Unit 5: Postpartum Part 2 (Ch 22 and 33)
1/65
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
66 Terms
processes of parent-infant relationships
attachment
bonding
proximity
mutuality
acquaintance
claiming process
bonding
the emotions and feelings experienced by the mother (or parent) in relation to the infant
attachment
two-way interaction between the mother (or primary caregiver) and the infant that develops during the first year of the infant’s life
proximity
staying close to the infant
mutuality
the infant’s behaviors and characteristics elicit a corresponding set of parental behaviors and characteristics
acquaintance
eye contact, touching, talking, and exploring to become acquainted with their infant
claiming
the identification of the new infant
The child is first identified in terms of likeness to other family members, then in terms of differences, and finally in terms of uniqueness
early interaction
skin to skin with mom or partner
helps with bonding and breastfeeding
couplet care / rooming in / dyading
promotes?
drawbacks?
mom and bay stay in the same room for the length of hospital stay
promotes bonding and learning but mom is required to be with baby 24/7
she may lose rest
biorhythmicity
the fetus is in tune with the mother’s natural rhythms, such as her heartbeat
en face is when
baby is 12 inches from mom making eye contact
entrainment
allows for?
what are the babies doing
Newborns move in time with the structure of adult speech
allows babies to begin to acquire speech
They wave their arms, lift their heads, and kick their legs, seemingly “dancing in tune” to a parent’s voice.
Reciprocity
baby’s part
mom’s part
Reciprocity is a type of body movement or behavior that provides the observer with cues
newborn fusses and cries, the mother responds by picking up and cradling the infant,
the baby becomes quiet and alert and establishes eye contact, and the mother verbalizes, sings, and coos while the baby maintains eye contact
back and forth
synchrony
the “fit” between the infant’s cues and the parent’s response
synchronous interaction is mutually rewarding
specific cry in response to different situations such as boredom, loneliness, hunger, and discomfort
Parents learn to interpret
parent may need assistance in interpreting these cries, along with trial-and-error interventions, before synchrony develops
common issues parents face
sexual intimacy
division of responsibilities
financial concerns
balancing work and parental responsibilities
social activities
adolescent moms are more at risk for
more at risk for preeclampsia, anemia, infection, preterm birth, LGW
PPD, IPV, substance abuse
lack of prenatal care
babies of adolescent moms are more at risk for
growth and development issues
language and speech delays / cognitive delays
neglect and abuse
issues with adolescent dads
may not live with mom & baby
limited education
live in poverty
cannot help financially
advanced maternal age issues
may lack time & energy
may have less support
may also be taking care of their own parents
same sex couples at risk for
lack of support bc of attitude of caregiver
visually impaired parents
need oral teaching by health care providers
needs an orientation to the hospital room that allows the parent to move about the room independently. For example, “Go to the left of the bed and trail the wall until you feel the first door. That is the bathroom.”
need explanations of routines.
need to feel devices and to hear descriptions of the devices.
chance to ask questions.
need the opportunity to hold and touch the infant after birth.
Nurses need to demonstrate infant care by touch and to follow with, “Now show me how you would do it.”
Nurses need to give instructions such as “I’m going to give you the baby. The head is to your left side.
hearing impaired parents
Before initiating communication, be aware of the parent’s preferences and capabilities. Do they wear a hearing aid? Do they read lips? Do they wish to have an interpreter
Make certain that the parent sees you approaching to avoid startling the parent.
Before speaking, be directly in front of the parent and have their full attention.
Avoid standing in front of a light or a window while speaking to the parent.
If the parent relies on lip-reading, sit close enough so that the parent can easily see your lip movements.
Speak clearly with a regular voice volume and lip movements while maintaining eye contact.
Speak in short, simple sentences to facilitate understanding.
If the parent does not understand something, it is better to find a different way to say what needs to be communicated rather than repeating the same words over and over.
Written / visual messages aid in communication. A small white or black erasable board can be useful.
Give educational materials to the hearing-impaired parent and ask them to read the materials before doing parent teaching. They can refer to the materials after discharge.
When doing parent teaching, it is helpful for a hearing person (partner or family member) to be present.
Allow ample time to communicate with the hearing-impaired parent; being in a rush can evoke stress and create barriers to effective communication.
Strategies for Facilitating Sibling Acceptance of a New Baby in Prenatal period
• Take your child on a prenatal visit. Let the child listen to the fetal heartbeat and feel the infant move.
• Involve the child in preparations for the infant, such as helping to decorate the infant’s room.
• Move the child to a bed (if still sleeping in a crib) at least 2 months before the infant is due.
• Read books, show videos or DVDs, and/or take your child to sibling preparation classes, including a hospital tour.
• Answer your child’s questions about the coming birth and what babies are like and any other questions.
• Take your child to the homes of friends who have newborns so that the child has realistic expectations of what babies are like
Strategies for Facilitating Sibling Acceptance of a New Baby During the Stay in the Birth Facility
• Have someone bring the child to the birth facility to visit you and the infant (unless you plan to have the child attend the birth).
• When the child arrives, make sure your arms are open to embrace the child.
• Do not force interactions between the child and the infant. Often the child will be more interested in seeing you and being reassured of your love.
• Help the child explore the infant by showing how and where to touch the infant.
• Give the child a gift (from you, from the father or your partner, and the infant).
Strategies for Facilitating Sibling Acceptance of a New Baby Going Home
• Have the grandmother or another adult available to focus on the child during discharge from the birth facility and on the trip home.
• Have someone else carry the infant from the car so that you can hug the child first.
Strategies for Facilitating Sibling Acceptance of a New Baby after the baby is home
Arrange a special time for the child to be alone with each parent.
Do not exclude the child during infant feeding times. The child can sit with you and the infant and feed a doll or drink juice or milk or sit quietly with a game. You can read aloud to the child while you are feeding the infant.
Prepare small gifts for the child so that when the infant receives gifts, the child will not feel left out. The child can also help open the infant’s gifts.
praise the child for acting age appropriately (so that being an infant does not seem better than being older).
Postpartum Hemorrhage (PPH)
2 defining factors
leading cause of
when is it recognized
(1) cumulative blood loss ≥1000 mL or
(2) bleeding associated with signs/symptoms of hypovolemia within 24 hours of the birth process regardless of type of birth
Leading cause of maternal morbidity and mortality
Often unrecognized until mother has profound symptoms
Early, acute, or primary PPH occurs when
occurs within 24 hours of the birth
Late or secondary PPH occurs when
occurs more than 24 hours but less than 6 weeks after the birth
Estimated vs quantitative blood loss
how much is blood loss underestimated by
EBL is looked at and estimated, under estimated by 50%
QBL is weighed - (blood and any pads or chucks with blood on them)
uterine atony is the ?
#1 cause of PPH
aka marked hypotonia of uterus
inadequate uterine contractions
uterus remains flaccid and rapid blood loss follows
uterine atony is asscoiated with
Overdistended uterus
Macrosmic (Large) fetus
Multiple fetuses
polyhydramnios
high parity
causes of pph other than uterine atony
• Anesthesia and analgesia
• Previous history of uterine atony
• High parity
• Obesity
• Prolonged labor, oxytocin-induced labor
• Chorioamnionitis
• Trauma during labor and birth
• Forceps-assisted birth
• Vacuum-assisted birth
• Cesarean birth
• Unrepaired lacerations of the birth canal
• Ruptured uterus
• Inversion of the uterus
• Placenta accreta syndrome/morbidly adherent placenta (placenta accreta, increta, or percreta)
• Coagulation disorders
• Placental abruption
• Placenta previa
• Manual removal of retained placenta
• Magnesium sulfate administration during labor or postpartum period
• Uterine subinvolution
• Hypertensive disorders
• Intrauterine fetal demise
• Failure to progress during second stage of labor
if the blood is dark red
it originated from veins, usually varicosities
if the blood is bright red
it is from arteries
deep lacerations of the cervix or genital tract
increased risk if vacuum or forceps used
can be trickle of blood or full blown hemorrhage
if there is increased bleeding during placenta separation
indicative of incomplete placental separation
if there is increased bleeding after placenta separation
it is either uterine atony or prolapsed uterus
late or secondary PPH Is indicative of
caused by
s/s?
subinvolution
uterus didn’t contract back down
from retained placenta/ endometriosis/ pelvic infection
Signs and symptoms include prolonged lochial discharge, irregular or excessive bleeding, and sometimes hemorrhage
subinvolution tx
D&curettage
antibitoics if infection
methergine - oxytocic drug
retained placenta
how long do we give the placenta to expel
if it doesn’t come out? what may we give her during this procedure?
what drug works best
after 30 mins of the placenta is not out it can cause PPH
may need manual removal - needs anesthesia & tocolytic to relax uterus so doc can remove easier
terbutaline works fastest
risk of giving tocolytic for manual removal
what can we give to combat?
increases risk of uterine atony bc it relaxes uterus
pitocin, cytotec, hemabate can be given to stimulate contractions after the procedure
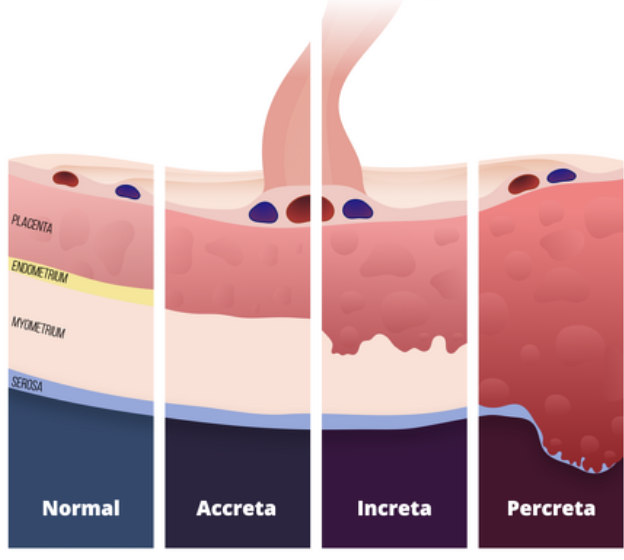
unusual placental adherence (placenta accreta)
3 degrees
r/o?
placenta accreta - slight penetration of myometrium
placenta increta - deep penetration of myometrium
placenta percreta - perforation of myometrium and uterine serosa, may involve adjacent organs
r/o PPH and previa for all 3
who is at a higher risk for placenta accreta
hx of uterine surgery like a c-section
fibroids
advanced maternal age
dx of placenta accreta
when we know?
what do we prepare for ?
ultrasound
if we know prior to brith she needs a c-section
prepare for blood transfusion
prepare for possible hysterectomy if placenta cannot come off of uterine wall (usually with intcreta and percreta)
if we do not know of placenta accreta
big r/o PPH
bleeding may not happen until placenta is coming out/ attempted manual removal
precipitous delivery
onset of labor to birth is less than 3hrs
this causes r/o lacerations → pph
other risk factors for tearing
abnormal fetus presentation/ positioning
abnormal uterine tissue
varicosities
previous scarring
hematoma
how can we identify it?
may cause/
tx?
collection of blood
may not be vaginal bleeding, but she will have persistent, abnormal perinuem/ vaginal pain especially with palpation when we assess the perimuem
may cause PPH
must be surgically evacuated
Inversion of the Uterus
can be caused by
tx?
can be caused by fundal pressure (either to get baby out or by fundal massage without supporting hand)
caused by traction/ pulling if cord
Potentially life threatening
OB emergency, needs surgery
s/s of hypovolemic shocks 7
consequences?
rapid and shallow RR
rapid pulse
cool, clammy, pale skin
urine output less than 30ml in 1 hour (won’t see unless there is a foley)
drop in LOC, lethargic , anxiety
decreased BP an H&H - late signs!
decreases venous pressure
may cause death via organs not being perfused and lack of O2
what do we do if she is PPH due to uterine atony
in this order:
firm & continuous fundal massage
catheterize/ empty bladder if fundus firms up
asses for lacerations
ensure venous access
IV - 10-40 units of pitocin/ hemabate/ cytotec
may need oxygen
draw labs - H&H, CBC, blood typing , coag factors
prepare for blood transfusion/ fluid
last resort - surgery
what do we do if she is PPH due to retained placenta (we ruled out uterine atony)
in this order
anticipate anesthesia - needs manual removal
tocolytic (tubertaline) as ordered
manual removal
combat r/o pph due to tocolytic use with oxytotic meds
what do we do if she is PPH due to suspected coagulopathy (ruled out uterine atony and retained placenta)
asses for underlying cause
start O2
anticipate fluids/ blood transfusion
anticipate antibiotics, vasodilators, uterotonic agents
may need surgery
aftermath of pph
may delay milk
increases risk of ppd
When postpartum bleeding is continuous and there is no identifiable source what should be suspected
an inherited or acquired coagulopathy should be suspected.
Idiopathic thrombocytopenic purpura (ITP)
Autoimmune disorder in which antiplatelet antibodies decrease the life span of platelets
von Willebrand disease (vWD)
A type of hemophilia
Deficiency or defect in blood clotting protein
causes of VTE
what doubles the risk
what do we assess
venous stasis and hypercoagualtion
c-section doubles risk
asses calf circumfrence, pain, color
Superficial venous thrombosis
prophylaxis?
involvement of the superficial saphenous venous system
most common VTE
anticoagulant therapy (heparin, lovenox, SCD)
Deep venous thrombosis (DVT)
what do we do?
occurs most often in the lower extremities; involvement varies but can extend from the foot to the iliofemoral region
bed rest, elevate limb, call MD
anticoagulant therapy (heparin, lovenox)
NO SCD
Pulmonary embolism (PE)
complication of DVT occurring when part of a blood clot dislodges and is carried to the pulmonary artery, where it occludes the vessel and obstructs blood flow to the lungs
rapid response emergency
C-section doubles what risk
risk of VTE
postpartum infection
when ?
temp?
first 24hrs?
Any clinical infection of the genital tract that occurs within 28 days after miscarriage, induced abortion, or birth
presence of a fever of 100.4 F or more on 2 consecutive days of the first 10 postpartum days (not including the first 24 hours after birth bc we know temp can rise, but we still notify MD)
endometritis
tx?
Infection of the lining of the uterus
Most common postpartum infection
Management: IV broad-spectrum antibiotic therapy
wound infections
rate after c-section
management?
Often develop after mothers are discharged home
Rates of wound infection after cesarean birth are 3% to 5%
Management: cleaning and drying site, look for s/s of infection and approximation
UTIs
Occur in 2% to 4% of postpartum women
void q2-3hrs to avoid