chapter 20 : venous valvular insufficiency testing
1/131
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
132 Terms
CVI (chronic venous insufficiency)
includes venous obstruction and or valvular insufficiency
pathologic reflux
must be differentiated from reverse flow that forces normal closure or fills veins segments between valves
aesthetic phlebology
is a term used to distinguish a visible condition from a truly symptomatic disorder
saphenous fascia
the saphenous veins lie within the — layers (give “eye” appearance)
GSV
courses medically in thigh and leg
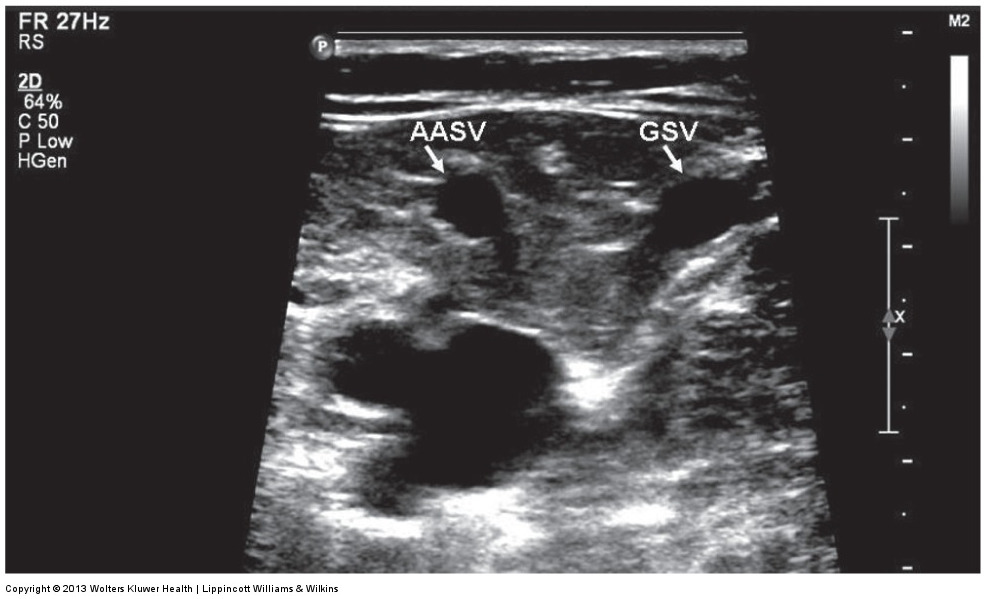
anterior accessory saphenous vein (AASV)
is aligned with femoral artery and vein in a transverse plane; lies within a saphenous compartment
courses anteriorly through thigh
posterior accessory saphenous vein (PASV)
courses posteriorly through thigh
may connect with VOG
tributaries
vessels that drain into another major vein
pierce saphenous fascia, enter the saphenous compartment, and drain into corresponding saphenous vein
ultrasound image of the alignment sign
bulging varicose veins
tributaries are often associated with —
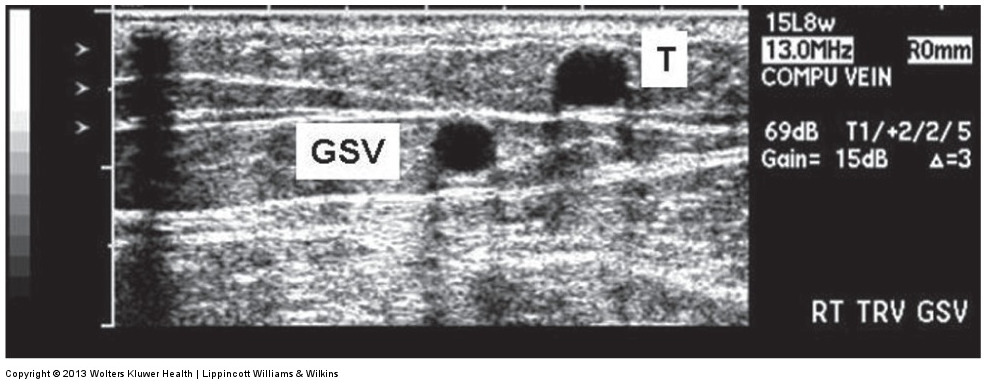
ultrasound image of a tributary vein
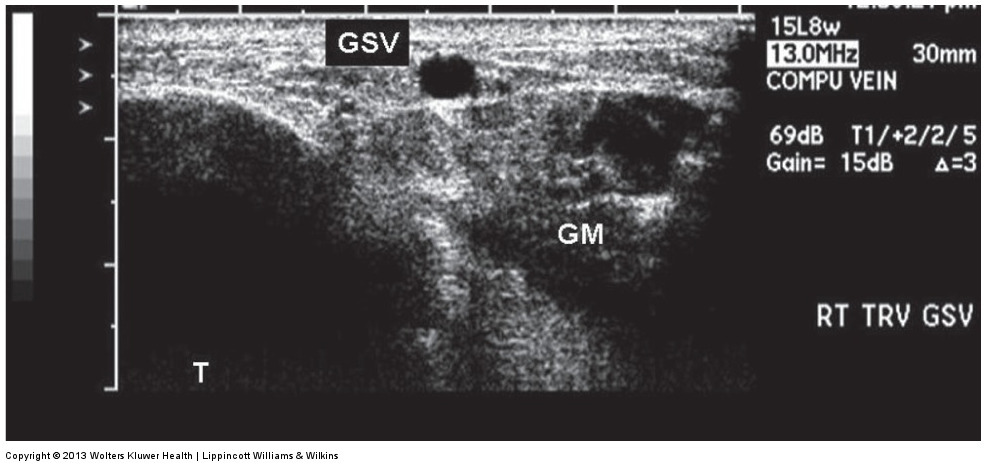
angle sign
GSV below the knee is identified by —
angle sign is a triangular form between the
gastrocnemius muscle
tibial bone
GSV within fascia
helps differentiate saphenous vein from prominent tributaries
ultrasound of the angle sign
segmental
most duplications are —; complete duplications are rare
parallel
to be duplicated, both saphenous veins must follow the same path and remain — within the fascia
saphenofemoral junction (SFJ)
confluence of the GSV and common femoral vein
contains terminal valve of the GSV
second valve (preterminal)
is distal to tributaries that join GSV and SFJ)
preterminal valves (?)
superficial epigastric vein (SEV) (tributary used as landmark for treatment)
superficial external pudendal vein
superficial circumflex iliac vein
SSV confluence with deep system is variable
popliteal vein at the saphenopopliteal junction
gastrocnemius vein
distal femoral vein of the thigh
small unnamed deep vein
perforating vein at the posterior thigh
GSV via the VOG
venous valves
bicuspid valves with leaflets that point in the direction of normal venous drainage
heart
venous valves vary in number, increasing frequency with distance away from the —
contraction
venous valves open with muscular — and close with muscular relaxation
incompetent valves
allow abnormal retrograde flow
order of blood regulating the body
blood returns to skin
to tributaries
to saphenous veins
to perforators
to deep veins
to heart
50%
of people have CVI at some point during a person’s life span
without
venous insufficiency can be present — varicose veins
35%
reflux of the lower extremities is present in up to — of general population
prevalence of reflux increases with age
highest
GSV shows the — prevalence of reflux
aesthetic phebology refers to visual signs and includes;
spider veins
telangiectasias
reticular veins
varicose veins
edema (also a palpable sign)
skin changes
ulceration
edema
patients may have temporary swelling at the end of a workday, after prolonged standing, or as a consequence of certain activities or leg positioning
edema source must be differentiated; sources include (besides venous obstruction or insufficiency)
lymphatic obstruction
sympathetic tone
cardiac disease
lipid disorders
arterial disease
skin changes
localized redness (with light or dark coloration)
atrophied blanche
corona phlebectatica (cluster of veins and skin changes)
lipodermatosclerosis (hardening of skin)
ulcerated wounds
treatment for superficial venous disease
stripping and ligation
endovenous thermal ablation
chemical ablation/sclerotheraphy
phlebectomy (micro incision)
stripping and ligation
have been traditional treatment
associated with “neovascularization”; reappearance of varicose veins
endovenous thermal ablation
has become more popular choice
thermal device top is positioned in saphenous veins distal to confluence with deep venous system
performed with either radio frequency or laser energy
vein is “closed” from within
anesthesia is places in saphenous sheath
treated vein with disappear after 6-9 month and before disapearance, treated vein will appear “thrombosed”
chemical ablation
foamed or liquid chemical (osmotic, detergent, or corrosive agent) is injected directly into the vein
effective treatment for small or tortuous veins
often used as a complement of thermal ablation
reverse trendelenburg
deep veins are evaluated initially using — position
standing
CVI evaluation should then be performed with the patient —
— allows for optimal dilation and venous filling
outward
GSV is examined with patient’s knee rotated —
back
SSV is examined with the patient’s — facing the sonographer
3.5-7.5 MHz
transducer can be used for deeper segments
7.5-17 MHz
transducers are optimal for superficial imaging
acute deep vein thrombosis (DVT)
if — is identified, CVI examination is discontinued and patient is referred for treatment
chronic DVT
is part of CVI examination
suspected in patients with history of DVT
superficial thrombosis
does not deter evaluation of CVI
— should be noted and may be treated in thrombus close to deep system junction
compression
— maneuvers are used to elicit reflux
recommended to use automatic cuff system to perform compressions
70 to 80 mm
compression cuff should quickly inflate to approximately — Hg, hold for a few seconds, then quickly deflate
normal response to proximal compression
cuff or other technique (i.e., valsalva maneuver) is used to compress veins — to segment being evaluated
flow should stop during compresssion and resume upon release of compression
normal response to distal compression
cuff or other technique is used to compress veins proximal— to segment being evaluated
flow should increase during compression (in an antegrade direction) and stop upon release of compression
abnormal responses for proximal compressions
retrograde flow occurs during compression
antegrade flow resumes upon release of compression
abnormal responses for distal compression
increase in antegrade flow during compression
retrograde flow is noted upon release of compression
reflux duration is dependent on
vein filling with blood and emptying with compression
duration of compression
interval between compressions
should wait at least 30 s between testing sites
reflux duration
(time measurement) should be performed with spectral doppler with vein in longitudinal image
parana maneuver
force patient to shift weight slightly
hand compression
less reproducible but allows more testing variability
valsalva maneuver
laughing, coughing, or talking may be alternatives
protocol for CVI should include
proper documentation of any anomaly in femoropopliteal segments
single documentation of saphenous or non saphenous abnormality
3 common test objectives for CVVI
selection of patients for thermal ablation
examination of patients of a phlebology clinic with perioperrative capabilities
examination of patients for limited or extensive stripping/ligation/phlebectomy
special considerations during foam sclerotherapy
visualize foam in the vein
transthoracic echo can be used to observe foam arrival in right heart
transcranial doppler (TCD) may demonstrate emboli in middle cerebral artery (MCA) (also indicate PFO)
alternative explanations to retrograde flow
where tributaries enter main saphenous
valve leakage (valves take too long to close or do not remain closed)
surgical correction to preserve drainage
normal b-mode:
smooth, thin-walled, fully compressible veins with no obvious change in venous diameter
acute DVT:
enlarged, incompressible veins with hypoechoic and/or hyperechoic material in lumen
chronic post-thrombotic changes:
small, retracted vein; partially or completely incompressible with hyperechoic material in lumen
b-mode ultrasound findings of chronic venous valvular insufficiency
enlarged vein diameter
vein remains completely compressible
lumen is hypoechoic
may see valve sinus with flapping valve leaflets
tortuous veins
b-mode ultrasound findings after ablation
immediately, vein still compressed by tuescence
over 6 to 9 months
segmentally sonographically absent
fibrosis or thrombosis is visualized
recanalization may occur
normal spectral waveform
spontaneous, phasic with respiration unidirectional flow toward heart
flow augments with distal compression or release of proximal compression
acute DVT spectral waveform
no flow if occlusive; lack of flow augmentation with distal compression or release of proximal compression
partial obstruction
acute or chronic or external compression can cause continuous flow
chronic post-thrombotic changes spectral waveform
small, tortuous channels within disease vein segment; flow in collateral veins
CVI spectral waveform
reverse flow (reflux) noted following proximal compression or release of distal compression
turbulent flow may be present in enlarged valve sinuses
DVT color flow
no flow if completely occlusive; flow around thrombus if not occlusive
color flow with CVI
retrograde flow can be visualized but is not quantitative
measurement of reflux duration
preferred over measurement of peak reverse flow velocity or volume flow rate
normal valve closure times for saphenous veins
less than 500 ms
normal valve closure ties for femoropopliteal veins
less than 1 s
normal valve closure times for perforating veins
less than 350 ms
duration of reflux depends on
vein diameter
venous blood volume distally
strength
duration of distal compression
characteristics of distal venous network
PPG
emits infrared light and detects signal reflected back from cutaneous vessels
compression/decompression
maneuvers performed and later the amount of blood detected
amount is reduced when blood is pumped back to heart
upon completion of maneuvers, blood volume returns to baseline
medial
PPG placed against skin in the — aspect of calf
can also be placed on posterior calf for evaluation of SSV
5-10 times
calf is emptied by halving the patient perform foot flexion/relaxation about —
PPG tracing
tracing is flatline at top of strip paper at baseline
tracing falls to bottom of strip paper with maneuvers
tracing returns to baseline position during recovery relaxation
25 mm/s
strip paper recording speed is usually —
absence of reflux
timing of blood return is measured and indicated presence or —
venous recovery time (VRT)
is measured from end of flexion/relaxation period to about 95% of the distance between the bottom curve and the baseline tracing
20 s
recovery time is normally greater than — for VRT
10 s
reflux is suspected with refill times less than 20 s; severe reflux is suggested if recovery time is less than —
air plethysmography (APG)
can be used to detect physiologic abnormalities to differentiate between pathophysiologic condition and aesthetic problem
recommended technique for quantification of chronic venous insufficiency
technique and required documentation for APG
patient starts from supine to standing positions
sensing cuff is wrapped around calf; inflated to 10 mm Hg
leg is elevated to empty venous volume
leg is brought back to horizontal; cuff is readjusted and calibrated
patient stands with weight on non-tested leg
while on nontested leg, tested leg maneuvers
relaxed
one toe raise
10 toe raises
blood venous volume
measurements of APG
(VV; in mL)
accumulated when patient moves from supine to standing
filling time (FT)
measurements of APG
how long to accumulate blood in calf to 90% of VV
volumetric filling rate (FR)
measurements of APG
blood accumulated per unit time
residual volume (RV)
measurements of APG
percentage of venous volume; indicates how much volume is pumped from calf after 10 toe raises
APG can also measure
ejection fraction
total blood volume accumulated in calf with thigh cuff compression
volumetric emptying rate (after thigh cuff deflation)
use of tourniquet to differentiate between deep and superficial reflux
VV normal
vary and depend on gender, age, and other characteristics
normal FT
longer than 25 s
normal FR
less than 2 mL/s
normal RV
less than 20%-35%