T5 - IE5 - Infectious Diseases I - Fong (Merna) - Meningitis
1/103
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
104 Terms
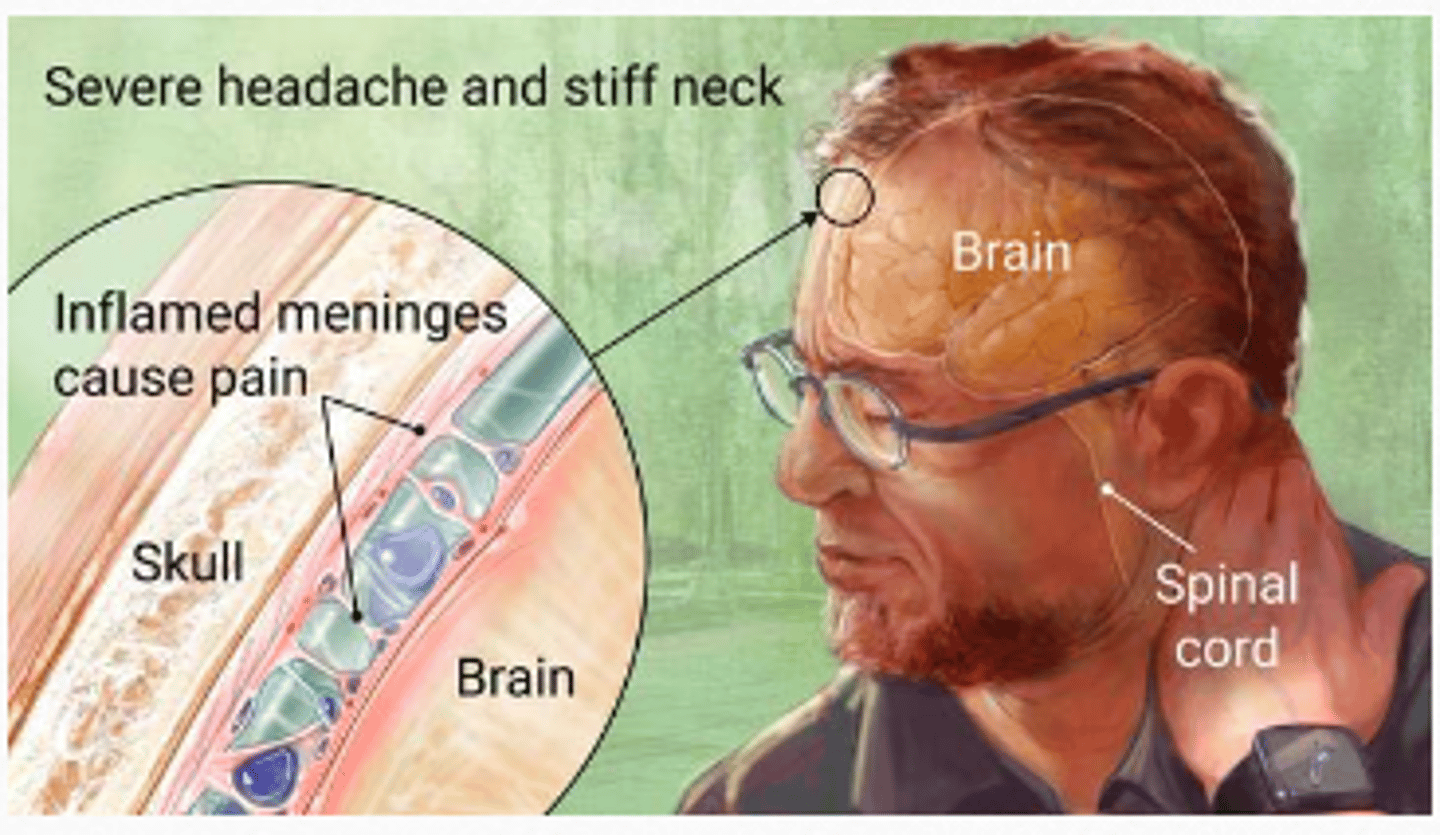
Meningitis often presents with _________ headache and _______ neck
- severe (headache)
- stiff (neck)
Meningitis clinical presentation figure
Meningitis
inflammation of the meninges
Epidemiology: risk factors and mortality rates widely vary depending on the causative ______________ and _____ ___________
- microorganism
- age group
Meningitis is a disease caused by __________ of the protective membranes covering the brain and spinal cord known as the __________
- inflammation (of the protective membranes)
- meninges
Meningitis is a disease caused by inflammation of the protective membranes covering the ______ and _______ ______ known as the meninges.
- (covering the) brain
- spinal cord
Meningitis can be ____-__________ because of the __________ to the brain and spinal cord; therefore the condition is classified as a medical emergency
- life-threatening
- proximity (to the brain and spinal cord)
Meningitis can be life-threatening because of the proximity to the brain and spinal cord; therefore the condition is classified as a ___________ _________
- (classified as a) medical emergency
Meningitis can strike quickly and kill within ________, so _______ medical attention is essential
- (kill within) hours
- urgent (medical attention is essential)
Meninges is the system of ____________ which develops the central nervous system
- (system of) membranes
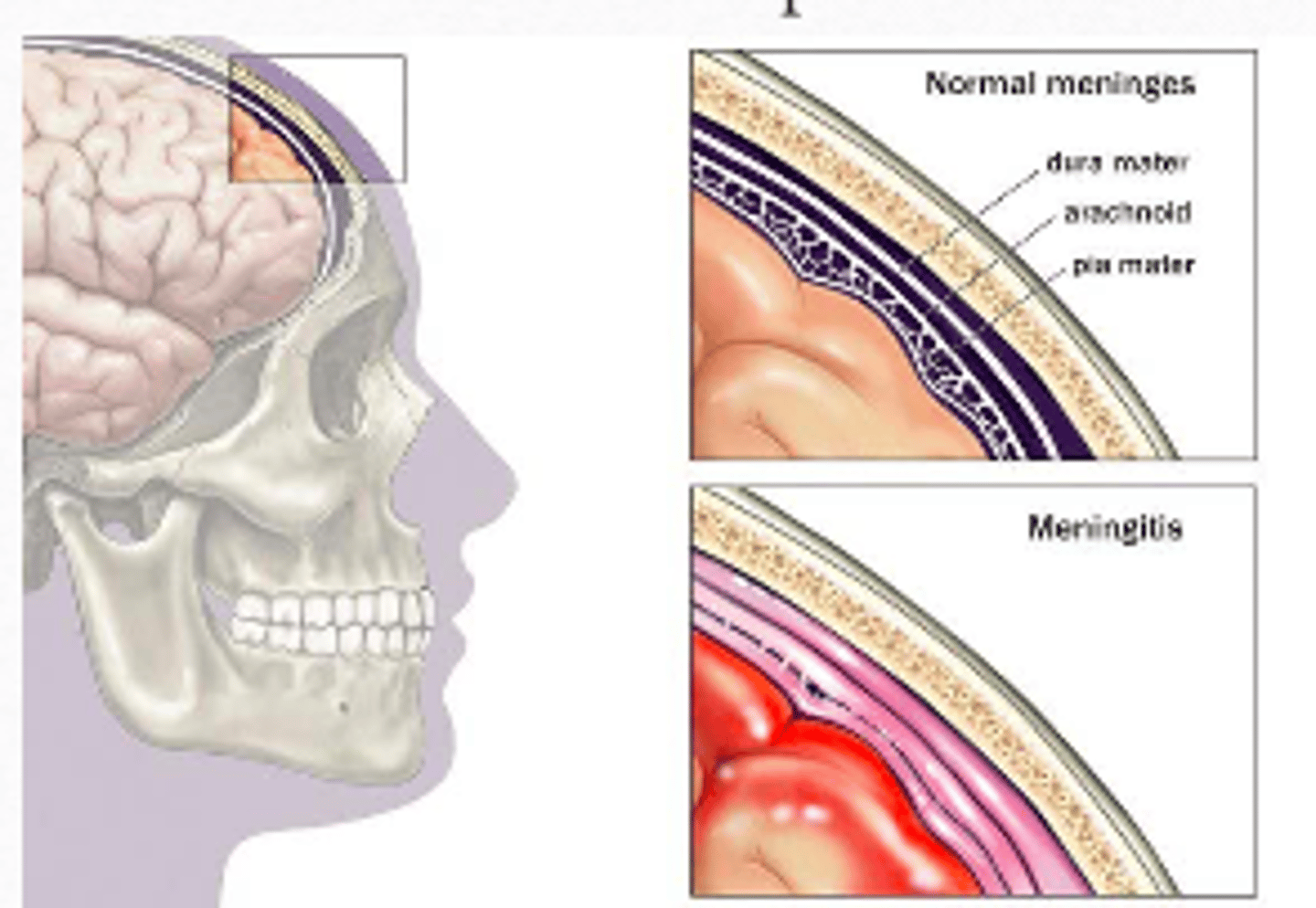
3 Layers of the meninges
Dura mater
Arachnoid mater
Pia mater
Subarachnoid space is located between the arachnoid and the Pia mater
Layers of the meninges: subarachnoid space is located between the ____________ and the ______ mater
- Arachnoid
- Pia (mater)
Meninges layers figure
Encephalitis
inflammation of the brain tissue itself
Meningoencephalitis
inflammation of the meninges and brain
(some combination of both)
Cause of meningitis
Viral
Bacterial
Fungal
Parasitic / protozoal
Viral meningitis is more ________ but bacterial meningitis can be more ___________
- (more) common
- (more) dangerous
Pathogenesis of bacterial meningitis diagram
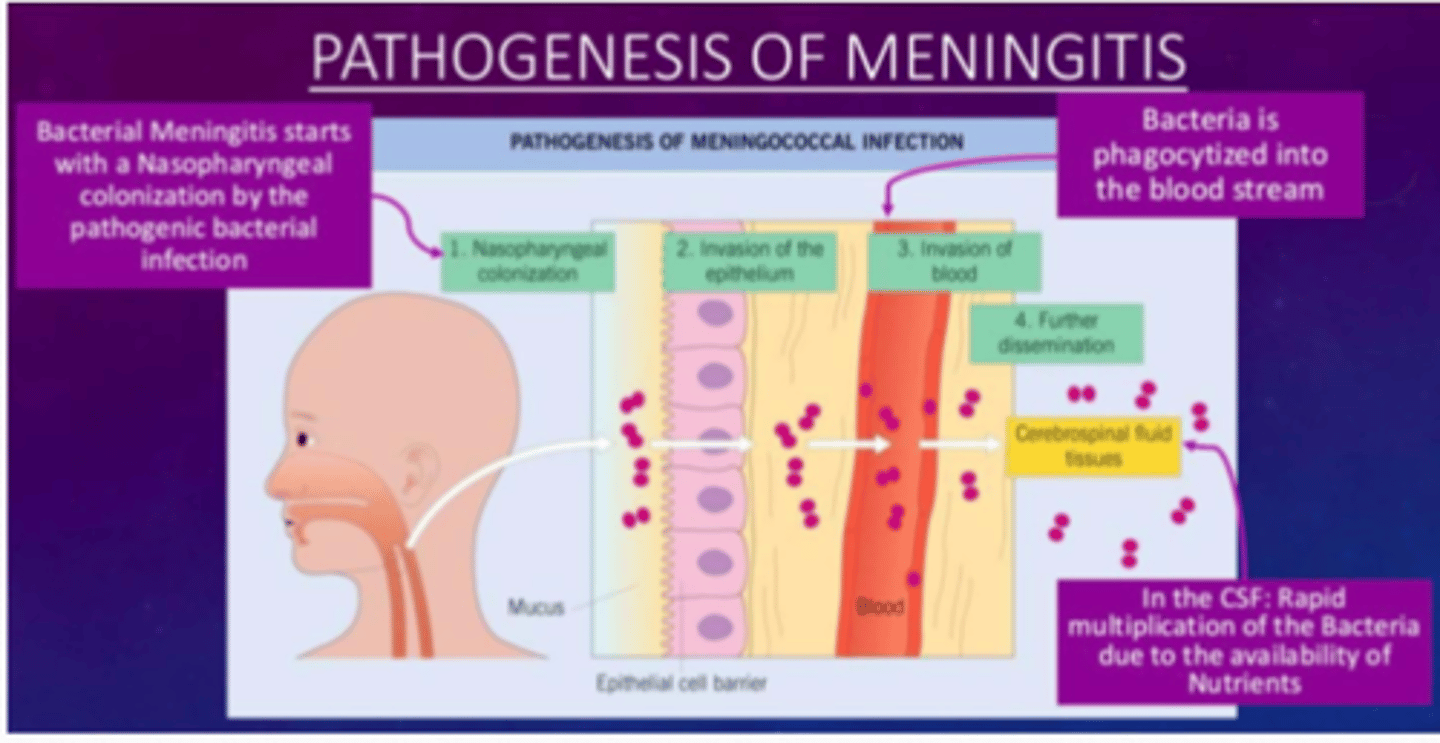
Pathogenesis of bacterial meningitis: bacterial meningitis starts with a _____________ ______ by the pathogenic bacterial infection
- Nasopharyngeal colonization (by the pathogenic bacterial infection)
Pathogenesis of bacterial meningitis: bacterial meningitis starts with a nasopharyngeal colonization by the ___________ ______ __________
- pathogenic bacterial infection
There is invasion of the epithelium
Pathogenesis of bacterial meningitis: bacterial meningitis starts with a nasopharyngeal colonization by the pathogenic bacterial infection
Then, there is an _____________ of the ____________
- invasion
- (of the) epithelium
Followed by invasion of the blood
Pathogenesis of bacterial meningitis: bacterial meningitis starts with a nasopharyngeal colonization by the pathogenic bacterial infection
Then, there is an invasion of the epithelium followed by invasion of the ________
Bacteria is ____________ into the blood stream and bacteria is then further _____________
- (invasion of the) blood
- phagocytized (into the blood stream)
- (further) dissemination
This dissemination may enter the CSF and tissues
Pathogenesis of bacterial meningitis: bacterial meningitis starts with a nasopharyngeal colonization by the pathogenic bacterial infection
Then, there is an invasion of the epithelium, then blood, further dissemination into the ___________ ______ and tissues.
In the CSF, _______ multiplication, of the bacteria due to the availability of the __________
- (dissemination into the) cerebrospinal fluid
- rapid (multiplication)
- (availability of the) nutrients
Risk factors of bacterial meningitis
Age
- children < 5 years ( particularly < 2 years)
- meningitis is severe in neonates (< 1 month)
- elderly
Large group communities (schools, campuses)
Immunocompromised
Smoking
Risk factors of bacterial meningitis - age: children ___ _____ years particularly ___ __ years
- < 5 (years)
- (particularly) < 2 (years)
Risk factors of bacterial meningitis - age: meningitis is severe in ___________
- neonates
< 1 month
Risk factors of bacterial meningitis - age: other large age group are the _________
- (are the) elderly
Risk factors of bacterial meningitis - large ______ ______________
- (large) group communities
e.g., schools, campuses
Risk factors of bacterial meningitis - those that are ____________ and/or ____________
- immunocompromised
- smoke
Complications of bacterial meningitis
cerebral edema
concentration / memory impairment
hearing loss of deafness
seizures
death
Clinical presentation of Bacterial Meningitis Diagram

Clinical presentation of Bacterial Meningitis
Fever
Neck stiffness (nuchal rigidity)
Altered mental status (AMS)
Headache
Nausea
Rash
Photophobia
Neurological deficits
Nuchal rigidity
neck stiffness
AMS
altered mental status
Testing for nuchal rigidity
Kernig's sign
Brudzinski sign
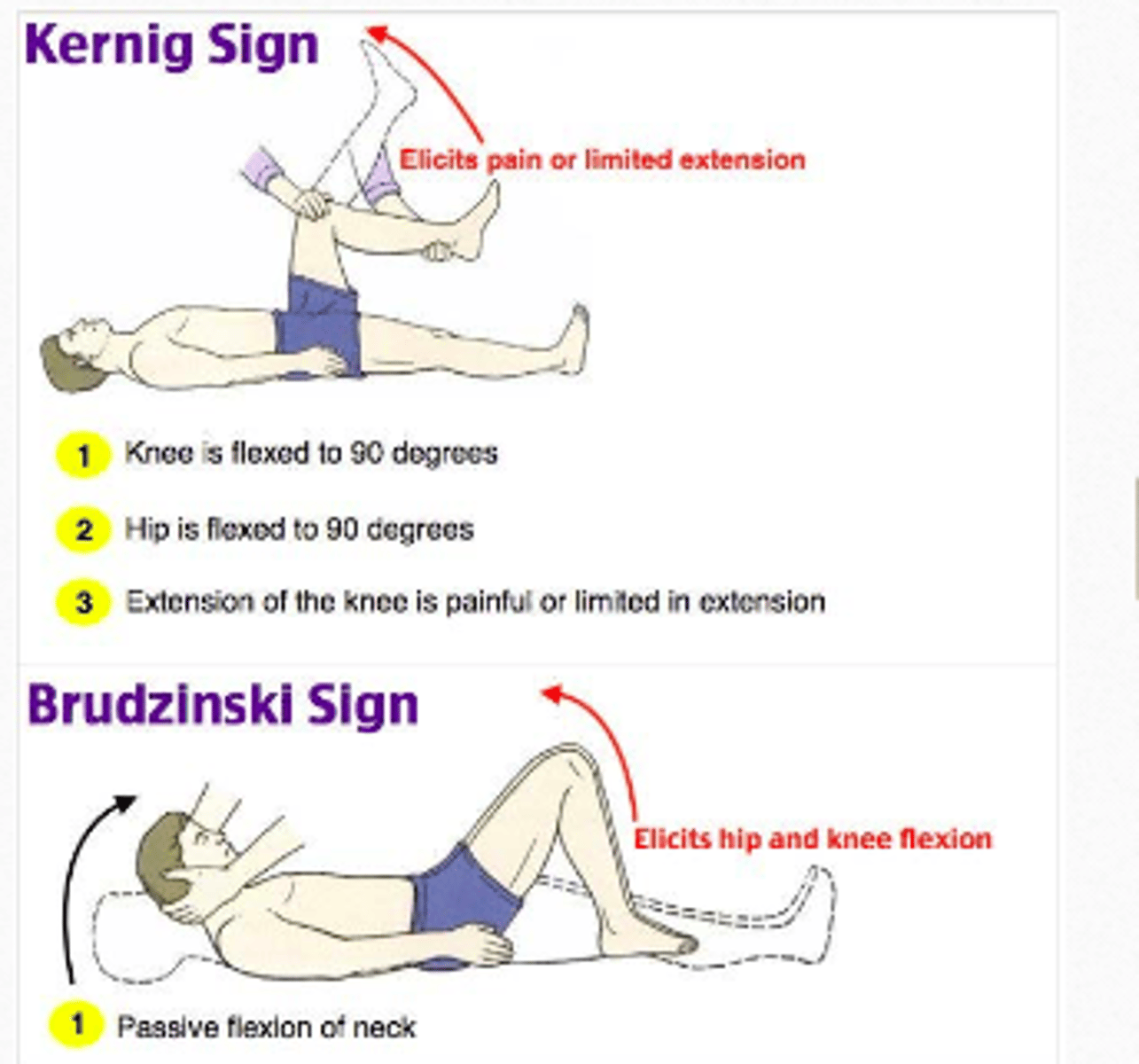
Nuchal rigidity tests: Kernig's sign: is assessed with the patient lying _______, with the hip and knee ______ to 90°.
In a patient with a positive Kernig's sign, _____ limits passive __________ of the knee
- (lying) supine
- flexed (to 90°)
- pain
- (limits passive) extension
Kernig's sign
inability to extend legs
Nuchal rigidity tests - Brudzinksi sign: positive sign occurs when flexion of the neck causes __________ ________ of the knee and hip
- involuntary flexion (of the knee and hip)
Classic triad of meningitis
Fever
Nuchal rigidity
Altered mental status
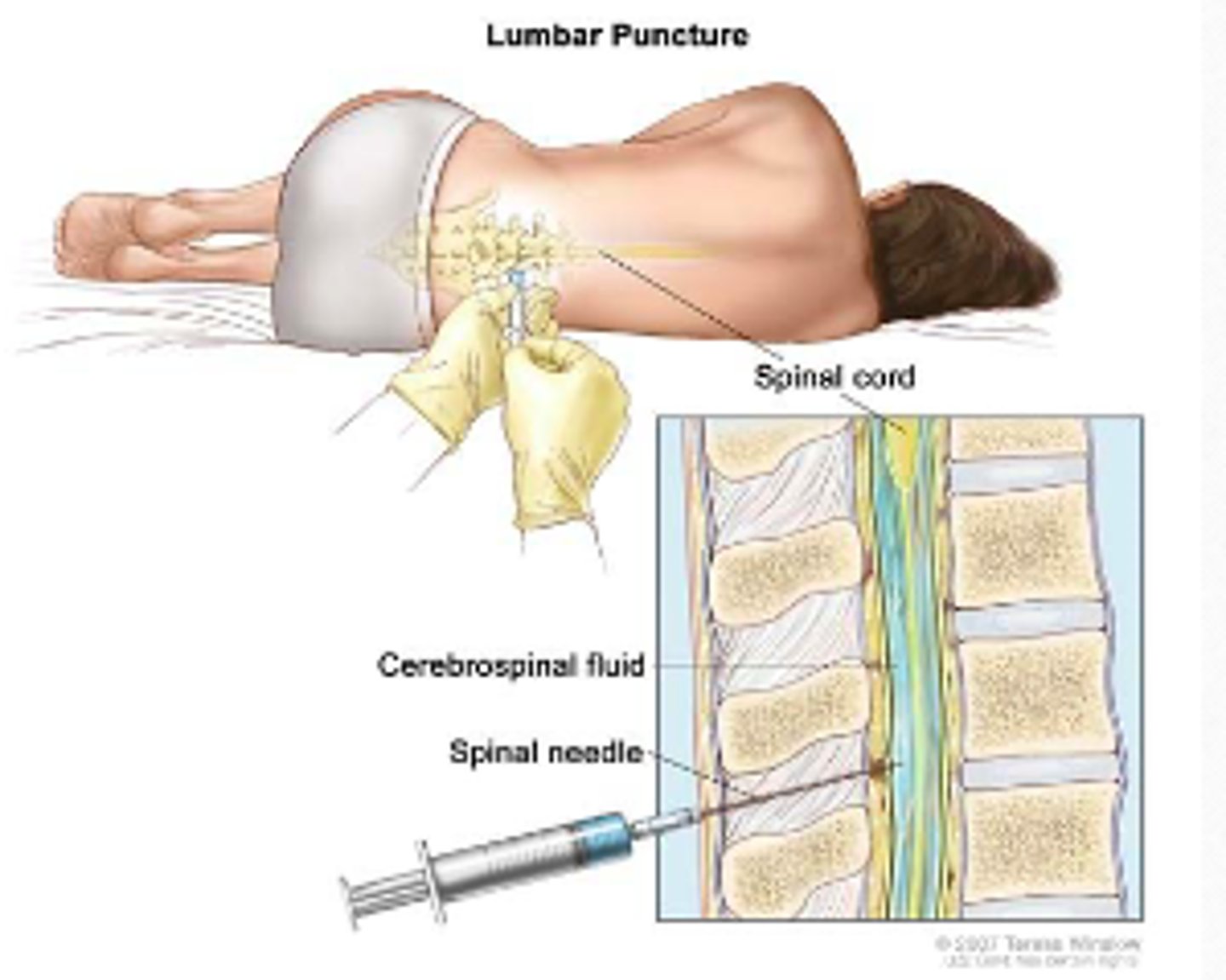
Diagnosis of meningitis - lumbar puncture
invasive procedure used to remove a sample of cerebrospinal fluid (CSF) from the subarachnoid space in the spine
Also called a "spinal tap"
Diagnosis of meningitis - lumbar puncture: is an invasive procedure used to remove a sample of cerebrospinal fluid (CSF) from the _____________ ____ in the ________
- subarachnoid space
- (in the) spine
Also called a "spinal tap"
CSF
cerebrospinal fluid
Spinal tap
another name for lumbar puncture
Diagnosis of meningitis - lumbar puncture figure
Diagnostic testing for bacterial meningitis
LP can cause brain herniation, need CT to ensure
Lumbar puncture (LP) required for definitive diagnosis
Getting CT delays the LP, which delays antibiotics
Delayed antibiotics lead to worse outcomes
Order of diagnostic testing for meningitis
1) CT (to ensure no risk of herniation)
2) LP required for definitive diagnosis
3) Antibiotics (delayed antibiotics lead to worse outcomes
Diagnostic testing for bacterial meningitis: LP can cause _______ ______________, need CT to ensure
- (can cause) brain herniation
Diagnostic testing for bacterial meningitis: Lumbar puncture (LP) required for _____________ ____________
- (required for) definitive diagnosis
LP
lumbar puncture
Diagnostic testing for bacterial meningitis: Getting _____ delays the ____, which ________ antibiotics
- (Getting) CT
- (delays the) LP
- delays (antibiotics)
Diagnostic testing for bacterial meningitis: delayed antibiotics lead to ___________ outcomes
- worse (outcomes)
CSF findings chart in meningitis
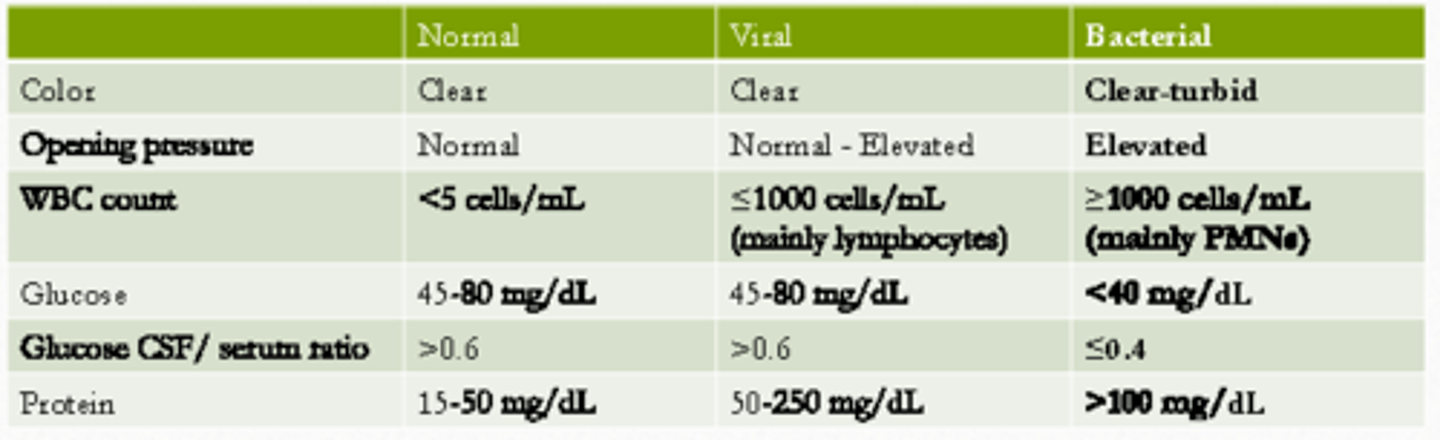
Bacterial meningitis CSF findings - color
clear-turbid
(i.e., from clear to cloudiness)
Bacterial meningitis CSF findings - opening pressure
Elevated (opening pressure)
Bacterial meningitis CSF findings - WBC count
≥ 1000 cells / mL (mainly PMNs)
Bacterial meningitis CSF findings - glucose
< 40 mg/dL
Whereas, in normal and viral it is 45-80 mg/dL; in bacterial meningitis, the bacteria will consume glucose
Bacterial meningitis CSF findings -protein
> 100 mg/dL
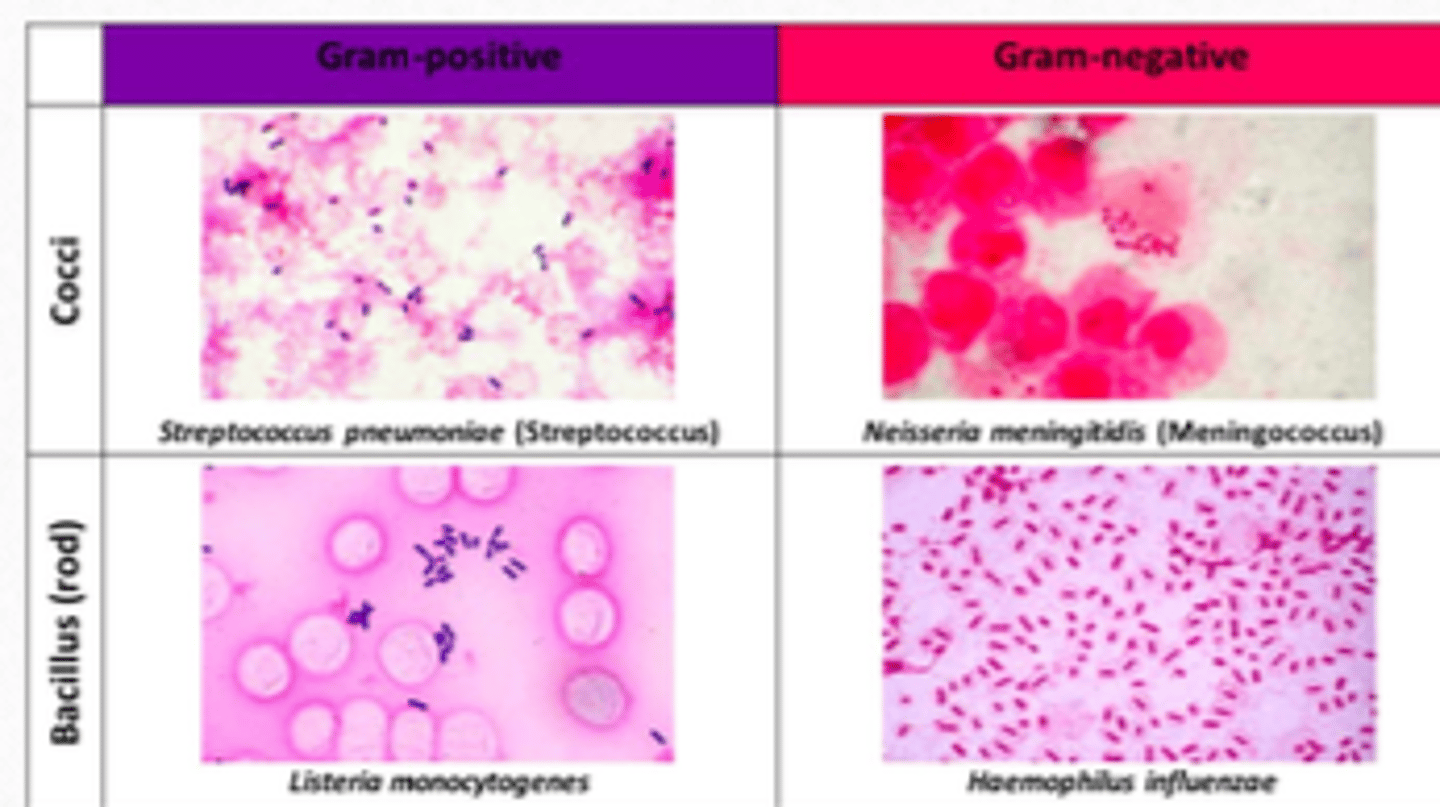
4 Bugs of Bacterial Meningitis (from most common to least)
Streptococcus pneumonia (58%)
- GBS (18.1%)
Neisseria meningitidis (13.9%)
Haemophilus influenza (6.7%)
Listeria monocytogenes (3.4$)
Bacterial meningitis figure
Most common bug in bacterial meningitis
Streptococcus pneumoniae (58%)
- GBS (18.1%)
GBS
Streptococcus agalactiae
Common pathogens of bacterial meningitis by age: < 1 month
S. agalactiae (GBS)
E. coli
Listeria monocytogenes
Klebsiella
< 1 month
Common pathogens of bacterial meningitis by age: 1-23 months
S. pneumoniae
N. meningitidis
S. agalactiae (GBS)
E. coli
H. influenzae
1-23 months
Common pathogens of bacterial meningitis by age: 2-50 years
S. pneumoniae
N. meningitidis
2-50 years
Common pathogens of bacterial meningitis by age: > 50 years
S. pneumoniae
N. meningitidis
L. monocytogenes
> 50 years
Empiric meningitis treatment for < 1 month
Ampicillin
plus
Cefepime*
OR
Aminoglycoside
empiric treatment: age < 1 month
Neonates should _______ ___ _______ ceftriaxone due to the increased risk of biliary sludging (solids that precipitate from bile) and kernicterus (brain damage from high bilirubin)
- not be given (ceftriaxone)
Neonates should not be given ceftriaxone due to increased risk of ________ _______ and _________
- biliary sludging
- kernicterus
Biliary sludging = sludge that precipitate from bile
Kernicterus (brain damage from high bilirubin)
Empiric meningitis treatment for Age 1-23 months
ceftriaxone
plus
vancomycin
empiric treatment age 1-23 months
Empiric meningitis treatment for age 2-50 years
ceftriaxone
plus
vancomycin
similar to age 1-23 months
Empiric meningitis treatment for age > 50 years OR immunocompromised
ceftriaxone
plus
vancomycin
plus
ampicillin
treatment for ages > 50 years or immunocompromised
In special populations, we add ____________ _________
- Pseudomonas coverage
Anti-pseudomonal β-lactam: cefepime, carbapenems, ceftazidime
Anti-pseudomonal β-lactams
cefepime
ceftazidime
carbapenems
Special populations for meningitis
Basilar skull fracture
Penetrating trauma
Neurosurgery
CSF shunt
Immunocompromised
Why vancomycin: NOT for __________ but ___ ____________ resistance to ceftriaxone (10%)
- (NOT for) MRSA
- S. pneumoniae (resistance)
Antibiotic dosing in meningitis: generally speaking, be ____ ___________
- very aggressive
This is required for CSF penetration
Antibiotic dosing chart: normal vs. meningitis
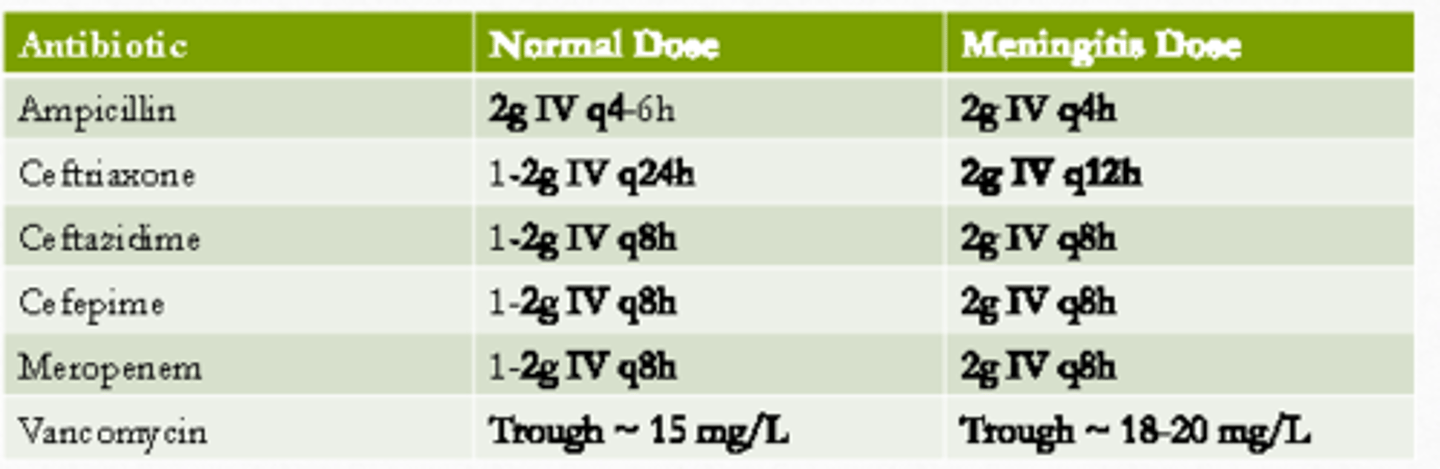
Ampicillin normal dosing and meningitis
2g IV q4-6
Meningitis:
2g IV q4h
Ampicillin meningitis dosing
Ceftriaxone normal dosing and meningitis
1-2 g IV q24H
Meningitis:
2g IV q12H
Ceftriaxone meningitis dosing
IMPORTANT
Vancomycin normal dosing and meningitis
Trough: ~15 mg/L
Meningitis dose
Trough ~18-20 mg/L
Vancomycin meningitis dose
Cefepime normal dosing and meningitis
1-2 g IV q8H
Meningitis dose
2 g IV q8H
Cefepime meningitis dose
Antibiotic dosing in meningitis: can even consider ___________ dosing of some drugs such as ____________ and ____________
- intrathecal (dosing)
- vancomycin
- aminoglycosides
NOT β-lactams
Common gram positive bacteria in meningitis
Streptococcus pneumoniae
Listeria monocytogenes
Common gram negative bacteria in meningitis
Neisseria meningitidis
Haemophilus influenzae
Meningitis duration of treatment: gram-negative tends to be ______ _________
- (tends to be) 7 days
e.g., Neisseria meningitidis, Haemophilus influenzae
Meningitis duration of treatment: Streptococcus pneumoniae
10-14 days
Meningitis duration of treatment: Listeria monocytogenes
≥ 21 days
Meningitis duration of treatment: Haemophilus influenzae
7 days
similar to Neisseria meningitidis
Meningitis duration of treatment: Neisseriea meningitidis
7 days
similar to Haemophilus influenzae
Role of corticosteroids in meningitis: ____________; corticosteroids inhibit the production of inflammatory cytokines such as ______ and ____-____
- controversial
- TNF
- IL-1
Role of corticosteroids: use _____________ 0.15 mg/kg q6H for ___-____ days, initiated 10 to 20 minutes prior to or concomitant with the first dose of antibiotics
- dexamethasone
- 2-4 (days)
Role of corticosteroids: use dexamethasone 0.15 mg/kg q6H for 2-4 days, initiated 10 to 20 minutes ________ ___ or __________ _____ the first dose of antibiotics
- prior to
- concomitant with (the first dose)
i.e., use before or WITH the first dose of antibiotics
Role of corticosteroids: clinical outcome is __________ to improve if dexamethasone is given ________ the first dose of antimicrobial
- unlikely (to improve)
- (given) AFTER
Vaccines available for meningitis
S. pneumoniae
- PPSV23 and PCV13
N. meningitidis
- Meningococcal conjugate vaccines (Men ACWY): 11-12 years, 16 years
- Serogroup B meningococcal vaccine (MenB): 16-23
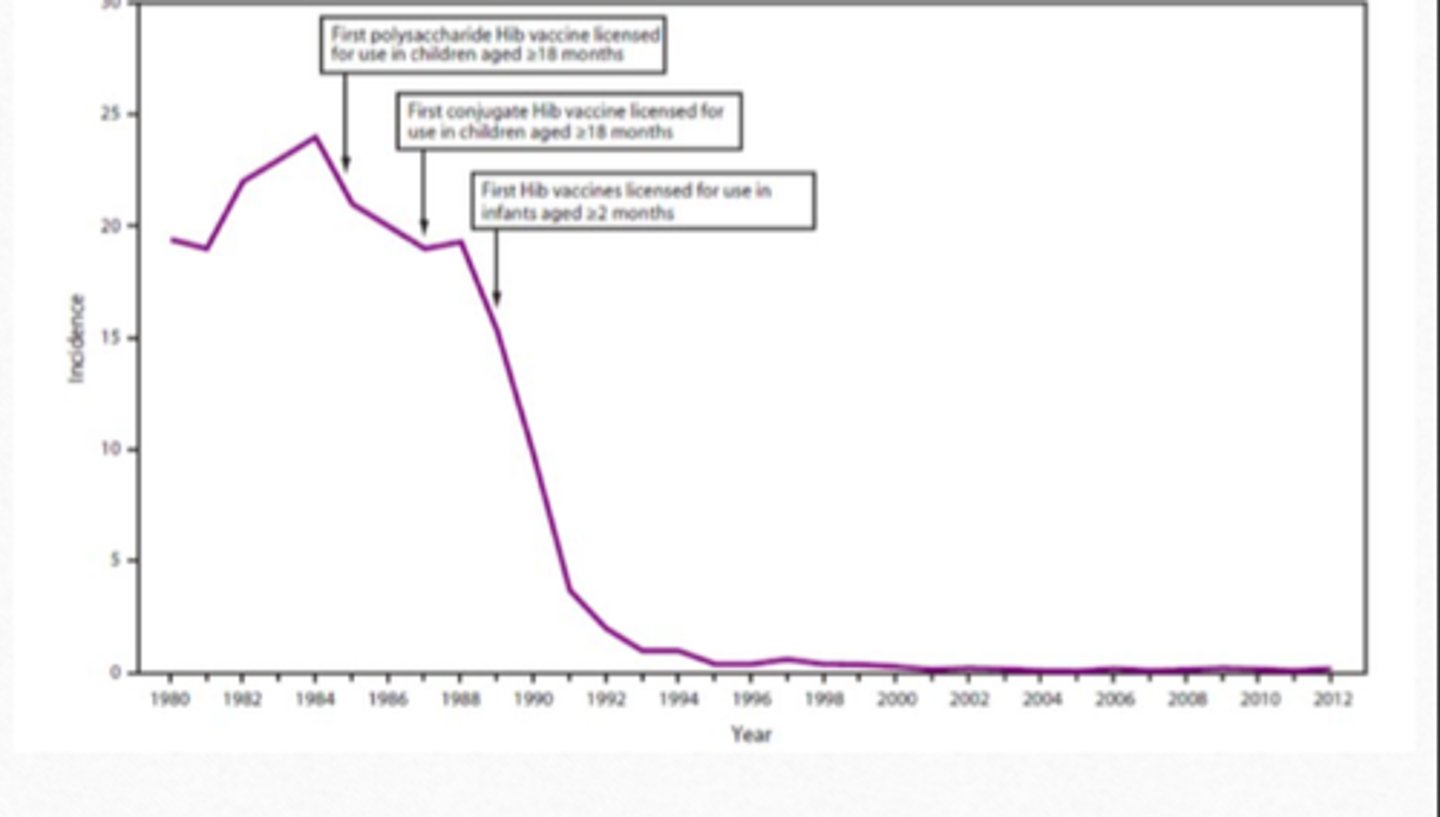
H. influenzae Type B (Hib)
- schedule: 2 months, 4 months ± 6 months, 12-15 months
- has dramatically reduce the incidence of invasive Hib disease
Listeria:
- NO vaccine available
Hib Vaccine Result Chart
Antibiotic prophylaxis: target at preventing ____ ____________ spread only (not the _____ bugs)
- N. meningitidis (spread only)
- (not the) other (bugs)
Antibiotic prophylaxis: generally for ____________ contacts / ____ ______ contact
- household (contacts)
- very close (contact)
Antibiotic prophylaxis: recommended agents
Rifampin 600 mg PO q12H x 2 days
Ciprofloxacin 500 mg PO x 1 dose
Ceftriaxone 250 mg IV x 1 dose
Summary: meningitis usually presents with ______, _________, ________ ________ and _________ _________ _________
- fever
- headache
- nuchal rigidity
- altered mental status
Summary: diagnosis is __________ with a lumbar puncture (_________)
- confirmed (with a lumbar puncture)
- LP