ANHB2212 - Digestive System Development
1/106
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
107 Terms
Histogenesis
formation of different tissues from undifferentiated cells
All body cavities include these 2 things
mesothelium lining
parietal and visceral regions
Mesothelium
Single layer of squamous epithelium that produces serous fluid to facilitate low friction movement of organs
What are the embryological origins of the parietal and visceral peritoneum?
parietal = somatic lateral plate mesoderm
visceral = splanchnic lateral plate mesoderm
What does the celiac trunk supply?
foregut organs
What does the superior mesenteric artery supply?
midgut organs
What does the inferior mesenteric artery supply?
hindgut organs
What 8 organs are foregut derivatives?
• Stomach
• Liver
• Gall bladder
• Pancreas
• Proximal duodenum
Abdominal esophagus
proximal ½ duodenum
Spleen
What 8 organs are derivatives of the midgut?
• Distal ½ duodenum
• Pancreas
• Jejunum
• Ileum
• Caecum
• Appendix
• Ascending colon
• Transverse colon (proximal 2/3)
What 4 organs are hindgut derivatives?
• Transverse colon (distal 1/3)
• Descending colon
• Sigmoid colon
• Anorectal canal (proximal 2/3)
What is the main arterial supply of the foregut organs?
Splenic a.
Left gastric a.
Common hepatic a.
What are the main arterial supply for the midgut organs?
Ileocolic a.
Right colic a.
Middle colic a.
What are the main arterial supply for the hindgut organs?
Left colic a.
Sigmoidal branches
Superior rectal a.
What is the main motor nerve supply for the foregut, midgut and hindgut?
foregut and midgut = vagus nerve
hindgut = Pelvic splanchnic nerves (S2-S4)
Peritoneum
continuous serous membrane lining the inner surface of the abdominal cavity
Mesentery
folds (reflections) of peritoneum that attach viscera to the body wall (ventral & dorsal)
Formation of the dorsal mesentery
Initially, primitive gut tube hangs from the posterior body wall by a broad bar of mesenchyme
Inferior to the septum transversum, the connection thins forming a membranous dorsal mesentery (= reflected peritoneum) extending from abdominal esophagus to rectum as a continuous sheet
What is the function of mesenteries?
mobility of organs
passage for blood vessels and nerves
Mesogastrium
relates to foregut structures
The Mesentery
suspends parts of the small intestine
Mesocolon
suspends parts of the colon
What does ventral mesentery suspend?
foregut organs
What is ventral mesentery derived from?
mesoderm of the septum transversum
What are the 3 ventral mesenteries?
falciform ligament
lesser omentum
triangular ligaments
What does the dorsal mesentery suspend?
foregut, midgut and hindgut organs
What 4 foregut mesenteries are part of the dorsal mesentery?
gastrosplenic ligament
splenorenal ligament
gastrocolic ligament
greater omentum
What 4 midgut mesenteries are part of the dorsal mesentery?
The Mesentery (Mesointestine)
Mesoduodenum
Mesoappendix
Transverse mesocolon
What hindgut mesentery is part of the dorsal mesentery?
sigmoid mesocolon
Falciform ligament
between liver & ventral body wall
Lesser omentum
between liver & stomach & between liver & duodenum
Triangular ligaments
between liver & diaphragm
Gastrosplenic ligament
between stomach & spleen
Splenorenal ligament
between spleen & kidney
Gastrocolic ligament
between stomach & colon
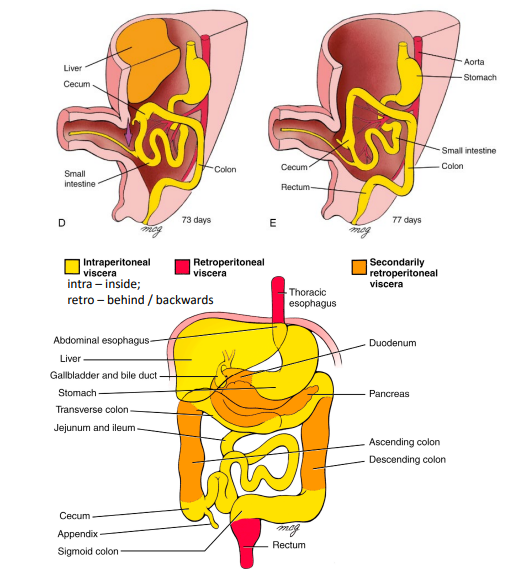
What differentiates the intraperitoneal organs, primary retroperitoneal organs and secondary retroperitoneal organs?
Intraperitoneal organs – have a mesentery and are inside the peritoneal folds
Primary retroperitoneal organs – never had a mesentery and are behind the peritoneal
Secondary retroperitoneal organs – lose their mesentery during development
What are the 10 intraperitoneal organs?
Stomach
Appendix
Liver
Transverse colon
Duodenum (first/superior part only)
Small intestines (jejunum and ileum)
Pancreas (only the tail)
Rectum (upper third)
Spleen
Sigmoid colon
What are the 5 primary retroperitoneal organs?
thoracic esophagus
rectum
kidneys
adrenal glands
bladder
What are the 4 secondary retroperitoneal organs?
duodenum
pancreas
ascending colon
descending colon
Peritoneal Zygosis
During development, secondary retroperitoneal organs get pressed against the posterior body wall
Causes adhesion of the dorsal mesentery to the peritoneum of the dorsal body wall
Results in “retro-peritonealisation” of the affected parts of the developing gut
What supplies the intraperitoneal and secondary retroperitoneal organs?
unpaired arteries of the vitelline system
When do the two muscle layers of the esophagus develop?
Inner circular layer – early week 5
Outer longitudinal layer – week 8
How is muscle development of the esophagus induced?
by gut endoderm
Describe the muscle of the adult esophagus
cranial (Adult ~ 2-4cm) = skeletal m.
caudal (Adult ~ 11cms) = smooth m.
middle = transitional mixed zone
What is the smooth and skeletal muscle of the esophagus derived from?
Smooth m. - splanchnic mesoderm of the gut
Skeletal m. - cranial paraxial mesoderm
How is the stomach attached to the body wall?
ventral mesentery (mesogastrium; lesser omentum) and dorsal mesentery (mesogastrium)
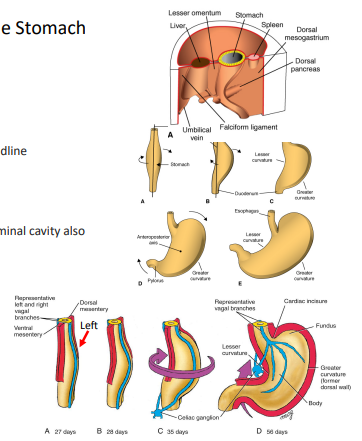
Development of the Stomach
Developing stomach becomes fusiform in shape
The cranial and caudal ends of the stomach originally lie in the body’s midline
There is a 90 degree clockwise rotation around the stomach’s longitudinal axis
This causes the left side to face ventrally & right side to face dorsally
The vagus nerves, which have travelled via the espohagus into the abdominal cavity also change position (left vagus faces ventrally; right vagus faces dorsally)
As this longitudinal rotation occurs, the stomach also starts to rotate around a ventro-dorsal axis
This causes the cranial (cardiac) part to shift slightly downward and to the left and the caudal (pyloric) part of the stomach to shift upward and right
Differential growth of the stomach during rotations gives rise to lesser curvature (pre-rotation = ventral surface - grows slower) and greater curvature (pre-rotation = dorsal surface - grows faster)
How are the greater and lesser omentum supplied?
coeliac truck derived arteries (greater omentum = left & right gastroepiploic arteries)
What are the 3 functions of the greater omentum?
Fat deposition
Immune function (areas called milky spots house macrophages & lymphocytes)
Infection and wound isolation - may isolate areas of infection and trauma (wraps around)
How does the greater omentum function in large mammals?
In large mammals the greater omentum may act as a sling around abdominal organs – helps to prevents twisting & reduce friction during movement
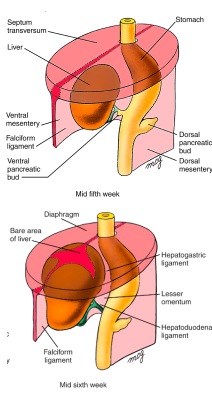
Development of the Liver
The hepatic diverticulum arises as a ventral endodermal outgrowth from caudal part of the foregut (future duodenum)
All gut tube endoderm has the potential to form liver cells but this is repressed by inhibitors secreted by mesoderm, ectoderm, and the notochord
Liver development begins in the septum transversum due to signalling pathways between septum transversum & cardiac mesoderm
Liver cells colonise the septum transversum
Subsequent growth causes the liver to bulge caudally into the abdominal cavity
Liver develops within ventral mesentery
As the liver grows, the ventral mesentery becomes membranous and divided into 2 parts: Falciform ligament and Lesser omentum
Mesoderm on the liver’s surface differentiates into visceral peritoneum
As the liver grows the cranial surface of the liver comes in contact with the diaphragm
This results in a bare area between the liver and diaphragm where there is no peritoneum
At the borders of the bare area the peritoneum folds from diaphragm to liver that creates the ventral and dorsal coronary ligaments (peritoneal reflections)
These meet on the right and left sides of the bare area to form the triangular ligaments
What contains the umbilical vein?
Caudal edge of the falciform ligament contains the umbilical vein
How much body weight does the liver take up at week 10?
By week 10 of development, liver ~ 10% of the total body weight
How much body weight does the liver take up at at birth?
At birth liver ~ 5% of total body weight
What are the 2 functions of the liver?
liver is large in utero due to its hematopoietic function (blood formation) where there are large areas between hepatic cells and blood vessels walls which produce red and white blood cells until week 8
bile secretion to emulsify fat
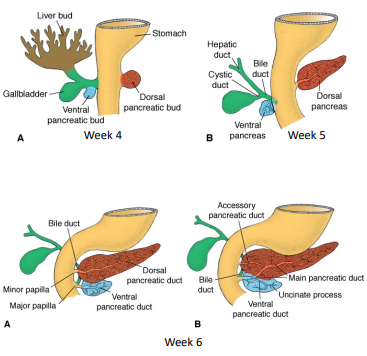
Gall Bladder Development
As liver develops into the septum transversum, the biliary duct system forms
Where the connection between the hepatic diverticulum and the foregut (duodenum) narrows = the bile duct
A small ventral outgrowth develops in the bile duct = gallbladder and cystic duct
Positional change of the developing duodenum (partly due to stomach development) causes the bile duct entrance to pass behind the duodenum
When does the liver start producing bile?
week 12
What is the passage of bile?
gall bladder
hepatic + cystic ducts
bile duct
gastrointestinal tract (duodenum)
Meconium
Baby’s first stool that is dark green due to cells, protein, fats, intestinal secretions and bile
Pancreas Development
The pancreas forms from two buds arising from duodenal endoderm: Ventral bud – close to the gall bladder (ventral mesentery) Dorsal bud – dorsal mesentery
Splanchnic mesoderm gives rise to pancreatic connective tissue
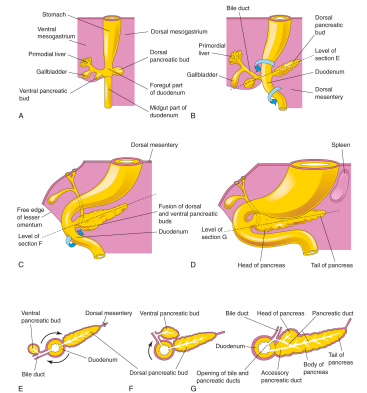
Growth pattern of the stomach causes the duodenum to rotate to the right and become C-shaped
Change in duodenum position causes the ventral pancreatic bud to move dorsally (similar to the bile duct entrance position change)
Ventral bud is brought immediately below and behind the dorsal bud
The two buds fuse: ventral bud = inferior part of the pancreas head; dorsal bud = remainder
Rapid stomach growth & consequent rotation of the duodenum causes pancreas & most of the duodenum to become retroperitoneal
Duct system of the 2 buds fuse (distal dorsal pancreatic duct + ventral pancreatic duct) form main pancreatic duct
Proximal part of the dorsal pancreatic duct usually disappears but may persist as the accessory pancreatic duct
Main pancreatic duct + bile duct enters the duodenum at the major papilla and accessory duct associated with minor papilla
What forms the foregut-midgut boundary?
major papilla
What supplies the pancreas?
branches of coeliac trunk + superior mesenteric a
What is the function of the pancreas?
Digestive function = secretion of enzymes for breakdown of fats & carbohydrates
Pancreatic islets (glucose regulation) = secrete Insulin and Glucagon start to develop in month 3 - distributed throughout the pancreas
When does insulin secretion begin?
Insulin secretion begins ~ month 5 of development
Function of the spleen
• contains infection-fighting white blood cells
• controls the level of blood cells (WBCs, RBCs and platelets)
• filters the blood and removes any old or damaged RBCs
Development of the spleen
Spleen primordium appears in week 5 in the dorsal mesogastrium
Stomach rotation and rapid growth causes dorsal mesogastrium lengthening
Dorsal mesogastrium between spleen and dorsal midline swings left causing the spleen to connect to : the posterior body wall near the left kidney (= splenorenal ligament) the stomach (= gastrosplenic ligament)
What supplies the spleen?
the splenic artery – arises from the coeliac trunk
How is the midgut suspended?
Week 5 - midgut is suspended from the dorsal abdominal wall by a short mesentery
Development of the small intestine
A cecal primordium develops distinguishing the future ileum from future colon
Developing ileum elongates more rapidly than the abdominal cavity
Midgut develops the primary intestinal loop
Cranial arm of loop becomes most of the ileum
Caudal arm of loop becomes ascending and transverse colon
Apex of the loop is attached to the umbilicus by the vitelline duct & superior mesenteric artery = axis of the loop
Week 6 – abdominal cavity becomes too small to contain all of the intestinal loops (partly due to rapid expansion of the liver)
Pressure from rapidly developing abdominal organs, especially liver, forces the intestinal loop into the extraembryonic cavity of the umbilical cord = midgut herniation
As the primary intestinal loop herniates it rotates around the axis of the superior mesenteric artery by 90 degrees
Cranial arm of loop moves to embryo’s right side & caudal arm moves left This first rotation is complete by early week 8
The gut continues to differentiate: lengthening jejunum and ileum form folds called jejunal-ileal loops and cecum expands and develops the worm-like vermiform appendix
In week 10 the midgut herniation rapidly returns to the abdomen due to increased size of abdominal cavity relative to the other abdominal organs where growth has slowed
As the intestinal loop returns to the abdomen, it rotates by 180 degrees
Cecum ends up just inferior to the liver near the right iliac crest
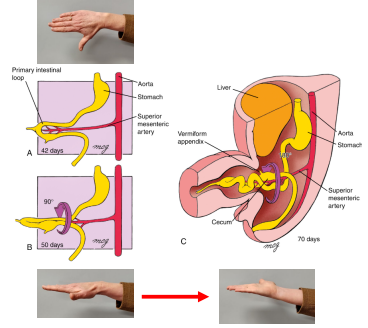
What is the total rotation of the intestinal loop?
Total rotation of intestinal loop is 270o = 90 degrees (Weeks 6-8) + 180 degrees (week 10)
When do all intestines return to the abdominal cavity?
week 11
What supplies the large intestine?
Supplied by both superior & inferior mesenteric arteries
Development of the large intestine
After the large intestine returns to the abdominal cavity, it continues to lengthen & cecum moves in a caudal direction
The dorsal mesenteries of the ascending and descending colon shorten and fold. This causes: ascending & descending colon to press against the dorsal body wall and they start to adhere to the dorsal body wall and their mesentery gradually disappears due to zygosis
Ascending & descending colon = secondarily retroperitoneal
Transverse & sigmoid colon remain intraperitoneal (suspended by mesentery)
Cloaca
The cloaca is an endoderm-lined cavity covered by the cloacal membrane = endoderm & ectoderm (no mesoderm)
Development of the rectum
Between weeks 4-6 the cloaca is partitioned into a dorsal anorectal canal & ventral urogenital sinus due to the formation of a coronal partition of mesoderm - the urorectal septum
As caudal folding continues & the embryo grows, the urorectal septum moves closer to the cloacal membrane
cloacal membrane ruptures creating an anal opening for the hindgut (anorectal orifice) & a ventral opening for the urogenital sinus.
Between the two openings, the tip of the urorectal septum forms the perineal body
After the anorectal orifice forms, mesenchyme surrounding the anal canal proliferates
This mesenchyme forms a raised border adjacent to the anal opening = anal pit
Describe the development of the definitive anorectal canal
Cranial two-thirds of the definitive anorectal canal develops from distal hindgut - lined with endodermally derived epithelium
Caudal third of the definitive anorectal canal from the anal pit - lined with ectodermally derived epithelium
Pectinate line
endoderm-ectoderm junction between caudal third and cranial two thirds of the definitive anorectal canal made of mucosal folds
Blood supply above pectinate line
branches of the inferior mesenteric arteries & veins (hindgut)
Blood supply below the pectinate line
branches of the internal iliac arteries & veins
Name the bones and cartilages that form the margins of the abdomen
Lower ribs, costal margin, xiphoid process, lumbar vertebrae, upper & anterior pelvis
Name the parts of the pelvic brim, which represents the junction between the abdominal and pelvic cavities.
Sacral promontory and alae, arcuate line, superior pubic ramus & pubic symphysis
Aponeuroses
sheets of dense regular connective tissue that exhibit an ordered arrangement of collagen fibres that take the place of a tendon in flat muscles that have a wide area of attachment. An ordered arrangement of connective tissue fibres in the same direction confers a high tensile strength in that direction. The trade-off is that a single flat abdominal muscle and its aponeurosis are vulnerable to
tensional or shear forces in other directions. Therefore, layering of abdominal muscles and aponeuroses with fibres arranged in different directions is critical to the mobility, strength and integrity of the abdominal wall.
Tensile strength
the maximum amount of stress a material can cope with before it breaks or ruptures.
The Rectus Sheath
The rectus abdominis muscle is surrounded by the tendinous rectus sheath, which is derived from the aponeuroses of the muscles on either side of it: the oblique muscles and transversus abdominis. The rectus sheath completely encloses the upper three-quarters of the rectus abdominis muscle. Anteriorly in this region, the rectus sheath consists of the aponeurosis of the external oblique and half of the aponeurosis of the internal oblique, which splits at the lateral margin of the rectus abdominis. Posteriorly in this region, the rectus sheath consists of the other half of the aponeurosis of the internal oblique and the aponeurosis of the transversus abdominis
Describe the direction of the rectus abdominis muscle
verticle
Describe the direction of the external oblique muscle
angling downwards and towards the midline (think “hands in pockets”, where the
forearm aligns with the muscle fibers in an inferomedial direction)
Describe the direction of the internal oblique muscle
angling upwards and towards the midline (think “hands on tits” (sorry!), where the forearm aligns with muscle fibers in a superomedial direction)
Describe the direction of the transversus abdominis muscle
horizontal
What function do these abdominal wall muscles perform when you cough?
By contracting during coughing the muscles increase intra-abdominal pressure to help expel air from the lungs when the diaphragm relaxes.
What function do these abdominal wall muscles perform when you defecate?
By contracting during breath holding the muscles increase intra-abdominal pressure to help expel urine, feces (and sometimes babies).
Primary hernias
occur at certain weak spots of the abdominal wall fascia such as the midline (epigastric = linea alba, or umbilical = above or below umbilicus), between rectus abdominis and oblique and transverse abdominal muscles that protrude through linea semilunaris, or in the lumbar region (between quadratus lumborum and oblique and transverse abdominal muscles)
Incisional hernias
The most common types of abdominal wall hernias, however, are incisional hernias. These can occur anywhere there has been an incision, trauma or previous repair of a primary hernia.
Name 2 structures that lie beneath the transversalis fascia.
Extraperitoneal fat & parietal peritoneum
What structure overlays the transversalis fascia?
Transversus abdominis muscle
Where are the origin and insertion points of the inguinal ligament?
Anterior superior iliac spine and pubic tubercle
Identify the major blood vessels and muscles that pass under the inguinal ligament
Femoral artery, vein and nerve, iliacus and psoas major muscles
Name the structures that pass through the inguinal canal in prosections with male and female genitalia
Male = spermatic cord
Female = round ligament of the uterus (ligamentum teres)
Inguinal hernias
An inguinal hernia is the protrusion of a peritoneal sac through a weakened part of the abdominal wall in the groin region. The protrusion may or may not include abdominal contents, such as intestine. Inguinal hernias are classified as either indirect or direct.
Indirect inguinal hernias
Indirect inguinal hernias occur because part or all of the embryonic processus vaginalis remains open (patent), which allows the peritoneal sac to enter the deep inguinal ring. Indirect hernias are, therefore, congenital in origin. They are the most common of the two types of inguinal hernia and present more frequently in assigned males at birth (AMAB) than in assigned females at birth (AFAB).
What does the extent of an indirect inguinal hernia depend on?
The extent of an indirect inguinal hernia depends on the amount of processus vaginalis that remains patent. If the entire processus vaginalis remains patent, the peritoneal sac may exit through the superficial inguinal ring and continue into the scrotum or labium majus (singular for labia majora).
Direct inguinal hernia
A direct inguinal hernia occurs when a peritoneal sac enters the medial end of the inguinal canal due to a weakened posterior abdominal wall. Being acquired in origin, it does not enter the deep inguinal ring. A direct hernia may protrude through the superficial inguinal ring but this is not always the case. Direct inguinal hernias occur most commonly in adult AMAB.