populations might prefer a calcium channel blocker as a first-line agent?
Black populations and older persons.
What is the risk of combining an ACE inhibitor or ARB with a potassium-sparing diuretic?
Increased risk of hyperkalemia.
Are ACE inhibitors or ARBs considered first-line agents for essential hypertension?
Yes, both are considered first-line agents.
What is a serious, potentially life-threatening side effect of both ACE inhibitors and ARBs that can occur at any time?
Angioedema.
Why is Metolazone typically used in clinical practice?
It is more commonly used for edema management in patients with congestive heart failure.
What is the primary mechanism of action of loop diuretics?
They inhibit sodium reabsorption in the loop of Henle, leading to increased excretion of sodium and water.
Which loop diuretic is commonly used for edema management with a significantly different dosing profile than others?
Furosemide (Lasix).
What is the mnemonic for remembering cardioselective beta-blockers?
BEAM (Bisoprolol, Esmolol, Atenolol, Metoprolol).
Why are cardioselective beta-blockers preferred in patients with chronic lung disease?
They have specificity for beta-1 receptors (cardiac) and avoid blocking beta-2 receptors in the bronchi.
What are two common side effects of non-selective beta-blockers due to beta-2 receptor blockade?
Bronchospasm and vasoconstriction.
Which patient populations benefit specifically from beta-blocker therapy?
Patients with congestive heart failure (CHF) and those who have had a previous myocardial infarction (MI).
What is the primary mechanism of action of Aldosterone Receptor Antagonists (MRAs)?
They induce sodium excretion by the kidneys and act as potassium-sparing diuretics.
What is a significant risk when combining MRAs with ACE inhibitors or ARBs?
Hyperkalemia.
Which specific side effect is associated with Spironolactone but not typically Eplerenone?
Breast pain and gynecomastia.
What is the mechanism of action of alpha-blockers in hypertension?
They block postsynaptic alpha-receptors, relaxing smooth muscle and reducing systemic vascular resistance (SVR).
What is tachyphylaxis in the context of alpha-blocker therapy?
The potential to lose the antihypertensive effect with long-term therapy.
Why should beta-blockers be avoided as monotherapy in patients with pheochromocytoma?
It can lead to unopposed alpha-adrenergic stimulation, worsening hypertension; they should be used in combination with alpha-blockers.
Which antihypertensive agent is considered a reasonable option for pregnant patients?
Methyldopa or Labetalol.
What is a major risk associated with the abrupt discontinuation of Clonidine?
Rebound hypertension.
What are the first-line antihypertensive classes for the general population?
ACE inhibitors, ARBs, CCBs, or Thiazide diuretics.
What is the preferred first-line antihypertensive therapy for Black patients?
CCBs or Thiazide diuretics.
What is the preferred first-line antihypertensive therapy for patients with CKD or Diabetes?
ACE inhibitors or ARBs.
How is resistant hypertension defined?
Blood pressure that remains uncontrolled despite the use of three or more antihypertensive drugs.
What does the mnemonic 'O CRAP - 3' stand for in the context of secondary hypertension?
Obstructive sleep apnea, Cushing's disease, Renal artery stenosis/Fibromuscular dysplasia, Aortic coarctation, Pheochromocytoma, and the 3 Hypers (Hyperthyroid, Hyperaldosteronism, Hyperparathyroidism).
What are the classic clinical findings of primary hyperaldosteronism?
Resistant hypertension, hypokalemia, and low renin levels.
What are the classic symptoms of a pheochromocytoma?
Paroxysmal hypertension, headache, palpitations, and sweating.
How does Cushing's disease contribute to hypertension?
Increased cortisol levels cause renal sodium retention, increased angiotensin II levels, and enhanced vascular response to norepinephrine.
What is the recommended amount of exercise per week for hypertension management according to the AHA?
150 minutes per week.
What is the standard approach for stepwise medication escalation in hypertension?
Start with one drug, then increase the dose or add a second agent, followed by a third agent, and finally adding spironolactone.
How much time should generally be allowed for a drug to reach its full antihypertensive effect before adjusting therapy?
Approximately 2 weeks.
What is the recommended time interval to allow for each antihypertensive drug to reach its full effect?
2 weeks