Nursing Process & Approach to Assessment | Quizlet
1/22
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
23 Terms
nursing process steps
ADPIE
Assessment
Diagnosis
Planning
Implementation
Evaluation
nursing process: assessment (noticing)
nurse collects & analyzes patient info
SODA:
Subjective: what the patient says (current complaint, history, meds, pain scale)
Objective: what you can see/measure (VS, intake & output of fluids, height/weight, grimacing,...)
Diagnostic: labs, imaging (x-ray, CT,...)
Assessment: your physical assessment (head to toe)
nursing process: diagnosis (interpreting)
RN's clinical judgement about actual or potential health problems to help prioritize plan & care
nursing diagnosis statement: problem, related to (r/t) (usually medical diagnosis), as evidenced by (AEB) (S&S)
nursing diagnosis (ND): client's response to disorder or condition
medical diagnosis (MD): made by provider about disorder or condition
NANDA list: a list of nursing diagnosis phrases
nursing process: planning (responding)
goals & outcomes formulated, personalized to individual's unique needs (client care conference held sometimes)
prioritizing problems (ABCs, safety, actual ND, risk for ND)
SMART goal (specific, measurable, achievable, relevant, time-bound)
nursing process: implementation (responding)
performing planned interventions
assist patient to meet SMART goal
have rationale for actions (why this will help the patient)
actions!!!: educating, administering medication, assessing/monitoring, changing dressings,...
nursing process: evaluation (reflecting)
effectiveness of nursing care plan is measured & evaluated -> determine if progress is satisfactory
was the SMART goal accomplished? -> change/adapt care plan if needed
how will you determine if they met this goal? -> assess/reassess
planning: prioritizing order
1.) ABCs (airway, breathing, circulation)
2.) safety
3.) risk vs. actual
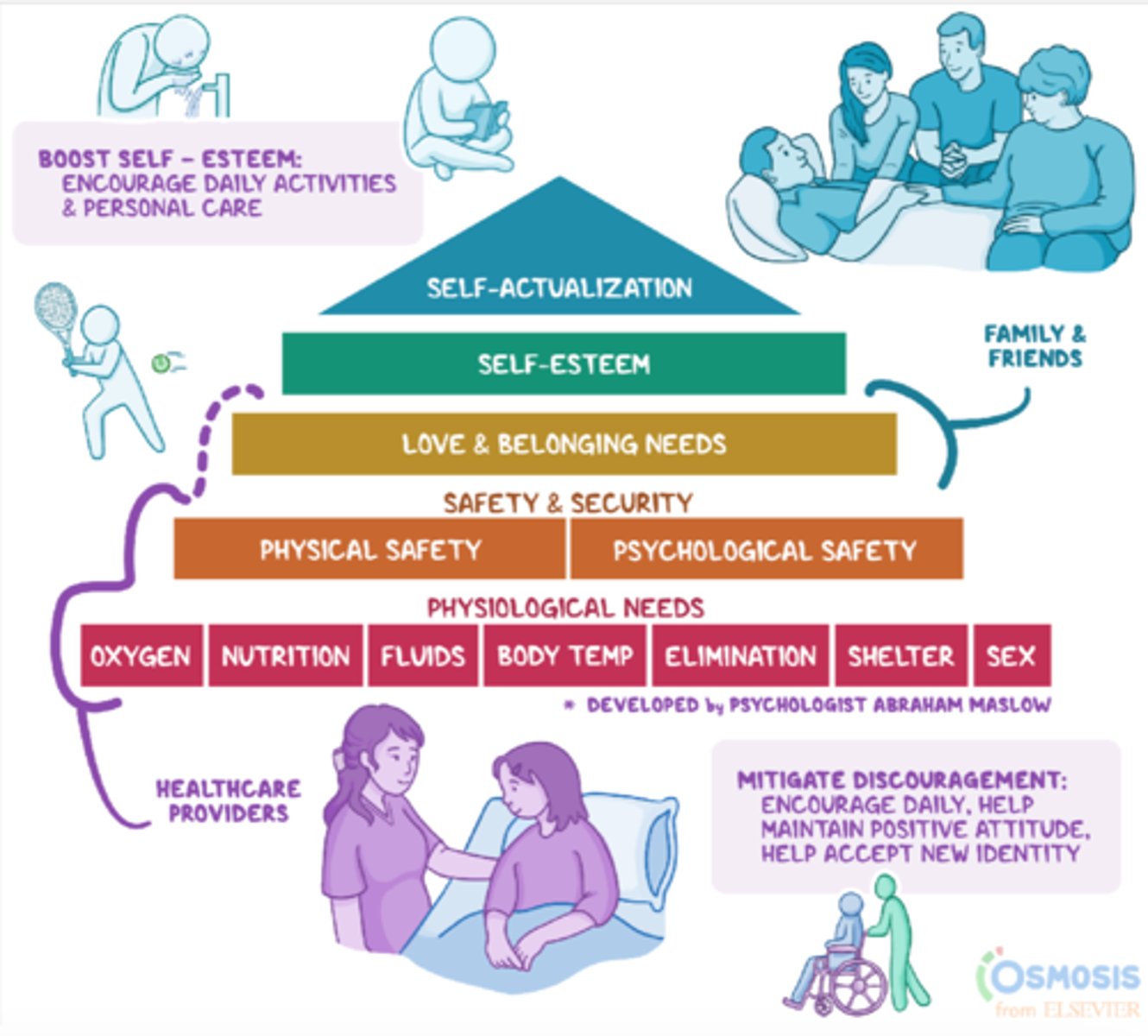
planning: prioritizing order: Maslow's Hierarchy of Needs
Bottom/most important/foundation (goes along with ABCs): physiological needs: oxygen, nutrition, fluids, body temp, elimination, shelter, sex (healthcare providers)
2nd level from bottom: safety & security: physical safety, psychological safety (healthcare providers)
middle level: love & belonging needs (family & friends, healthcare providers)
2nd level from top: self-esteem (to boost: encourage daily activities & personal care)
top level: self-actualization
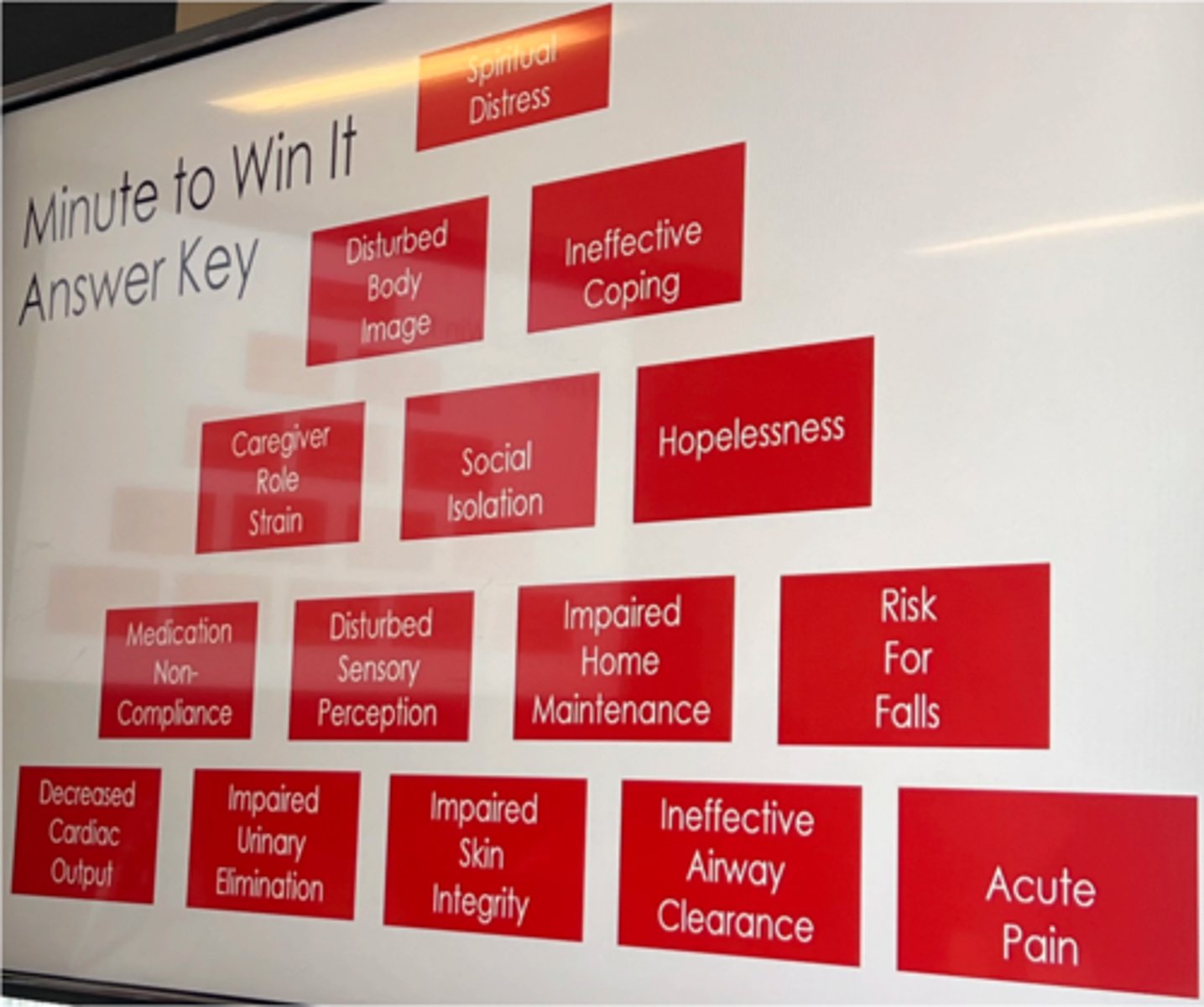
Maslow's Hierarchy of Needs practice: put in the right order (bottom level has 5 needs):
social isolation
disturbed body image
impaired urinary elimination
risk for falls
acute pain
decreased cardiac output
medication non-compliance
spiritual distress
impaired skin integrity
hopelessness
caregiver role strain
disturbed sensory perception
ineffective coping
ineffective airway clearance
impaired home maintenance
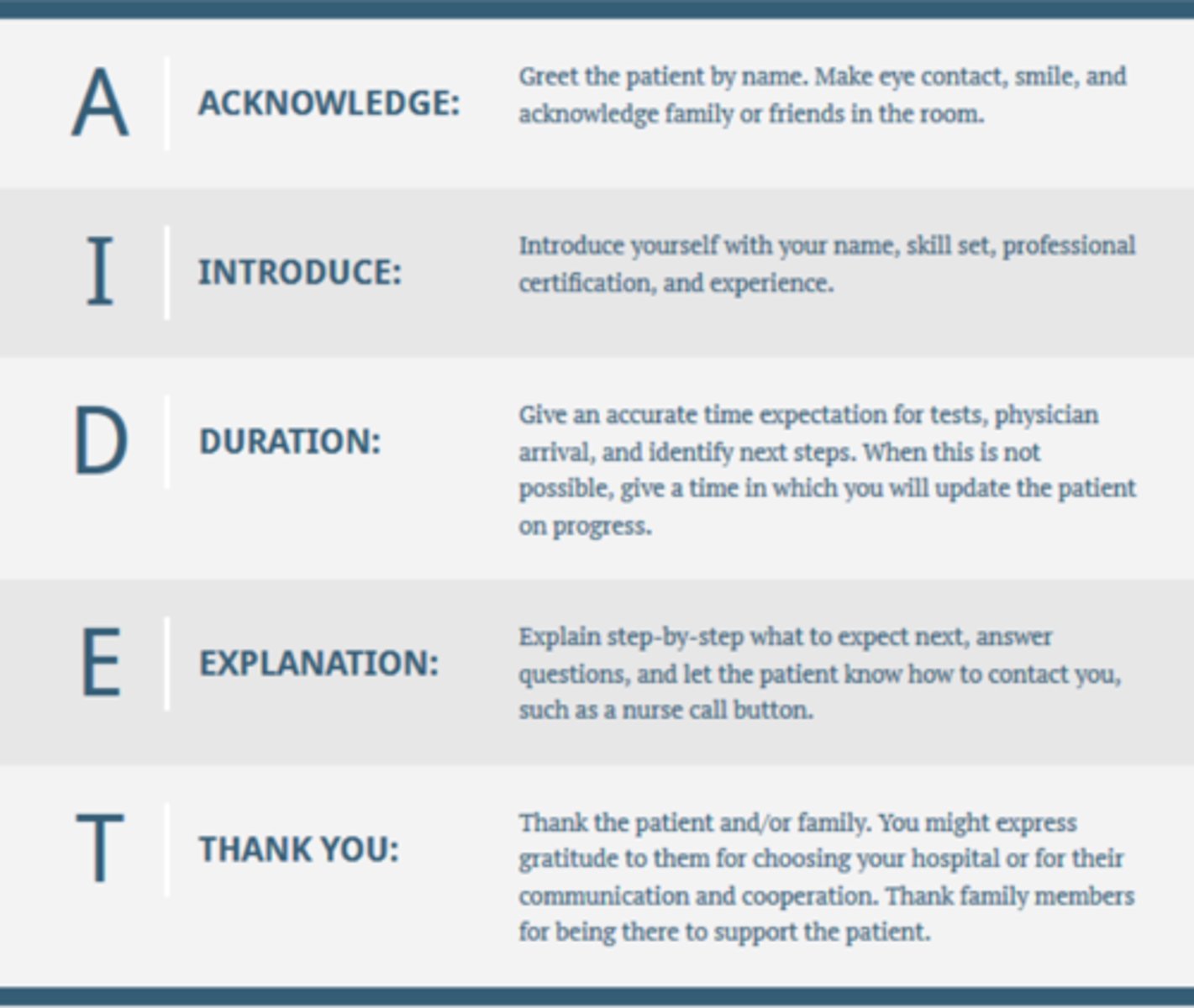
AIDET
Acknowledge: greet patient by name (verify name & DOB)
Introduce: introduce yourself by name and job title
Duration: give a time for how long the certain process will take
Explanation: explain what you are going to do; answer questions
Thank you: after you're done, thank patient & family
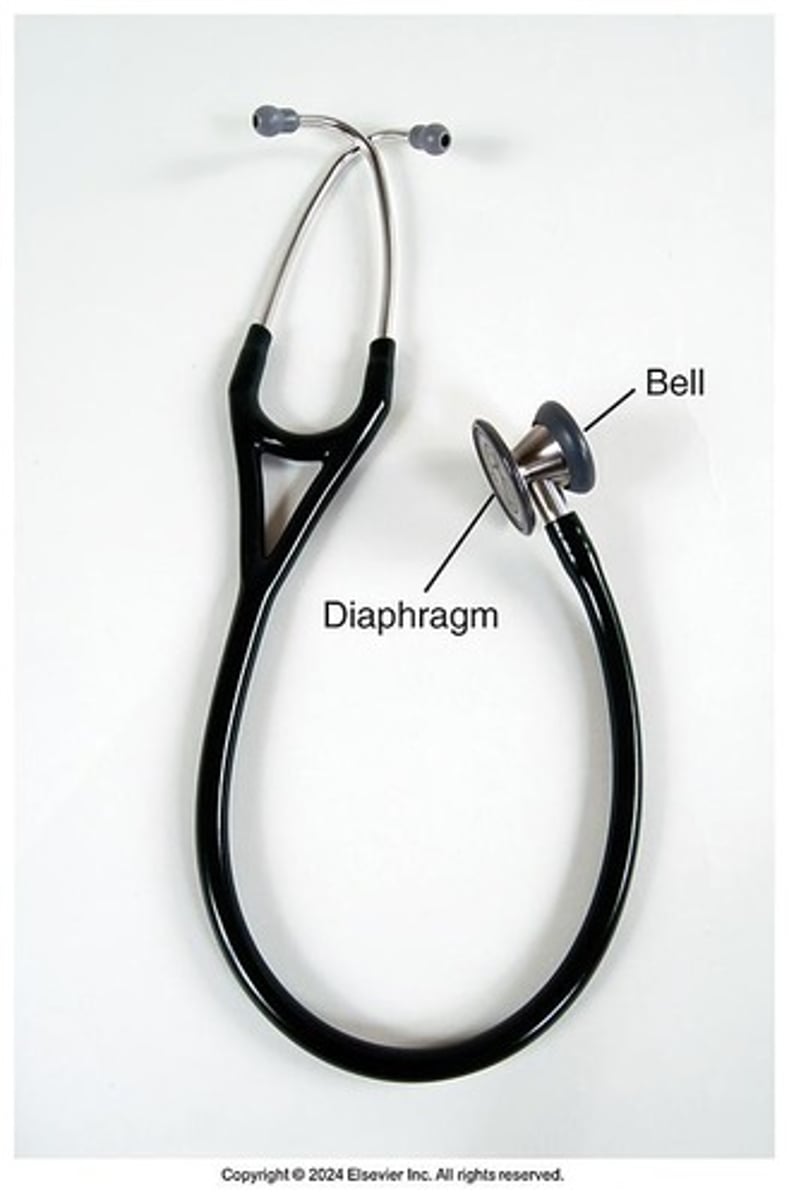
stethoscope diaphragm uses
used for high-frequency/high-pitched sounds (ex: bowel or lung sounds)
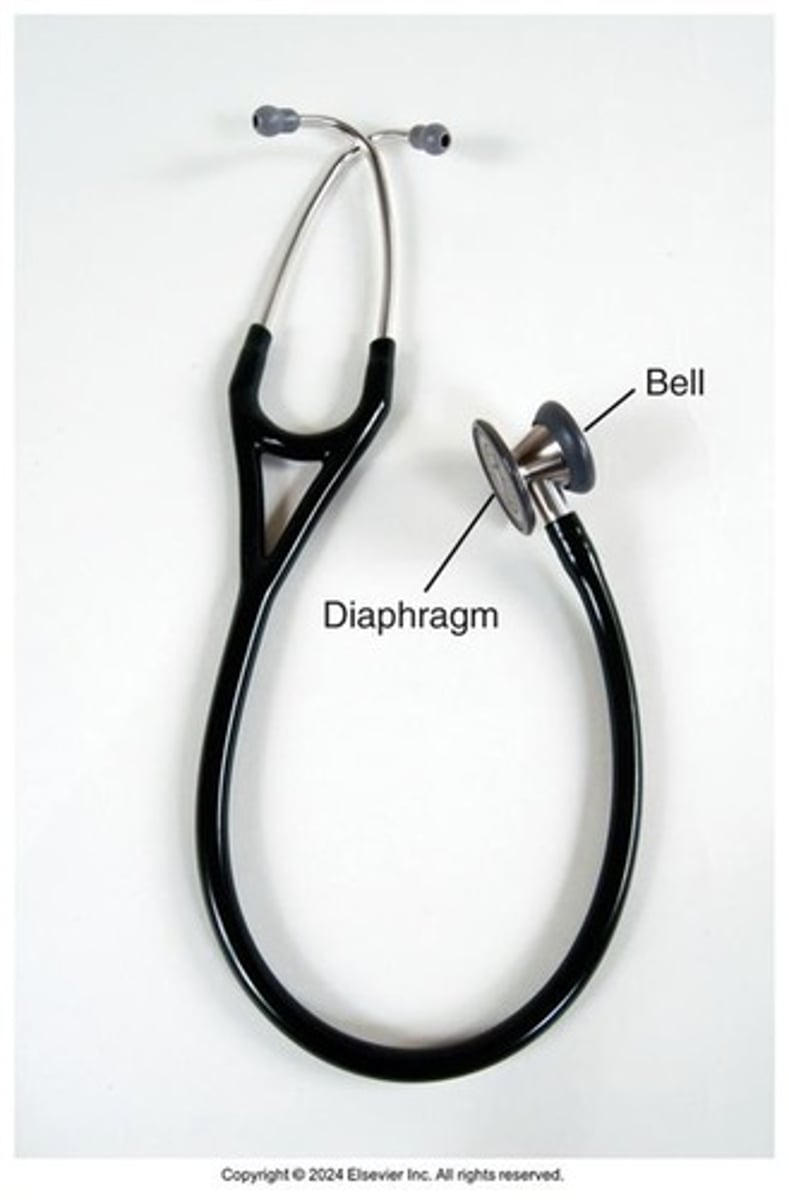
stethoscope bell uses
used for low-frequency/low-pitched sounds (ex: heart sounds)
place it lightly on the skin (using too much pressure doesn't pick up the low frequencies)
penlight uses
uses focused light to enhance inspection
assess PERRLA: are
Pupils equal,
Round,
Reactive to light, and do they have
Accommodation?
also used to closely visualize certain structures: eyes, ears, nose, mouth, throat, lesions, or skin changes
tape measure uses
to measure certain parts of body (ex: circumference of swollen extremities, fundal height of pregnant patients, circumference of infant's head, dimensions of a wound,...)
types of assessment: comprehensive/complete assessment
full head-to-toe (HTT) assessment (all body systems)
tells info about general health status
for general wellness visit, during hospital admissions, & during shift change
types of assessment: focussed assessment
depends on the situation; based on patient's presenting symptoms
used for certain medications, new problem/complaint (C/O), evaluation of intervention effectiveness, status change, in the ED
ex: abdominal pain -> assess GI system
ex: difficulty breathing -> assess respiratory system, skin, VS, level of consciousness
techniques of assessment: inspection
eyes
general inspection: gender, height & weight, race(s), age, signs of distress, body type, posture, gait, movements, hygiene, dress, mood, speech, signs of abuse, substance abuse
use adequate lighting
inspect each area for size, shape, color, symmetry, position, and abnormality
position and expose body parts as needed for viewing but respect privacy
validate findings with the patient (talk to patient about what you find)
techniques of assessment: palpation
touch
uses touch to gather info (pain, swelling, temp, texture,...)
use different part of hands to detect different characteristics
hands should be warm, fingernails short
start with light palpation (press down 1 cm to asses texture, temp, pulsations); end with deep palpation (press down 4 cm to asses internal structures & their size, shape, mobility)
techniques of assessment: palpation: bimanual palpation
2 hands
top hand applies pressure & bottom hand feels underlying structure
often used for kidney exam or if client is obese
techniques of assessment: percussion
percuss
tap finger on skin with fingertips to vibrate underlying tissues & organs
sound determines location, size, & density of structures (the denser the tissue, the quieter the sound)
*being replaced by imaging nowadays
techniques of assessment: auscultation
listen
listen for sounds produced by body -> stethoscope or hear for respiratory stridor (high-pitched, whistling or crowing sound when airway is narrowed)
order of assessment techniques: non-abdominal
IPPA
Inspection
Palpation
Percussion
Auscultation
order of assessment techniques: abdominal
IAPP
Inspection
Auscultation
Percussion
Palpation
(percussing and palpating might change abdomen sounds, so you do those after auscultation)
(think "listen first" -> but obviously you look with your eyes/inspect first in any situation duh)