DHED 315: FINAL EXAM REVIEW (chs. 1-16)
1/158
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
159 Terms
CHAPTER 1
What is local anesthesia?
loss of sensation in area; creates numbing feeling
What is pain?
unpleasant sensory and emotional experience
What is pain control?
mechanism to alleviate pain
What is pain perception?
neurologic event; little difference between individuals
What is pain reaction?
personal response to pain; highly variable between individuals
What is pain threshold?
point when sensation is painful & discomfort occurs
What are analgesics?
meds that relieve pain; includes topical + local anesthetics
What is the Gate Theory of Pain Control?
pain results from a spinal cord mechanism that carries pain sensation between peripheral N.S. and the brain
CHAPTER 2
What are Type A Fibers?
largest myelinated fibers = fastest impulse conduction which may be afferent or efferent; requires more LA vol
Includes 4 subtypes:
1) Type A-alpha
2) Type A-gamma
3) Type A-beta
4) type A-delta
What are Type A-alpha fibers?
largest; fastest; efferent → muscle movement
What are Type A-gamma fibers?
efferent → muscle tone
What are Type A-beta fibers?
afferent → proprioception; touch; pressure
What are Type A-delta fibers?
afferent → PAIN + temperature
What are Type B fibers?
slightly myelinated; efferent; pre-ganglionic ANS → vascular smooth muscle
What are Type C Fibers?
smallest, most numerous unmyelinated; efferent and afferent; post-ganglionic ANS → temperature; PAIN
**Responsible for dull, achy pain → TOOTH PAIN
There are high numbers of what types of fibers in the oral cavity?
Type A and Type C
Nerve impulses are called _____.
ACTION POTENTIALS
• generated by "all or none" voltage change
If the stimulus is stronger, does it change the strength of the impulse?
NO - no difference in strength of impulse
• nerve impulse DOES NOT weaken as it travels
What are the 3 stages in the generation of a nerve impulse?
1. Neuron membrane is POLARIZED → inside of cell is RMP = negatively charged
2. Neuron membrane DEPOLARIZES → inside of cell is positively charged
3. Neuron membrane REPOLARIZES → inside of cell moves back to negatively charged
An action potential is generated when the neuron membrane is _____.
depolarized = INCREASED positively charged ions on the inside
In order to depolarize, the stimulus must reach a minimum threshold level of ___.
+15-20 mV = "all or none"
Greater intensity of stimulus can produce ____.
MORE impulses per second
The threshold stimulus triggers what channels to open?
triggers Na+ and K+ ion channels to open = Na+ ions flow into neuron → inside becomes positively charged
What occurs as depolarization travels along the membrane?
conduction of an action potential (nerve impulse)
The impulse crosses both ___ and ___.
• Electrical synapses - gap junctions between neurons
• Chemical synapses - synaptic clefts at end of each axon
What is released at the synaptic cleft?
neurotransmitters;
can be:
excitatory (triggers impulse - ACh/NE) OR inhibitory (increases polarization - dopamine/serotonin)
How do L.A.s cause reversible anesthesia?
by:
1) preventing generation of impulses
2) preventing conduction of impulses
Why are L.A.s considered a chemical block?
L.A.s provide a block between the source of impulse and the brain
Why are L.A.s considered "membrane-stabilizing drugs"?
they DECREASE the rate of depolarization + stops firing
How do L.A.s provide a "state-dependent blockade"?
bind easier to Na+ channels that are firing (not resting)
L.A.s bind to Na+ channels ____ the cell.
INSIDE = prevents Na+ ions from moving outside
Small diameter nerve fibers are (more/less) sensitive to L.A.s.
Large diameter nerve fibers require (more/less) volume of L.A.s.
MORE
CHAPTER 3
What are Ester L.A.s?
INCREASED RATE of allergic reactions (10%)
• if allergic to one ester, probably allergic to all esters
• metabolized in blood (plasma) via pseudocholinesterase
What are Amide L.A.s?
all injectable dental L.A.s in US are amides (topicals = ester or amide)
• low cross-hypersensitivity with Esters
• metabolized in liver
What are RNH+ molecules?
active form = binds to Na+ channels that CANNOT cross membrane
• cations (acids)
What are RN molecules?
inactive form = cannot bind to Na+ channels that CAN cross membrane
• anions (bases)
Increased lipid solubility = __ duration of L.A.
INCREASED
Increased Protein Binding = __ duration of L.A.
INCREASED
Increased Vasoconstrictor = __ duration of L.A.
INCREASED
Ester L.A.s include (3):
Where are they metabolized?
includes Topicals:
• Benzocaine
• Tetracaine
• Procaine
• all metabolized in Plasma (blood) via pseudocholinesterase + small amount in liver
Amide L.A.s include (5):
Where are they metabolized?
includes Injectables and Topicals:
• Lidocaine → metab in Liver only
• Mepivacaine → metab in Liver only
• Bupivacaine → metab in Liver only
• Prilocaine → metab in Lungs+Liver
• Articaine → metab in Plasma (90%) + Liver
Which amide L.A. has the shortest half-life?
ARTICAINE
CHAPTER 4
What is the preservative added to vasoconstrictors and what is it associated with?
Sodium Bisulfite - added for stability
• associated with allergic reactions - 10% asthmatics (dried apples, nuts, wine)
What are the 4 functions of vasoconstrictors?
1) Constrict blood vessels at site = lower dose of L.A.
2) Increases duration of L.A. = 6x longer
3) Decreases absorption rate of L.A. = decreases risk of toxicity
4) Provides hemostasis at injection site
All L.A.s are (5)
Vasodilators
Acidic
Metabolized in the liver
Excreted via kidneys
Can cross the blood-brain barrier
Overdose symptoms appear within ____.
60 seconds
The body clears the drug within ____.
5-10 minutes (via re-uptake)
What are the symptoms of overdose on vasoconstrictors?
dysrhythmias, ventricular fibrillation, dramatic increase in HR, increased BP, throbbing headache, hyperventilation, tremors, anxiety/apprehension
*can lead to cardiac arrest in patients with CV disease
CHAPTER 5
What are the available formulations of lidocaine?
Mepivacaine?
Bupivacaine?
Prilocaine?
Articaine?
• 2% 1:50,000 epi (green)
• 2% 1:100,000 epi (red)
—
• 3% plain (tan)
• 2% 1:20,000 levo (brown)
—
0.5% 1:200,000 epi (blue)
—
• 4% plain (black)
• 4% 1:200,000 epi (yellow)
—
• 4% 1:100,000 epi (gold)
• 4% 1:200,000 epi (silver)
L.A.s are expressed as ____. Vasoconstrictors are expressed as ____.
PERCENTAGES; RATIOS
What is the trade name for
Lidocaine?
Mepivacaine?
Bupivacaine?
Prilocaine?
Articaine?
Lidocaine / Xylocaine
Mepivacaine / Carbocaine
Bupivacaine / Citanest
Prilocaine / Septocaine
Articaine / Marcaine
What is the half-life of
lidocaine
mepivacaine
bupivacaine
prilocaine
articaine
1.6hrs (96 min)
1.9hrs (114 min)
1.6hrs (96 min)
2.7hrs (162 min)
45 min **SHORTEST half-life
What are the 2 L.A.s available WITHOUT a vasoconstrictor?
1. 3% Mepivacaine - Plain
2. 4% Prilocaine - Plain
CHAPTER 6
---
Know how long to apply topical anesthesia before giving an injection.
topical should be placed at the site of injection for 1-2 minutes
What are the 3 topical anesthetics?
1. Benzocaine (ester)
2. Lidocaine (amide)
3. Cetacaine: Benzocaine + Butamben + Tetracaine (all esters)
List the 2 topical anesthesias associated with methemoglobinemia.
1. Benzocaine spray
2. Prilocaine
List 3 reasons why topical anesthetics cause increased toxicity. (slide #16)
increased blood levels = increased toxicity
1. Concentrations of topicals are higher than injectable L.A.s
**inc concentration needed for diffusion through mucous membranes
2. NO vasoconstrictors in topicals = increased abs rate = increased toxicity
3. Elderly, children, medically compromised = increased toxicity/adverse rxn risk
CHAPTER 7
What are systemic diseases that are absolute contraindications for vasoconstrictors? (9)
MI within + Coronary bypass surgery within 6 months
Uncontrolled HAHAs: hypertension, angina pectoris (daily attacks), arrhythmias, hyperthyroidism
Sulfite allergy
Cocaine/amphetamine abuse
Pheochromocytoma (tumor of adrenal gland)
What are relative contraindications of vasoconstrictors?
1) Cardiovascular disease patients → use cardiac protocol
2) Taking phenothiazines → use cardiac protocol
3) Taking non-selective beta blockers → use cardiac protocol
4) Taking tricyclic antidepressants → use 0.04mg EPI; no LEVO, no 1:50,000 epi
6) Taking digitalis → consult physician before using vasoconstrictors
If the patient has a blood pressure of 140-159/90-94:
consider nitrous for stress reduction
If the patient has a blood pressure of 160-199/95-114:
retake; refer for med consult before treatment
If the patient has a blood pressure of >200/>115:
retake; refer for immediate med consult
Which L.A.s are safe to use during pregnancy?
• Prilocaine
• Lidocaine
Which L.A.s are safe to use with liver disease?
• ARTICAINE
• prilocaine (maybe)
Taking an H2 Receptor Blocker:
Taking Beta Blockers:
Significant Liver Disease:
Renal Dysfunction:
Taking Cholinesterase Inhibitors:
Taking CNS Depressants:
History of Malignant Hyperthermia:
decreases liver metabolism = use decreased dosage of Lidocaine
decreases amide metabolism = use decreased dosage of all amides
decreases amide metabolism = use Articaine/decreased dosage of amides
decreases excretion → slight risk of toxicity = use with caution
decreases plasma metabolism → NO articaine, NO ester-based topicals
possibly decreases metabolism → use DECREASED dosage of all amides
use decreased dosage of all amides; med consult
CHAPTER 8
What is MRD?
STANDS FOR maximum recommended dose. It is the highest amount of drug that can be safely administered per appointment based on pt's weight
• considers pt's physical health
What is AMD?
STANDS FOR absolute maximum dose; highest amount of drug that any patient can receive per appt regardless of weight
What is the cardiac dose?
It is the vasoconstrictor dose that can be administered safely to patients with ischemic heart disease
• EPI: 0.04mg
• LEVO: 0.2mg
What is a limiting drug?
drug that limits the total volume of L.A. delivered; can be the L.A. or the vasoconstrictor
• based on pt's medical status
Know the amount of solution in one cartridge.
1.7-1.8ml
What is the MRD and AMD for
lidocaine?
mepivacaine?
bupivacaine?
prilocaine?
articaine?
• MRD: 3.2mg/lb
• AMD: 500mg
—
• MRD: 3.0mg/lb
• AMD: 400mg
—
• MRD: 0.9mg/lb
• AMD: 90mg
—
• MRD: 4.0mg/lb
• AMD: 600mg
—
• MRD: 3.2mg/lb
• AMD: none listed
How to calculate the mg of anesthetic in one carpule
**KNOW THE MATH
• change % of L.A. to mg/ml
• multiply mg/ml by 1.7ml/carpule
Know the healthy dose and cardiac dose of epinephrine/LEVO. (slide #14)
• HEALTHY dose: 0.2mg epi + 1.0mg LEVO
• CARDIAC dose: 0.04mg epi + 0.2mg LEVO
How many carpules of epinephrine can a healthy patient have?
11.1 carpules maximum
• 0.2mg epi divided by 0.018mg/carpule = 11.1 carpules max
How many carpules of epinephrine can a cardiac patient have?
2.2 carpules maximum
• 0.04mg epi divided by 0.018mg/carpule = 2.2 carpules max
How many carpules of 1:50,000 epi can a patient with CV disease have?
How many carpules of 1:100,000 epi can a patient with CV disease have?
How many carpules of 1:200,000 epi can a patient with CV disease have?
1.1 carpules
2.2 carpules
4.4 carpules
How many carpules of 1:20,000 levo can a patient with CV disease have?
2.2 carpules
CHAPTER 9
LARGER number of gauge = ____ diameter of needle
SMALLER
• 30g is smaller than 25g
The SMALLER the diameter = the ___ reliable aspiration
LESS
What 3 needle gauges used in dentistry.
1) 25 gauge
2) 27 gauge
3) 30 gauge
Gauge selection is based on:
1) depth of penetration needed
2) risk of intravascular injection
KNOW: If there is a high risk for positive aspiration, use ___ gauge needle.
25 gauge
KNOW: Needle length selection is based on what?
the amount of tissue that must be penetrated to reach target location
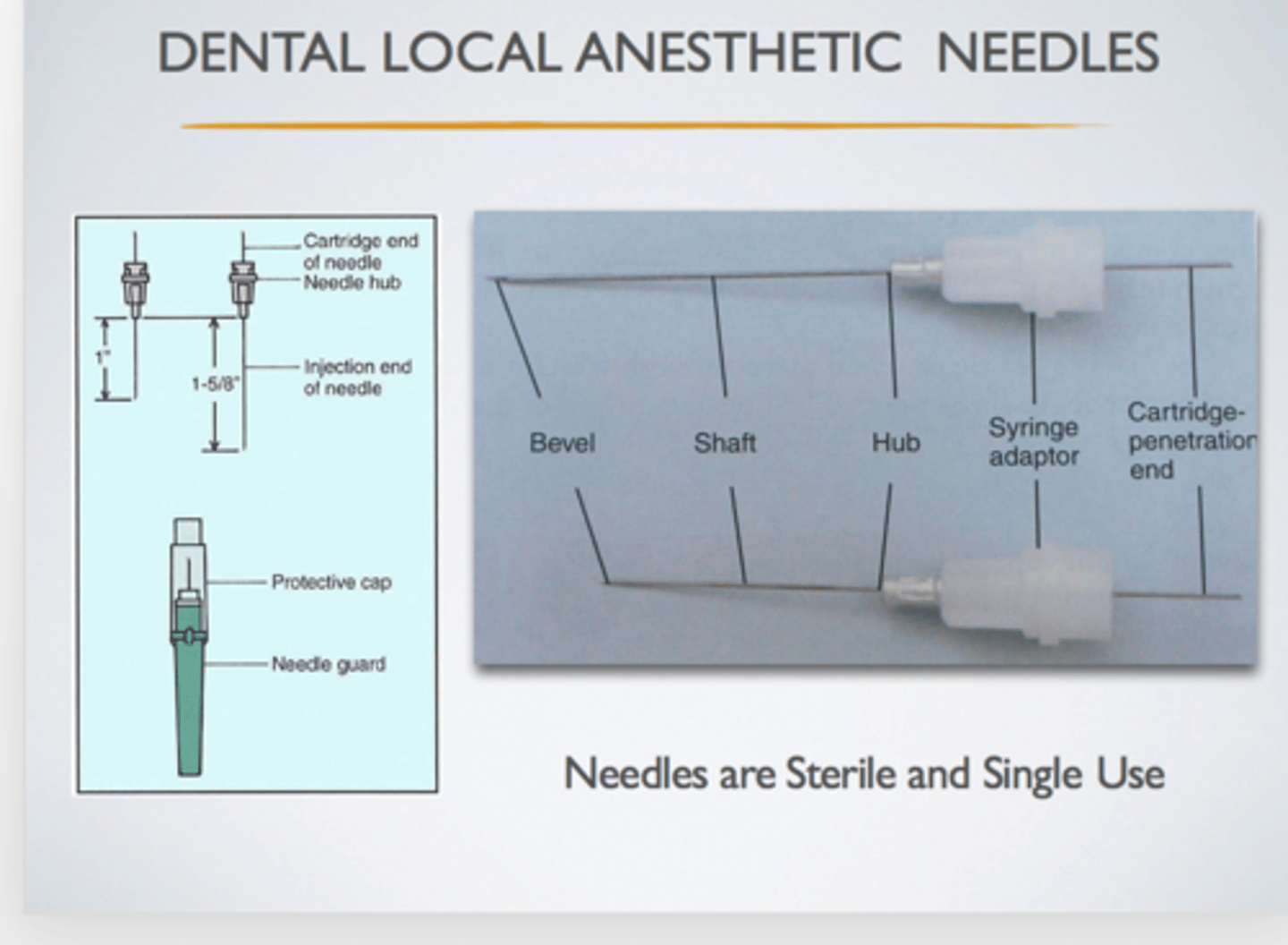
KNOW: What is the weakest part of the needle?
the hub
Know the proper way to store anesthetic cartridges.
store in a dark place; room temperature; original container
Know the 5 parts of a needle. (slide #19)
1. Bevel
2. Shaft
3. Hub
4. Syringe adaptor
5. Carpule-penetrating end
CHAPTER 10
Know the locations of:
• mandibular foramen
• mental foramen
• incisive foramen
• infraorbital foramen
Where is the mandibular foramen located?
mandible
• medial surface of ramus
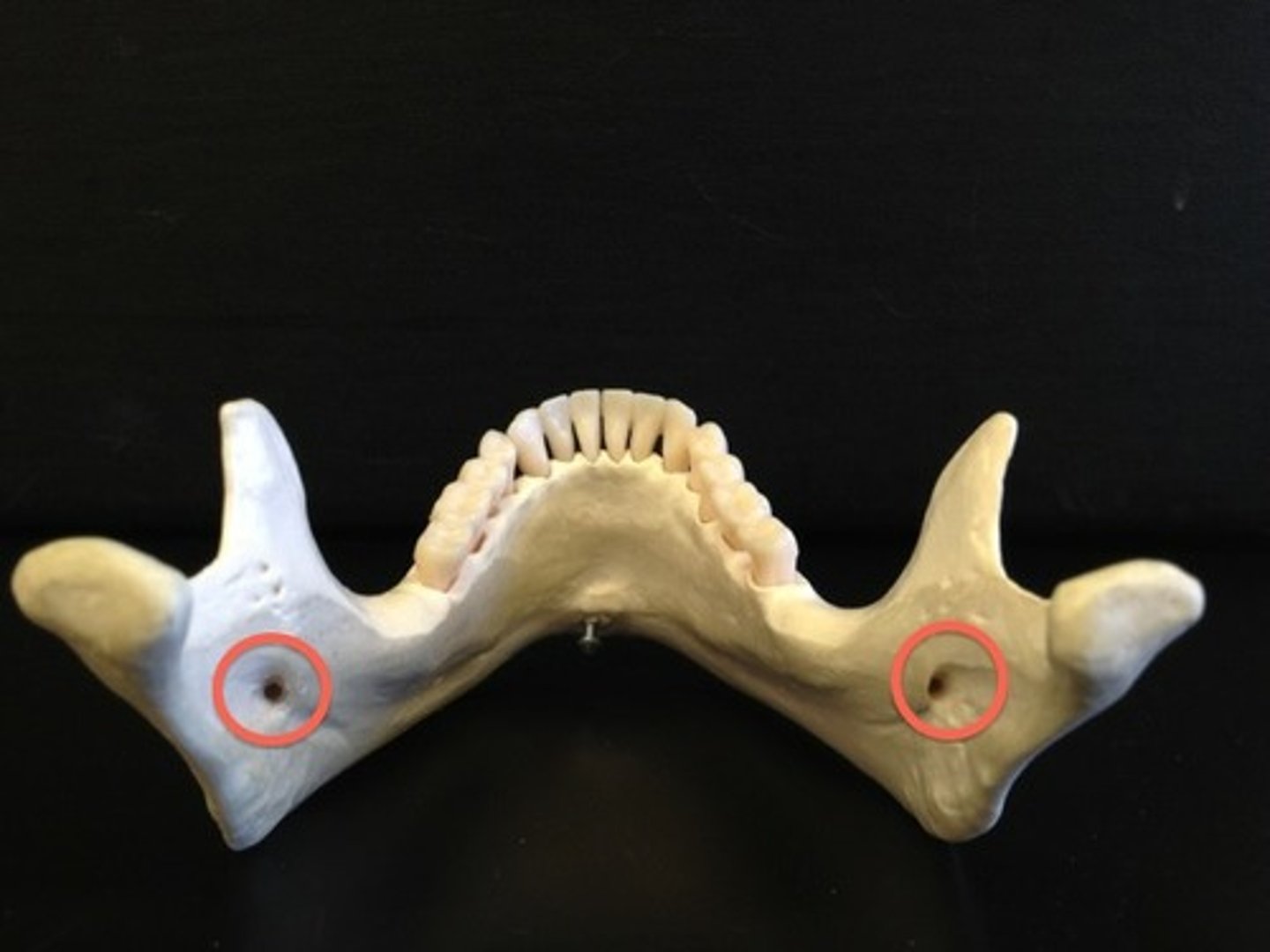
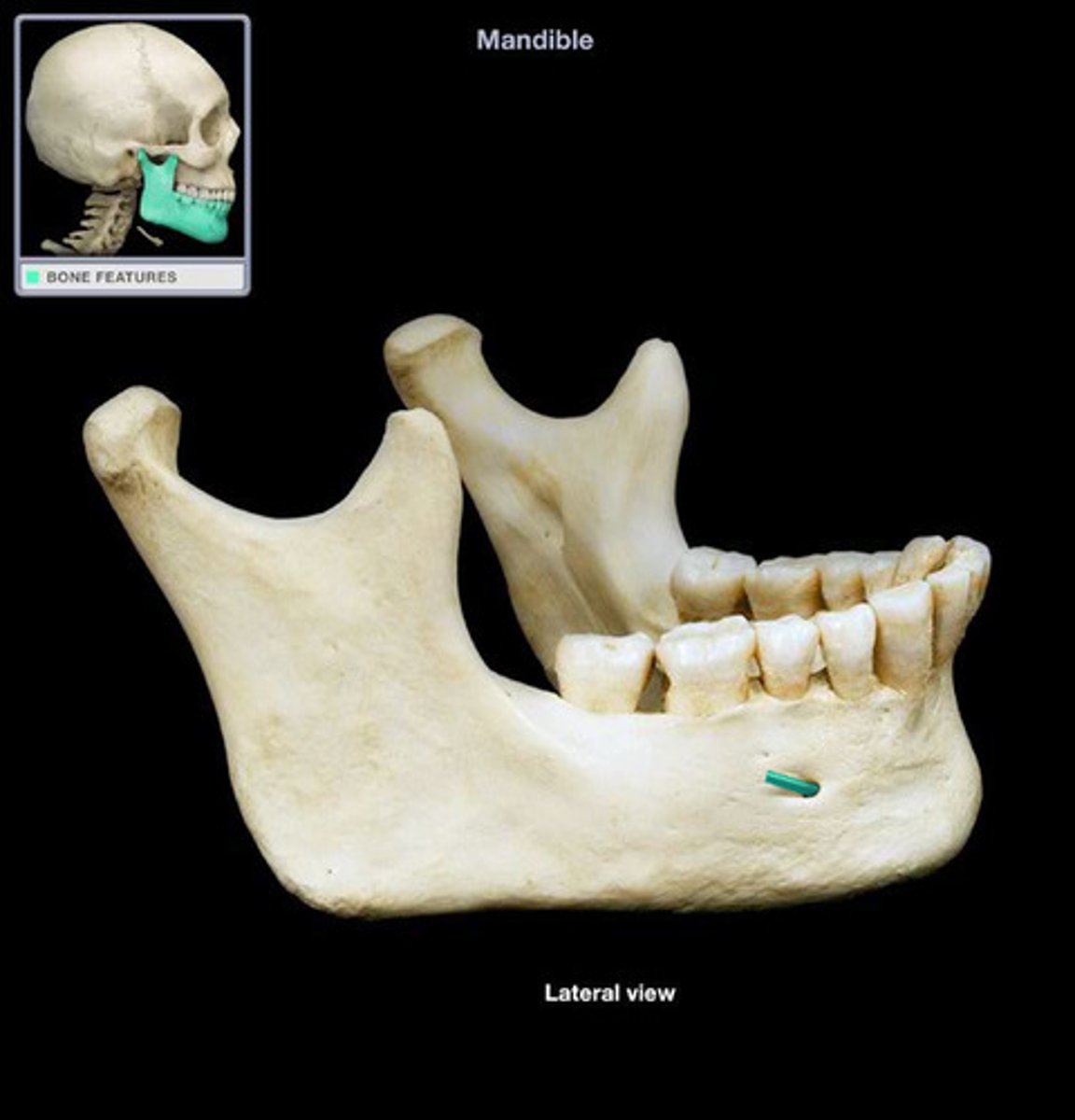
Where is the mental foramen located?
mandible
• facial surface between apices of 1st & 2nd premolars
Where is the incisive foramen located?
maxilla
• where incisive papilla is
