Microscopic Examination Part 1
1/95
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
96 Terms
What is the main purpose of doing a microscopic examination of urine?
To identify and semi-quantitate formed elements in the urine.
What types of formed elements are identified during a microscopic exam?
Cells (RBC, WBC, epithelial), casts, crystals, bacteria/yeast/parasites, mucus, sperm, and artifact.
Do all labs perform a microscopic exam on every urine specimen?
No — some labs do microscopics on all urines, but many do a macroscopic (dipstick/chemical) screening first to increase cost effectiveness.
What factors determine whether a specimen gets a microscopic exam?
It depends on the hospital's criteria, including dipstick results and the patient populations.
Why is standardization important when performing a microscopic exam?
Because specimen preparation steps (mixing, volume, centrifuge speed/time, decanting, sediment volume, and slide method— need to have the same every time) must be consistent for reliable results.
What are the key standardized steps in specimen preparation for a microscopic exam?
The urine must be well mixed, a standard volume is used, centrifuge speed/time is set (400 RCF for 5 minutes), a set supernatant volume is decanted, a set sediment volume is examined, and a slide/coverslip or commercial system is used.
What does RCF stand for?
Relative Centrifugal Force.
Why might RCF differ between centrifuges even at the same RPM?
Because RCF depends on the radius of the centrifuge head, so RCF differs from RPM and varies by centrifuge.
What is the formula for calculating RCF?
RCF = 1.118 x 10⁻⁵ x radius of centrifuge head (cm) x RPM²
In this lab's procedure, how much urine is poured into a conical tube, and what should be noted if the total volume is less than this?
12 ml is poured into a conical tube; note if the total volume is less than 10 ml.
At what speed and for how long is the sample centrifuged in this procedure?
Centrifuge for 5 minutes at 400 RCF.
How should the supernatant be decanted, and how much should be left behind?
Decant the supernatant carefully so as not to disturb the sediment, leaving 1 ml behind.
What are the final steps after decanting in this procedure?
Gently resuspend the sediment, then place it on a slide.
How many fields should be scanned on low power, and what objective is used?
At least 10 fields should be scanned on low power, using the 10x objective.
What should you look for when scanning on low power, and what part of the slide should be scanned?
Look for casts and the general composition of the sample, and be sure to scan the edges and middle, and all the way through.
How many fields should be scanned on high power, what objective is used, and what is being assessed?
At least 10 fields should be scanned on high power, using the 40x objective. It assesses qualitatively or semi-quantitatively (ballpark) WBCs, RBCs, epithelial cells, crystals, etc.
How are microscopic urinalysis results typically reported?
Each lab will have its own standardized reporting format.
What should microscopic results be correlated with?
The physical and chemical findings of the urinalysis.
What are the three types of microscopy used for urine sediment examination?
Bright Field (most common from a regular microscope), Phase Contrast, and Polarizing. (all three could be on a single microscope)
How do objects appear under bright field microscopy?
Objects appear dark on a light background.
What kind of light does a bright field microscope use?
A light source that emits light in the visible wavelength.
What is a limitation of bright field microscopy, and how can it be addressed?
Many elements with a lower refractive index are hard to see; this can be addressed by decreasing the light (in order to see certain cells).
How commonly is bright field microscopy used for urinalysis?
It is used routinely.
How do objects appear under phase contrast microscopy?
Objects appear dark and more 3D on a darker background.
What is "phase difference" in phase contrast microscopy?
Light rays that pass through the object are slowed compared to rays that pass through the air.
How does phase contrast microscopy produce contrast?
Decreased light intensity produces the contrast.
For what is phase contrast microscopy especially helpful?
It is helpful for viewing casts.
What is a polarizing microscope?
A bright field scope fitted with polarizing filters.
How does light behave after passing through the first polarizing filter?
Light emerging from the first filter vibrates in one plane.
What does the second filter (set at 90°) do, and what can pass through it?
It blocks incoming light except for light that has been rotated by birefringent substances.
What does "birefringent" mean?
The ability to refract light in two dimensions at 90° to each other.
What happens visually when objects that polarize light are viewed, and what is polarization especially useful for?
Such objects produce characteristic colors and patterns; polarization is especially good for identifying lipids and crystals.
What happens if an object viewed under polarization is not birefringent?
No light reaches the second filter, so the object appears dark.
Why might urine sediment be hard to see on bright field, and how can visibility be improved?
Sediment may be hard to see on bright field; changing the refractive index (using stains) may increase the visibility of some objects.
What is the Sternheimer-Malbin stain composed of, and what is it used for?
It is composed of crystal violet and safranin O (with different commercial configurations) and is used to enhance visibility of urine sediment.
What lipid stains are used to enhance urine sediment, and what does Hansel stain identify?
Lipid stains include Oil Red O and Sudan III; the Hansel stain (not very common) is used to identify eosinophils.
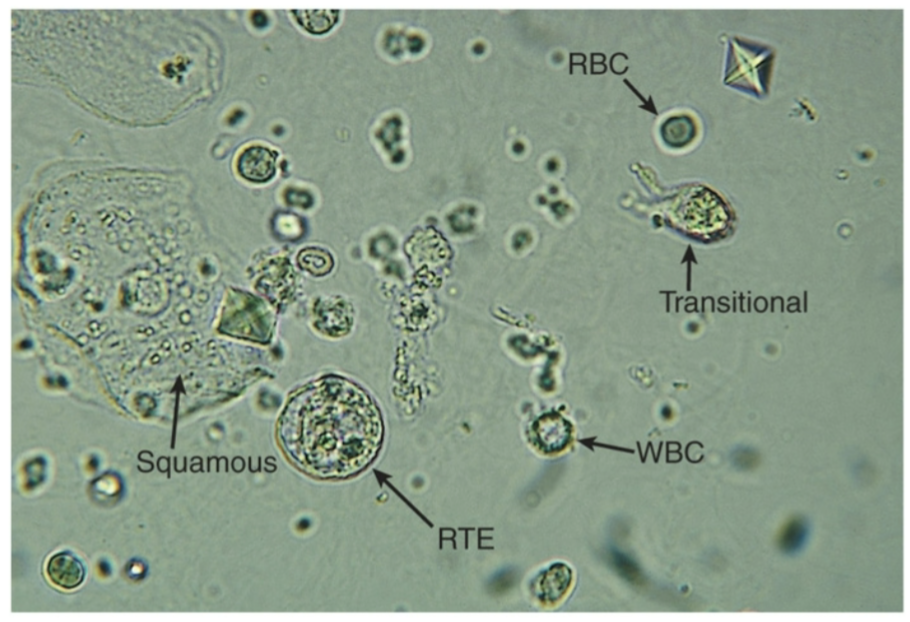
Describe the appearance and size of red blood cells in urine.
Smooth, biconcave discs, approximately 7 µm (microns) in size, with no nucleus.
At what magnification are RBCs identified, and how are they reported?
They are identified at 40x (all cells are found on 40x) and reported as the average number per high power field (#/HPF).
What is considered a normal number of RBCs per HPF?
0-5/HPF is normal.
What are some nonpathologic causes of RBCs in urine?
Exercise, contamination (e.g., menstrual contamination).
What pathologic process can cause RBCs in urine, and how does it differ between early and advanced stages?
Damage to the glomerular membrane (RBCs not filtered out)— early stages cause microscopic hematuria, while advanced stages cause macroscopic (visible) hematuria (gives a red tinge from blood in urine).
What types of injury in the genitourinary (GU) tract can cause RBCs in urine?
Calculi, trauma, UTI, acute infection, and coagulation disorders.
What is a "crenated RBC"?
A red blood cell with a shrunken, scalloped/spiky appearance, as can be seen in urine sediment.
Describe the appearance and size of white blood cells in urine.
Granular, round cells approximately 12 µm in size (bigger than RBC); a single or multi-lobed nucleus may be visible.
What type of WBC predominates in urine sediment, at what magnification are they identified, and how are they reported?
Predominantly neutrophils; identified at 40x and reported as the average number per HPF. (also report as just WBC, not what kind)
What are "Glitter Cells," what causes them, and how are they reported?
WBCs seen in hypotonic urine that have a sparkling appearance of granules due to Brownian motion (movement within cells); they are simply reported as WBCs.
What is considered a normal number of WBCs per HPF, and in which population may it be higher?
0-5/HPF is normal; it may be higher in females.
What types of conditions/causes can lead to increased WBCs in urine?
Glomerular damage, trauma, (most often)—infections (bacterial, yeast, parasitic), and inflammation/other causes.
What specific inflammatory or other conditions are associated with increased WBCs?
SLE (systemic lupus erythematosus), glomerulonephritis, interstitial nephritis, and tumors.
What are the three major types of epithelial cells found in urine?
Squamous, Transitional (urothelial), and Renal Tubular. (last 2 are in the urinary tract)
Describe the appearance of squamous epithelial cells.
They are big, with abundant irregular cytoplasm and a prominent nucleus.
Why can squamous epithelial cells be problematic in a urine specimen, and how can their numbers be decreased?
They may obscure other elements (blocking other cells); CCMS (clean-catch midstream) specimens help decrease the numbers seen.
How are squamous epithelial cells reported?
They are identified and quantified per HPF.
Where are squamous epithelial cells normally expected to come from?
The vagina, the female urethra, or the lower portion of the male urethra (sloughed off, old cells).
What does it mean if squamous epithelial cells are present in large numbers?
They are considered contaminants when present in large numbers. Sample may need to be recollected because of this
What are "Clue cells," what may they indicate, and where are they typically reported from?
Clue cells are squamous epithelial cells covered with Gardnerella vaginalis (bacteria), which may indicate a vaginal infection; they are usually reported from vaginal wet preps, although they may be present in urine.
Where are transitional (urothelial) epithelial cells normally found?
They are the normal lining cells of the urinary tract: the renal pelvis, calyces, ureters, bladder, and the upper male urethra (because theirs are shorter).
Describe the shape and nucleus of transitional epithelial cells.
They can be spherical, polyhedral, or caudate (shape depends on their ability to absorb water), with a distinct, centrally-located nucleus; they are smaller than squamous cells. (need to know how to spot to see they are different than squamous)
How are transitional epithelials reported, and what is the normal range?
They are identified and quantified per HPF; 0-5/HPF is normal.
How can spherical transitional epithelials be distinguished from RTEs?
Transitional epithelials have a central nucleus, whereas RTEs do not, helping distinguish the two even though they may look similar.
When might increased numbers of transitional epithelial cells be seen? (clumped together aswell)
After invasive procedures. (ex: cathederalization)
What should be done if vacuoles or irregular nuclei are present in transitional epithelial cells, and what might this indicate?
The sample should be evaluated by a pathologist or sent to cytology (per facility protocol); this may indicate malignancy or viral infection.
How does the appearance of RTEs vary, and what do larger, rectangular, coarsely granulated columnar cells originate from?
RTE appearance varies based on origin(proximal, distal, or collecting duct); larger, rectangular, coarsely granulated columnar cells originate from the PCT (proximal convoluted tubule).
Why are RTEs important to check for when testing urine?
Because they come from the kidneys
What do finely granulated, irregular cuboidal cells with a straight edge originate from, and what do smaller, round or oval cells originate from?
Finely granulated, irregular cuboidal cells with a straight edge come from the collecting duct; smaller, round or oval cells come from the DCT (distal convoluted tubule).
What features of the RTE nucleus and cell contents can help identify them?
The nucleus is usually eccentric, and the cell may contain reabsorbed material such as bilirubin, hemoglobin/hemosiderin, or fat.
How are RTEs reported, and what is the normal range?
They are identified and quantitated per HPF; 0-3/HPF is normal.
Among epithelial cells, which type is most clinically significant, and what can it be indicative of?
Renal Tubular Epithelial (RTE) cells are the most clinically significant of all epithelial cells; they can be indicative of tubular necrosis and questionable overall renal function.
How to spot RTEs in urine sample?
Their nucleus will be prominant
What conditions or causes are associated with increased RTEs?
Toxins, pyelonephritis, malignancy, transplant rejection, and others.
What are "Renal Fragments," and what may they indicate?
Finely granulated cuboidal cells appearing in groups of 3 or more; they may indicate severe damage.
Comparison of Epithelial Cells
What are Oval Fat Bodies?
RTEs that contain lipids absorbed from the glomerular filtrate.
How are Oval Fat Bodies reported, and how significant is their presence?
They are quantitated per HPF and are NEVER NORMAL so VERY significiant
How can the presence of Oval Fat Bodies be confirmed, and what pattern does cholesterol show under polarization?
Confirm with a fat stain or polarization; cholesterol shows a "Maltese Cross" formation under polarization and is very refractile upon focusing.
Besides Oval Fat Bodies, what else may be present and what is its appearance?
Free floating fat droplets may also be present.
What is lipiduria frequently associated with?
Glomerular damage, including nephrotic syndrome, tubular necrosis, and diabetes mellitus (DM).
What is nephrotic syndrome?
A problem with the electrical charge within the kidneys that allows lipids to pass through
How clinically significant is the presence of any fat in urine?
The presence of any fat is clinically significant.
Is bacteria normally present in urine, and how is it typically introduced?
Bacteria is not normally present; it is usually a contaminant from vaginal, urethral, or container sources.
When is bacteria in urine indicative of infection, and at what magnification is it observed?
Bacteria is indicative of infection when accompanied by WBCs (unless the patient is immunocompromised); it is observed on 40x.
What is vaginal flora?
Mostly in women and usually found within woman’s samples but may be some in males
In which patient populations may yeast be seen in urine?
Diabetics, immunocompromised patients, and patients with vaginal yeast infections.
What can yeast be confused with, and what feature helps distinguish it?
Yeast may be confused with RBCs; look for budding to distinguish it.
At what magnification is yeast noted?
40x.
What is the most frequent parasite found in urine?
Trichomonas vaginalis.
Why will we not see Trichomonas vaginalis in our lab?
Because they dont like being kept in the cold/refridgerator
Describe the appearance of Trichomonas vaginalis.
A pear-shaped trophozoite with flagella and an undulating membrane.
When is Trichomonas vaginalis easy to identify, and what can dead or nonmotile forms be confused with?
It is easy to identify when motile; dead or nonmotile Trichomonas may be confused with WBCs or epithelial cells.
At what magnification is Trichomonas vaginalis noted?
40x.
What is Enterobius vermicularis, how does it get into urine, and what do its eggs look like?
Enterobius vermicularis (pinworm) is a fecal contaminant; its eggs appear oval with a flattened side.
What is Schistosoma haematobium, what do its eggs look like, and how common is it in the US?
It is a bladder parasite whose eggs appear large and oval with a pointed end; it is not common in the US.
Are sperm found in urine typically motile, and what is their general clinical significance?
Sperm found in urine are nonmotile and usually have little clinical significance.
How is the reporting of sperm in urine typically handled?
Follow lab policy for reporting — some labs report sperm while others do not.
What produces mucus in urine, and what is its major constituent?
Mucus is composed of proteins produced by epithelial cells of the lower genitourinary tract and by RTEs; its major constituent is Tamm-Horsfall protein (uromodulin).
In whom is mucus more commonly seen, what does it look like, and what is its clinical significance?
Mucus is more common in women, appears as threadlike structures in irregular patterns, and has no clinical significance