Quiz 2 LOs: Inflammatory/Reactive/Traumatic Oral Lesions
1/139
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
140 Terms
Describe acute inflammation
injury is brief, minimal, and source is removed from the tissue
Describe chronic inflammation
injury to tissue continues and inflammation response is longer lasting
produces more extensive damage and tissue heals slower
What cells are involved in chronic inflammation?
neutrophils, monocytes, and plasma cells to proliferate fibroblasts
What are the local clinical signs of inflammation?
limited to area of injury
redness
swelling
heat
pain
loss of function
What are the systemic clinical signs of inflammation?
injury becomes extensive
fever
leukocytosis
lymphadenopathy
elevated C - reactive protein
What are biochemical mediators involved in inflammation?
chemical in the body that either start or amplify response
chemotactic factors
kinin system
clotting mechanism
complement system
prostaglandins
WBC lysosomal enzymes released from granules or pathogenic m/os
endotoxins
Describe chemotactic factors
biochemical mediators that enhance chemotaxis - the movement of WBC toward the site of injury
Describe kinin system
causes increase dilation of blood vessel at site of injury and increases permeability
can induce pain
When and how is the kinin system activated?
early stages of inflammation
activated by substances present in plasma and in injured tissue
What is the primary kinin?
bradykinin
Describe clotting mechanism
clots blood to stop bleeding at site of injury, important in tissue repair
forms a fibrinous meshwork at site of injury to protect adjacent tissues and keep foreign substances from gathering at the site
certain products can be activated when tissue is injured and activates the kinin system
Describe complement system
series of plasma proteins activated in cascading fashion
functions in inflam and immunity
cause mast cells to release granules from their cytoplasm that contains histamine and other biochemical mediators into surrounding tissue --> causes an increase in vascular permeability and dilation
cause cell death by creating holes in the membrane --> cytolysis
attach to surface of bacteria stimulate WBCs for phagocytosis --> opsonization
Describe prostaglandins
mediating inflam response by increasing vasodilation and permeability, pain, and changes in connective tissue
Describe WBC lysosome enzymes released from granules or pathogenic m/os
act as chemotactic factors
damage CT and clot at site of injury
Describe endotoxins (from gram neg cell wall)
act as chemotactic factors
function as an antigen and damage bone tissue
What WBCs are involved in inflammation?
neutrophils (PNMs)
monocytes (become macrophages)
Describe neutrophils and their primary function
the first WBC recruited to the area of injury in response to chemotactic factors
Compose 70% of the
WBC population
Mobile cells that are produced throughout life
The primary function is phagocytosis of substances such as pathogenic microorganisms and tissue debris (contains lysosomal enzymes)
What are the microscopic characteristics of neutrophils?
has a multilobed nucleus
has a granular cytoplasm containing lysosomal enzymes (destroy substances after cell has engulfed them)
mobile
Describe macrophages and their primary function
Develops from a monocyte, the second responder to the site of injury
Important in phagocytosis and immune response
What are the microscopic characteristics of macrophages?
has a single round nucleus
has a cytoplasm containing lysosomal enzymes (destroy substances after cell has engulfed them) (no granular cytoplasm)
mobile
What has a longer lifespan, macrophage or neutrophil?
macrophage
What is anti inflammatory therapy?
drugs to block or suppress inflammatory response
prevents or reduces clinical signs of inflammation and ADRs of injury
can be steroidal or non
What are some examples of anti inflammatory therapy?
Steroidal: prednisone, inhibit prostaglandin synthesis
Nonsteroidal: NSAIDS, inhibit prostaglandin synthesis
Antihistamines
Drugs used to treat cancer
Describe regeneration
when tissue damage has been slight, the inflamed area may return completely to its normal structure and function
most favorable resolution of acute inflam and involves complete removal of all cells, by products, and inflam exudate
returns microcirculation to its pre inflam state
Describe repair
occurs when complete return of the tissue to normal is not possible bc the damage has been too great
final defense mechanism of the body in its attempt to restore injured tissue to its original state
dead cells are replaced with live cells and new tissue components or nonfunctioning scar tissue
CANNOT BE COMPLETED UNTIL SOURCE OF INJURY IS REMOVED OR INJURIOUS AGENTS ARE DESTROYED
What tissues can undergo repair?
connective tissue, epithelium, bone
NOT ENAMEL
What are the local factors that can impair healing?
bacterial infections - strep or staph strains
tissue destructions / necrosis
hemorrhage into tissue causing a hematoma
excessive movement of injured tissue
poor blood supply
What are the systemic factors that can impair healing?
malnutrition
immunosuppression due to chemotherapy or steroids
genetic disorder
metabolic disorders
tobacco and recreational drug use
Describe the process of bone healing
1. Clot forms
2. Cellular proliferation occurs to convert the clot to granulation tissue
3. Granulation tissue forms a matrix, which allows osteoblasts to lay down immature bone called osteoid
4. Osteoid becomes more calcified over time and the area of tissue damage is replaced by viable bone trabeculae
Describe attrition
wearing away of tooth structure during mastication, creating flattened occlusal, incisal, and interproximal surfaces
a more fibrous diet causes greater attrition
typically greater in MEN than women and in ELDERLY

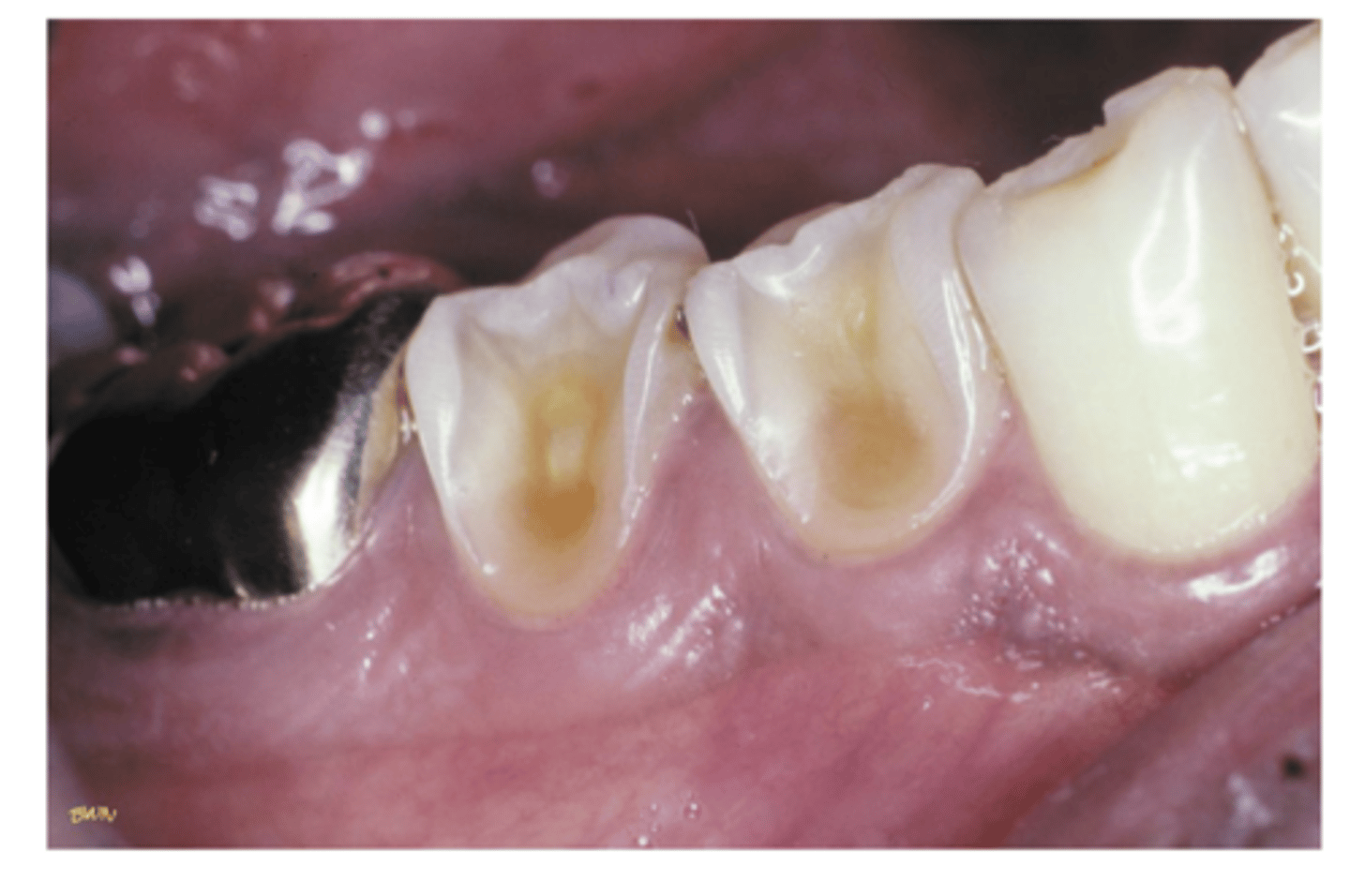
Describe abrasion
wearing away of the tooth structure caused by an repetitive mechanical habit like aggressive toothbrush/flossing or holding sharp things in the mouth
commonly seen on exposed root surfaces where dentin and cementum are exposed
appears as a notching of the root surface in areas of gingival recession
increase risk for hypersensitivity and caries
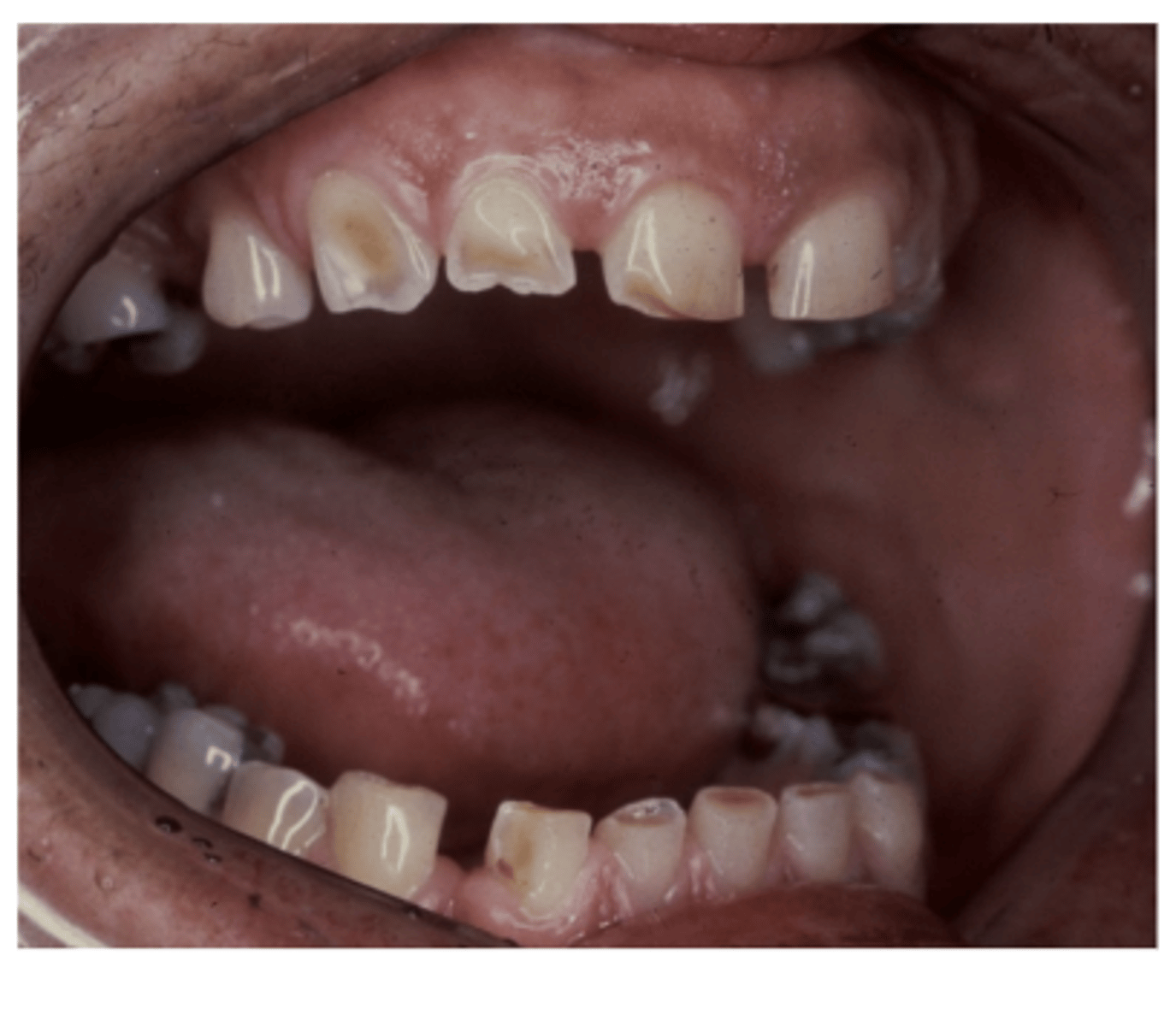
Describe erosion
loss of tooth structure due to chemical actions --> chemicals, acidic food and drink, meds, pools with low ph, gastric secretions, eating disorders, etc
commonly affects facial and lingual surfaces and palate
appears smooth and polished
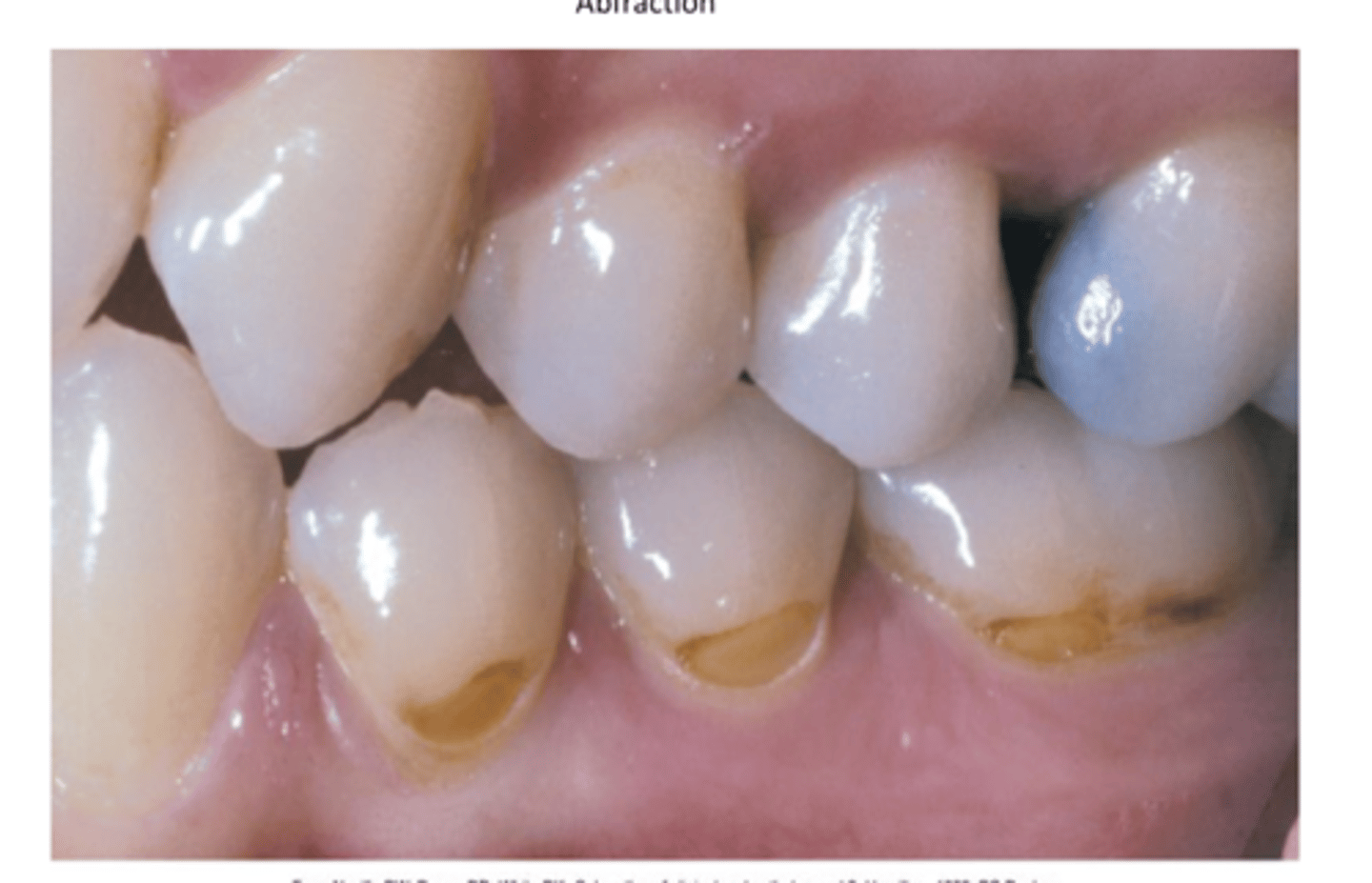
Describe abfraction
affects cervical areas
--> V or wedge-shaped defect, deep and narrow
caused by microfracture to tooth structure in areas of high stress, can be related to fatigue, flexure, fraction, and deformation of tooth structure due to biomechanical forces
Describe bruxism and its symptoms
Grinding of the teeth together for nonfunctional reasons
Triggered by occlusal interferences, stress, and tension
Symptoms include wear on masticatory surfaces, attrition, hypertrophy of masticatory muscles, increase muscle tone and tenderness, cheek biting, jaw pain, etc
Describe internal resorption
can occur in any tooth, usually involves one tooth
associated with an inflammatory response in the pulp
if internal resorption occurs coronally, seen as a pinkish area in the crown
if internal resorption occurs apically, it can only be seen radiographically and appears as a round/oval radiolucent area
Describe external resorption
resorption of the tooth structure beginning at the outside
usually involves root of tooth or crown of an impacted tooth
appears as slight raggedness or blunting of the root apex and can proceed to severe loss of tooth structure
What are the types of oral mucosal burns?
aspirin, phenol and chemical, electric, and thermal
What are the causes of aspirin burns?
chemical burn
aspirin in contact with mucosa for a period of time

What are the clinical and microscopic features of aspirin burns?
painful ulcer with necrotic surface
How can you treat aspirin burns?
palliative
What are the causes phenol and chemical burns?
caustic chemical in contact with mucosa
What are the clinical and microscopic features of phenol and chemical burns?
painful ulcer with necrotizing center
How can you treat phenol and chemical burns?
palliative
What are the causes of electric burns?
live electric cord in contact with mucosa
What are the clinical and microscopic features of electric burns?
tissue destruction
How can you treat electric burns?
tissue repair
What are the cause of thermal burns?
hot food or liquid
How can you treat thermal burns?
runs its course or palliative
What are the clinical and microscopic features of thermal burns?
painful erythema and superficial ulceration
What are the causes of lesions from cocaine use?
cocaine use
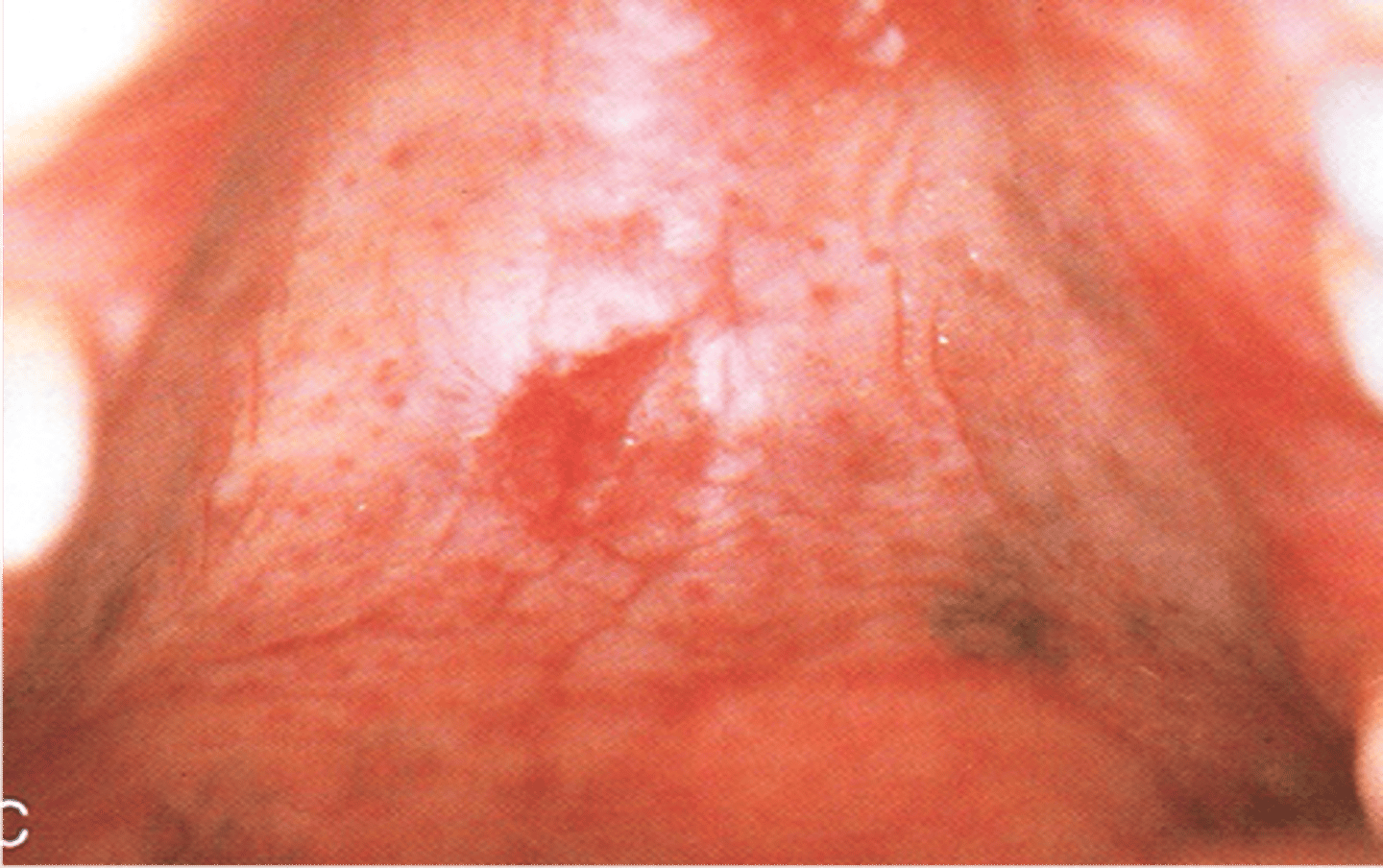
What are the clinical and microscopic features of lesions from cocaine use?
lesions located at midline of hard palate
painful ulceration and erythema, necrotic ulcers, palatal perforation
How can you treat lesions from cocaine use?
elimination of cause
What is the cause of hematomas?
trauma

What are the clinical and microscopic features of hematomas?
red / purple / blue / black mass lesion
How can you treat hematomas?
no treatment
What is the cause of traumatic ulcers?
trauma to mucosa
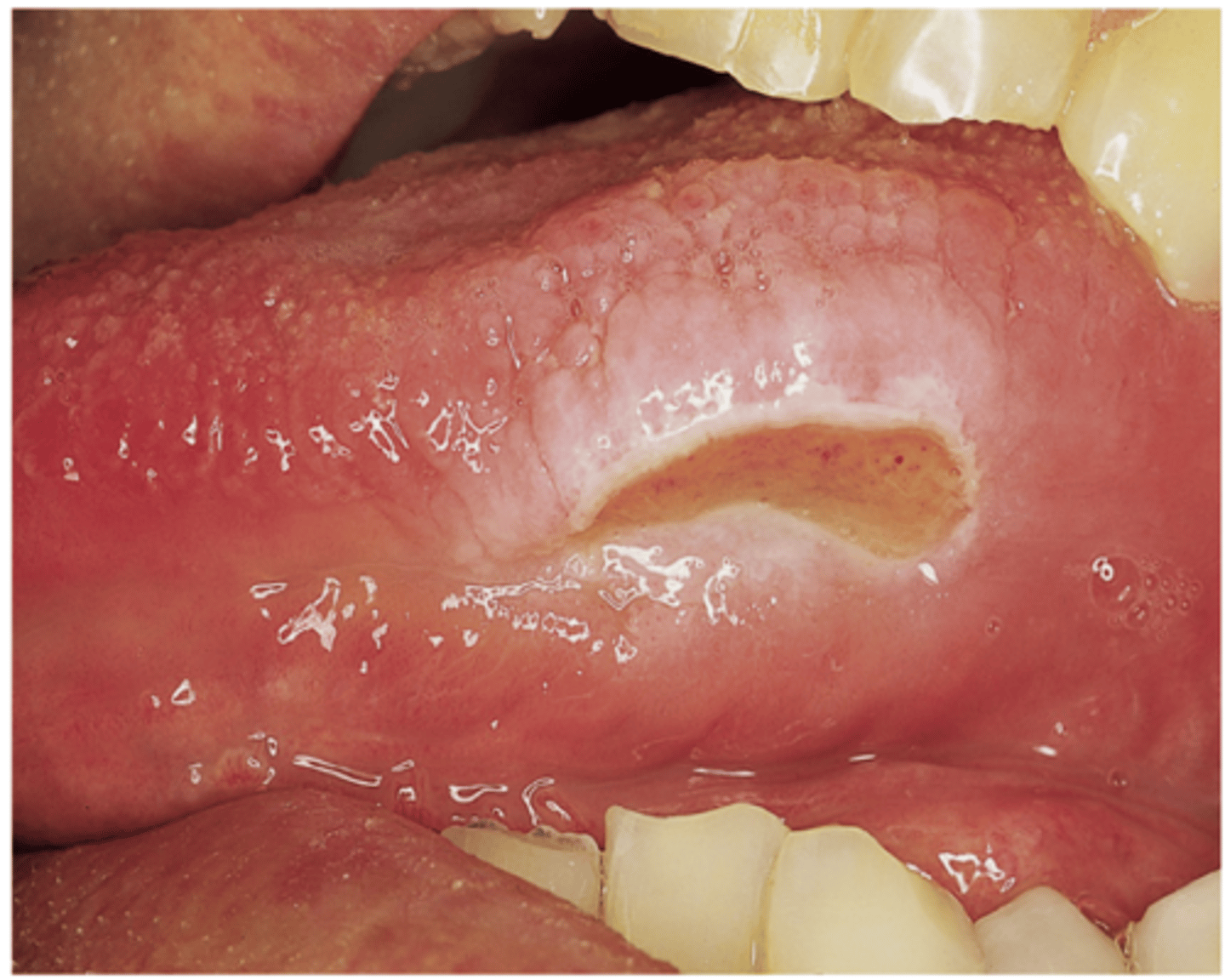
What are the clinical and microscopic features of traumatic ulcers?
painful, mucosal ulceration
ulcer with eosinophils present in inflammatory infiltrate
How can you treat traumatic ulcers?
elimination of cause
What is the cause of frictional keratosis?
chronic friction against mucosal surface
What are the clinical and microscopic features of frictional keratosis?
white mucosal surface
hyperkeratosis
How can you treat frictional keratosis?
elimination of cause
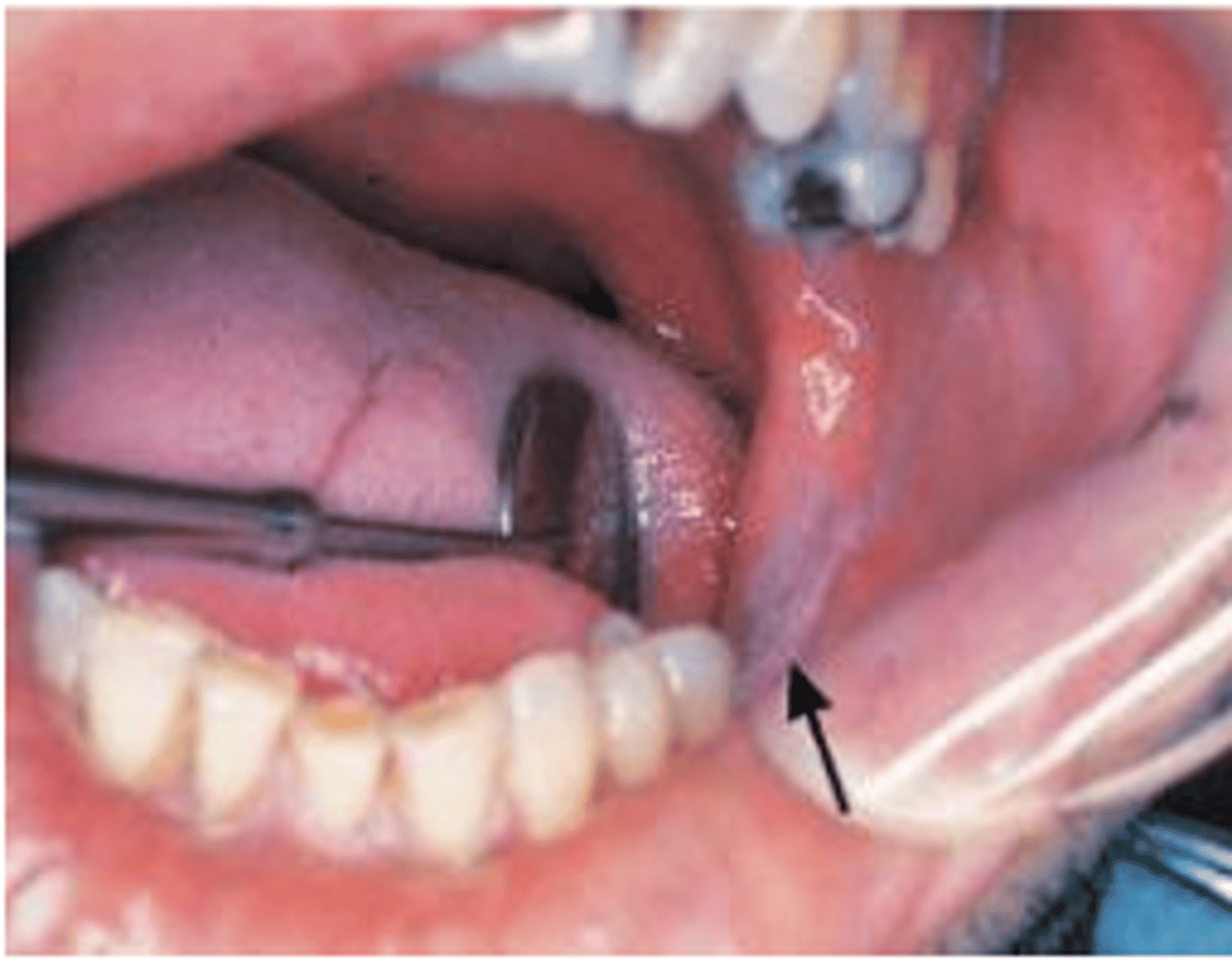
What is the cause of linea alba?
teeth clenching / cheek biting
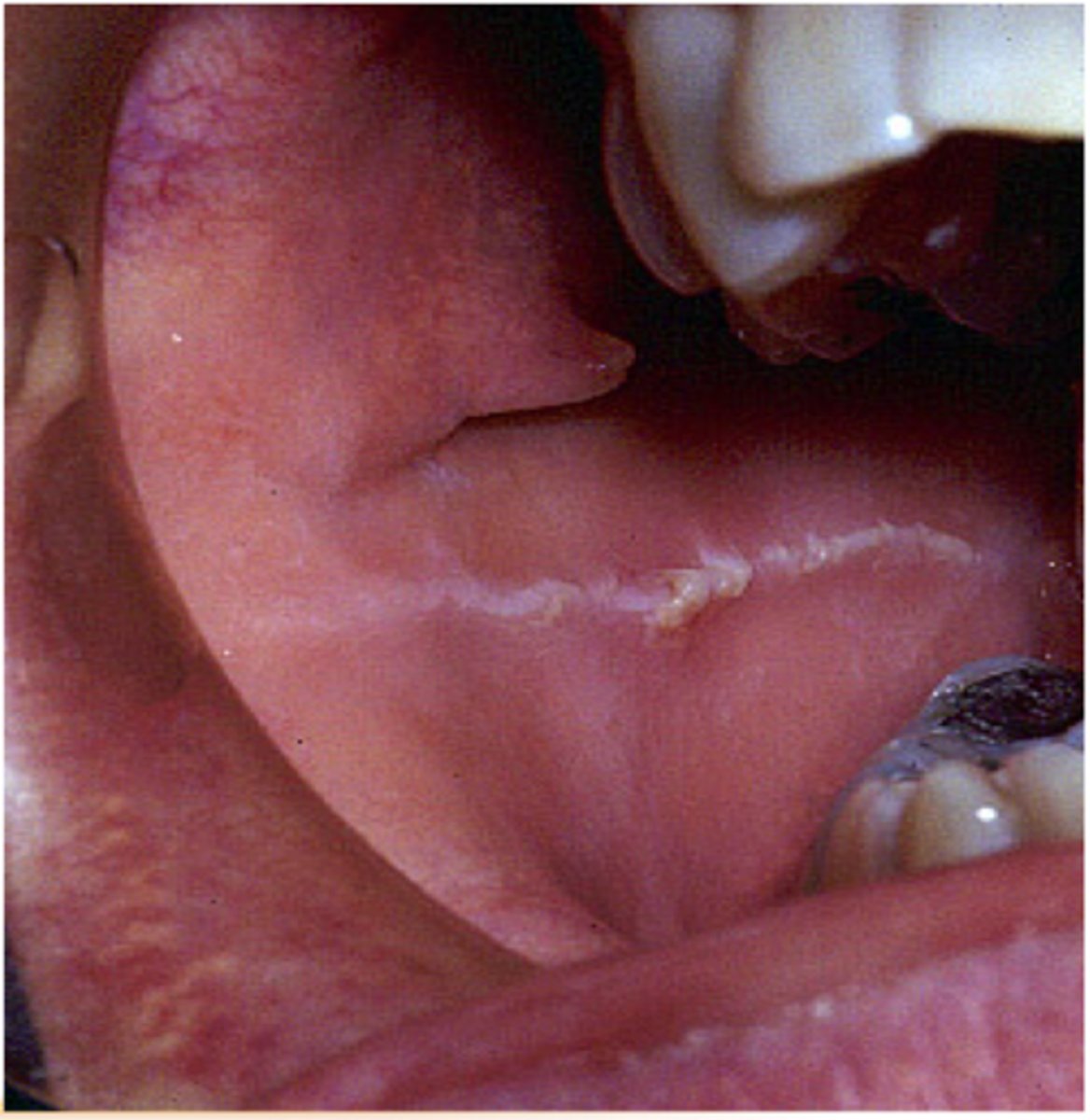
What are the clinical and microscopic features of linea alba?
anterior to posterior white line
epithelial hyperplasia and hyperkeratosis
How can you treat linea alba?
none
may regress slightly if you stop the habit
What is the cause of nicotinic stomatitis?
smoking
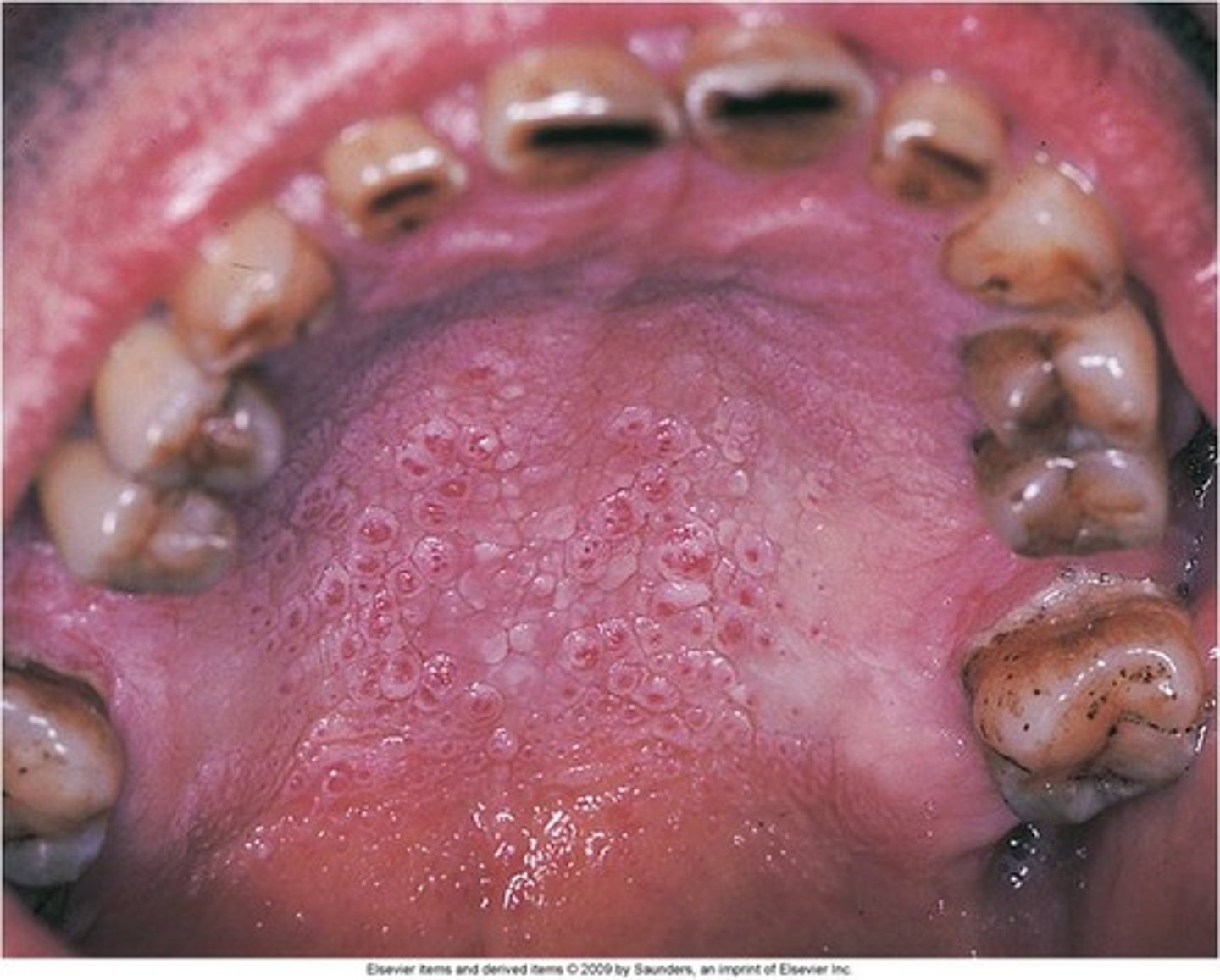
What are the clinical and microscopic features of nicotinic stomatitis?
white, opacification of palatal mucosa with raised red dots
hyperkeratosis with inflamed minor salivary glands
How can you treat nicotinic stomatitis?
elimination of cause
What is the cause of solar cheilitis?
sun exposure
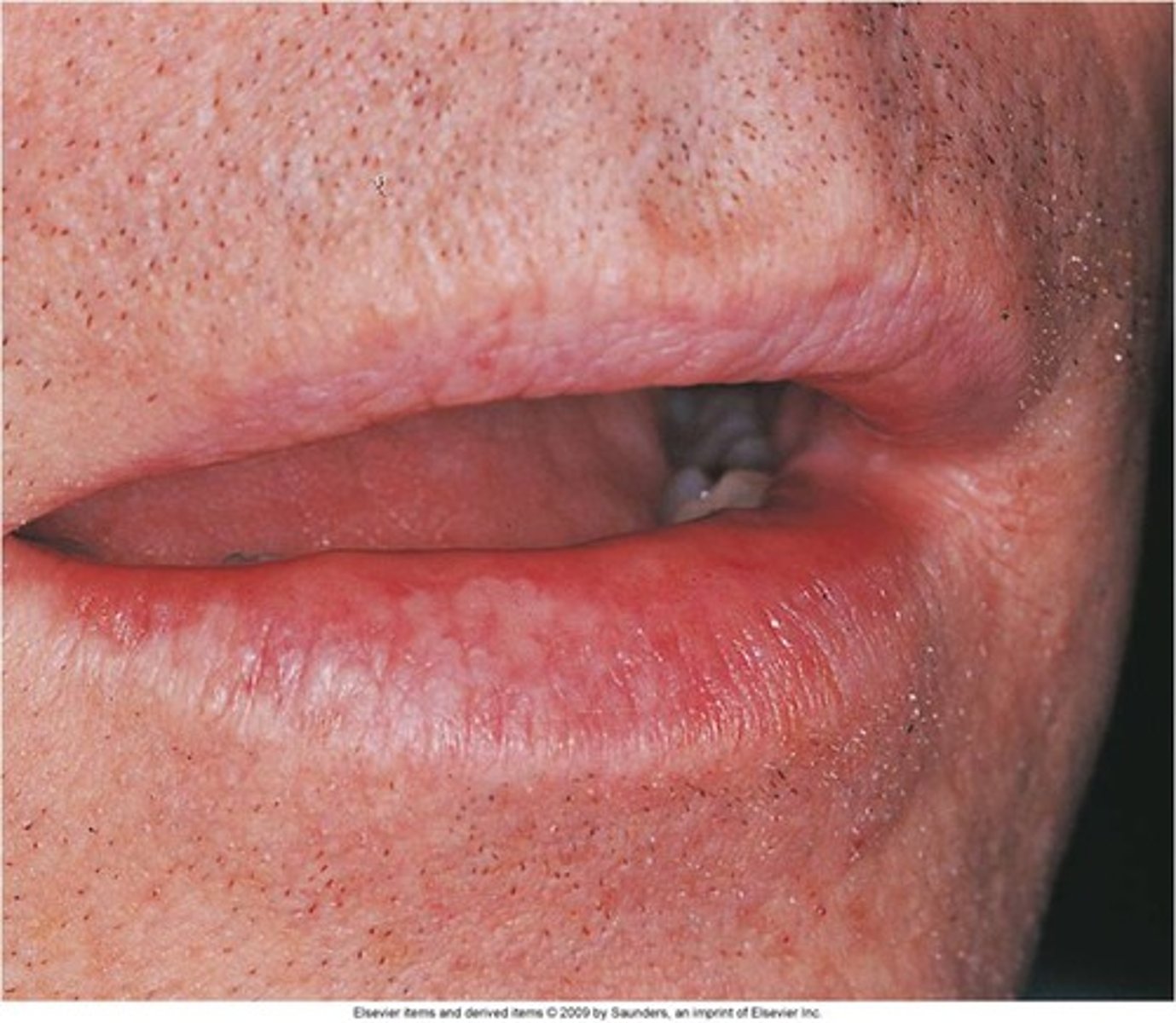
What are the clinical and microscopic features of solar cheilitis?
indistinct, fissured skin mucosal interface
degenerative changes in CT
How can you treat solar cheilitis?
protect lips and skin from sun exposure
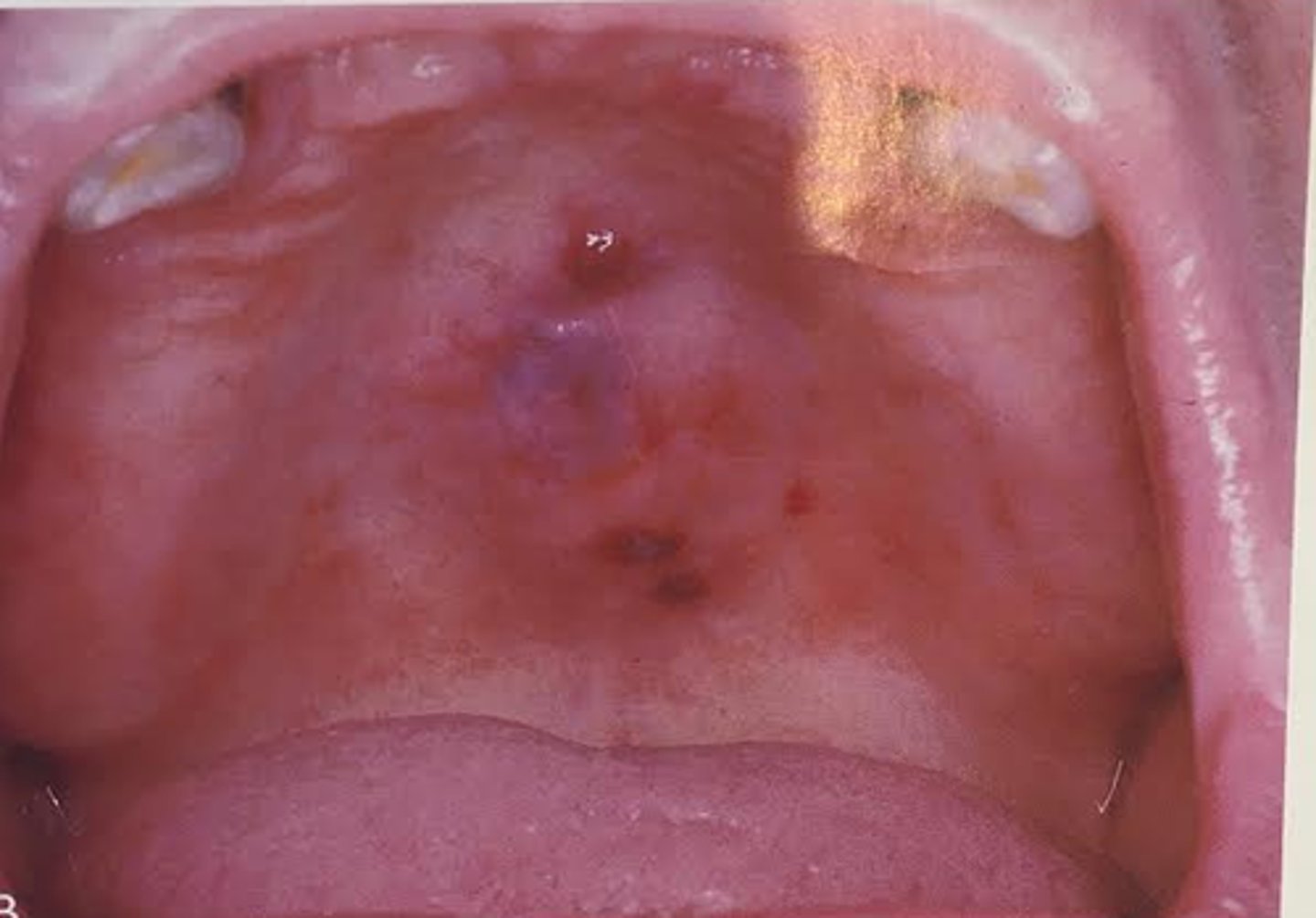
What is the cause of mucocele?
severed salivary gland duct

What are the clinical and microscopic features of mucocele?
localized tissue swelling that increases and decreases in size
extravasated mucus in tissue surrounded by granulation tissue
What is the cause of ranula?
obstruction / severing of salivary gland duct

How can you treat mucocele?
excision
may spontaneously resolve
What are the clinical and microscopic features of ranula?
fluid filled swelling that increase / decreases in size
resembles mucocele or mucous cyst
How can you treat ranula?
surgery
What is the cause of peripheral ossifying fibroma?
not known

What are the clinical and microscopic features of peripheral ossifying fibroma?
exophytic gingival lesion that resembles an irritation fibroma
composed of cellular fibrous CT interspersed with scattered bone and cementum like calcifications
How can you treat peripheral ossifying fibroma?
surgical excision and scaling of adjacent teeth to remove any irritants
What is the cause of denture induced fibrous hyperplasia? (also called epilus fissuartum)
ill fitting denture
What are the clinical and microscopic features of denture induced fibrous hyperplasia?
elongated folds of exophytic tissue surrounding denture flange
dense fibrous CT surfaced by epithelium that may be hyperplastic and ulcerated
How can you treat denture induced fibrous hyperplasia?
surgical excision
new denture
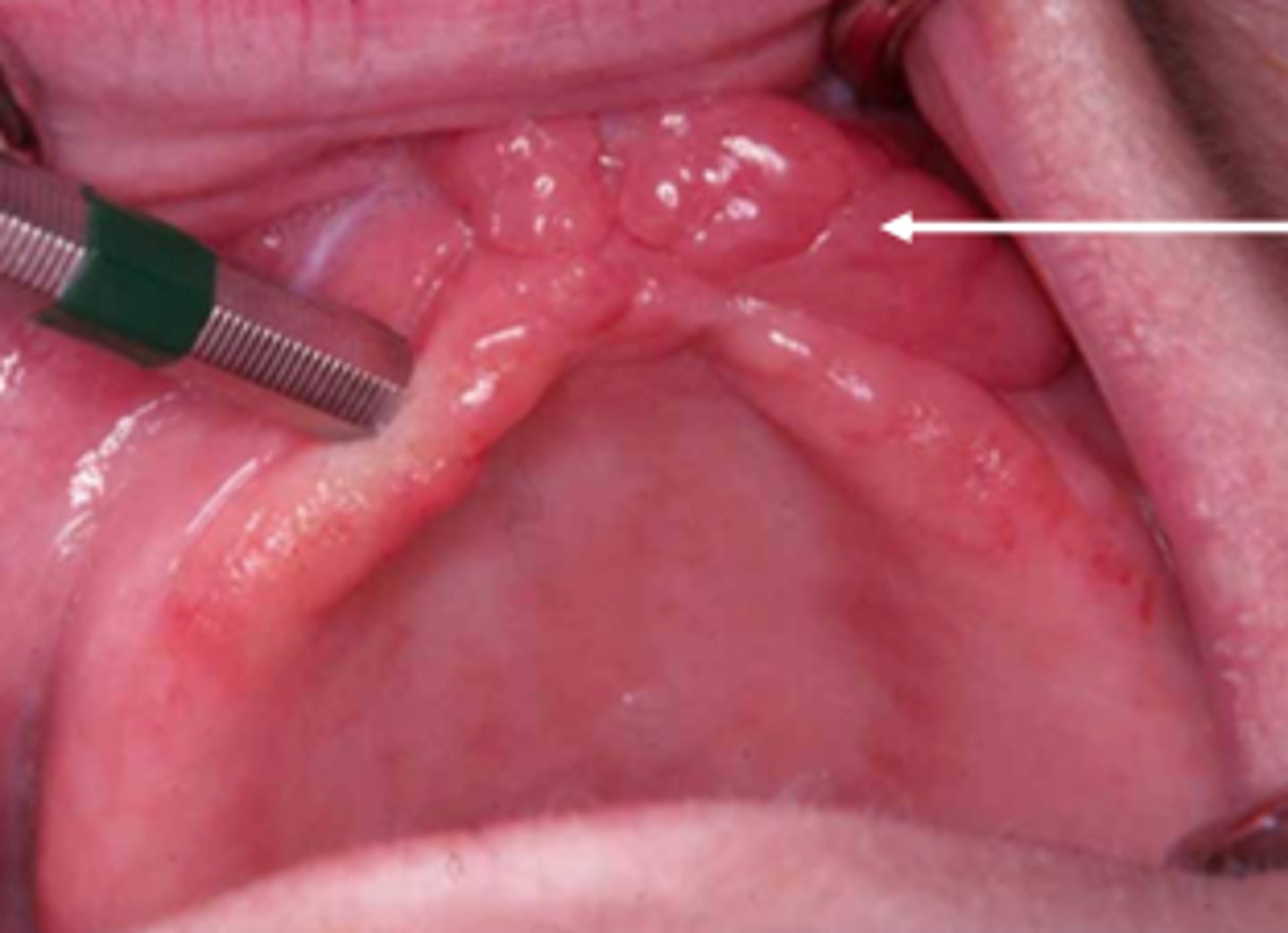
What is the cause of gingival enlargement?
response to chronic inflam
idiopathic
drug reaction
hormonal changes
genetic

What are the clinical and microscopic features of gingival enlargement?
increase in bulk of free and attached gingiva
no stippling
erythematous to normal color
CT surfaced by squamous epithelium
What is the cause of chronic hyperplastic pulpitis?
caries

How can you treat gingival enlargement?
gingivectomy
good oral hygiene
What are the clinical and microscopic features of chronic hyperplastic pulpitis?
red or pink nodule protruding from pulp chamber of tooth with large, open carious lesion
granulation tissue surfaced by squamous epithelium
How can you treat chronic hyperplastic pulpitis?
extraction of tooth
endodontic treatment
What is the cause of periapical abscess?
inflammation of dental pulp
pre existing periapical chronic inflammation

What are the clinical and microscopic features of periapical abscess?
pain, swelling, fistula, light extrusion of tooth
acute inflammatory infiltrate
How can you treat a periapical abscess?
drain
What is the cause of radicular cyst?
radicular cyst not removed with extracted tooth
What are the clinical and microscopic features of periapical granuloma?
asymptomatic
tooth sensitivity to percussion
slight extrusion of tooth
chronic inflammatory infiltrate
How can you treat a periapical granuloma?
extraction
endodontic therapy
What is the cause of periapical granuloma?
pulpal inflam and necrosis
What are the clinical and microscopic features of radicular cyst?
asymptomatic
spaced lined by epithelium surrounded by an infiltrate of chronic inflammatory cells
How can you treat a radicular cyst?
endodontic therapy
apicoectomy (remove root of tooth)
extraction and curettage of extraction site
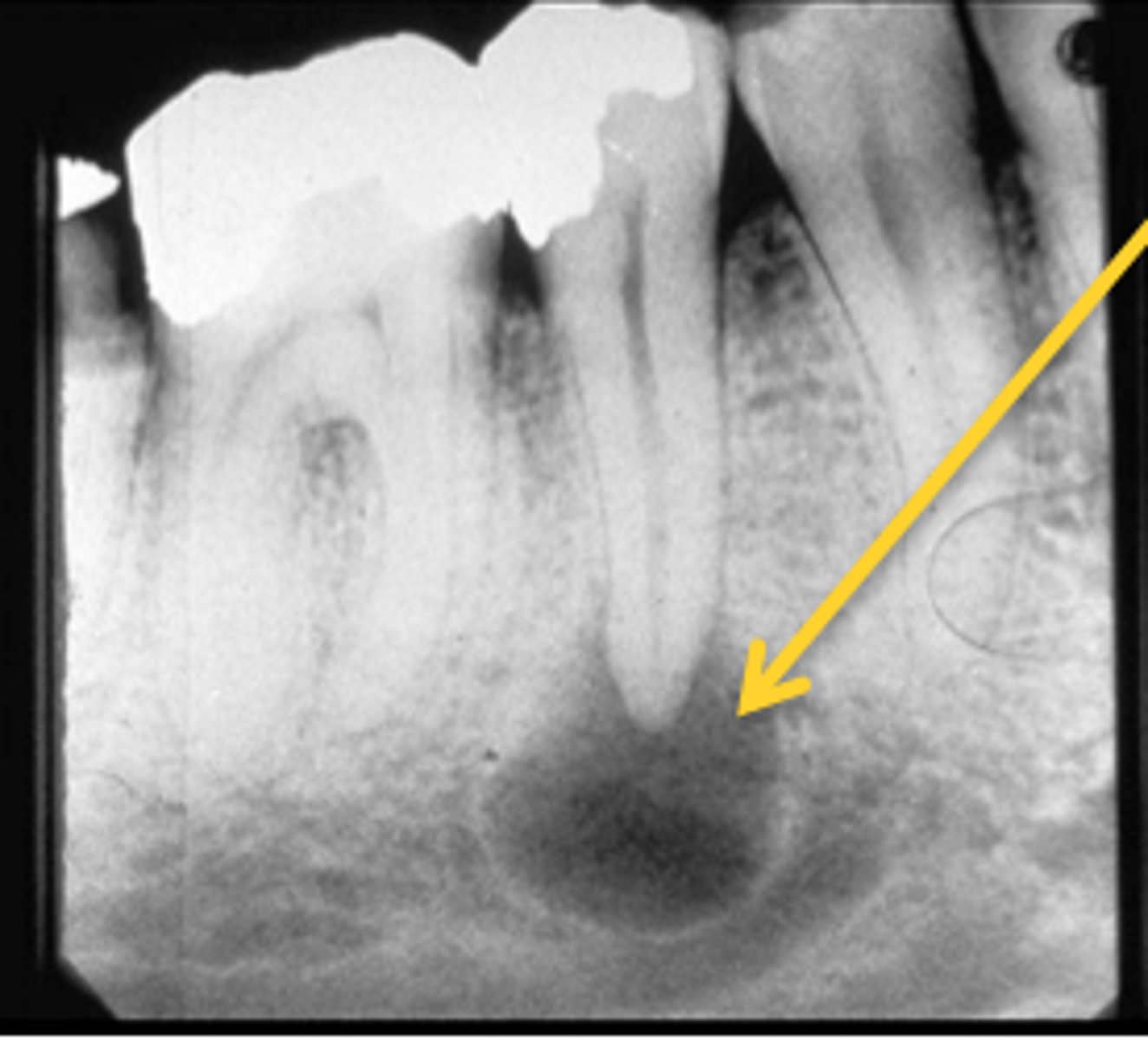
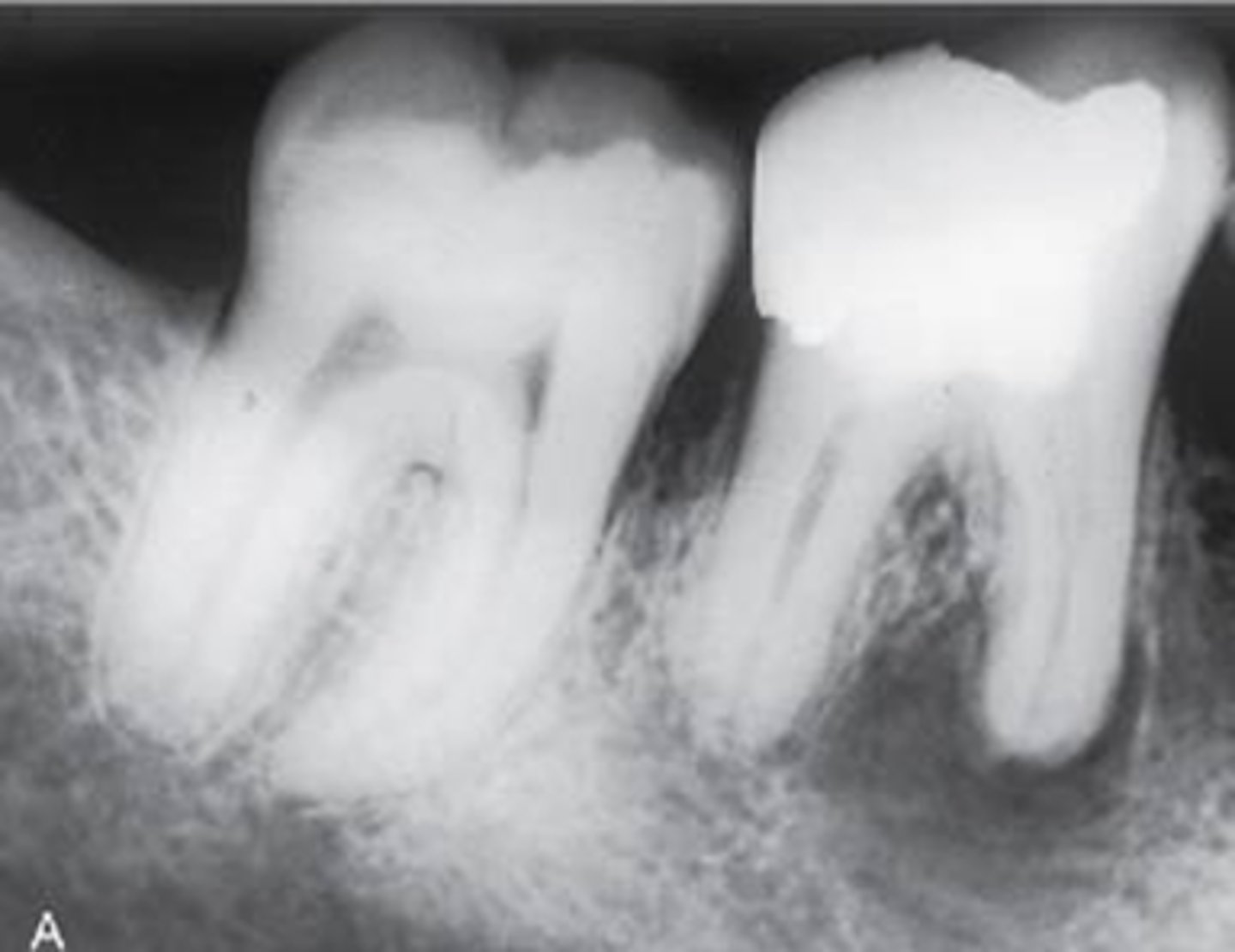
What is condensing osteitis and its cause?
change in bone near apices of teeth
may be a reaction to a low grade infection
What tooth is most commonly associated with condensing osteitis?
md first molar
(can also include md second molar and md premolars)
How do you diagnose condensing osteitis?
appears radiopaque in the periapical area of teeth with defined or diffuse borders
can be seen as radiolucent or radiolucent center with radiopaque borders
associated with caries or restored tooth, asymptomatic