NAPLEX - Key Drug Guy
1/110
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
111 Terms
Drugs with Leaching Adsorption, Absorption issues with PVC containers
p110
Leach Absorbs To Take In Nutrients
Lorazepam
Amiodarone
Tacrolimus
Taxanes (most excluding paclitaxel + albumin bound Abraxane_
Insulin
Nitroglycerin
Common Drugs with Diluent Solution Requirements
- Saline (no dextrose)
p110
SALINE (no Dextrose)
A DIAbetic Can't Eat Pie
Ampicillin
Daptomycin (Cubicin)
Infliximab (Remicade)
Ampicillin/Sulbactam (Unasyn)
Caspofungin (Cancidas)
Ertapenem (Invanz)
Phenytoin (Dilantin)
Common Drugs with Diluent Solution Requirements
- Dextrose (no saline)
p110 D5W
BOAS will strangle the pharmacist who puts these drugs into anything but dextrose
Bactrim - SMX/TMP
Oxaliplatin
Amphotericin B (all)
Synercid - Quinupristin/Dalfopristin
Vesicants
Vasopressors (dopamine and NE)
Anthracyclines (doxorubicin)
Vinca alkaloids (vincristine, vinblastine)
examples of key drugs that have filter requirements
Key drugs guy p112
GAL PLAT (who's head is flat... ampules)
- Golimumab (Simponi)
- Amiodarone
- Lorazepam*
-Phenytoin*
- Lipids (1.2 micron)
- Amphotericin B lipid formulations (5 micron filter)
- Taxanes except docetaxel
- Isavuconazonium (azole)
*only when administered by continuous infusion, not for IV push
key drugs that do not require refrigeration (most IV drugs do though...) BUT NOT THESE
Key drugs guy p112
Dear Sweet Pharmacist, Freezing Makes Me Edgy!
- Dexmedetomidine (Precedex) *
- Sulfamethoxazole/Trimethoprim ( Bactrim)
- Phenytoin - crystallizes
- Furosemide - crystallizes*
- Metronidazole
- Moxifloxacin (Avelox)
- Enoxaparin (Lovenox)
*diluted precedex and furosemide can be kept cold
key drugs that require light-protection during administration
Key drugs guy p113
Protect Every Necessary Med from Daylight
- Phytonadione (vitamin K; Mephyton)
- Epoprostenol (Flolan) for Pulmonary HTN
- Nitroprusside (nitropress) - for acute HF
- Micafungin (Mycamine)
- Doxycycline
Hazardous Key Drugs
Key drugs guy p237
Antineoplastic Drugs (Chemotherapies)
Non-Antineoplastic Hazardous Drugs on NIOSH LIST
Aboritfacient
+ Misoprostol
Antibiotics
+ Chloramphenicol
+ Telavancin
Anticoagulants
+ Warfarin
Antifungals
+Fluconazole, Voriconazole
Antiretrovirals, HIV
+ Abacavir, Entecavir, Nevirapine, Zidovudine
Antivirals, Cytomegalovirus
+ Cidofovir, Ganciclovir, Valganciclovir
Acne
+ Isotretinoin
Arrhythmias
+ Dronedarone
Autoimune Conditions
+ Acitretin (psoriasis), Leflunomide, Teriflunomide
+ Fingolimod
+ Interferon Beta 1b
BPH
+ Dutasteride, Finasteride
Depression
+ Paroxetine
Diabetes
+ Exenatide
Dyslipidemia
+ Lomitapide
Seizures/Epilepsy
+ Clobazam, Clonazepam
+ Carbamazepine, Oxcarbazepine, Eslicarbazepine, Divalproex, Fosphenytoin, Phenytoin, Topiramate, Vigabatrin, Zonisamide
Gout
+ Colchicine
Heart Failure
+ Ivabradine, Spironolactone
Hepatitis
+ Ribavirin
Hormones
+ Androgens (testosterone)
+ Estrogens (estradiol)
+ Progesterones (medroxyprogesterone)
+ SERMS (Raloxifene)
+ Ulipristal
Hypercalcemia of Malignancy
+ Pamidronate
+ Zoledronic Acid (& Osteoporosis)
Hyperthyroidism
+ Methimazole, Propylthiouracil
Insomnia
+ Temazepam
+ Triazolam
Migraine
+ Dihydroergotamine
Parkinson Disease
+ Apomorphine, Rasagiline
PAH
+ Ambrisentan, Bosentan, Macitentan, Riociguat
Renal Disease
+ Darbepoetin alpha (increase RBC count)
Schizophrenia
+ Ziprasidone
Transplant
+ Azathioprine, Cyclosporine, Mycophenolate, Tacrolimus, Sirolimus
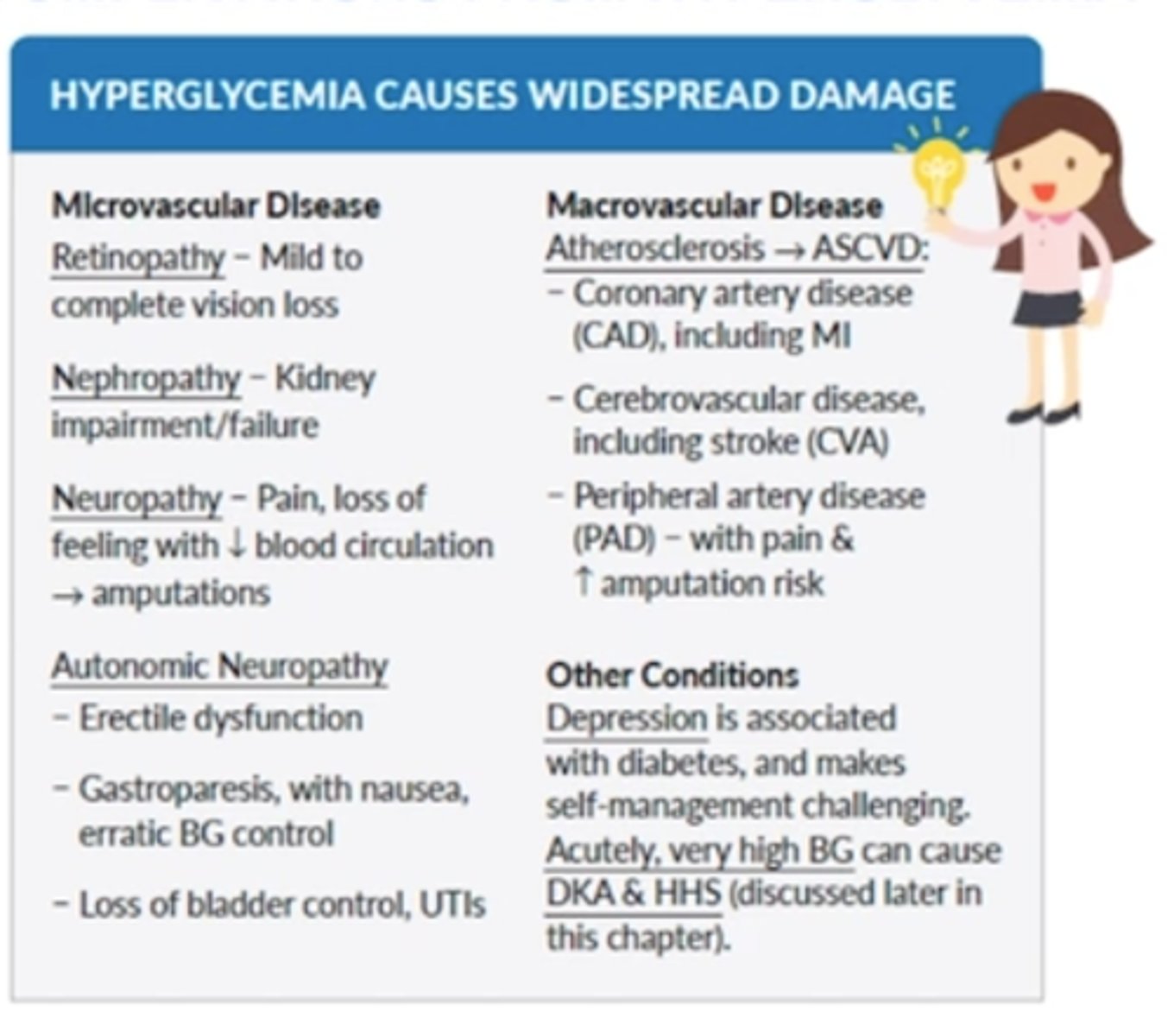
micro/macrovascular complications of diabetes
Studytip gal p627
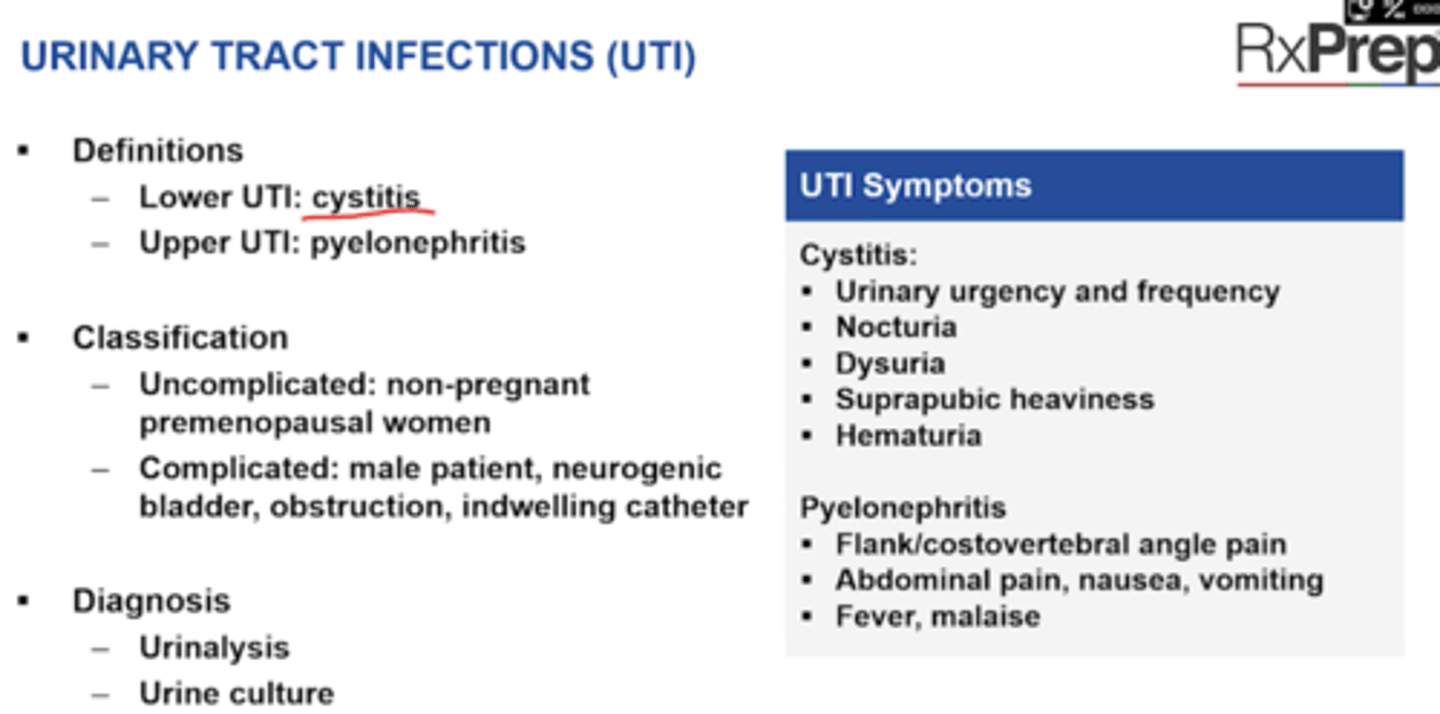
1. micro = retinopathy, nephropathy, neuropathy, autonomic neuropathy (erectile dysfunction, UTI, bladder control loss, gastroporesis)
2. atherosclerosis (ASCVD), hypertension, heart disease, stroke, CVA/stroke, PAD increases amputation
Other conditions
- Depression
- Acutely very high BG = DKA (mostly in T1DM) and HHS (mostly in T2DM)
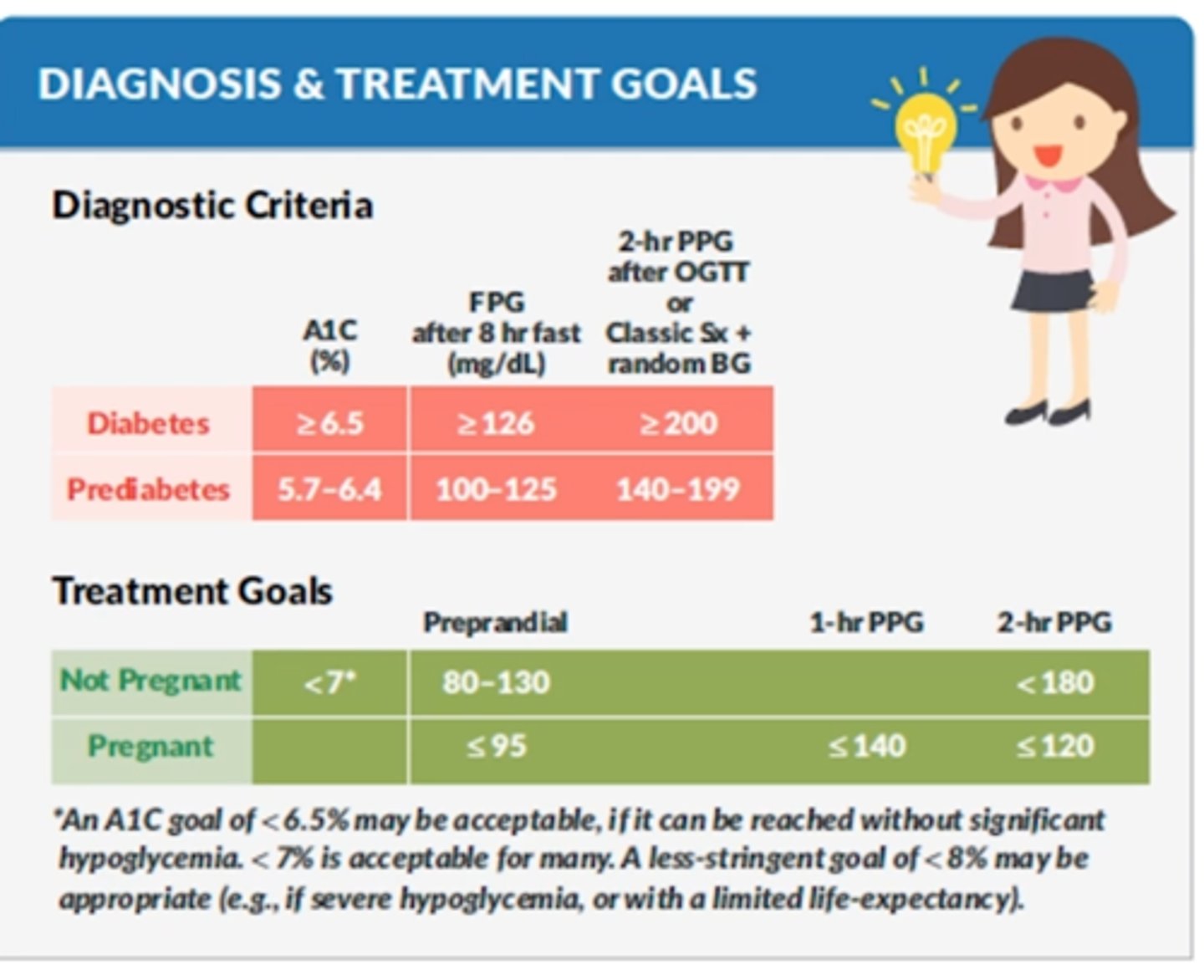
Diagnosis of
Prediabetes and Diabetes
Treatment goals
Not pregnant, Pregnant
p628 Study Tip Gal
Pre-diabetes:
FPG 100-125 mg/dL,
2-hr PG 140-199, or
A1C 5.7-6.4
Diabetes :
FPG > 126 mg/dL,
2 hour PG: > 200 mg/dL,
A1C > 6.5
require two abnormal test.
FPG= no food for 8hrs
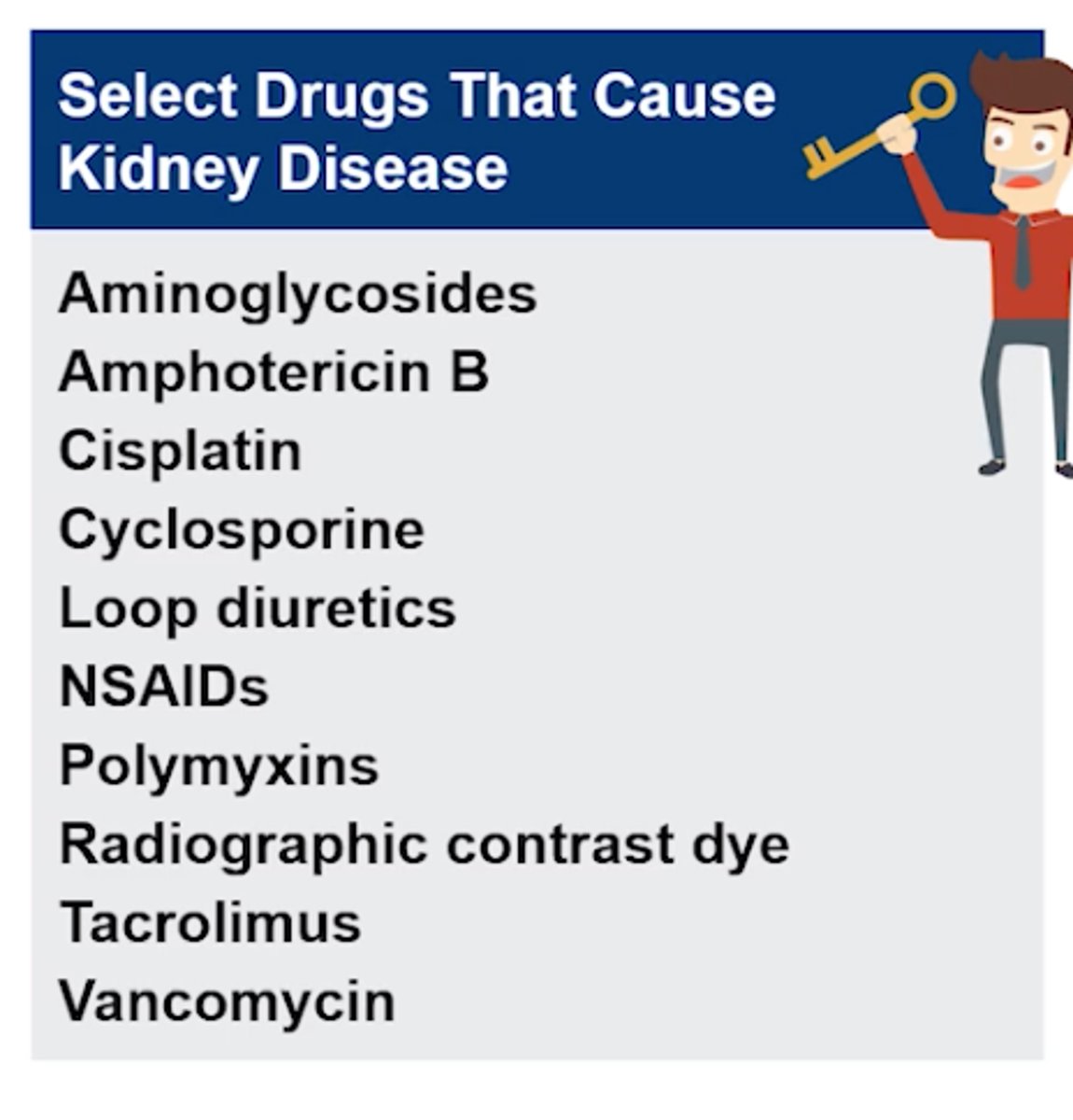
What key drugs cause Kidney Disease?
Key Drug Guy p300
+ Aminoglycosides (Tobramycin, Amikacin, Neomycin, Gentamycin, Streptomycin - TANGS)
+ Amphotericin B
+ Cisplatin
+ Cyclosporine
+ Loop diuretics (ie: Lasix-furosemide)
+ NSAIDs
+ Polymyxins (Colistin, Polymyxin B, depolarizing Daptomycin)
+ Radiographic contrast dye*
+ Tacrolimus
+ Vancomycin
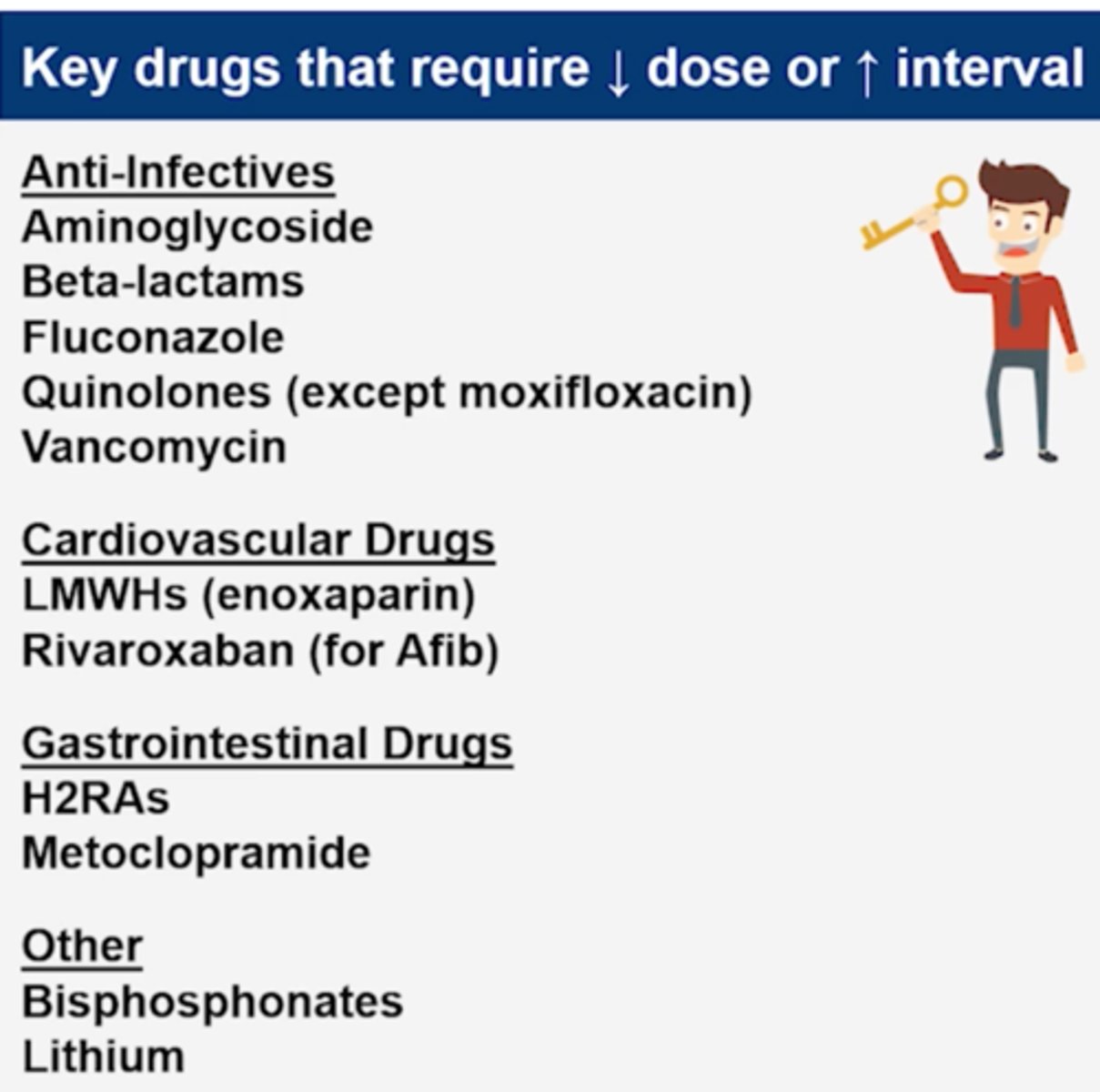
Select Drugs that Require Decrease Dose or Increase Interval in CKD?
Key Drug Guy p302
Anti-lnfectives
+ Aminoglycosides (increase dosing interval primarily - cause nephrotoxicity so give Extended interval)
+ Beta-lactam antibiotics (most, except antistaphylococcal, these are time dependent so increase dose/interval risk of seizure)
+ Fluconazole
+ Quinolones (except moxifloxacin, not cleared through kidney) - risk of seizure
+ Vancomycin (nephrotoxic)
Cardiovascular Drugs - BLEEDING RISK
+ LMWHs (enoxaparin)
+ Rivaroxaban* (for AFib)
+ Apixaban* (for AFib)
+ Dabigatran* (for AFib)
+ Fondaparinux?
Gastrointestinal Drugs
+ H2RAs (famotidine, ranitidine) - CNS effects, thrombocytopenia
+ Metoclopramide - EPS, Parkinson's like sx
Other
+ Bisphosphonates*
+ Lithium (100% excreted in kidney, can be toxic)
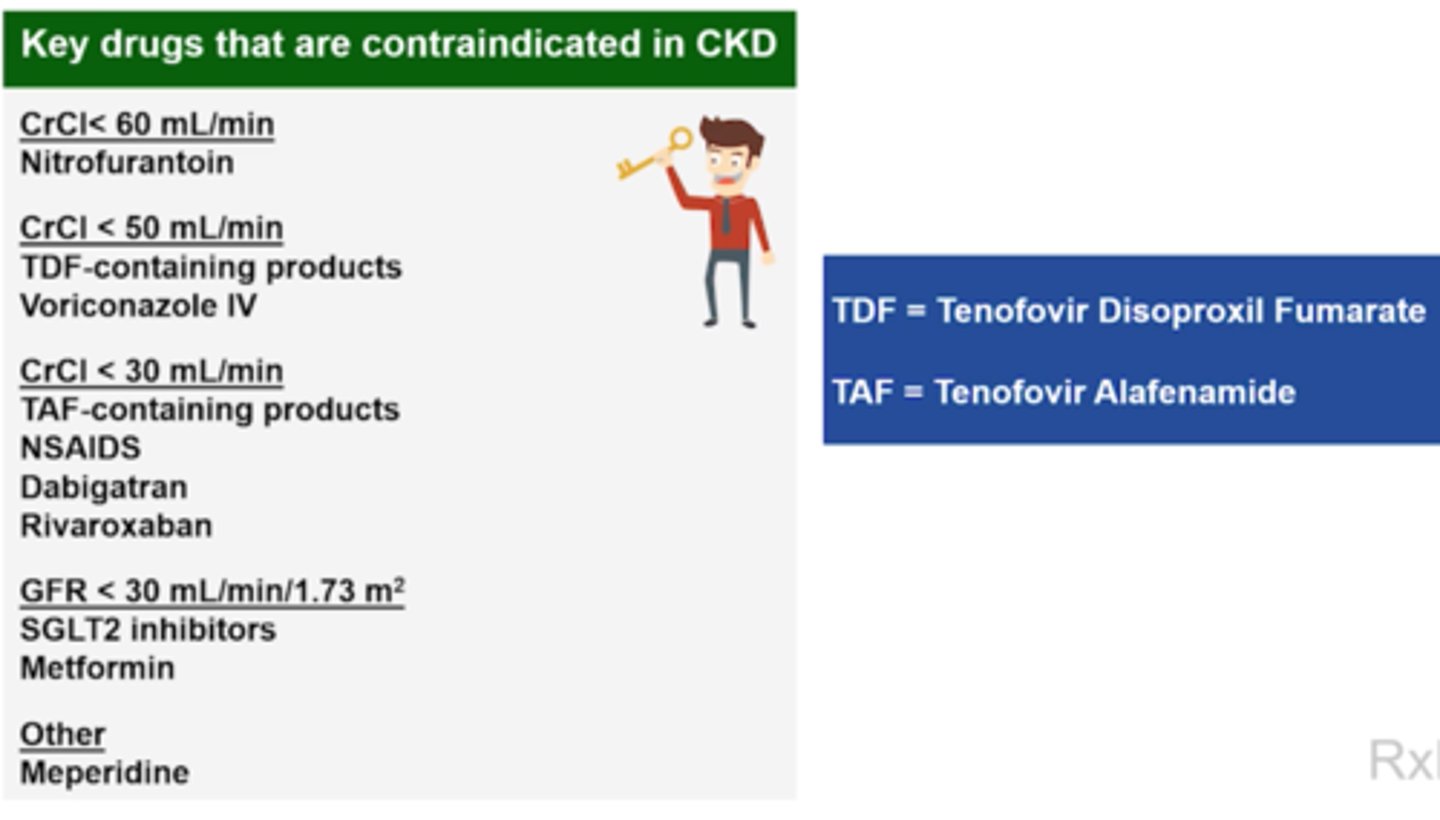
Select Drugs that are C/I n CKD
Key Drug Guy p302
CrCl < 60 mL/min
+ Nitrofurantoin
CrCl < 50 mL/min
+ Tenofovir disoproxil fumarate (TDF) containing products (e.g., Stribild*, Complera, Atripla, Symfi, Symfi Lo)
*Stribild is C/I for a patient already on drug but CrCl falls <50, C/I to START NEW at CrCl of <70
+ Voriconazole IV (due to the vehicle)
CrCl < 30 mL/min
+ Tenofovir alafenamide (TAF) containing products (e.g., Genvoya, Biktarvy, Descovy, Odefsey, Symtuza) --> TDF products better
+ NSAIDs
+ Dabigatran* (DVT/PE)
+ Rivaroxaban* (DVT/PE)
+ Fondaparinux????
GFR <30 mL/min/1.73 m2
+ SGLT2 inhibitors (canagliflozin, dapagliflozin, empagliflozin)
+ Metformin
Other***
Mepiridine
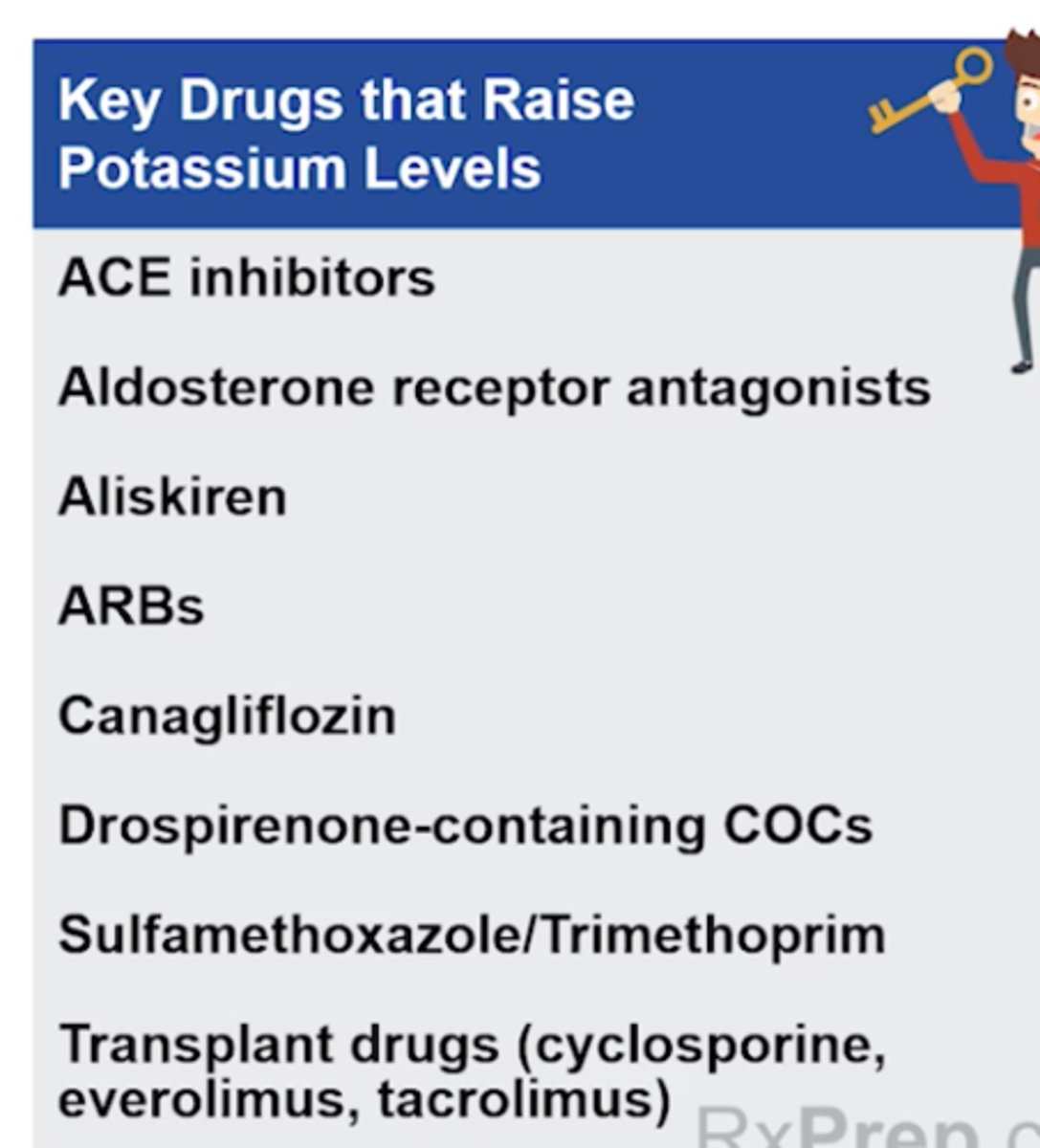
Key drugs that raise potassium levels
Key Drug Guy p306
RAAS
+ ACE inhibitors/ARBS
+ Aldosterone receptor antagonists (aldosterone, eplerenone)
+ Aliskiren (direct renin inhibitor)
+ Canagliflozin (SGLT-2i - )
+ Drospirenone-containing COCs (Yaz)
+ Sulfamethoxazole/ trimethoprim (Bactrim tx pneumocystis pneumonia)
+ Transplant drugs (cyclosporine, everolimus, tacrolimus)
Which key drugs cause liver damage?
Key Drug Guy p 317
+ Acetaminophen (high doses, acute or chronic)
+ Isoniazid
+ Ketoconazole (oral)
+ Methotrexate
+ Nefazodone
+ Nevirapine
+ NRTIs (TDF/Viread, TDA/Vemlidy, Entecavir/Baraclude, Lamivudine/Epivir HPB)
+ Propylthiouracil
+ Tipranavir
+ Valproic acid
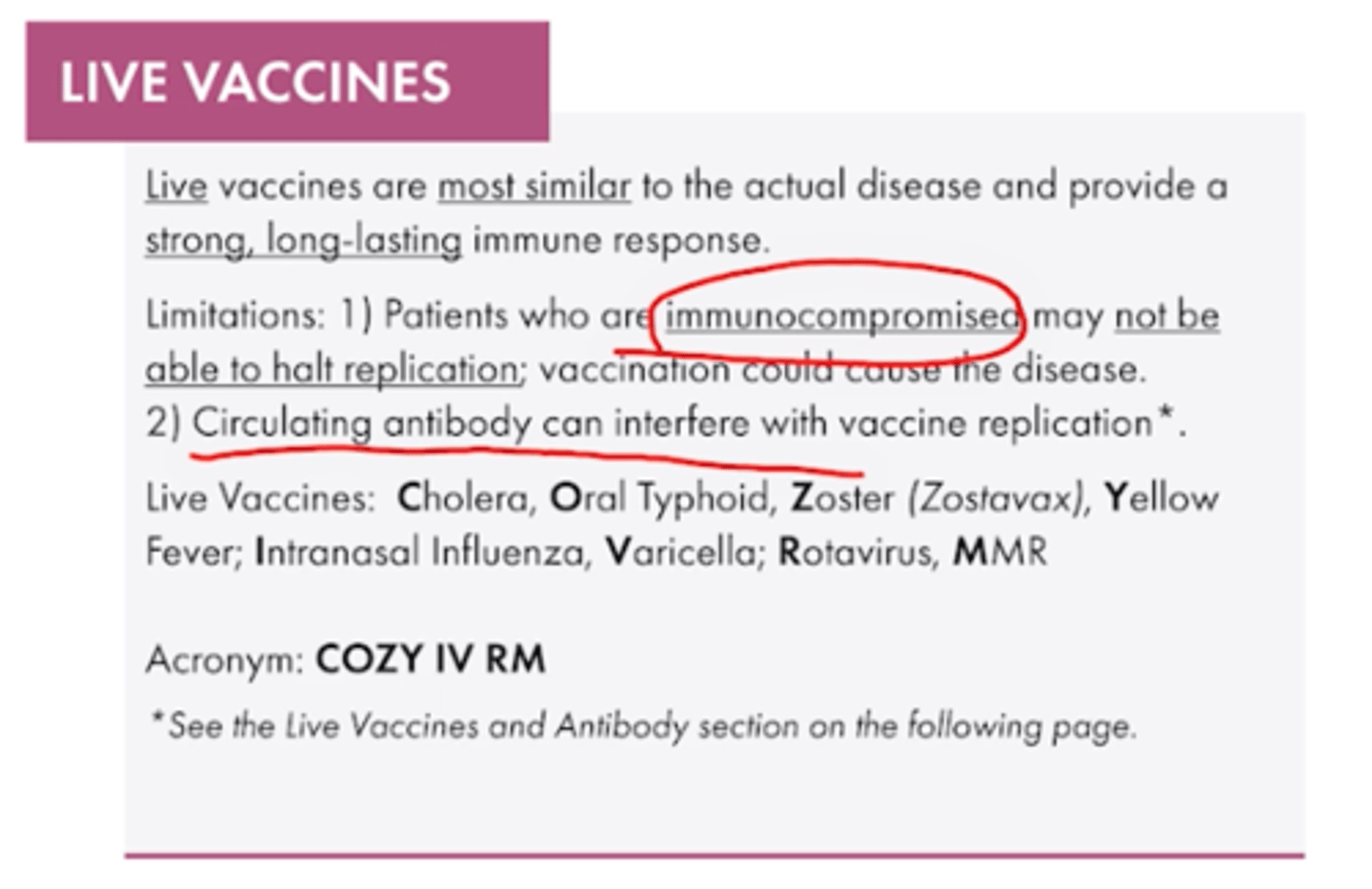
Live Vaccines
Key Drug Guy p326
COZY IV RM
Cholera
Oral Typhoid
Zoster (Zostavax)
Yellow Fever
Intranasal Influenza
Varicella
Rotavirus
MMR
Remember these are CI in immunocompromised or pregnant patients
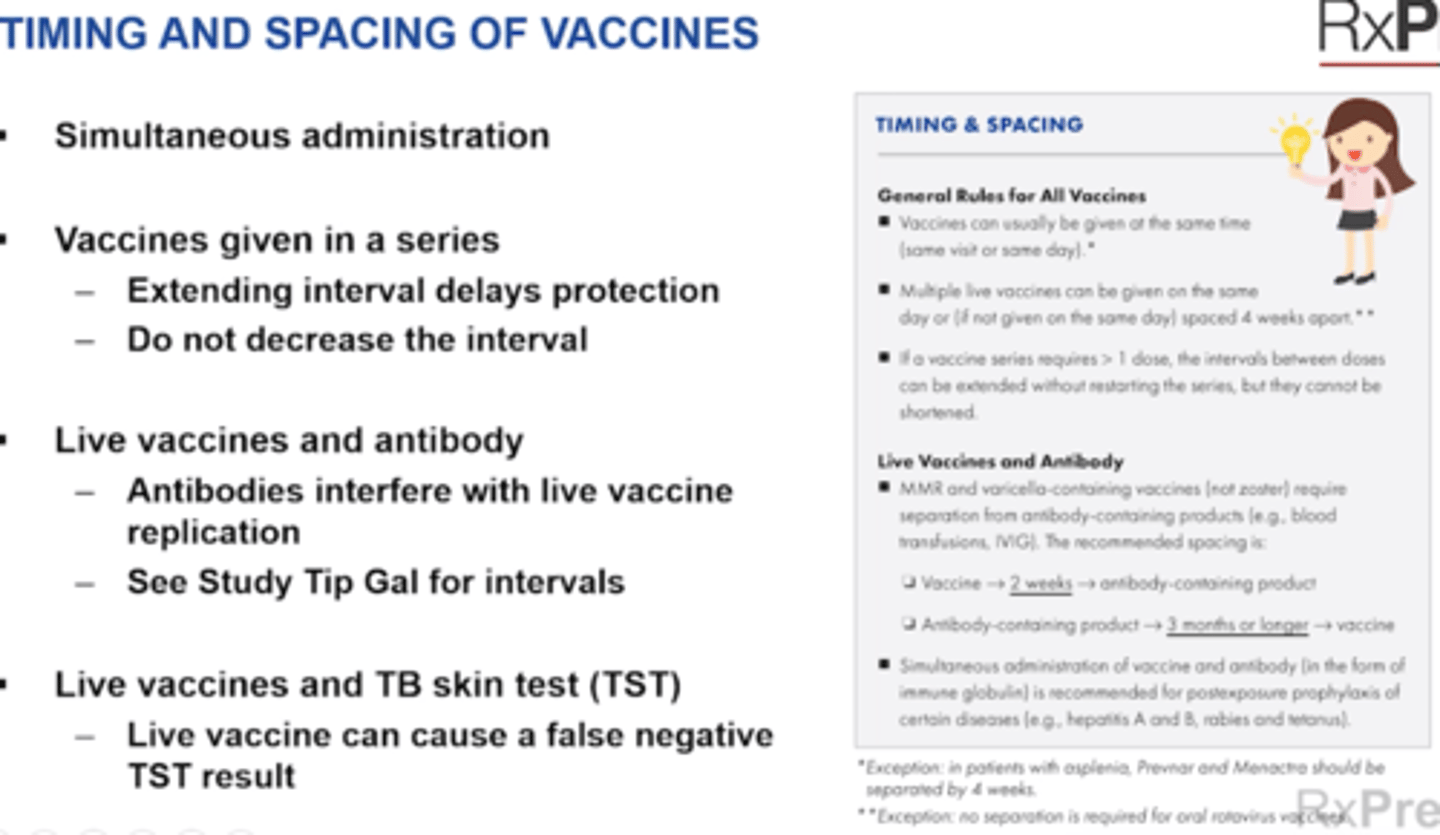
Timing and Spacing of Vaccines
Study Tip Gal p327
General Rules for All Vaccines
+ Vaccines can usually be given on same day (exception - Prevnar 13 and Menacta meningitis separate by 4 weeks)
+ Multiple live vaccines can be given on the same day (if not givn on same day then seperate by 4 weeks)
+ In series > 1 dose, intervals can be extended
Simultaneous administration - usually okay
+ Both live and inactivated (same day for live or seperate by 4 weeks)
Vaccines given in a series
+ Extending interval delays protection
+ Do not decrease the interval
Live vaccines and antibody
+ Antibodies interfere with live vaccine replication
Live vaccines and TB skin test (TST or PPD test)
+ Live vaccine can cause a false negative TST result
+ Give the live vaccine on the same day as skin test OR
+ Wait 4 weeks after live vaccine to perform skin test
Live Vaccines and Antibody
+ MMR and varicella containing vaccines (not zoster) require separation from antibody containing products (blood transfusions, IVIG).
+ Spacing: Vaccine --> 2 weeks --> antibody containing product OR
+ Spaciing: Antibody containing product --> 3 months or longer --> Vaccine
+ Simultaneous vacccine + antibody is recommended in post=exposure of certain diseases (Hep A and B, rabies, and tetanus)
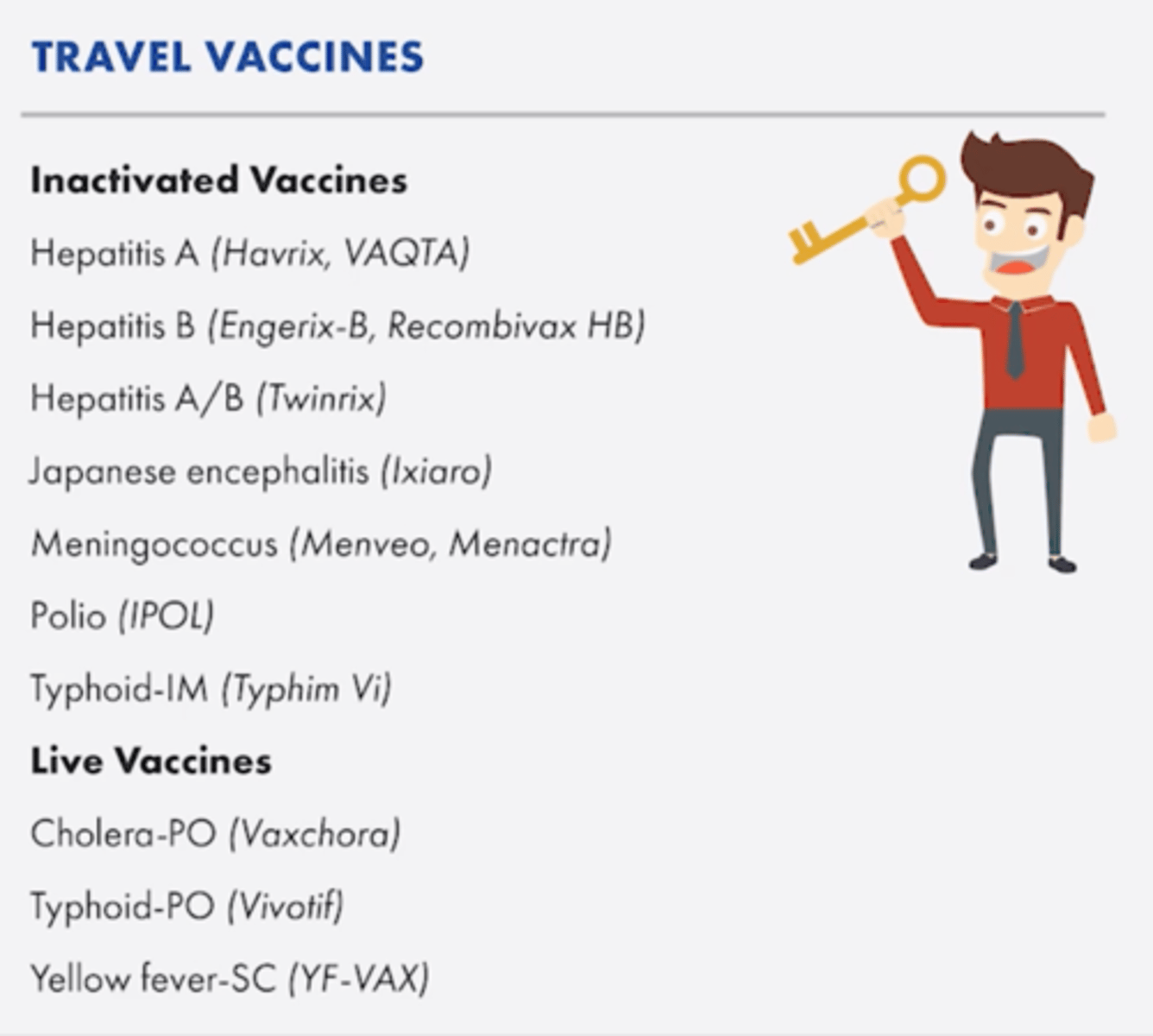
Background on Travel Vaccines
Key Drug Guy p344
Inactivated Vaccines
+ Hepatitis A
+ Hepatitis B
+ Hepatitis A/B
+ Japanese encephalitis
+ Meningococcus
+ Polio
+ Typhoid-IM
Live Vaccines
+ Cholera-PO
+ Typhoid PO
+ Yellow Fever-SC
Cholera and Typhoid are both PO
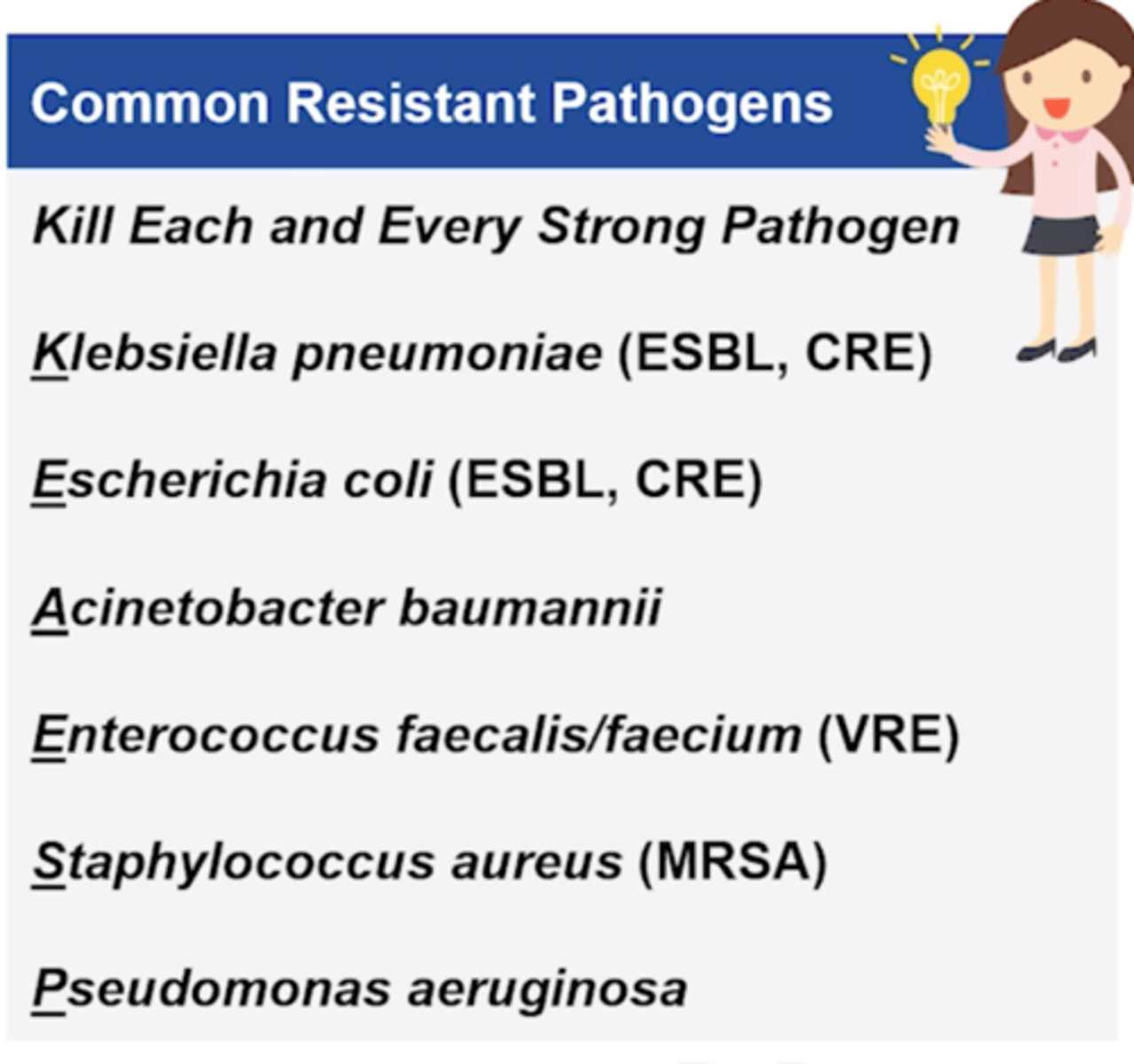
What are common resistant pathogens?
Study Tip Gal p 355
+ Klebsiella pneumoniae (ESBL, CRE)
+ Escherichia coli, (ESBL, CRE)
+ Acinetobacter baumannii
+ Enterococcus faecalis / Enterococcus faecium (VRE)
+ Staphylococcus aureus (MRSA)
+ Pseudomonas aeruginosa
Remember: Kill Each And Every Strong Pathogen
ESBL = extended-spectrum beta-lactamase
CRE= carbapenem-resistant Enterobacteriaceae
VRE= vancomycin-resistant Enterococcus
ESBL usually needs CARBAPENEM
CRE - needs polymixins
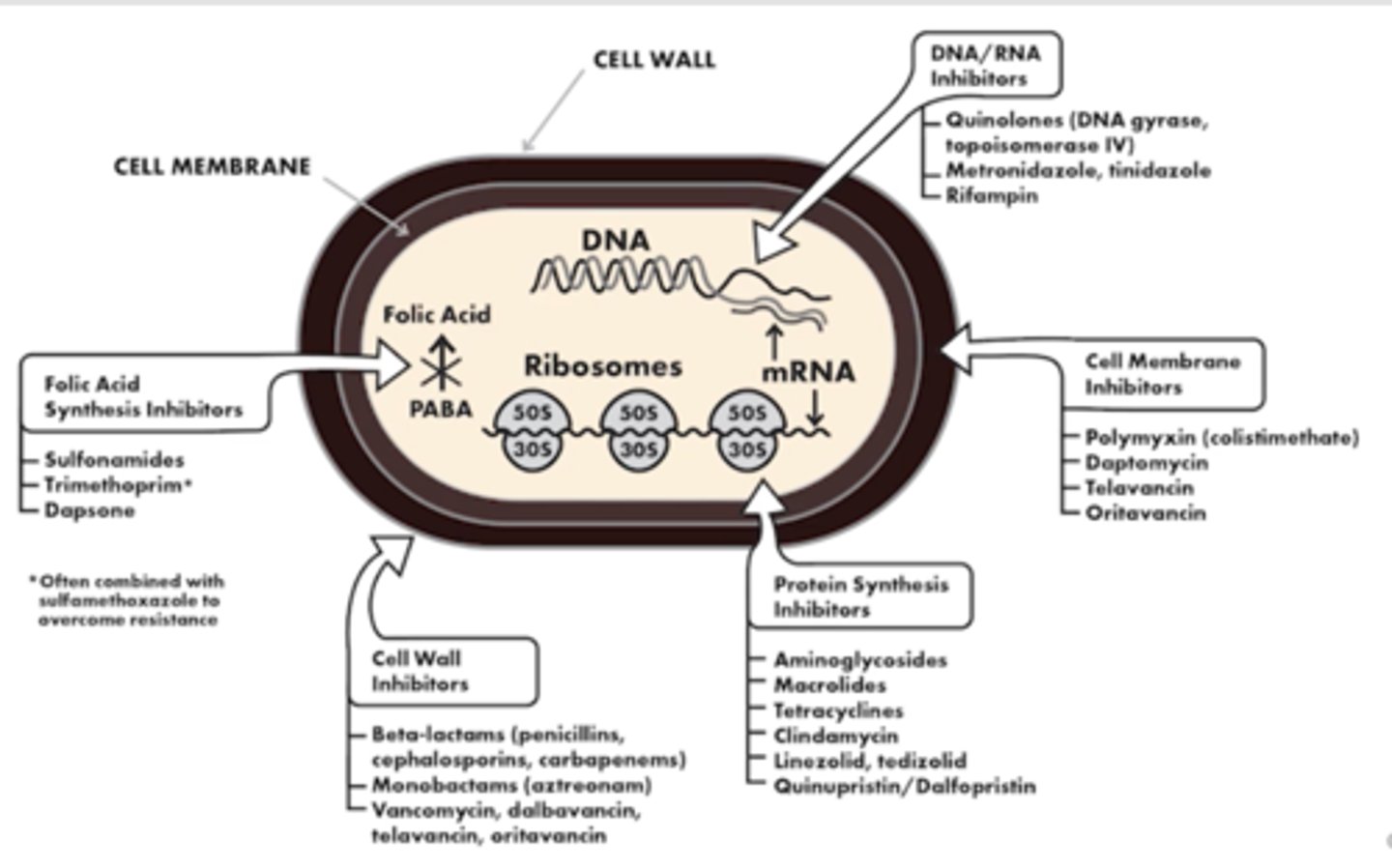
Antibiotic Mechanism of Action
1. Cell Wall Inhibitors
=
+ Beta lactams (penicillins, cephalasporins, carbapenems)
+ Monobactams (Aztreonam)
+ Vancymycin, dalbavancin, televancin, oritavancin
2. Protein Synthesis Inhibitors
+ Aminoglycosides
+ Macrolides
+ Tetracyclines
+ Clindamycin
+ Linezolid, tedizolid
+ Quinupristin/Dalfopristin
3. Folic Acid Synthesis Inhibitors
+ Sulfonamides
+ Trimethoprim (added with sulfamethoxazole to overcome resistance = Bactrim)
+ Dapsone
4. Cell Membrane Inhibitors
+ Polymiyxins
+ Daptomycin
+ telavancin
+ Oritavancin
5. DNA/RNA Inhibitors
+ Quinolones (DNA gyrase, topoiomerase IV)
+ Metronidazole, trinidazole
+ Rifampin
Key Feature of Penicillins
Study Tip Gal p359
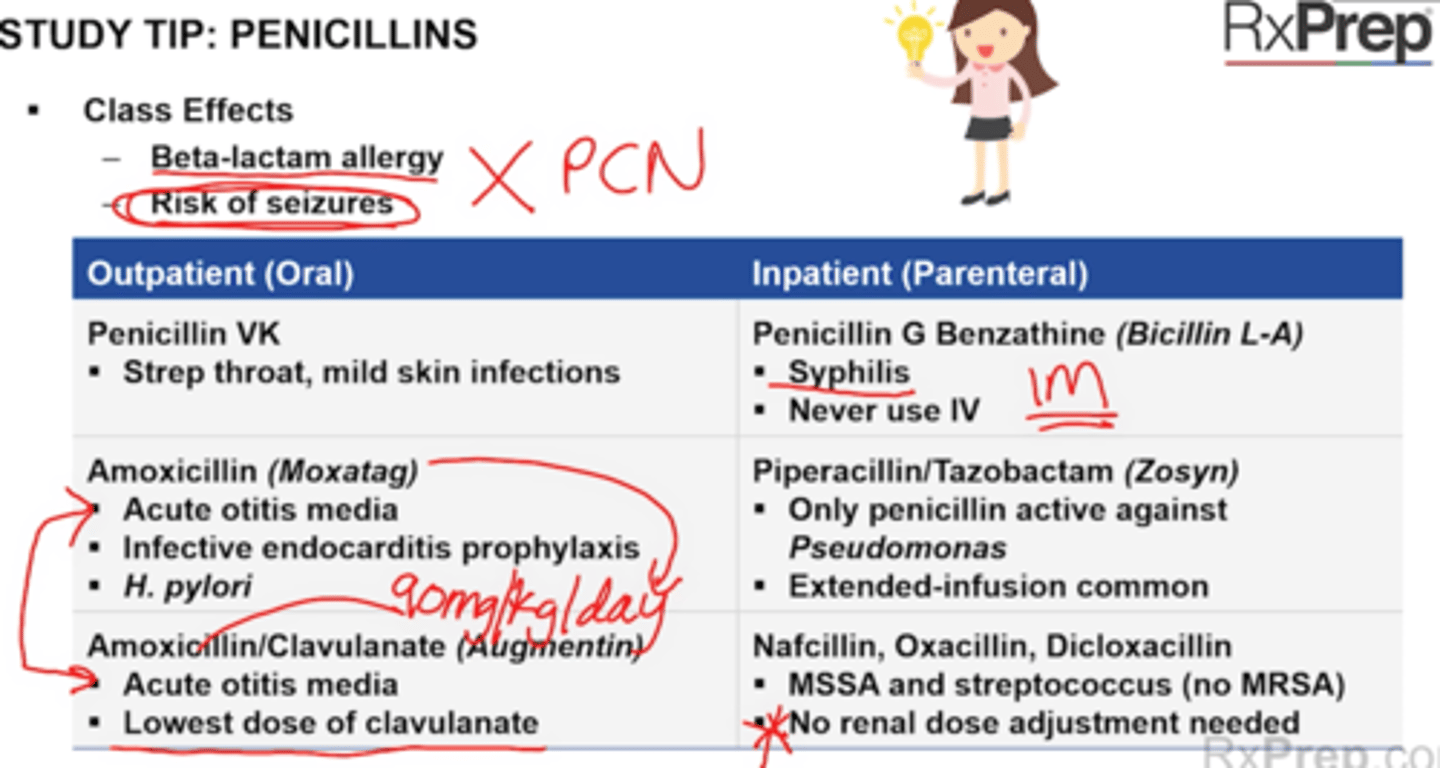
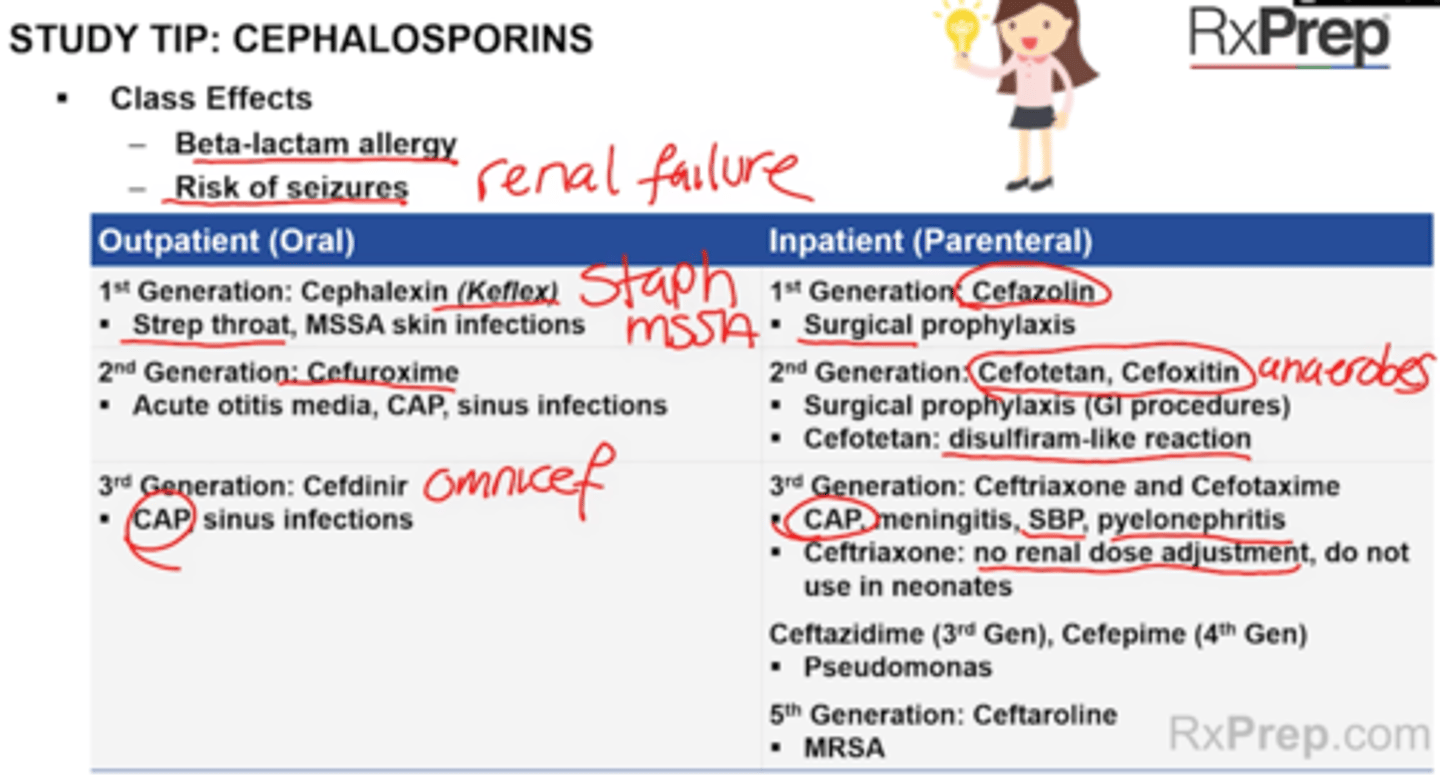
Class effects
+ All pnc should be avoided in patients with beta-lactam allergy
+ All PNC increase the risk of seizures if accumulation occurs (eg renal failure)
Outpatient (PO)
1. Penicillin VK
+ A first-line treatment for strep throat and mild nonpurulent skin infections (no abscess)
+ Strep throat, mild skin infections
2. Amoxicillin
+ Treats otitis media, infective endocarditis ppx, h. pylori
+ First line treatment for acute otitis media (80-90 mg/kg/day)
+ Drug of choice for infective endocarditis prophylaxis before dental procedure (2 g PO x1, 30-60 min before procedure)
+ Used in H.pylori treatment + PPI
3. Amoxicillin/Clavulanate (Augmentin)
+ First line treatment for acute otitis media (90 mg/kg/day) and for sinus infections (if an antibiotic is indicated)
+ Use the lowest dose of clavulanate to decrease diarrhea
4. Dicloxacillin and Oxacillin
+ Cover MSSA only (no MRSA)
+ No renal dose adjustment needed
Inpatient (Parenteral)
1. Penicillin G Benzathine (Bicillin L-A)
+ Drug of choice for syphilis (2.3 milliion units IM x1)
+ Not for IV use, can cause death - lipid emmulsion
2. Nafcilllin
+ See dicloxacillin and oxacillin above
No renal adjustment and covers MSSA only
3. Piperacillin/Tazobactam (Zosyn)
+ Only PCN active against Pseudomonas
+ Extended infusions (4 hours) can be used to maximize T > MIC
Penicillin Safety and side effects
p358
Penicillin V Potassium - PO
Penicllinin G Benzathine (Bacillinn L=A) - IM
Amoxicillin = Po, chewable, suspension
Augmentin (amox/clav) = Po, chewable, suspension
Ampicillin: injection (dilute in NS only)
Ampcillin/sulbactam (Unasyn): Injection (dilute in NS only)
Zosyn - Injection, prolonged or extened infusion over 4 hours
Nafcillin, Oxacillin - Injection
Dicloxacillin - PO
Boxed warning
+ Penicllin G benzathine - not for IV use
Contraindications
+ Severe renal impairment CrCl < 30 mL/min; do not use extended release oral forms of amoxicilllin and augmentin or 875 mg strength of Augmentin
SE:
+ Seizures (with accumulation - ie renal), GI upset, diarrhea, rash (SJS/TEN)
Notes
+ Aminopenicillins: IV ampicillin and Unasyn must be diluted in NS only
+ Antistaphylococcal Penicillins = preferred for MSSA soft tissue, bone/joint, endocarditis, and BSI
+ No renal adjustment
+ Nafcillin is a veiscant = If extravasation occurs use cold packs and hyaluronidase injections
DDI
+ Probenecid can increase levels of beta-lactams
Which abx only work with NS
Ampicillin (w/wo sulbactam Unasyn), ertapenem
Study Tip Cephalasporins
And Safety
p360
Study Tip Gal p361
Contraindications
+ Ceftriaxone: Neonates - cause biliary sludging, kernicterus (brain damage from bilirubin levels); concurrent use w/ Calcium containing IV products in neonates < 28 days old
Warnings
+ Cross sensitivity (10%) with PCN allergy - do not use in patients who have type 1 PCN allergy (agnioedema, anaphylaxis)
+ Cefotetan (Cefotan) contains a side chain --> increase risk of bleeding and cause disulfiram-like reaction
SE
+ Seizures (with accumulation), GI upset, diarrhea, rash (SAME AS PCN)
Notes
+ Ceftriaxone - no renal adjustment
+ Cefixime available as chewable tablet (3rd gen)
+ Ceftazidime/avibactam: covers some carbapenem resistant enterobaceriacae (CRE)
DDI
+ Cefpodoxime, Cefuroxime + drugs that decrease stomach acids should be separated from short-acting antacids. Avoid H2RAs and PPIs
Outpatient (PO)
1. 1st Generation: Cephalexin (Keflex)
+ Strep throat, MSSA skin infections
+ Keflex PO 250-500 mg Q6-12H
2. 2nd Generation, Cefuroxime
+ Acute otitis media, CAP, sinus infections (if abx indicated)
3. 3rd generation: Cefdinir
+ CAP, sinus infections (if abx indicated)
Inpatient (Parenteral)
1. 1st Generation: Cefazolin
+ Surgical prophylaxis
2. 2nd generation: Cefotetan, Cefoxitin
+ Surgical prophylaxis (GI procedures - colorectal)
+ Anaerobic coverage - b.fragilis
+ Cefototetan: disulfiram like reaction with alcohol = bleeding
3. 3rd Generation: Ceftriaxone and Cefotaxime
+ CAP, meningitis, SBP, pyelonephritis
+ Ceftriaxone: No renal adjustment, do not use in neonates 0-28 days old (biliary sludge)
4. Ceftazidime (3rd generation), Cefepime (4th Gen)
+ Pseudomonas
5. 5th Generation: Ceftaroline (Teflaro)
+ only beta lactam active against MRSA
6. Ceftolozane/Tazobactam and Ceftazidime/Avibactam (3rd gen)
+ used for MDR Gram negative organisms (Including pseudomonas)
dose: keflex
Cephalexin (Keflex)
PO 250-500 mg Q6-12 H
MSSA skin infections, strep throat
p360
Carbapenems
Safety
Study Tip Gal p363
Reserved for MDR Gram negative infection
+ They are active against most Gram + and gram neagative (including ESBL-producing bacteria) and anaerobic pathogens
+ No coverage of atypical pathogens, MRSA, VRE, Cdif, and stenotrophomonas
Drugs
Doripenem
Imipenem
Meropenem (Merrem)
Ertapenem (Invanz)
CI
+ Anaphylactic rx to beta lactam antibiotics
Warning
+ Do not use in patients with PCN allergy
+ CNS AEs - seizures
SE
+ Diarrhea, rash, seizures with high doses (like PCN)
Notes
+ Imipenem is combined with cilastatin to prevent drug degredation
+ Ertapenem has no coverage of Pseudomona, Acinobacter, or Enterococcus (PEA)
Class Effects
+ ESBL-producing organisms (extended beta lac)
+ All except Ertapemen cover Pseudomonas
+ Do not use with penicillin allergy
+ Seizure risk (higher doses, renal failure, or use of imipenem)
+ All are IV only, MUST USE normal saline NS for Ertapenem
DO NOT COVER
+ Atypicals, VRE, MRSA, Cdif
+ ErtAPenem does not cover PEA (Pseudomonas, Acinobacter, or Enterococcus)
Common uses
+ Polymicrobial infections (moderate-severe diabetic food infection)
+ Empiric therapy when resistant organisms suspected, MDR
+ Resistant Pseudomonas or Acinobacter infection (except ertapenem)
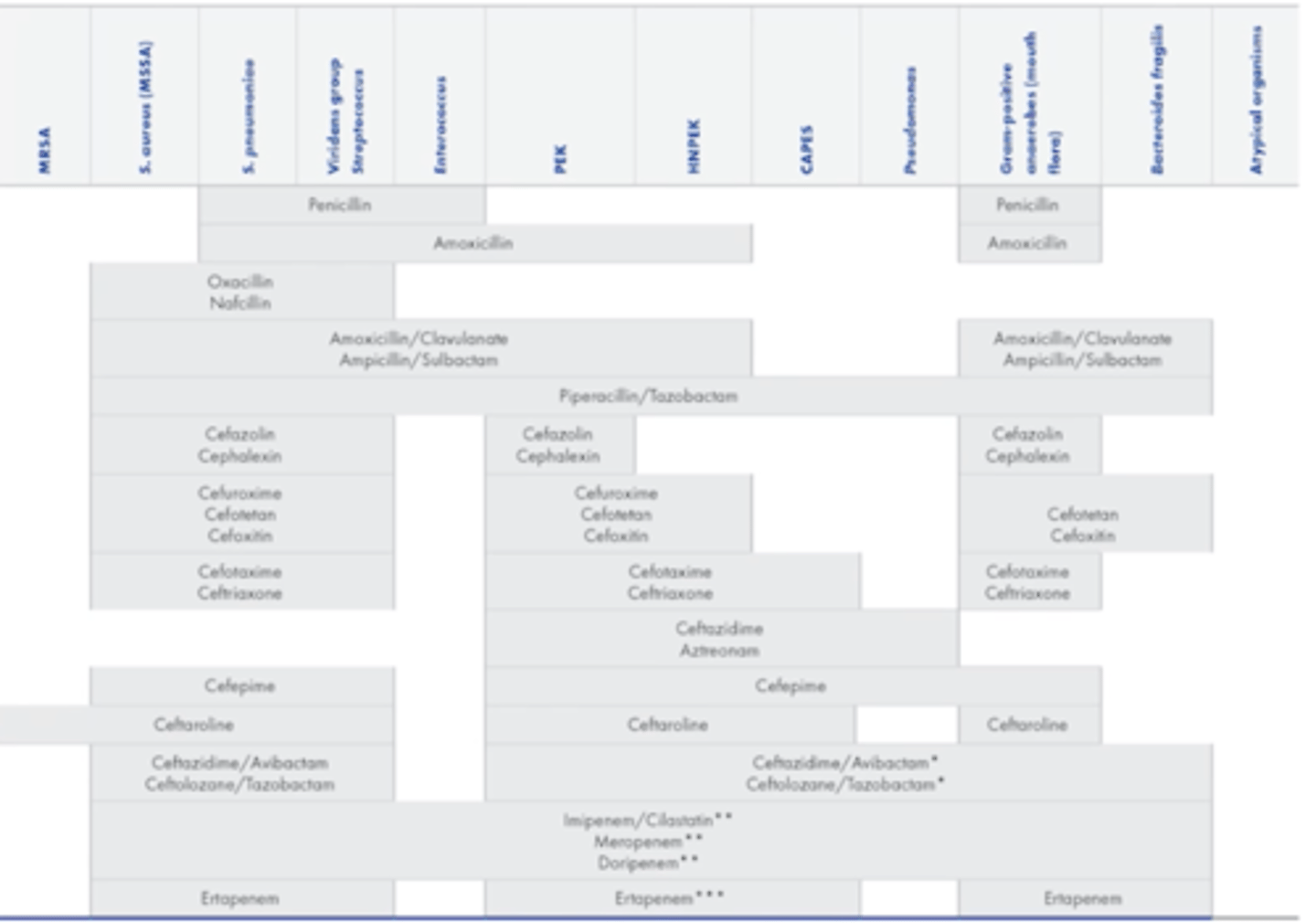
ABX antibiotic Spectrum of Activity Summary
p 363
Beta lactam that cover pseudomonas
+ Cefepime
+ Ceftazidime
+ Aztreonam
+ Carbapenems (imipenem, doripenem, meropenem only Not ertapenem)
+ Ceftazidime/Avibactam and Ceftolozane/Tazobactam
Coverage of Aminoglycoside
What are the two dosing strategies of aminoglycosides?
Monitoring
Study tip gal p364
Coverage
+ Gram negatives, including pseudomonas
+ Synergy for Gram-positives (staphyloccci/Enterococci)
Dosing Strategy
1. Traditional - use lower doses more frequently (q8h if renal function normal)
= Trying to get peaks and troughs
2. Extended interval dosing uses higher doses (to attain higher peaks) less frequently (Q24 hr)
= Draw a random level and use nomogram
= Less accumulation = less nephrotoxicity and decrease cost
Monitoring
+ Renal function, serum levels
Study Tip Gal
Pros
+ Kills gram negatives, synergistic with beta=lactams for gram positive infections, low resistance and cost
Cons
+ Highly toxic - renal toxicity and ototoxicity (require monitoring)
Smart Idea
+ Concentration dependent killing (Cmax:MIC) --> give larger doses less frequently -- gives kidneys time to recover between doses
High peak, low trough
Coverage of Aminoglycoside
What are the two dosing strategies of aminoglycosides?
Monitoring
Study tip gal p364
Drugs - All are basically IV and IM
Gentamicin
Tobramycin
Amikacin
Dosing
+ If underweight (
Trough: 30 min before 4th dose (<2 mcg/mL)
Peak: 30 minutes after end of 30 min drug infusion of 4th dose (5-10 mcg/mL)
Tobramycin/Gentamicin
Extended interval dosing: 4-7 mg/kg/dose
Draw random level
Aminoglycosides
Monitor: drug levels, renal function, hearing
Boxed warning - nephrotoxicity, ototoxicity
Caution in elderly, impaired renal function, taking other nephrotoxic drugs (amphotericin B, cisplatin, polymyxins, cyclosporin, loop diuretics, NSAIDs, Radiocontrast dye, vancomycin, tacrolimus
Trough of Gentamicin and tobramycin
< 2 mcg/mL
That is what causes the toxicity so want to know this!!!
If higher than want to hold the dose and give dose less frequently
So traditional dosing is q8h if CrCl > 60
Aminoglycosides
Safety
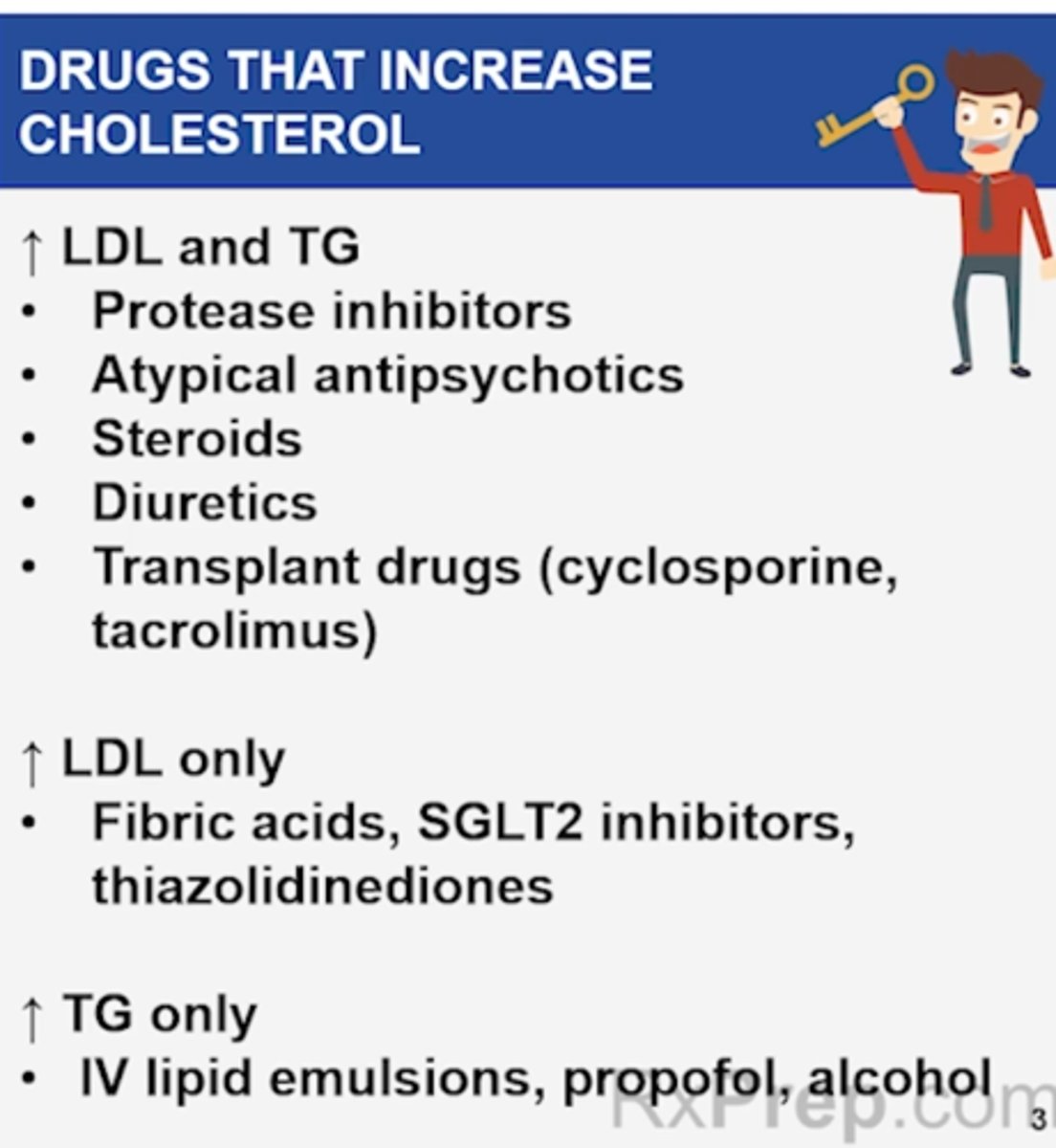
Drugs that increase LDL AND TG
+ Diuretics (loop, thiazides)
+ Steroids
+ Efavarienz (HIV tx)
+ Immunosuppresants (cyclosporine, tacrolimus)
+ Atypical antipsycotics (ie: Clozapine, asenapine, olanzapine, quetiapine, paliperidone, risperidone, sertindole, ziprasidone, zotepine, and aripiprazole)
+ Protease inhibitors (-navir)
Increase LDL Only
+ Fish oils (except Vascepa)
Increase TG Only
+ Propofol
+ IV Lipid emulsions
+ Clevidipine (DHP CCB)
+ Bile Acid Sequestrants (Colesevelam - Welchol, Cholestyramine)
Conditions
+ Obesity
+ Poor Diet
+ Hypothyroidism
+ Alcoholism
+ Smoking
+ Diabetes
+ Renal/liver disease
+ Nephrotic syndrome
Quinolones Safety
Study Tip Gal p 367
Ciprofloxacin (Cipro)
+ dexamethasone (Ciprodex)
Levofloxacin (Levaquin)
Moxifloxacin (Avelox)
Ofloxacin (Ocuflox)
Concentration dependent kill
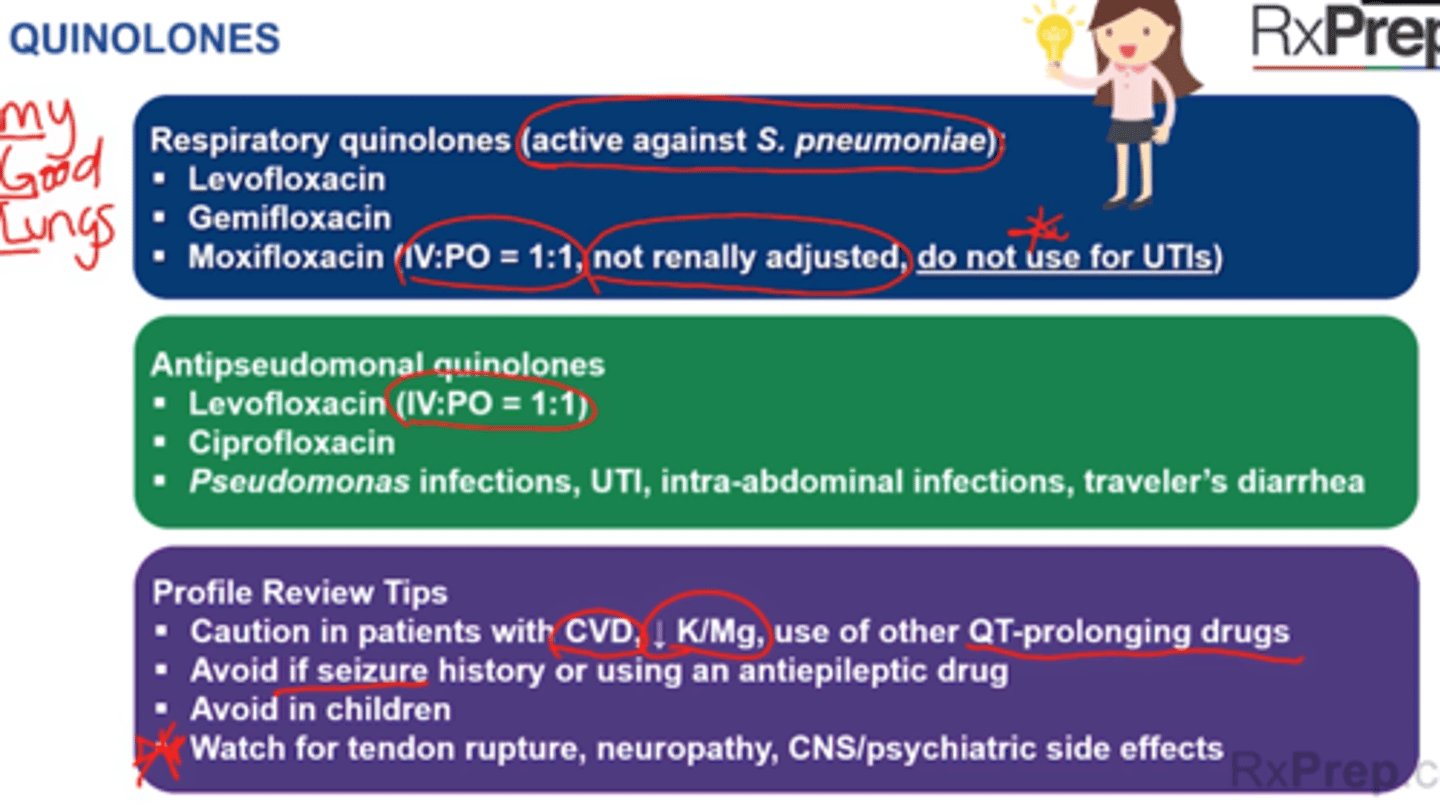
Gemifloxacin, Levofloxacin, and Moxifloxacin are respiratory quinolones - enhanced coverage of S pneumoniae and atypical coverage
+ (My Good Lungs) = Moxifloxacin (Avelox), Gemifloxacin, Levofloxacin (Levaquin)
+ Ciprofloxacin (Cipro) + Levofloxacin = enhanced gram negative & Pseudomonas coverage
+ Moxifloxacin = enhanced gram positive, anaerobic coverage. Moxi is the ONLY FQ CANNOT be used in UTI
+ Delafloxacin - MRSA activity, other
Boxed warnings
+ Tendon rupture (Achilles)
+ Peripheral neuropathy (long lasting)
+ CNS effects (including seizures)
+ Use last-line (only if no alternatives)
Warnings (MANY!)
+ QT prolongation
+ Hypo and hyperglycemia
+ Psychiatric disturbances (agitation, disorientation, delirirum, etc)
+ Photosensitivity
+ Avoid use in children and pregnancy/breastfeeding - musculoskeletal toxicity
Interaction
+ Chelation with divalent cations
Boxed warning
+ Tendon inflammation and/or rupture
+ Peripheral neuropathy
+ CNS - seizures
+ Caution in patients with CNS disorders or drugs that cause seizures
+ Caution in elderly
Notes
+ Cipro PO suspension - shake before use. DO NOT put through NG or other feeding tube (oil-based)
+ Moxifloxacin cannot reach urine - don't use in UTIs
DDI
+ Lanthanum and sevelamer (Renvela) dereases PO quinolone concentration
+ Caution in CVD because lower K and Mg and other QT prolonging drugs
+ Antacids and other polyvalent cations (Mg, aluminum, Ca, Fe, Zn) - can chelate and inhibit quinolone absorption
Macrolides
Study Tip gal p368
50S ribosomal subunit - RNA inhibitor
Coverage: atypicals, community-acquired respiratory tract infections, STIs - chlamydia, gonorrhea
Agents
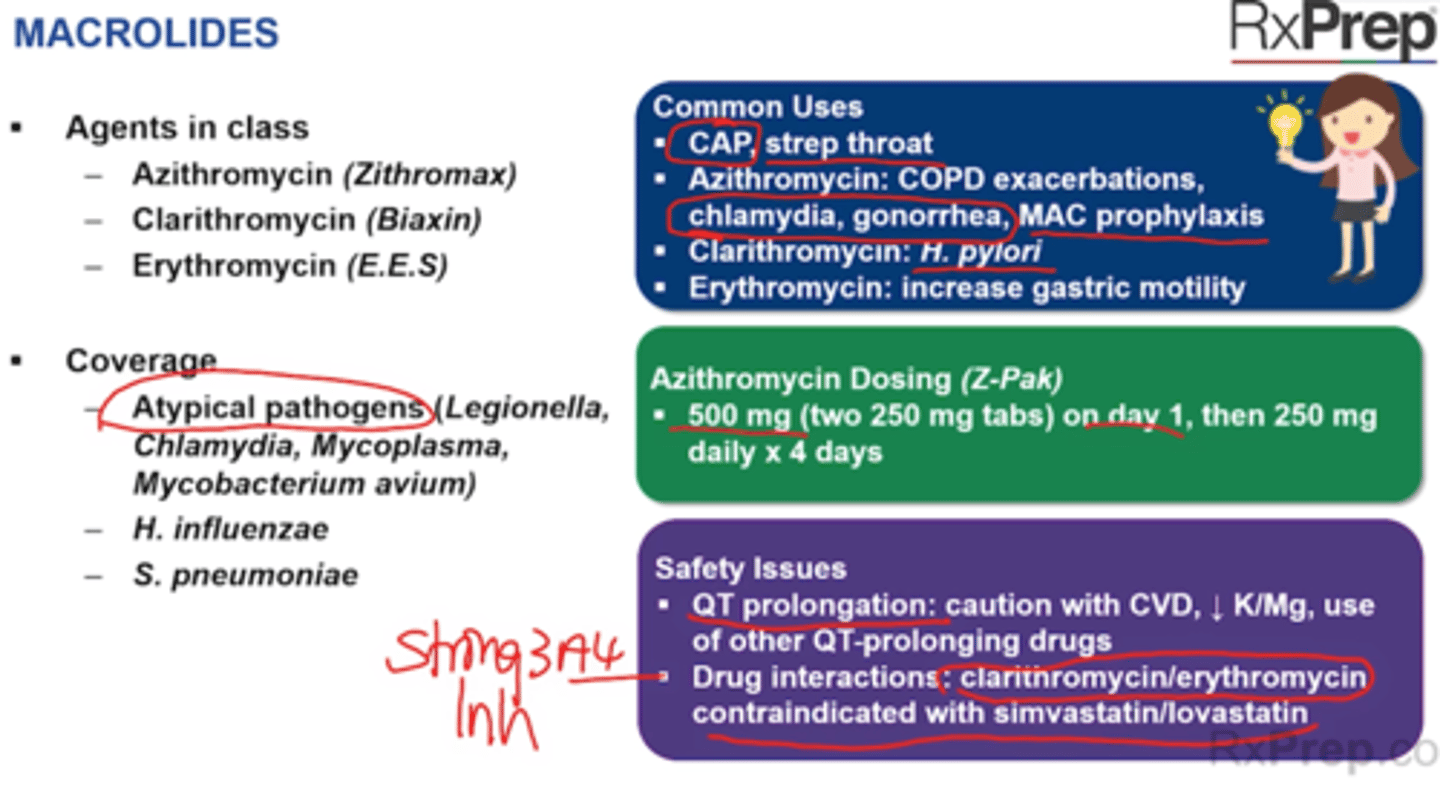
+ Azithromycin (Zithromax, Z-Pak)
Z-pak: 500 mg on day 1 then 250 mg on days 2-5
Tri-pak: 500 mg daily for 4 days
+ Clarithromycin (Biaxin)
+ Erythromycin (E.E.S., Ery-Tab, Erythrocin)
Coverage
+ Atypical pathogens (Legionella, Chlamydia, Mycoplasma, Mycobacterium avium)
+ H. influenzae (respiratory)
+ S pneumonia (resp track)
Common Uses
+ CAP, Strep throat
+ Azithromycin: COPD exacerbation, chlamydia, gonorrhea, MAC prophylaxis
+ Clarithromycin: H. pylori (GERD)
+ Erythromycin: increases gastric motility
Safety Issues
+ QT prolongation
+ Drug interactions: clarithromycin/erythromycin CI with simvastatin/lovastatin = Strong 3A4 Inhibitors
+ Azithromycin is minor substrate = less clinically significant drug interactions
+ Hepatotoicty
+ CAD + Clarithromycin = mortality higher in 2+ weeks of treatment
SE:
+ GI Upset
Tetracycline
Study Tip Gal 369
30S ribosomal subunit protein synthesis inhibition
Cover atypicals*
Agents in Class
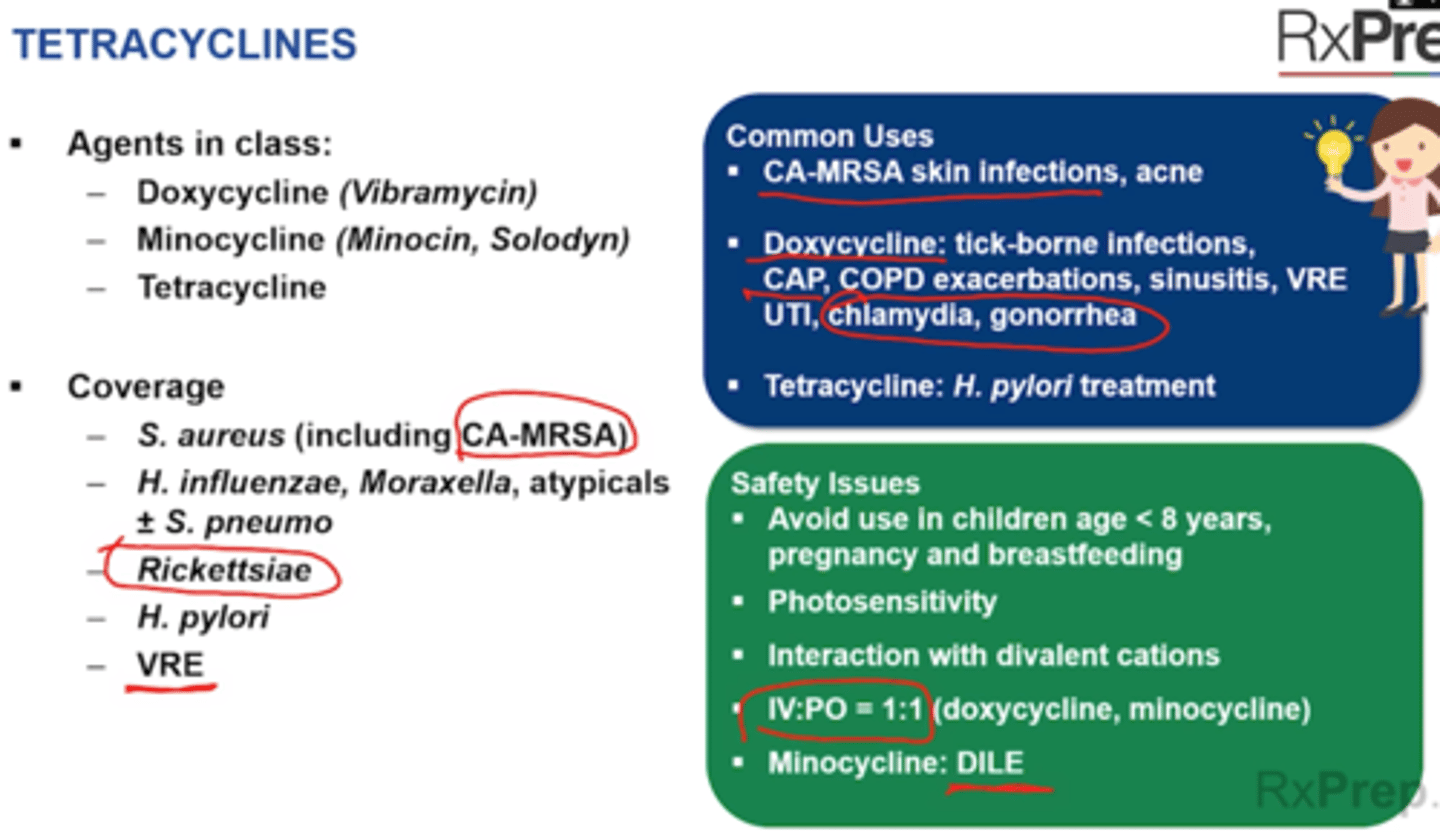
+ Doxycycline (Vibramycin)
+ Minocycline (Minocin, Solodyn)
+ Tetracycline
Coverage
+ S. aureus (including CA-MRSA)
+ H influ + S. pneumo
+ Richettsiae (Lyme disease, rocky mountain)
+ H. pylor
+ VRE
Doxycyciline
+ No dose adjustment in renal impairment
Common uses
+ Ca-MRSA skin infections, acne
+ Doxycycline: tick-borne infections, CAP, COPD exacerbations, sinusitis, VRE UTI, chlamydia, gonorrhea
+ Tetracycline: H. pylori treatment
Warning
+ Children < 8 years old, pregnancy, breastfeeding
+ Photosensitivity
+ Minocycline = DILE
Notes
+ IV:PO ratio is 1:1 (doxy and minocycline)
+ Doxycycline sit upright for at least 30 minutes after taking to avoid esophageal irritation
DDI
+ Antacids - polyvalent cations (Mg, Al, ), sucralfate, bismuth subsalicylate, bile acid resins can chelate and inhibit tetracycline absorption
Sulfonamides Safety
Study Tip Gal 370
Inhibition of bolic acid pathway
Covers Shingella, Salmonella, Stenotrophomonas, opportunistic pathogs (Penumocytis PCP pneumonia, Toxoplasmosis)
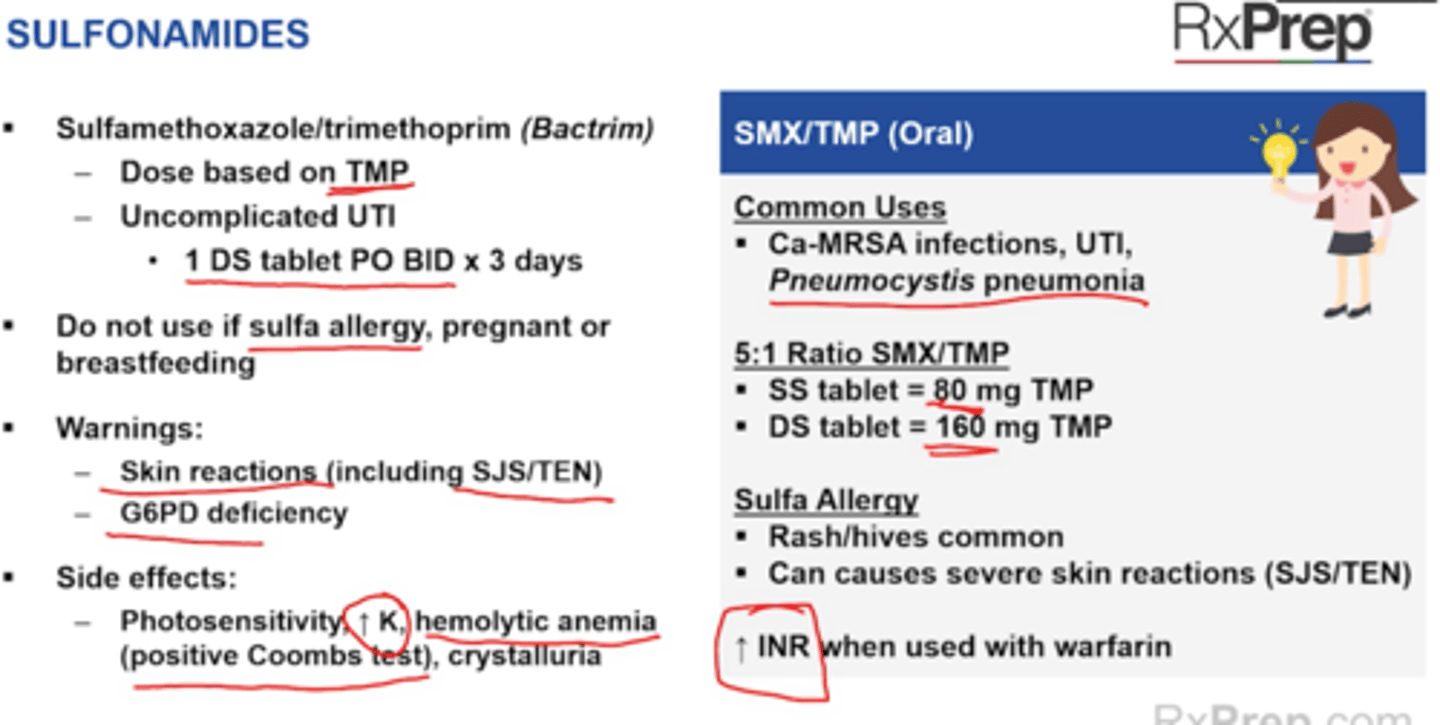
Sulfamethoxazole/trimethoprim (Bactrim)
+ dose based on TMP = 5:1 SMX:TMP ration, SS = 80 mg TMP, DS = 160 mg TMP
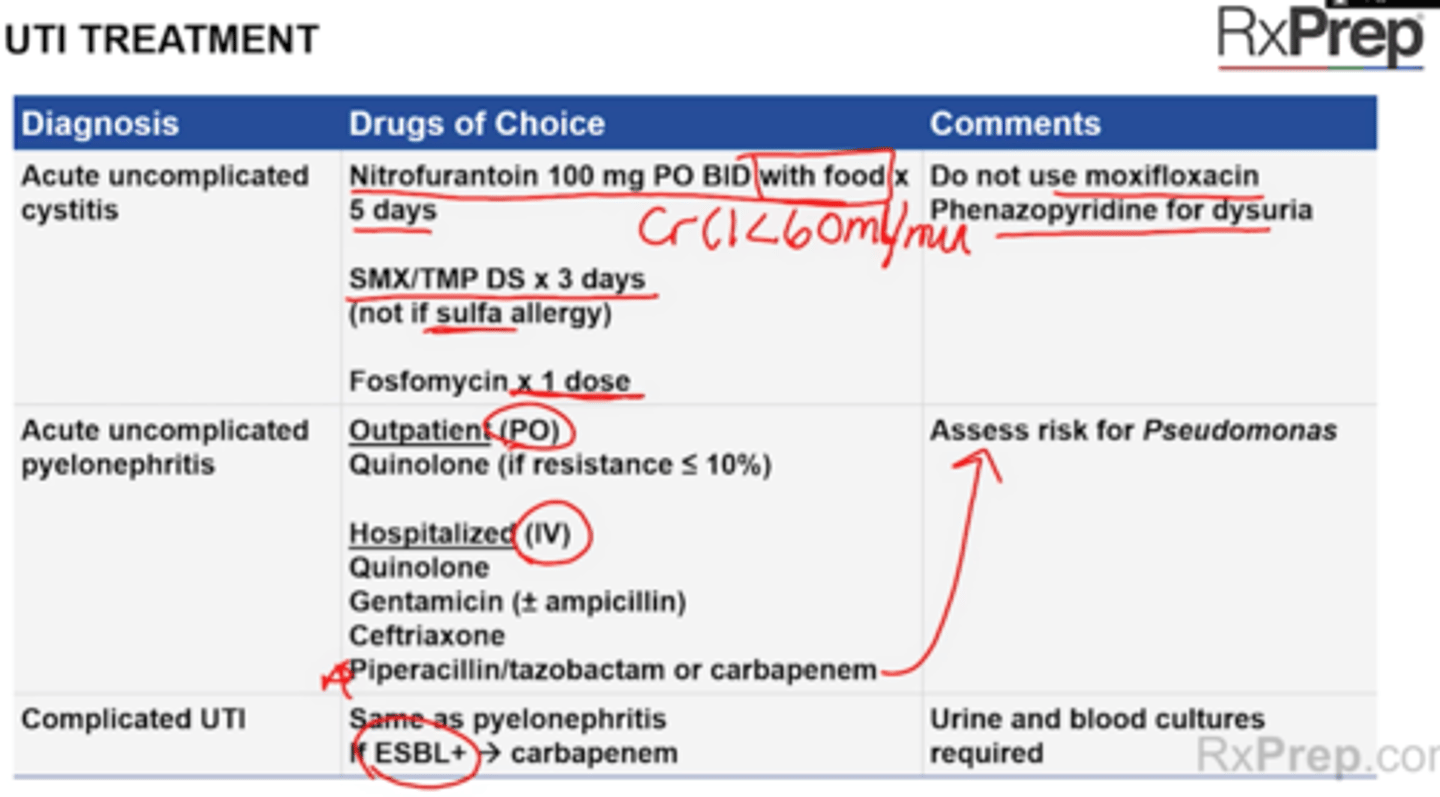
+ Uncomplicated UTI = 1 DS PO BID x3 days
Do not use if sulfa allergy, pregnant or breastfeeding
Warnings
+ Skin reactions (including SJS/TEN)
+ TTP
+ G6PD deficiency
Side effects
+ Photosensitivity, Increase K, hemolytic anemia (positive Coombs test), crystalluria, rash risk, take with water 8oz
Interactions
+ CYP2C9 - increase INR with warfarin
+ Levels of bactrim can be lowered by CYP2C9 inducers
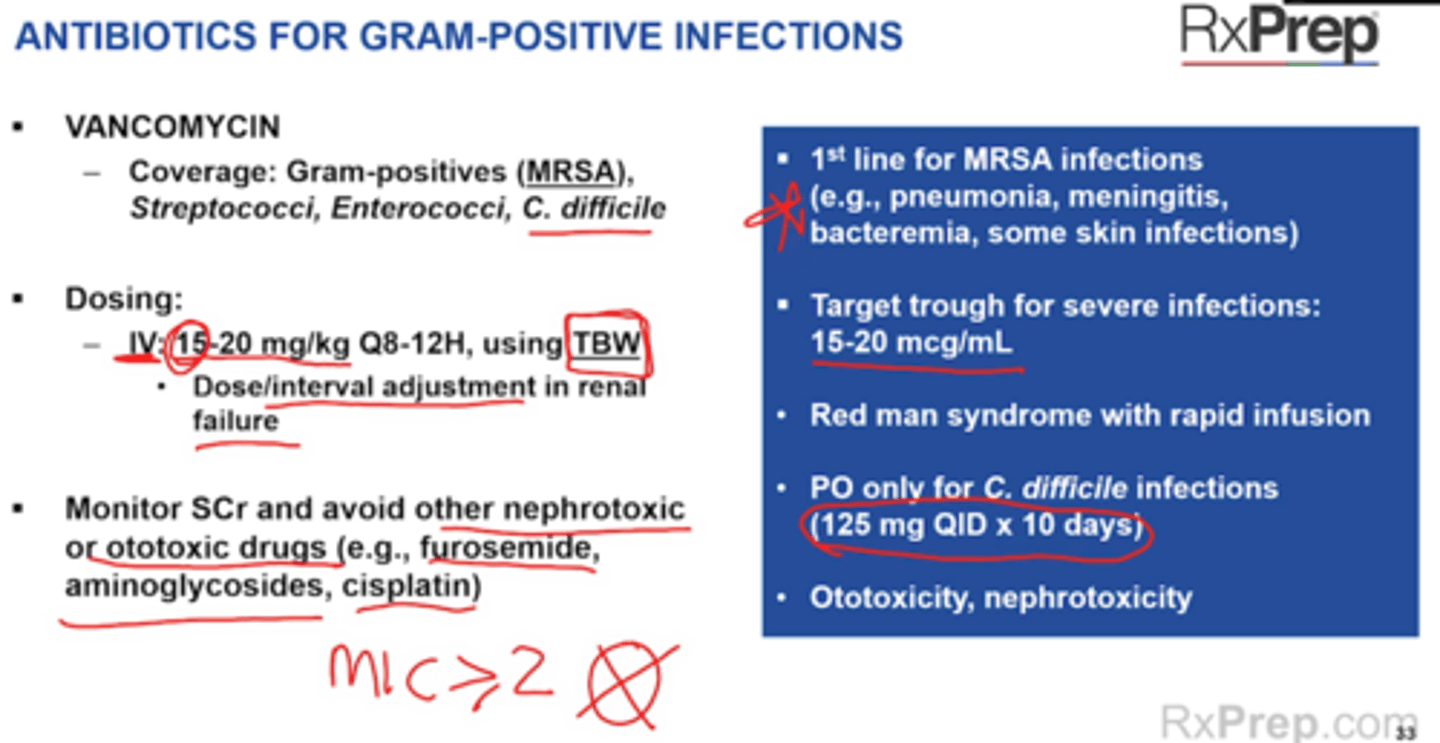
Vancomycin
Study Tip Gal 370
Vancomycin (Vancocin)
Inhibits bacterial cell wall synthesis binding to D-Ala-D-Ala
Good for MRSA, Cdif (PO route)
First line tx treatment for MRSA infections
Consider alternative drugs when MRSA MIC > 2mcg/mL
Dosing
IV Systemic infections: 15-20 mg/kg Q8-12H
--> TBW
CrCl 20-49 = Q24h
Cdif PO only
PO: 125-500 mg QID x 10 days
Warnings
+ Ototoxicity, nephrotoxicity
+ PO only for C.dif, not for systemic infections
+ Infusion rxn = red man syndrome in rapid infusion
Monitoring
+ Renal Function SCr, AUC/MIC ratio or trough
+ Serious MRSA infections - target AUC/MIC ratio of 400-600 or goal trough of 15-20 mcg.mL
Monitor SCr and avoid other nephrotoxic and ototoxic drugs
DDI
+ Increased nephrotoxicity with other nephrotoxic drugs (aminoglycosides, amphotericin B, cisplatin, cyclsporin, Vancomycin, tacrolimus, Radiocontrast dye, polymixins , nsaids, loop diuretics)
+ Ototoxic drugs - Aminoglycosides, cisplatin, loop diuretics, Asa (tinnitus)
Lipoglycopeptides
Study Tip Gal p371
Telavancin, oritavancin, dalbavancin
Work on the D-alanyl-D-alanine
Coverage: Similar to IV vanco
Approved for skin infections (SSTI)
- Televanced approved for HAP/VAP
Can ALL CAUSE RED MAN SYNDROME
Oritavancin and dalbavancin are single-dose regimens (stay in system for long time)
Boxed warning
+ Televancin: Fetal risk; nephrotoxicity, increased mortality compared to vanco in pneumonia in patients with CrCl < 50 mL/min
Contraindications
+ Televancin concurrent use of IV UFH, falst aPTT/PR/INR
+ Oritavancin: Use of IV UFH for 5 days after --> can falsely increase PT/INR for up to 12 hours and aPTT for up to 5 days
SE:
+ Infusion reaction (red man syndrome)
Notes
+ Dalbavancin, Oritavancin = singledose regimen for both, have long half life
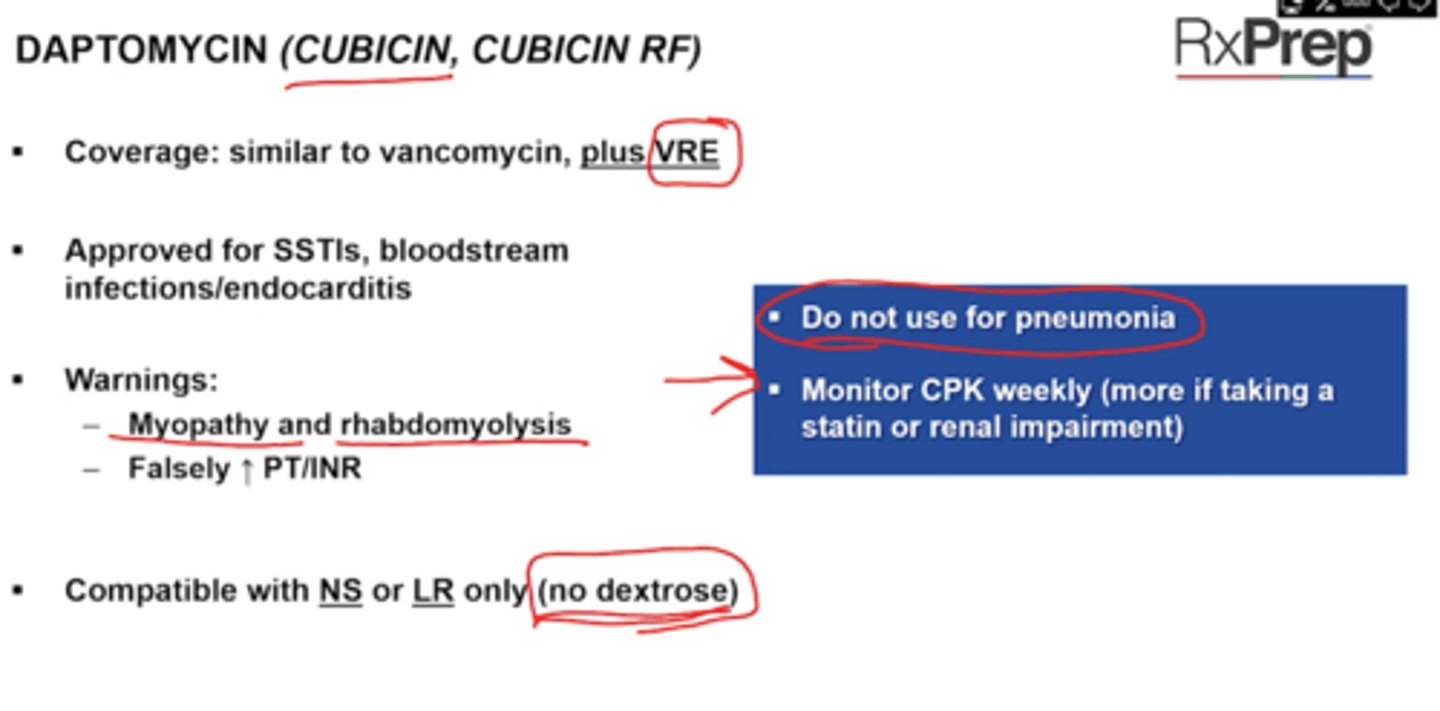
Daptomycin
Study Tip Gal p372
Daptomycin (Cubicin, Cubicin RF)
Concentration-dependent killing --> MRSA, VRE
Tx SSTIs, blood stream infections, endocarditis
DO NOT USE TO TREAT PNEUMONIA (inactivated by lung)
D for no dextrose in Dapto
Warnings
+ Myopathy and rhabdomyolysis (ie think statins or renal impairment)
+ Can falsely Increase PT/INR
SE
+ Increase CPK
Monitoring
+ CPK levels weekly
Notes
+ Cubicin: compatible with NS or LR
CUbicin RF: Compatibly with NS (no dextrose)
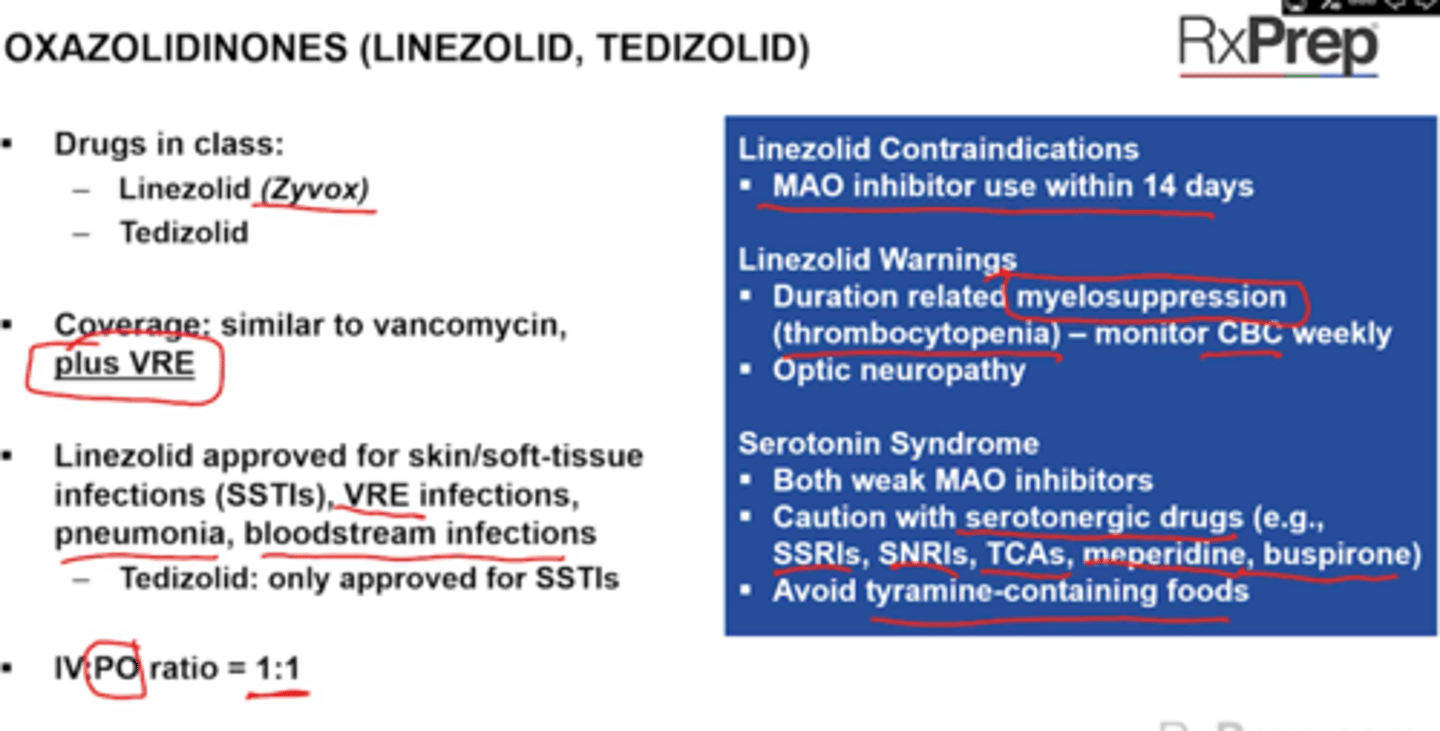
Oxazolidinones
50S subunit inhibitor of protein synthesis
Drug: Linezolid (Zyvox), Tedizolid
Coverage: Similar to vanco - plus VRE
Linezolid approved for SSTI, VRE infections, pneumonia, BSI
Tedizolid only SSTI
No dose adjustment in renal impairment (unlike vanco)
IV:PO ratio is 1:1
CI
+ Do not use with or within 2 weeks of MAO inhibitors
Warnings:
+ Duration related myelosuppression (thrombocytopenia)
+ Optic neuropathy
+ Serotonin syndrome
+ Hypoglycemia
SE
+ Decrease plts
Notes
+ Do not shake
Interactions
+ Linezolid and tedizolid are reversible monoamine oxidase inhibitors
+ Caution with serotenergic drugs (SSRIs, SNRIs, TCAs, meperidine, buspirone)
+ Avoid tyramine containing foods and serotonergic drugs (aged, pickled, smoked)
Quinupristin/Dalfopristin (Synercid)
p373
Coverage: Gram positive organisms --> MRSA, VRE (e faecium)
Indications: SSTIs
Poorly tolerated: arthralgyias/myalgias, infusion reactions, hyperbilirubinemia, phlebitis (Administer via CENTRAL LINE - PICC)
Compatible with D5W only
Clindamycin (Cleocin)
Binds to 50S subunit
COVERS ANAEROBES and Gram Positive Bacteria (INCLUDING CA-MRSA)
Formulations: Injection, topical
Topical (Cleocin-T, Clindagel)
No dose adjustment in renal impairment
Boxed warning
Cdif
SE
+ N/V/D
Notes
+ An induction test (D-test) should be performed on S. aureus that is susceptible to clindamycin but not erythromyci ( a flattened zone indicated inducibile clindamycin resistance - positive = DO NOT USE Clinda)
USE: Purulent and non-purulent skin infections, beta-lactam alternative for dental abscesses
Metronidazole (Flagyl), Tinidazole
Coverage: anaerobic and protozoal infections
Use: bacterial vaginosis, trichomoniasis, intra-abdominal infections
Multiple formulations (topical, vaginal)
IV:PO = 1:1
CI
+ Pregnancy
+ Alcohol (disulfiram reaction)
SE
+ metallic taste
+ Increases INR with Warfarin
Secnidzole - single dose PO f
+ SE vulvovaginal candidiasis
Tinidazole same as flagyl
DDI
+ Flagyl should not be used with alcohol (during or for 3 days after dc = dt disulfiram like reaction (abdominal cramping, N/V, headaches and flushing
+ Flagyl and tinidazole can increase INR
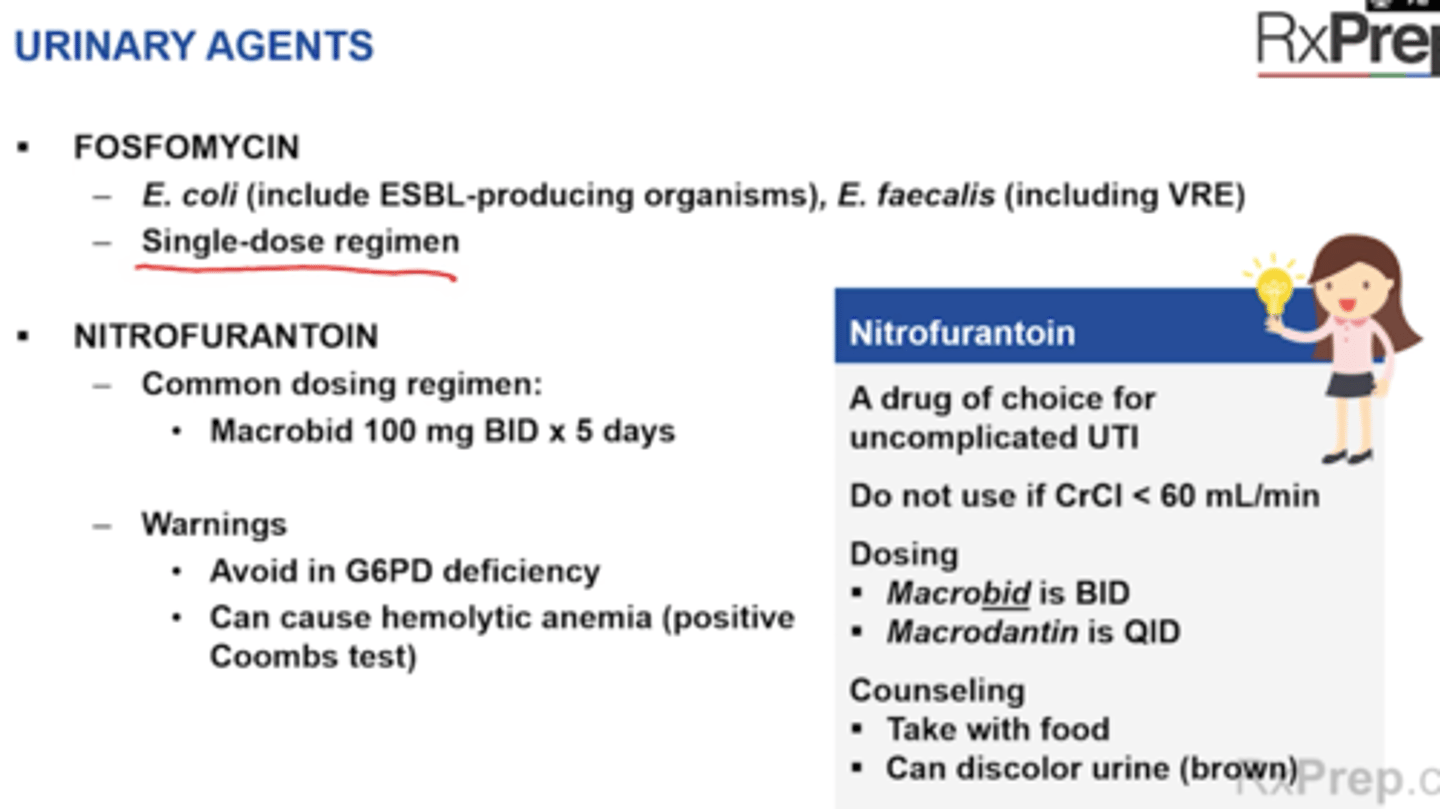
ABX urinary agents
Study Tip Gal p377
Fosfomycin
+ E. coli (including ESBL-producing organisms), E. faecalis (including VRE)
+ Single dose regimen for uncomplicated UTI (cystitis only)
Nitrofurantoin (Macrobid, Macrodantin)
+ Common dosing regimen = Macrobid 100 mg BID x5 days, Macrodantin is QID
+ Warnings
- Avoid in G6PD deficiency
- Can cause hemolytic anemia (positive coombs test)
+ CI: Renal impairment CrCl < 60 mL/min
Warning: hemolytic anemia (caution in G6PD deficient patients)
+ SE: GI upset (take with food), brown urine discoloration (harmless)
Which meds can interfere with coagulation laboratory assays?
lipoglycopeptides (oritavancin, Televancin)
Flagyl
Daptomycin
all effect INR or aPTT
The Following Drugs Outdue --> INR/aPTT
*Bactrim significantly interacts with warfarin and truly increases INR but DOES NOT falsely elevate
Lipoglycopeptides and UFH are CI within 120 hours/5 days of oritavancin false elevation of aPTT
Daptymycin and televancin falsely increase PT/INR
Drugs that increase warfarin INR
+ MAT =
M = Metronidazole, macrolides,
A = Amiodarone, azoles
T = TMP/SMX (FQs, amoxicillin, tetracycline, tigercycline)
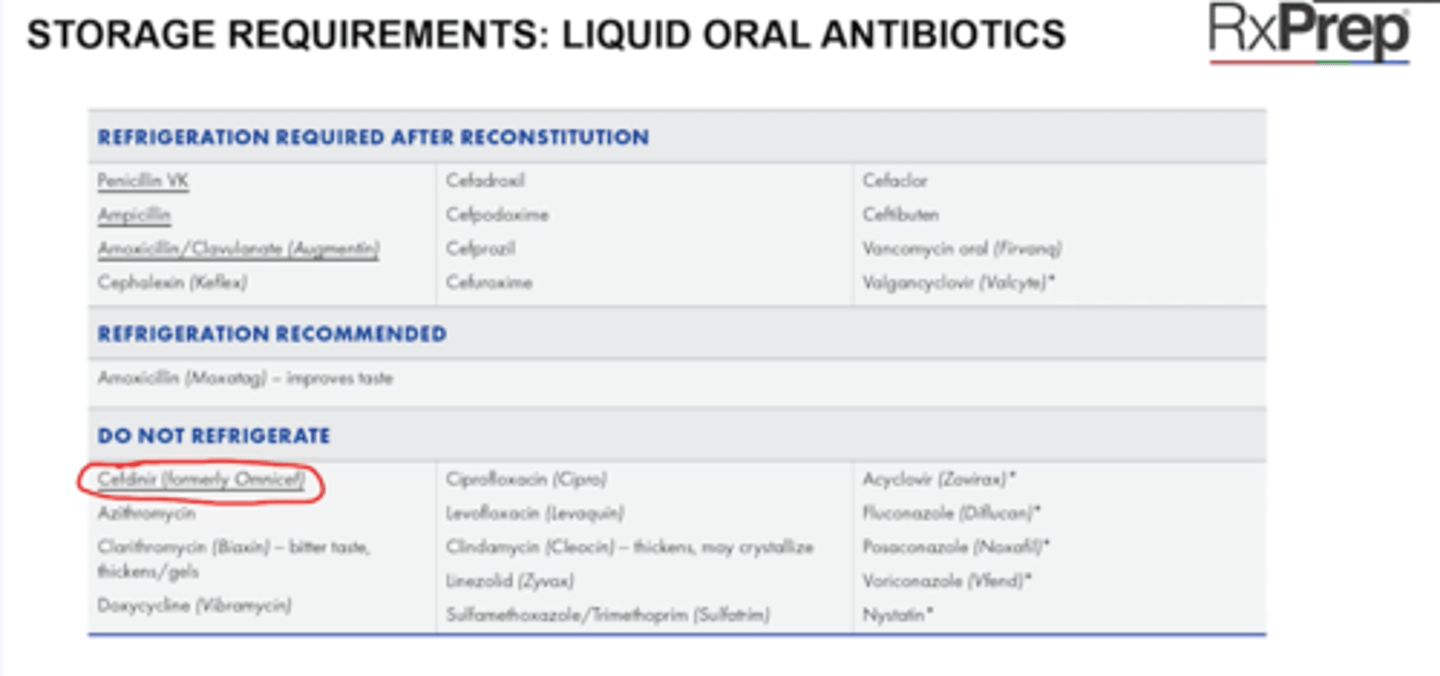
Storage requirements: Liquid oral abx
IV antibiotics
Most oral liquid abx in beta lactam category will require refrigeration
Ex: Penicillin VK, Ampicillin, Amoxicillin/Clav (Augmentin)
Exception: Cefdinir (Omnicef - 3rd gen ceph)
Non=beta lactams monly not frigerated (FQs, azoles, nystatin, linezolidl clindamycin, doxycycline, azithromycin, clarithromyciN)
IV ABX
DO not Refrigerate
+ Flagyl (metronidazole)
+ Moxifloxacin (Avelox)
+ Bactrim Sulfameth/trim
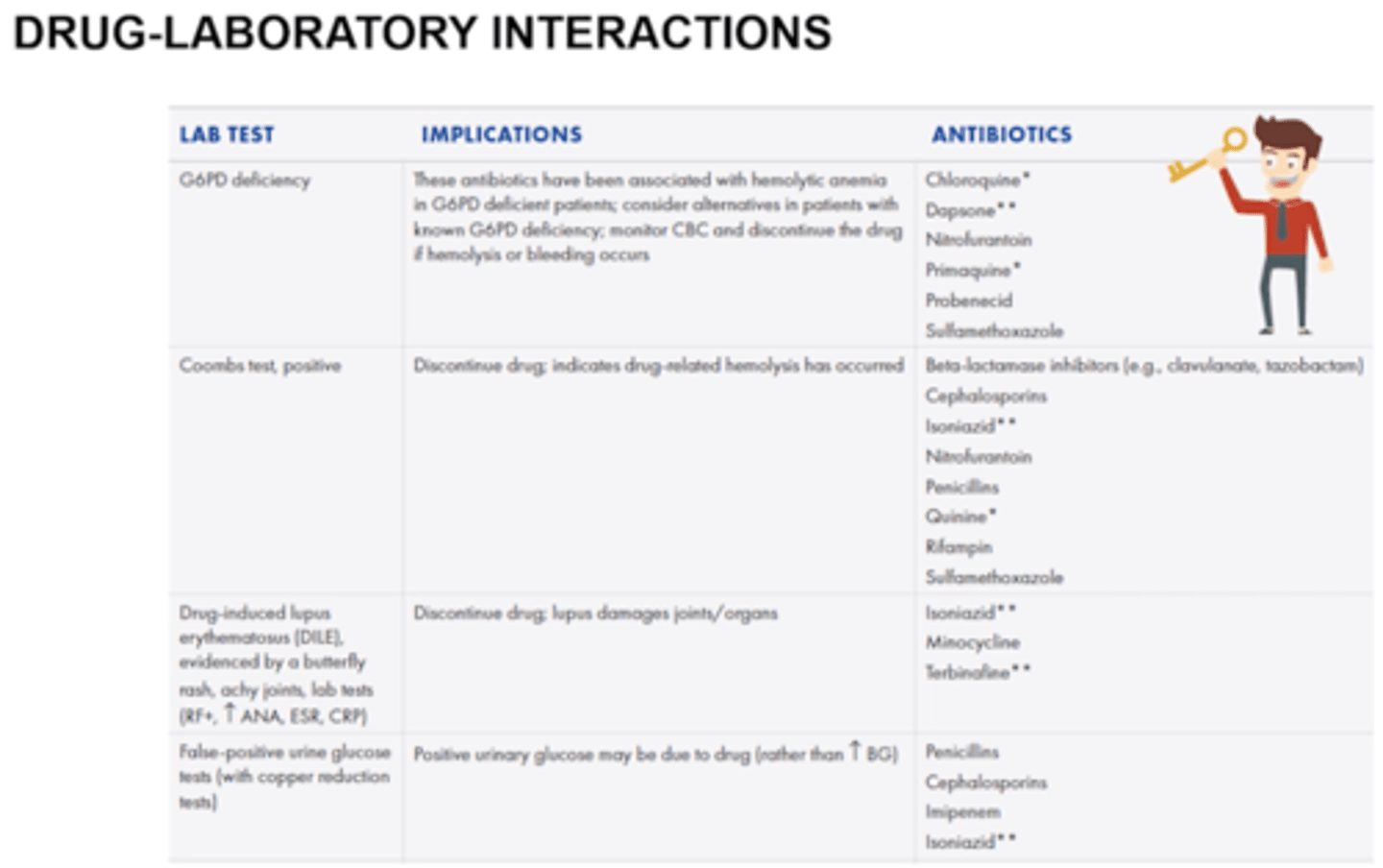
Drug Laboratory Interactions
G6PD deficiency - leads to hemolysis, bleeding
+ Chloroquine
+ Dapsone
+ Nitrofurantoin
+ Primaquine
+ Probenecid
+ Sulfamethoxazole, Bactrim
Coombs test, positive = dc drug -> hemolysis occurred, hemolytic anemia
+ Beta-lactamase inhibitors (clavulanate, tazobactam - augmentin, zosyn)
+ Cephlasporins
+ Isoniazid
+ Nitrofurantoin
+ Pencillins
+ Quinine
+ Rifampin
+ Sulfamethoxazole, Batrim
Drug Induced Lupus (DILE) - d/c drug, damages joints
+ Isoniazid
+ Minocycline
+ Terbinafine
False-positive urine glucose test
+ Penicillins
+ Cephlasporins
+ Imipenem
+ Isoniazid
ID 2
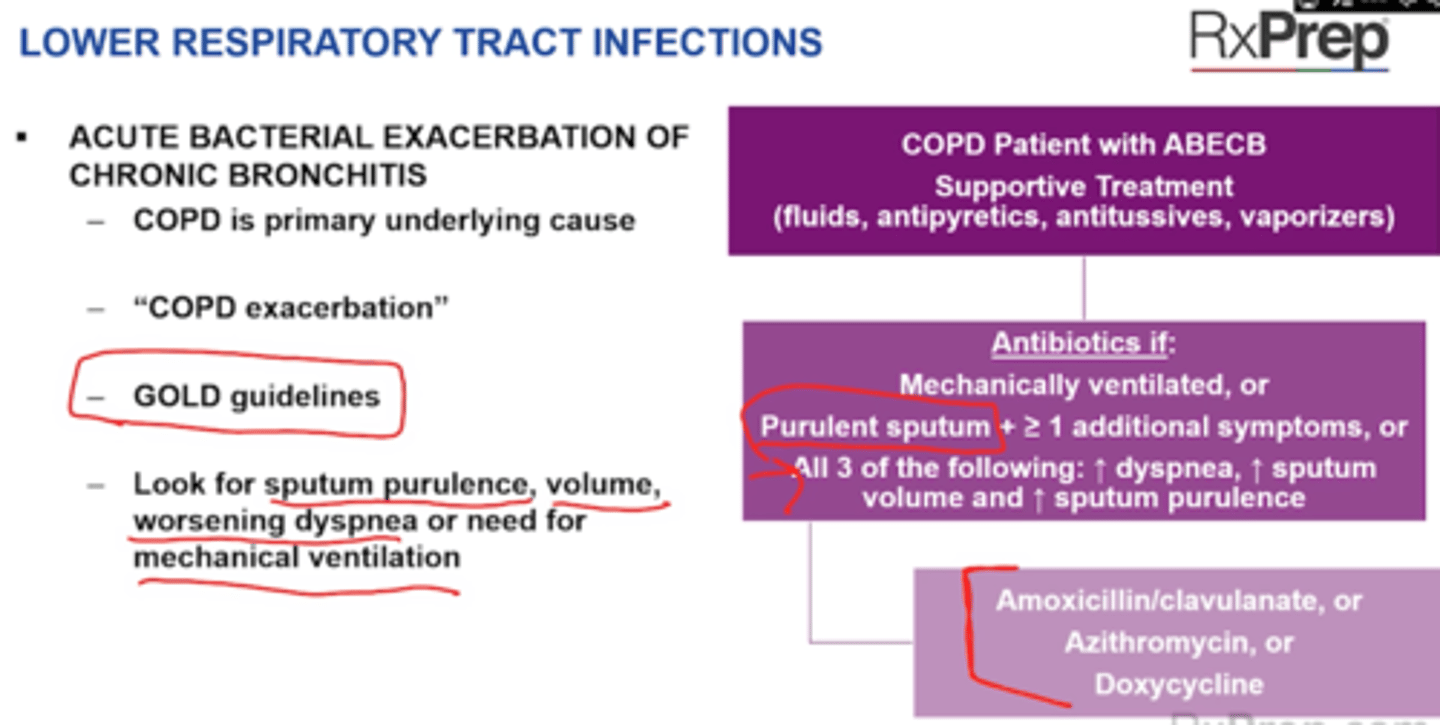
Bronchitis Treatment
Acute Bacterial Exacerbation of chronic Bronchitis (ABECB)
want to cover Bordetella pertussis (whooping cough)
Abx not recommended unless pneumonia is present - exception is Bordetella pertusis -->
Tx: macrolide (azithromycin, clarithromycin) or Bactrim
Chronic Bronchitis ABEcb - COPD
+ Supportive tratment (O2, short acting inhaled bronchodilators, IV or PO steroids)
Use Abx for 5-7 days if
+ Increased dyspnea, increased sputum volume, increased sputum purulence
+ Or if mechanically ventilated
+ ABX: Augmentin, or azithromycin, or doxycycline
ID 2 CAP treatment
Outpatient
Empiric treatment depends on 2 categories
Look at comorbidities: chronic heart, lung, liver or renal disease; DM, alcoholism, malignancy, asplenia
1. Category 1: no comorbidities (choose 1)
+ Amoxicillin high dose (1 g TID)
+ Doxycyclin
+ Macrolide (Azithromycin or clarithro)
2. Category 2: Has comorbidities
+ Beta lactam* + Macrolide or Doxycycline
+ Respiritory quinolone monotherapy (MGL)
* Beta lactam (Augmentin, cephalosporin - cefininir, cefuoxime, cefpodoxime)
---- See if patient needs MRSA or pseudomonas coverage (isolation respiratory, hospitalization in past 90 days)
+ Pseudomonas risk = Zosyn, cefepime, or meropenem + Levofloxacin or aminoglycoside and azithromycin
+ MRSA risk = Vanco, linezolid
ID 2
CAP Inpatient Treatment
1. Non-severe (similar to outpatient w/ comorbidities)
+ Beta lactam + Macrolide or doxycycline
+ OR Respiratory quinolone monotherapy (MGL)
2. Severe (typically ICU care required):
+ Beta-lactam + Respiratory quinolone (DO NOT USE MONOTHERAPY Quinolone)
+ OR Beta-lactam + Macrolide
*Beta-lactam preferred: ceftriaxone, cefotaxime, Augmentine
Risk factors for Pseudomonas or MRSA
+ MRSA: - Add vanco or linezolid
+ Psuedomons: Add Zosyn, cefepime, ceftazidime, imipenem, meropenem, aztreonam
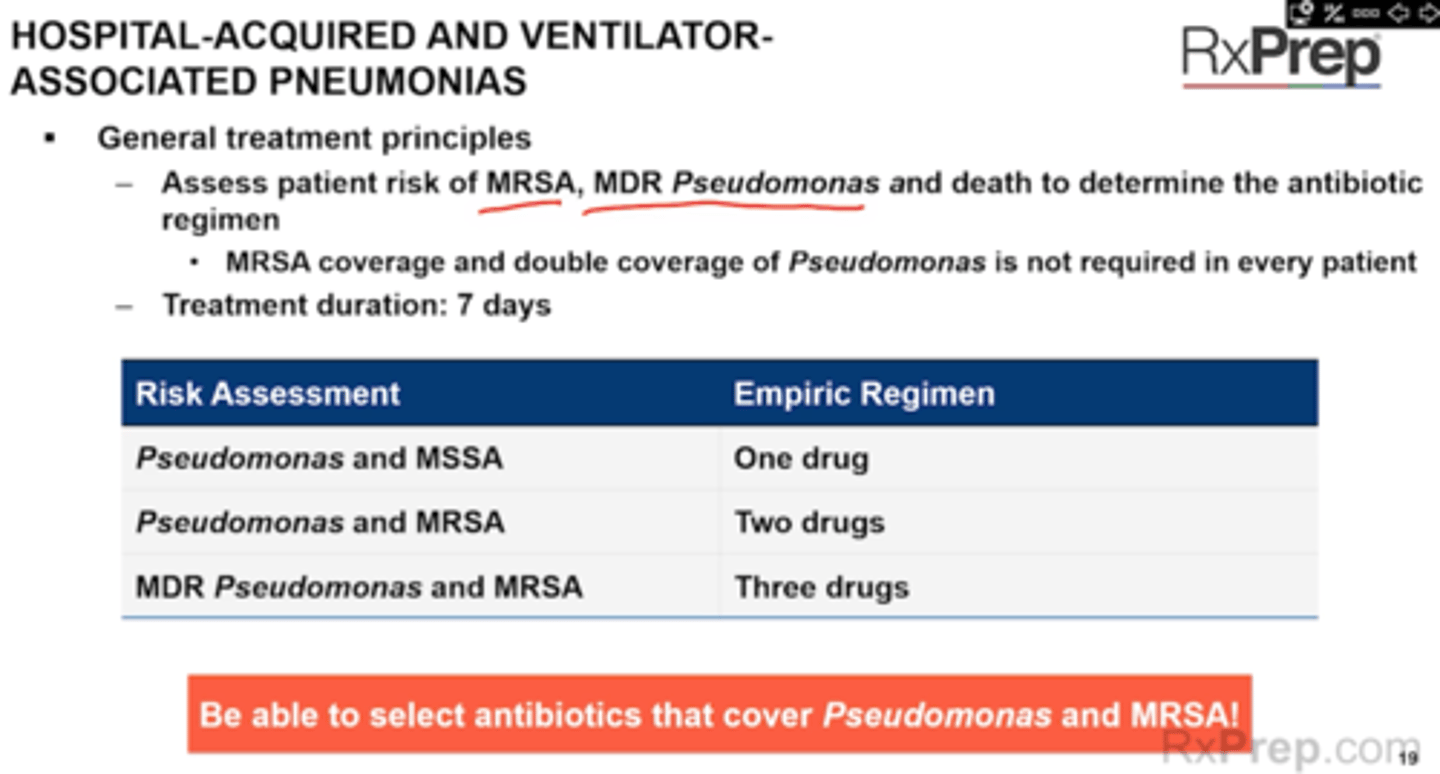
ID 2
HAP and VAP
HAP has onset > 48 hours after hospital admission
VAP > 48 hours after start of mechanical ventilation
Pathogens: nosocomial pathogens - MRSA and MDR gram neg rod risk (P. aeruginosa, Acinetobacter, Enterobacter = Pseudomonas, CAPES)
Empiric Treatment
1 drug if low risk for MRSA or MDR pathogen
+ Cefepime or Zosyn or meropenem
Choose 2 drugs - one for MRSA one for Pseudomonas if risk for MRSA but low risk for MDR pathogen
+ Cefepime + Vanoc
+ Meropenem + Linezolid
Choose 3 abx one for MRSA 2 for pseudomonas if risk for both MRSA and MDR pathogen (IV abx w/in 90 days)
+ Zosyn + Ciprofloxacin_ vanco
+ Cefepime + Gentamicin + LInezolid
Risk for MRSA or MRDR pathogens
+ Positive MRSA nasal swab
+ High prevalence of resitant pathogen noted in hospital unitl
+ ABX IV use within past 90 days
ABX for PSueodomonas (do not use 2 beta lactams together0
+ Zosyn
+ Cefepime, ceftazidime, or ceftolozane/tazobactam
+ Levofloxacin or ciprofloxacin
+ Imipenem/cilastatin or meropenem
+ Tobramycin, gentamycin or amikacin (use with another agent!)
+ Colistimethate or polymixin B (use with another agent)
MRSA abx
+ Vanco or linezolid
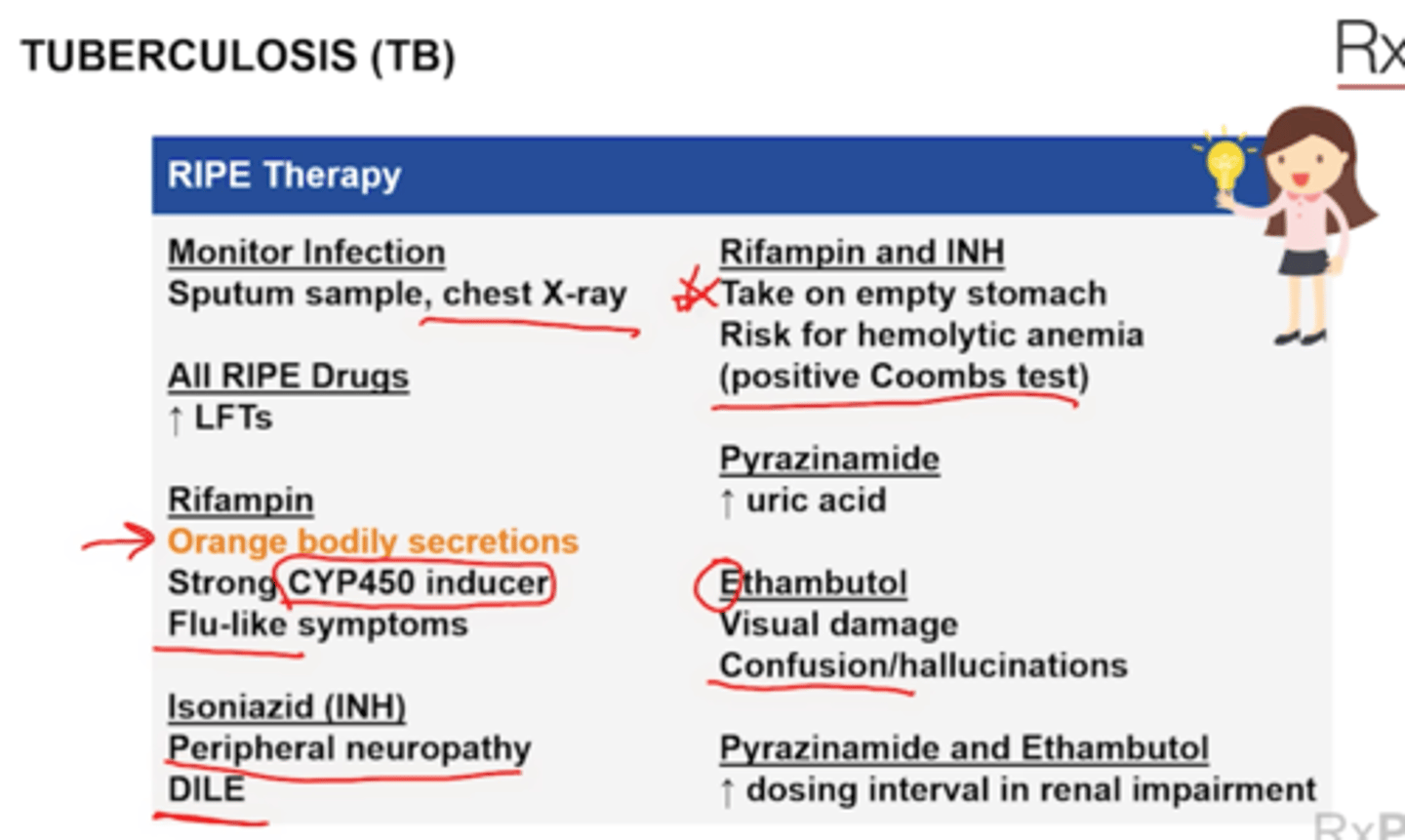
TB
RIPE intensive phase = 2 months
Continuoation phase x4 months = INH + Rif
Infective Endocarditis
Gentamicin used for synergy
+ Peak 3-4 mcg/mL
+ Trough <1 mcg/mL
Treatment
Streptococci = Penicillin or ceftriaoxne +/- gentamicin (beta allergy uses vanco mono)
MSSA staph = Nafcilin of cefazolin
+ With prostetic valve add gentamicin and rifampin
MRSA = vancomycin + gen/Rif if valve
Use dapto if patient has allergy
Enterococci = penicillin or ampicillin + gent
Allergy = vanco + gent
VRE = daptomycin or linezolid
Dental ppx
KNOW
Amoxicillin 2 g 30-60 min before procedure
If can take PO but allergic to PNC
+ Clindamycin 600 mg
+ Azithromycin or clarithromycin 500 mg
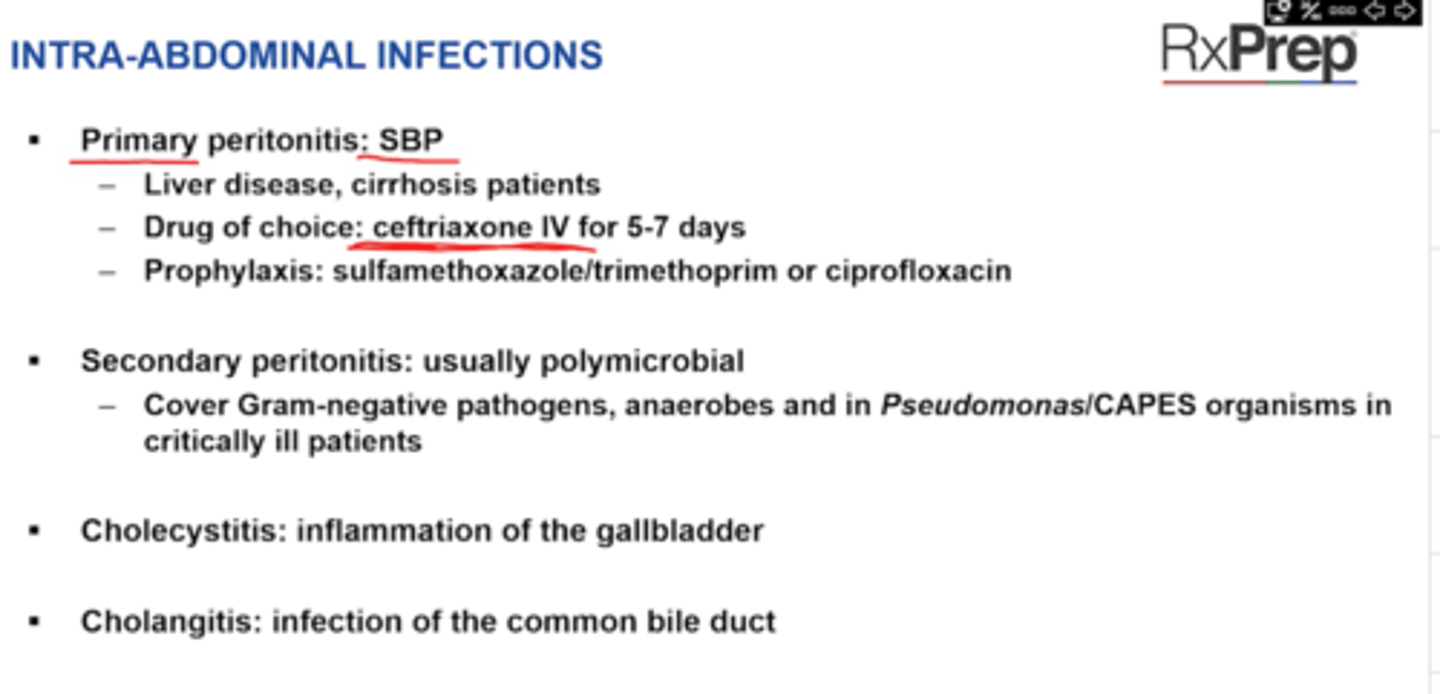
ID 2
Intra-abdominal Infections
SBP
1st: DOC ceftriaxone
2nd: bactrim or ciprofloxacin
ID 2
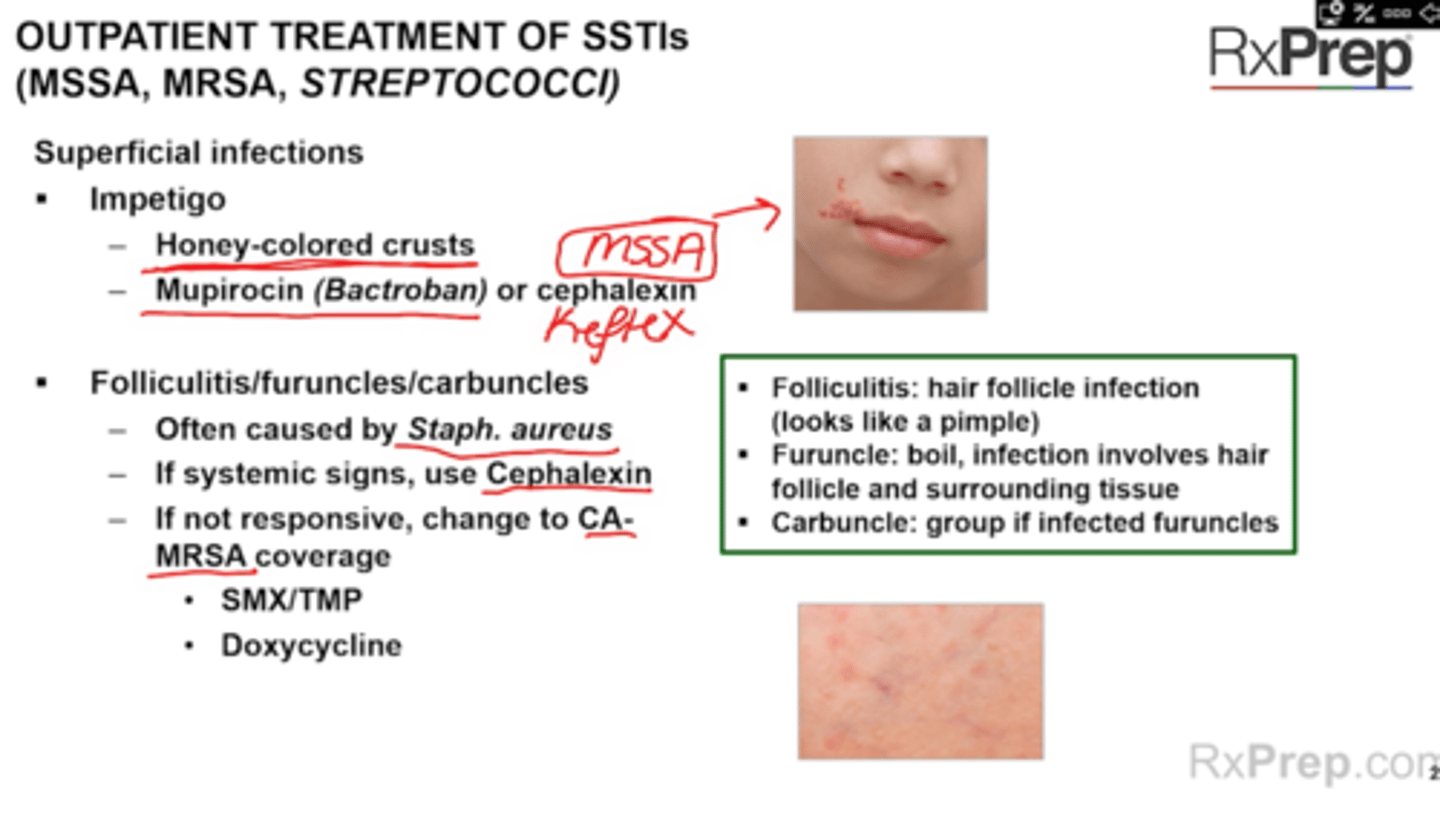
Outpatient of SSTIs (MSSA, MRSA) and Streptococci SSTI
Want oral for these MSSA SSTI
Impetigo
Folliculitis furuncles carbuncles
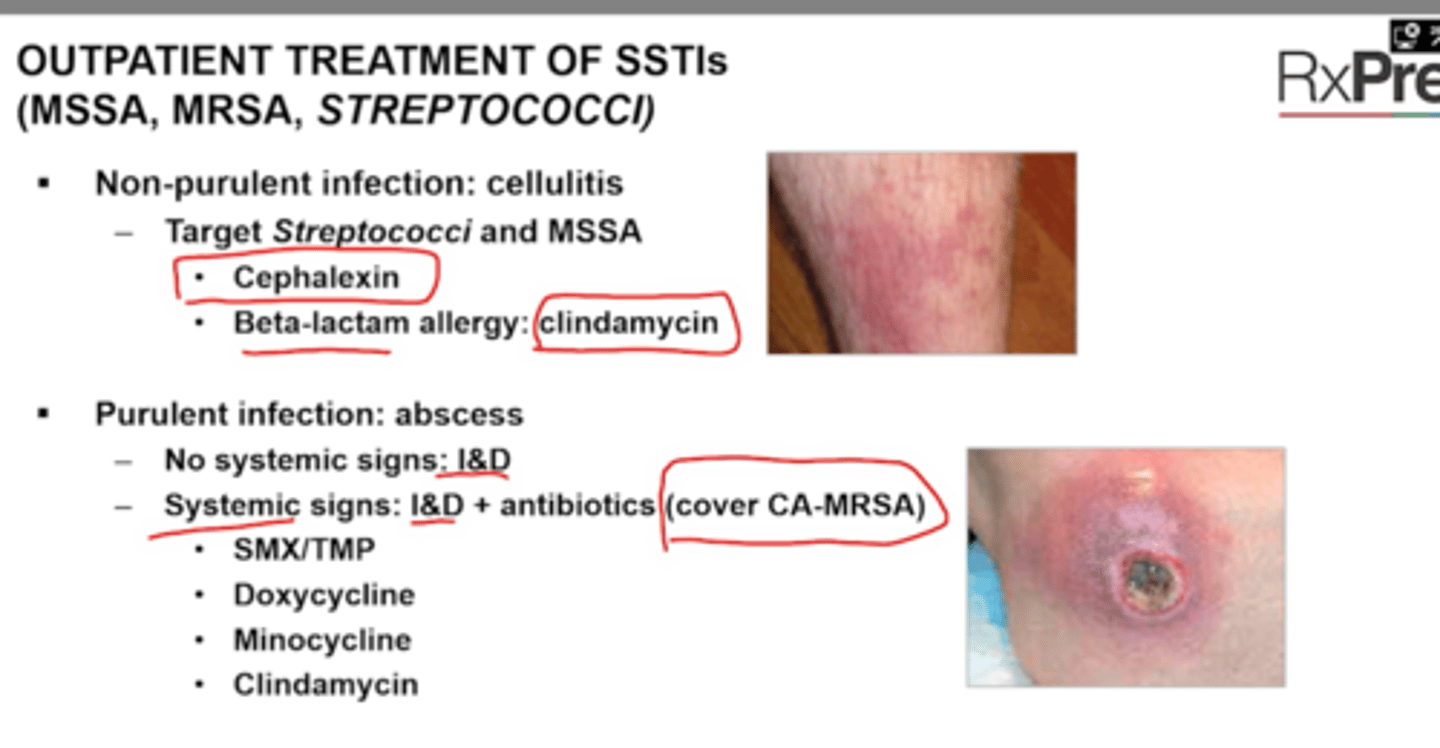
ID 2
SSTI MSSA MRSA and streptococci
Non-purulent infection: cellulitis
Purulent infection: abscess
ID 2
Severe Purulent SSTIs
Necrotizing Fasciitis
IV abx here
Diabetic food infection
moderate/severe diabetic foot infections
= combo-
vanco + ceftazidime/cefepime/zosyn/aztreonam/carbapenem
+ Vanco alternatives: daptomycin or linezolid
Adding anaerobe coverage if ceftazidime, cefepime, or aztreonam is selective
No MRSA or Pseudo risk: mono therapy: zosyn/unasyn, carbapenem (except doripenem), moxifloxacin
DOT: 7-14 days-severe, limb threatening infection 4-6 weeks
ID 2
UTI - Definition, classification, diagnosis , symptoms
ID 2
UTI Treatment
Pregnant
+ Bacteruirea
Treat even if asymptomatic (3-7 days)
DOC 1st line = Amoxicillin + Clavulanate or PO cephlasporin
Beta lactam allergy = Nitrofurantoin and Bactrim (avoid in 1st trimester if possible)
Avoid quinolones
ID 2
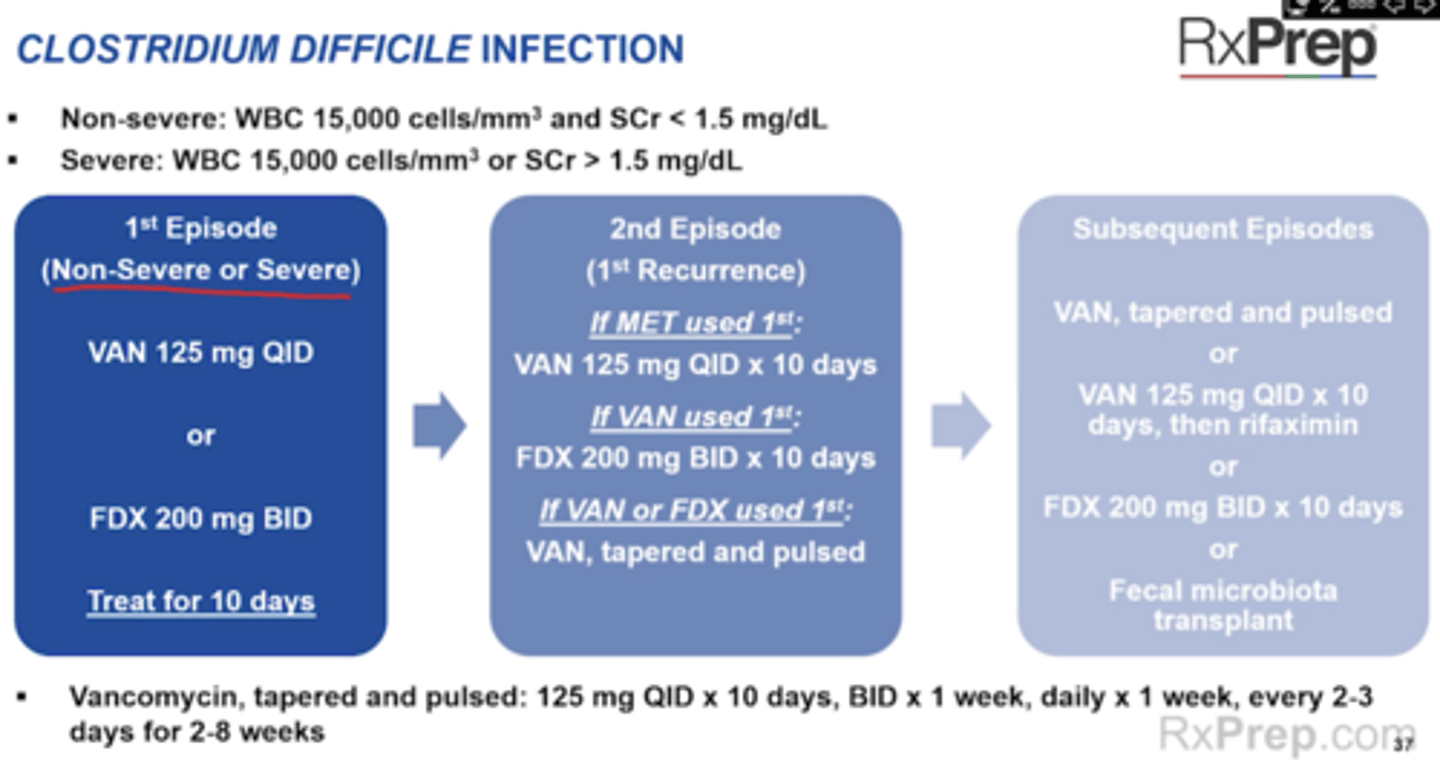
Cdif
Toxic mega colon
Use metronidazole IV + Vanco NG
ID 2
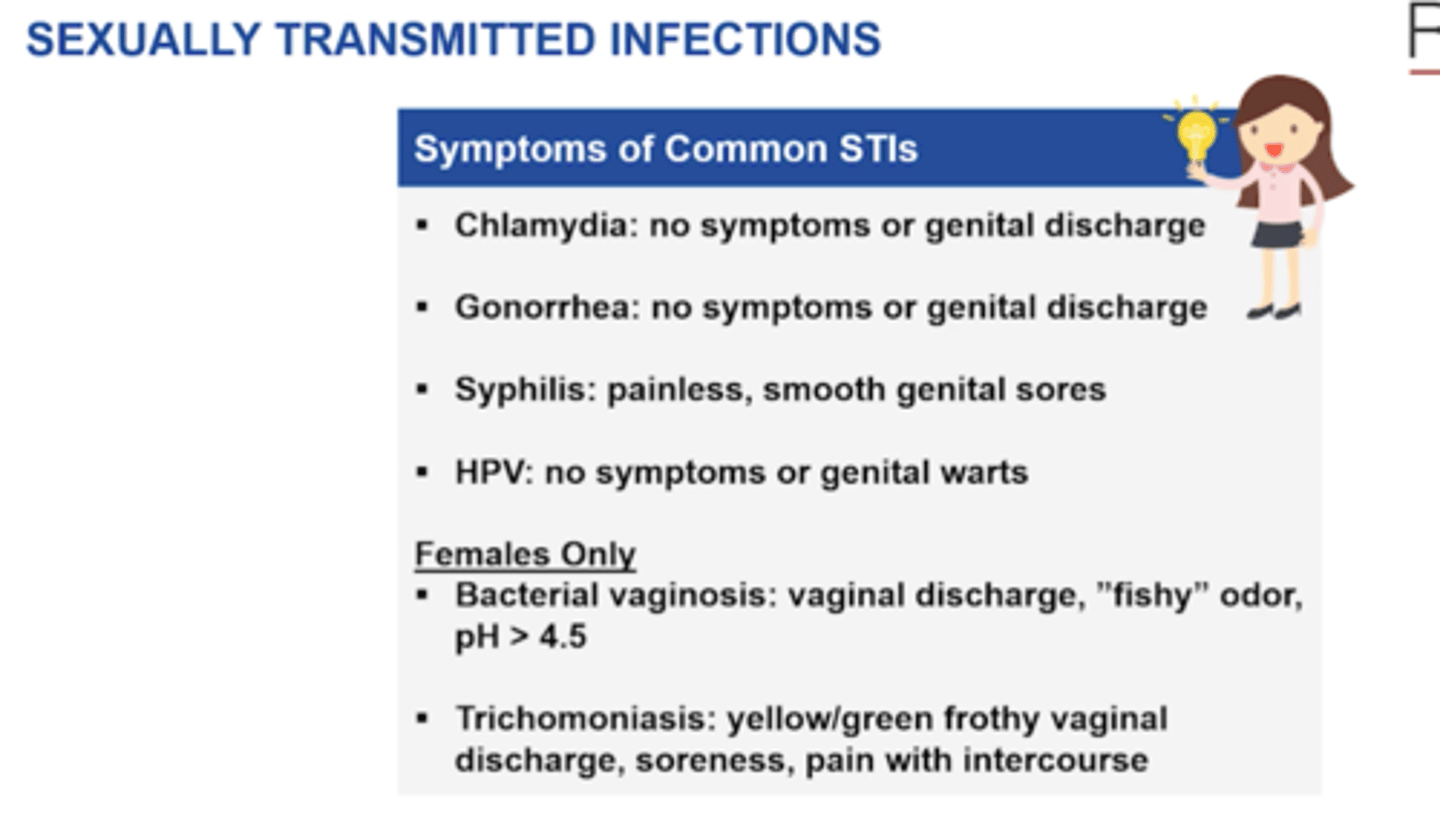
STI Symptoms
Gonorrhea
Chlamydia
Syphilis
HPV
Trichomoniasis
Bacterial vaginosis
ID 2
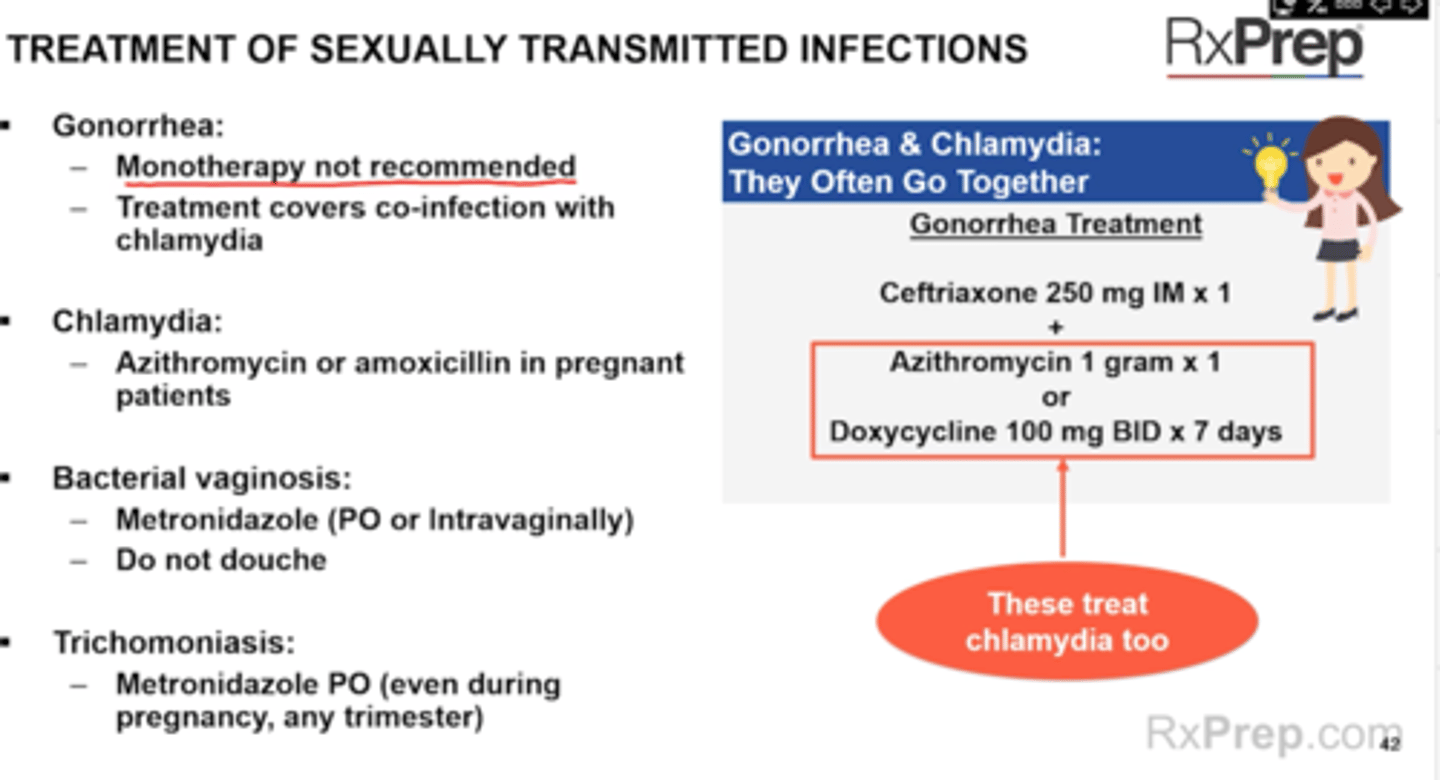
STI Treatment
Gonorrhea - ceftriaxone + Azithro of doxy (NO MONOTHERAPY)
Chlamydia - Azithro of amoxicillin
Syphilis
HPV
NEED FLAGYL
Trichomoniasis - PO or Intravaginal (fishy)
Bacterial vaginosis - PO regardless if pregnant
ID 3
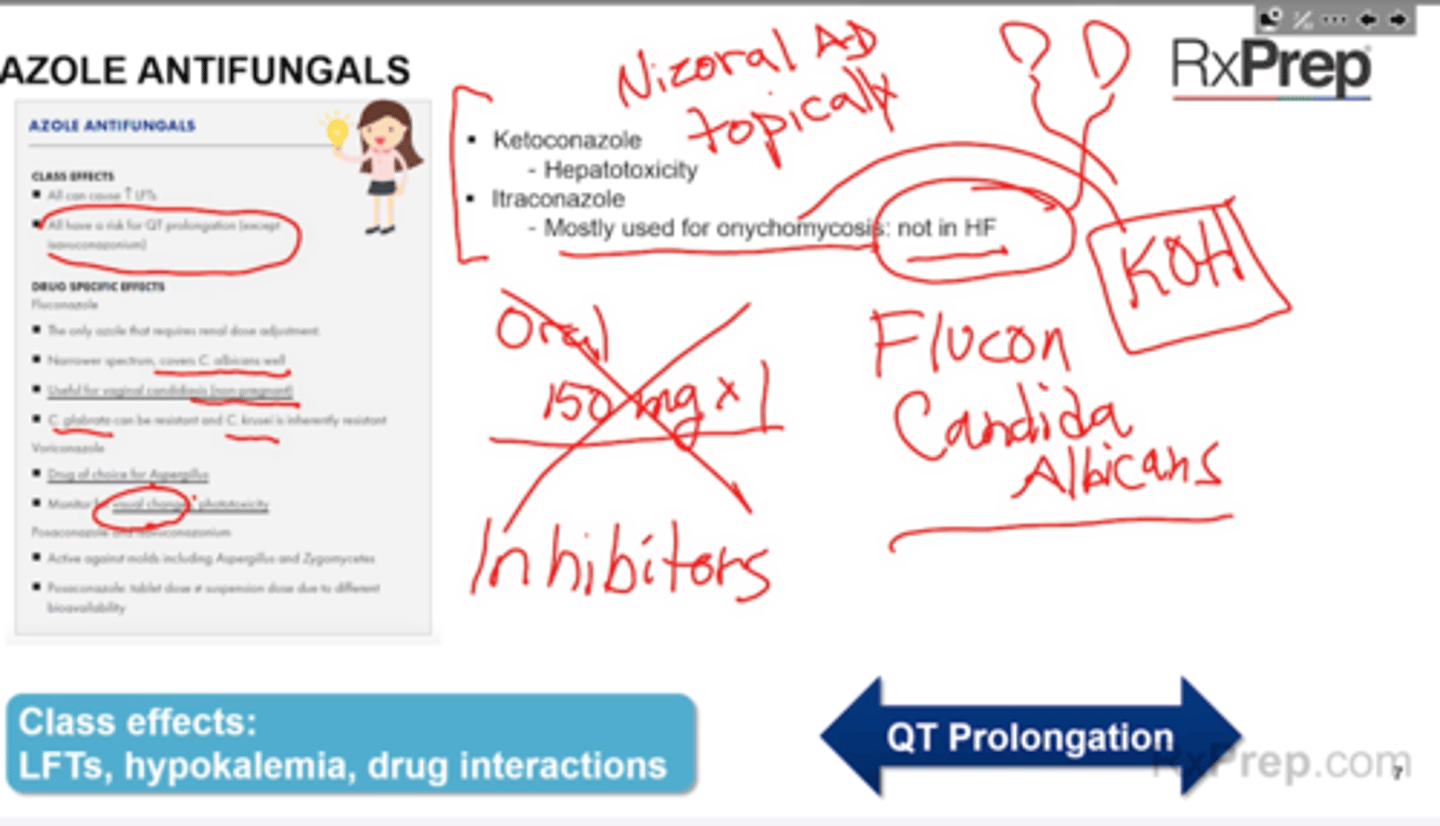
Key Issues with Azole Antifungals
Study Tip Gal p406
All IV/PO 1:1
All increase LFTs and QT (except QT cresemba isavuconazonium does not rolong)
Fluconazole (Diflucan) is PO/IV and 1:1
Can use vaginal candiasis 150mg PO x1
Candida albicans (can use fluconazole rather than iconocandids
Ketoconazole - hepatotoxicity = transplant
Itraconazole = can cause HF, don't use in patients with ventricular dysfunction of HF, can increase plasma concentration and lead to QT prolongation and Vtach
Voricoazole (Vfend, Vfend IV)
+ Take VFend on empty stomach
V = vision, vision disturbances, don't try at night, visual changes
+ Avoid direct sunlight - photosensitivity
Monitor SCr b/c CrCl < 50 leads to increase SBECD and so PO is preferred (CNS toxicity hallucinations)
Posaconazole (Noxafil)
+ QT prolongation
+ Take with food for PO
+ Like Voriconazole SBECD can accumulate look at SCr
Isavuconazonium (Cresemba)
= requires a filter
No QT prolongation --> instead has shortening
Ketoconazole and igtraconazole absorption is pH dependent
Azoles can increase wafarin so monitor INR (and apixaban and rivaroxaban)
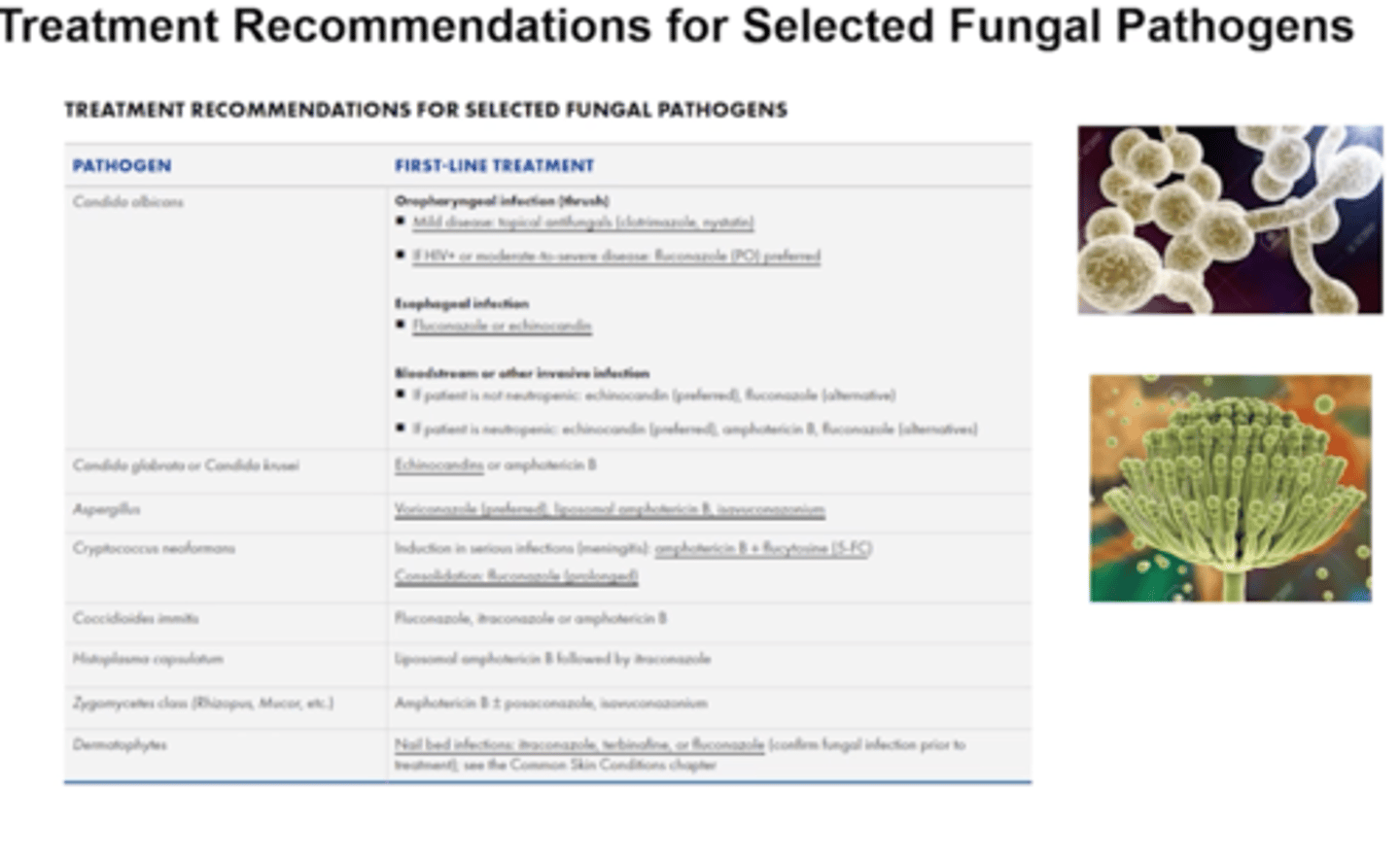
ID 3
Empiric Treatment for select fungal pathogens
Study Tip Gal p406
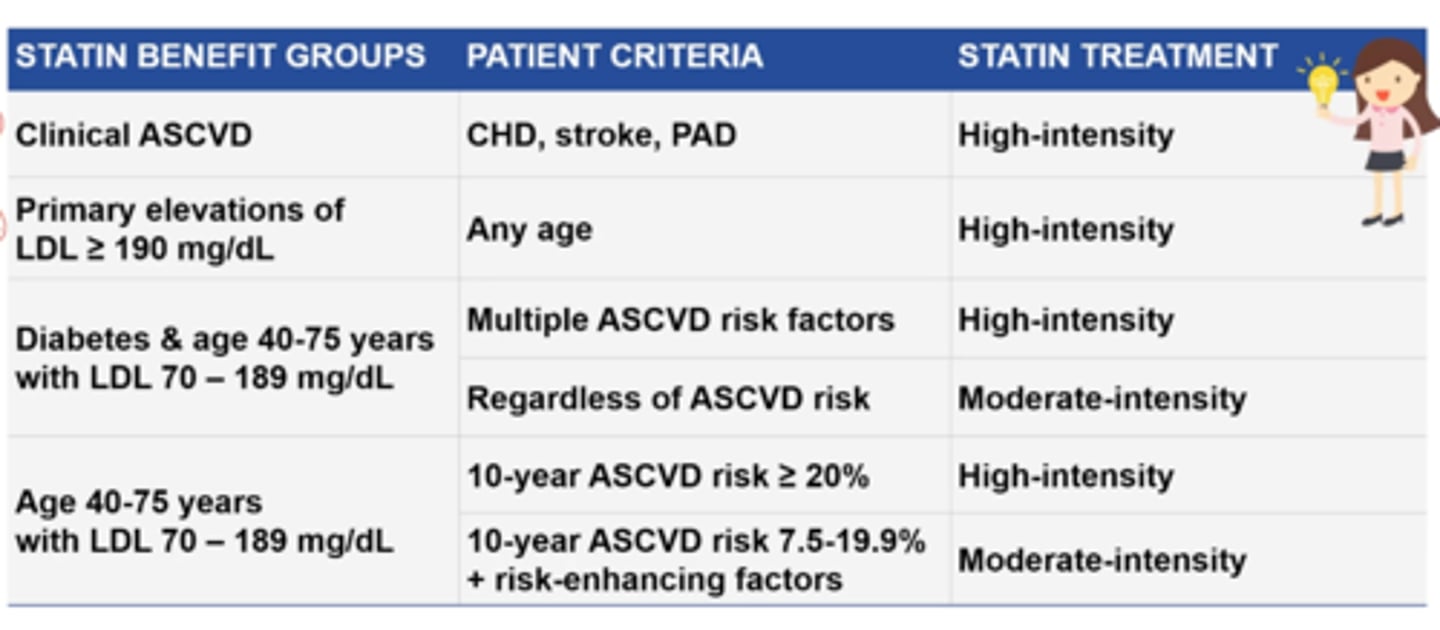
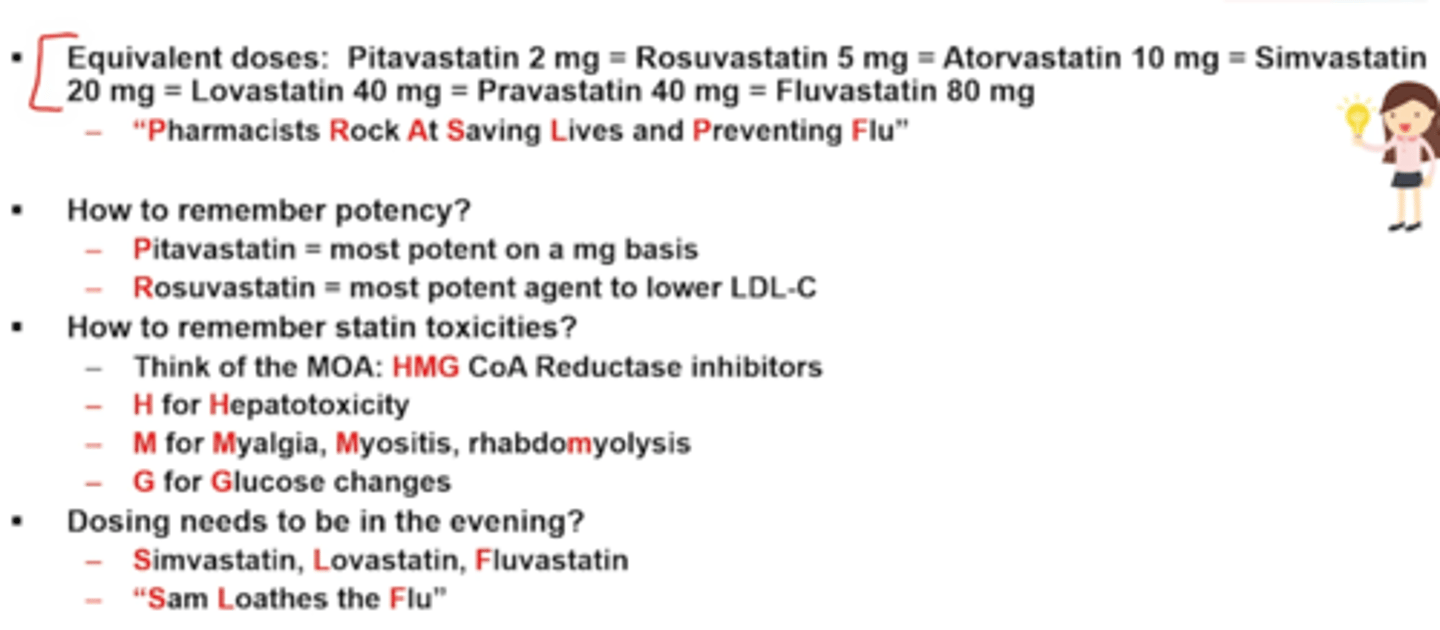
Statin Treatment Intensity Based on Patient Risk
Study Tip Gal p443
Statin Pneumonic
Potency
Pharmacists Rock At Saving Lives and Preventing Fat/Flu
Pitavastatin 2 mg
Rosuvastatin 5 mg
Atorvastatin 10 mg
Simvastatin 20 mg
Lovastatin 40 mg
Pravastatin 40 mg
Fluvastatin 80 mg
Potency
+ Pitivastatin = most Potent on a mg basis
+ Rosuvastatin = most potent agent to lower LDL
Toxicities
Think MOA: HMG
+ H = hepatotoxicity
+ M = Myalgia (muscle soreness), Myositis (muscle inflammation), myopathy (muscle weakness + cpk elevation) rhabdoMyolysis (muscule sx with high CPK = can cause renal failure)
+ G = Glucose changes
Dosing needed to be in evening?
+ Simvastatin (Zocor), Lovastatin (Altoprev - evening meal), Fluvastatin (Lescol)
+ Saving Lives from FLU
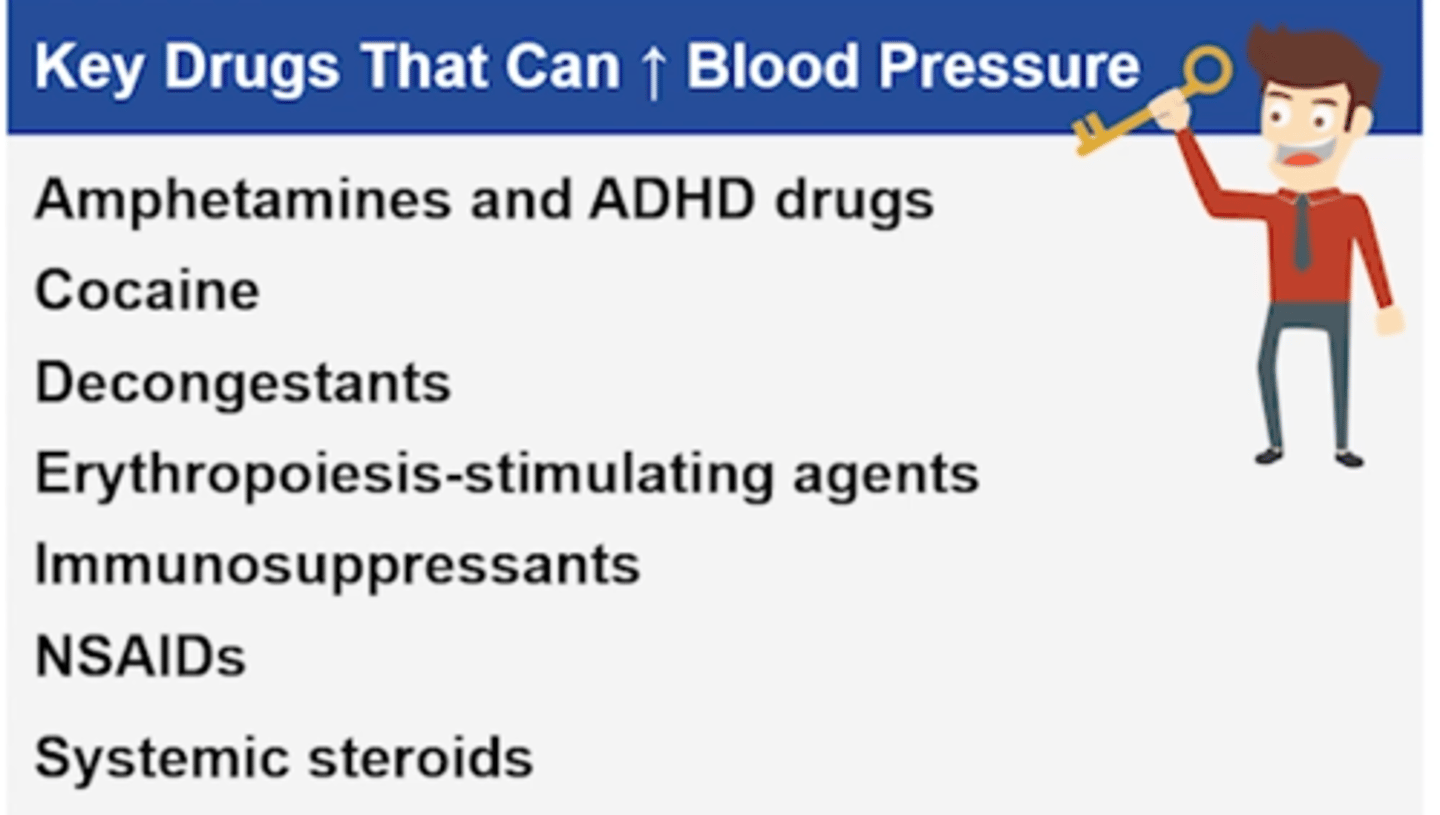
Key drugs that can increase BP
Key Drug Guy p454
1. Amphetamines and ADHD drugs
2. Cocaine
3. Decongestants (i.e. pseudoephedrine, phenylephrine)
4. Erythropoiesis-stimulating agents (ESA - epopoeitin)
5. Immunosuppressants (i.e. cyclosporine)
6. NSAIDs
7. Systemic steroids
List the key IV HTN meds
Key Drug Guy p467
+ Chlorothiazide (thiazide)
+ Clevidipine, Nicardipine (CCB)
+ Diltiazem Cardizem / Verapamil Calan (non DHP CCB)
+ Enalaprilat - Vasotec (ACEi)
+ Esmolol, Labetalol, Metoprolol tartrate Lopressor, propranolol Inderal (BB) --
MELT the BP in an emergency= Metoprolol, Esmolol, Labetalol, Tart
+ Nitroglycerin, Nitroprusside (post-MI)

Drugs for ACS
Key Drug Guy p475
MONA-GAP-BA
MONA: Immediate
- Morphine
- Oxygen
- Nitrates
- Aspirin
GAP: Give next
- GPIIb/IIIa antagonists (PCI + stent)
- Anticoagulants
- P2Y12 inhibitors
BA: W/in 24 hrs and outpatient
- Beta blockers
- ACEi
- (statin after high intensity unless 75+ might do mod)
NSTEMI/UA: MONO-GAP-BA + PCI
STEMI: MONA-GAP-BA + PCI (preferred) or fibrinolytic
1. Give MONA immediately (PRN)
2. Next give GAP (drug choice relates to plan if PCI vs CABG vs med management)
3. BA: Give within 24 hrs PRN; Continue outpatient
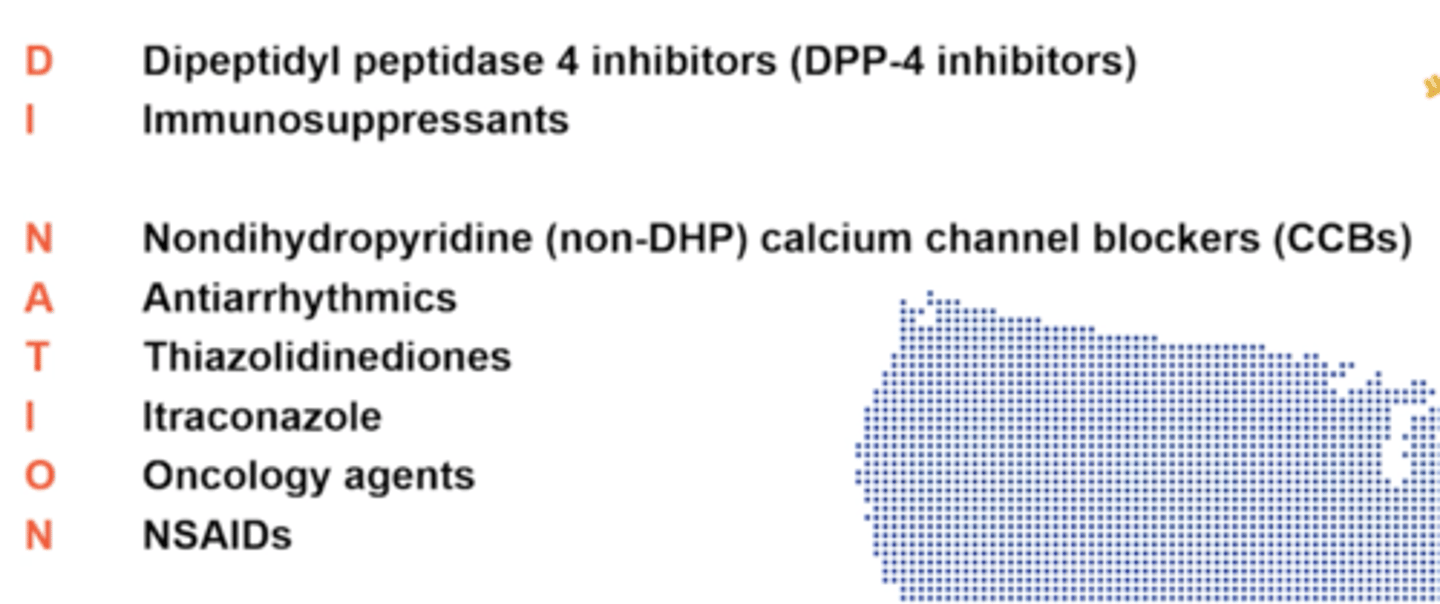
What select drugs cause or worsen HF?
Key Drug Guy p484
Drug Information NATION
DI NATION
Dipeptidyl peptidase 4 inhibitors (DPP-4 inhibitors)-Alogliptin, sitagliptin, saxagliptin
Immunosuppressants
TNF inhibitors (etanercept, adalimumab, rituximab) and interferons
Nondihydropyridine CCBs- Diltiazem and verapamil (specifically in systolic HF - b/c they have non-inotropic effect)
Antiarrhythmics- Avoid Class I agents (e.g., procainamide, quinidine, flecainide) in HF
Amiodarone and dofetilide have less risk of worsening HF
Thiazolidinediones- increase risk of edema
Itraconazole
Oncology agents Anthracyclines (doxorubicin, daunorubicin)
NSAIDs- All (including celecoxib) compete with loop diuretics
fluid retention/edema, by increasing blood pressure or via negative inotropic effect
What is the oral equivalent dosing for the loop diuretics?
Oral equivalent dosing:
bumetanide(bumex) 1 mg =
torsemide(demadex) 20 mg =
furosemide(lasix) 40 mg =
ethacrynic acid (edecrin) 50 mg
Furosemide IV:PO ratio 1:2
All others are 1:1
Remember T = twenty
F = Fourty
E is 5th leter = 50
B just is 1
Target Doses of HF meds
ACEi
ARBs
ARA
BB
Digoxin
Ivabradine
1. ACEi (REQLC)
+ Rapamil (Altace) = 10 mg QD
+ Enalapril (Vasotec) 10-20 mg BID
+ Quinpril (Accupril) (A 20 mg BID
+ Lisinopril (Prinivil, Zestril)- 20-40 mg QD
+ Catopril (Capoten)- TID
2. ARBs
+ Losartan (Cozaar)
- Target dose: 50-150 mg QD
+. Valsartan (Diovan)
- Target dose: 160 mg BID
Goes from 50-150 qd, then 160 BID
3. ARA
+ Spironolactone (Aldactone)
- Target dose: 25 mg QD or BID
4. Digoxin
- 0.125-0.25 mg PO QD
Target levels of 0.5-0.9 ng/mL
5. Beta Blockers
Beta-1 Selective Beta Blockers
+ Bisprolol
+ Metoprolol succinate ER (Toprolol XL)
- Target dose 200 mg
Non-selective Beta Blocker and Alpha=1 Blocker
+ Carvedilol (Coreg)
Target
< 85 kg = 25 mg BID
> 85 kg = 50 mg BID
6. Ivabradine
Target: resting heart rate between 50-60 BPM
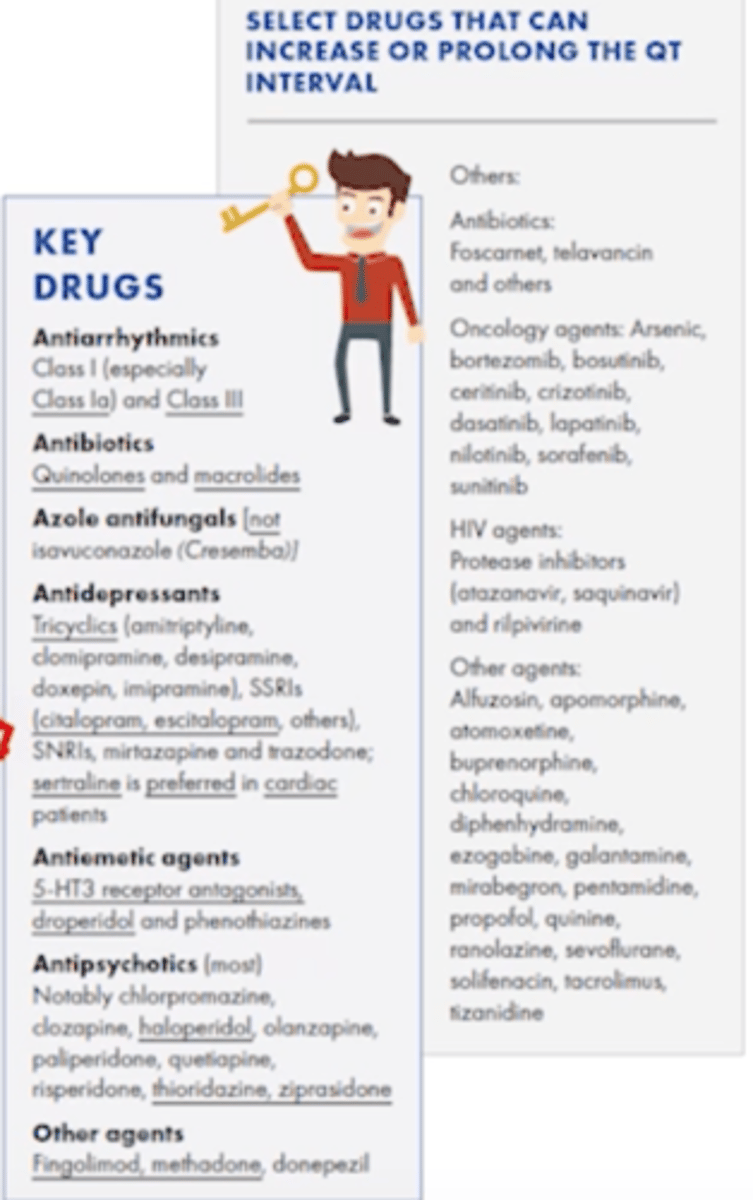
Which key drugs prolong the QTc?
Key Drug Guy p500
Antiarrhythmics
+ Class I (especially Class la) and Class III (amiodarone)
Antibiotics
Quinolones and macrolides
Azole antifungals
All except isavuconazonium
Antidepressants
Tricyclics (e.g., amitriptyline, clomipramine, doxepin)
SSRIs (e.g., citalopram/Celexa 40 mg, escitalopram/Lexipro 20 mg - have max doses to avoid QT prolong); sertraline (Zoloft) is preferred in cardiac patients
SNRIs, mirtazapine and trazodone
Antiemetic agents
5-HT3 receptor antagonists (zofran/ondansetron), droperidol (one of the worst QT prolongers antidopaminergic drug) and phenothiazines
Antipsychotics (most) - haloperidol, thio, and ziprasidone are top antipsychotics
+ Chlorpromazine, clozapine, haloperidol IV, olanzapine (Zyprexa), paliperidone, quetiapine, risperidone, thioridazine, ziprasidone (Geodon)
Other drugs
Donepezil, fingolimod (for Multiple Sclerosis), methadone (anti-arrhythmic at high doses), tacrolimus
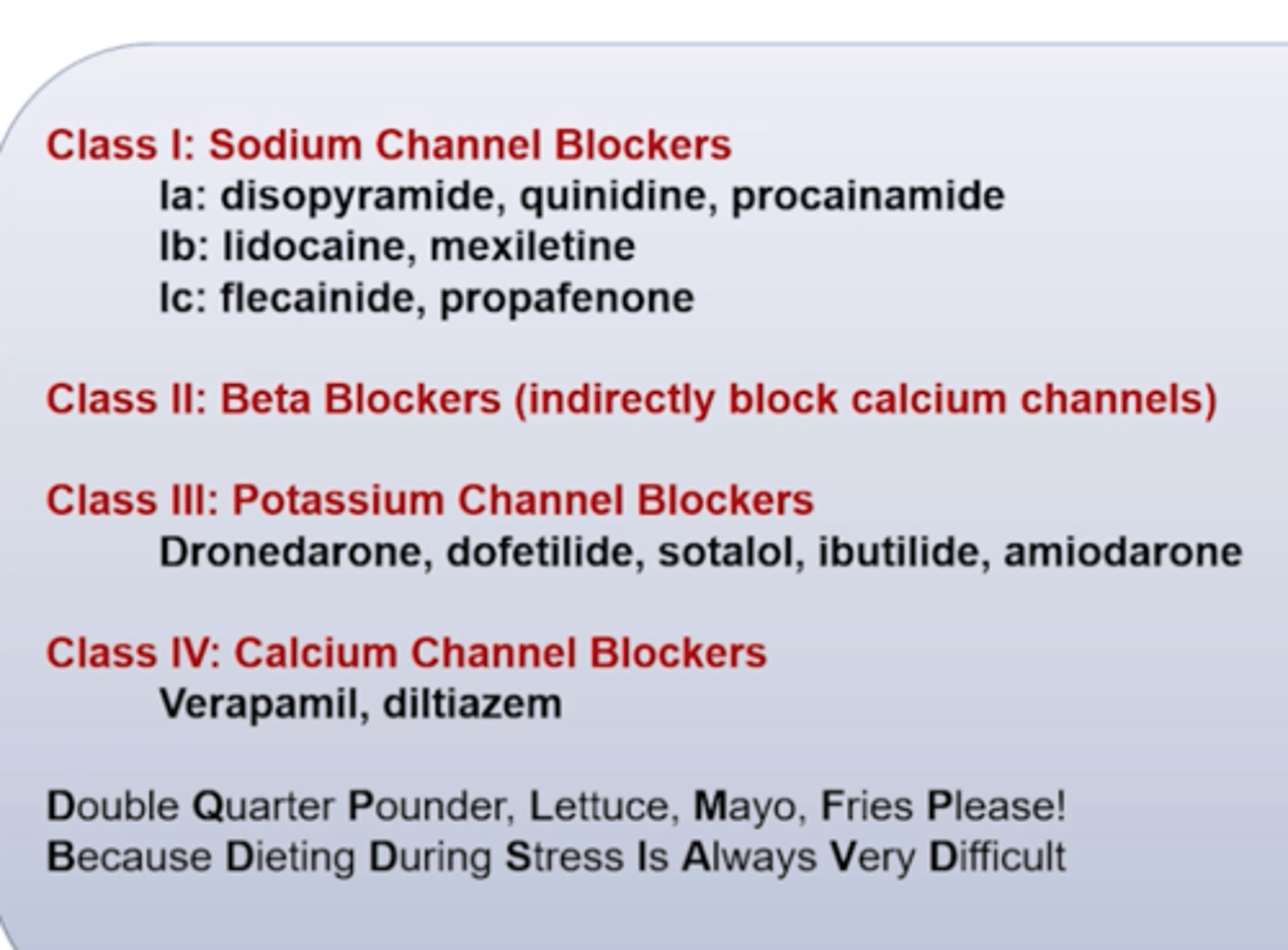
Vaughan Williams Classification of antiarrhythmic drugs
Study Tip Gal p501
CLASS I - Sodium Channel Blockers
la: Disopyramide, Quinidine, Procainamide
lb: Lidocaine, Mexiletine
Ic: Flecainide, Propafenone
1a is especiallly dangerous for qt (proarrhythmics)
CLASS II
Beta-blockers (indirectly block calcium channels)
CLASS III Potassium Channel Blockers
- Dronedarone, Dofetilide, Sotalol (also BB), Ibutilide, Amiodarone
Amiodarone
CLASS IV: Calcium Channel Blockers - Rate Control
- Verapamil, Diltiazem
Class 4 mostly rate control, slow HR
Remember:
Double Quarter Pounder, Lettuce Mayo, Fries Please! Because Dieting During Stress Is Always Very Difficult
AFib Rate vs Rhythm Control and Stroke Prophylaxis
Study Tip Gal p501
Rate Control
+ Patient remains in AFib and takes medication to control ventricular rate (HR)
--> BB or non-DHP CCBs (sometimes digoxin)
Rhythm Control
+ Goal is to restore and maintain NSR
--> Class 1a, 1c, or III antiarrhythmatic or electrical cardioversion
+ If Afib is permanent, avoid rhythm control antiarrhythmic drugs (risk > benefit)
Stroke Prophylaxis
+ Clots can form when a patient is in AFib, which can embolize (causing stroke) when patient returns to NSR
+ For many patients, it is safer to remain in Afib with rate control than to try and restore NSR. A rate control strategy may require anticoagulation for stroke prevention dependent on the CHADS-VASc score
--> NOACs (eg apixaban, rivaroxaban) are preferred over warfarin for non-valvular Afib
--> Warfarin is indicated for mechanical heart valves
+ When a rhythm control strategy is chosen, restoration and maintenance of NSR is not guaranteed. Long term anticoagulation decisions depend on the patient's clot risk
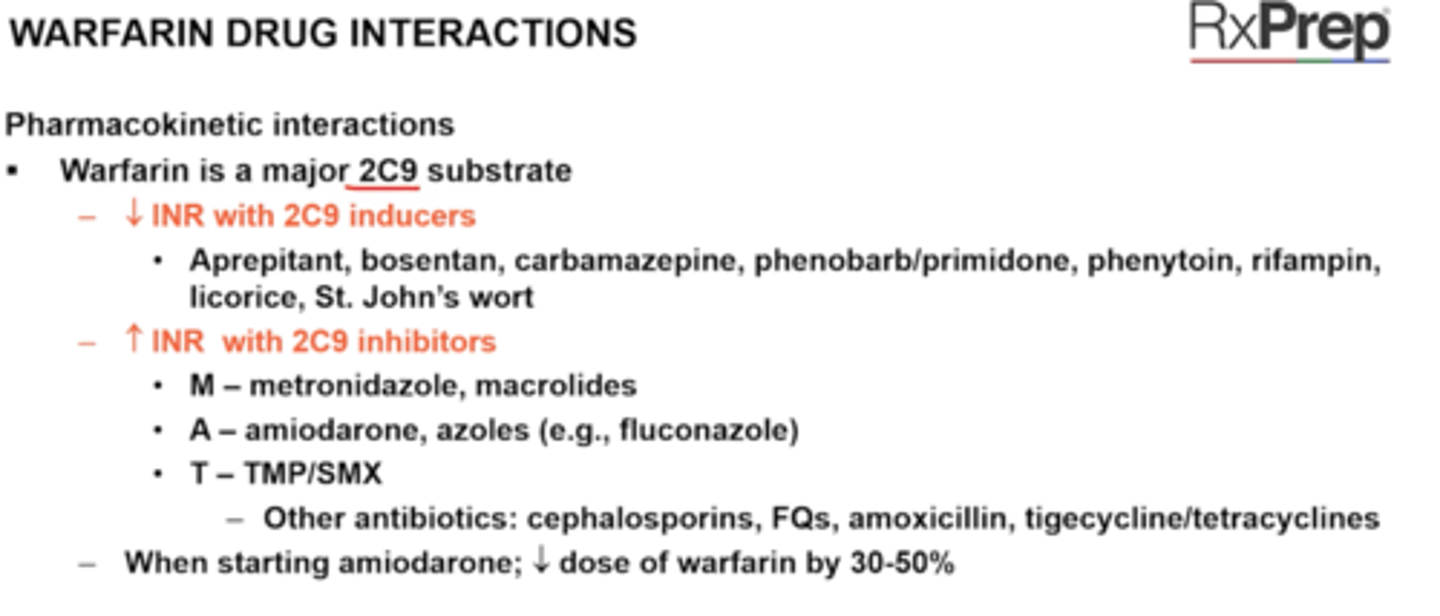
Amiodarone interactions
When starting amiodarone, decrease digoxin by 50% and decrease warfarin by 30-50%
+ Simvastatin:
Do not exceed 20 mg/day of simvastatin
+ Lovastatin: 40 mg/day of lovastatin
+ Sofosbuvir can enhance bradycardic effect of amiodarone - don't use together
Amiodarone can increase the level of many other drugs; it is an inhibitor of CYP450 2C9 (moderate), 2D6 (moderate), 3A4 (weak) and P-gp.
■ Amiodarone is a substrate of CYP3A4,2C8 and P-gp. Strong/ moderate inhibitors of these enzymes will increase amiodarone and strong/moderate inducers will decrease amiodarone.
■ When starting amiodarone, decrease digoxin by 50% and decrease warfarin by 30 - 50%. Do not exceed 20 mg/day of simvastatin or 40 mg/day of lovastatin; statin levels will increase. Consider use of alternative statin.
■ Additive effect with other drugs that decrease HR, including non-DHP CCB, digoxin, beta-blockers, clonidine and dexmedetomidine (Precedex).
■ Sofosbuvir (hep C drug) can enhance the bradycardic effect of amiodarone; do not use together.
Warfarin tablet colors
study tip gal p529
Pink = 1 mg
Lavender = 2mg
Green = 2.5 mg
Brown/Tan = 3mg
Blue = 4 mg
Peach = 5mg
Teal = 6mg
Yellow = 7.5 mg
White = 10 mg
Please Let Greg Brown Bring Peaches To Your Wedding
Warfarin Drug Interactions
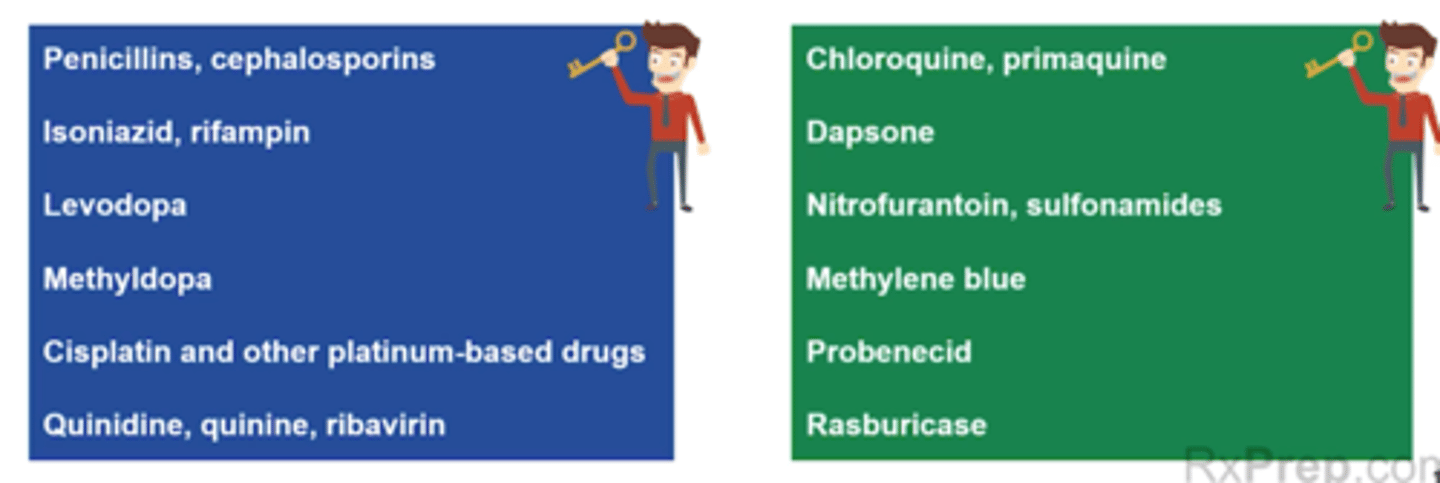
Hemolytic Anemia Acquired (drug-induced)
Drugs
Key Drug Guy p542
+ Penicillins, Cephlasporins
+ Isoniazid, rifampin
+ Levodopa
+ Methyldopa
+ Cisplatin and other platinum based drugs
+ Quinidine, quinine, ribavirin
+ Sulfonamides (Bactrim)
+ Dapsone
+ Nitrofurantoin
+ Primaquine
+ Rasbucase
+ Probenecid
+ Methylene blue
Identify with coombs test
Elemental Iron amount
Ferrous sulfate
Dried ferrous sulfate
Ferrous fumurate
Ferrous sulfate = 20% (65 mg)
Dried Ferrous sulfate = 30% (50 mg)
Ferrous fumurate = 33%
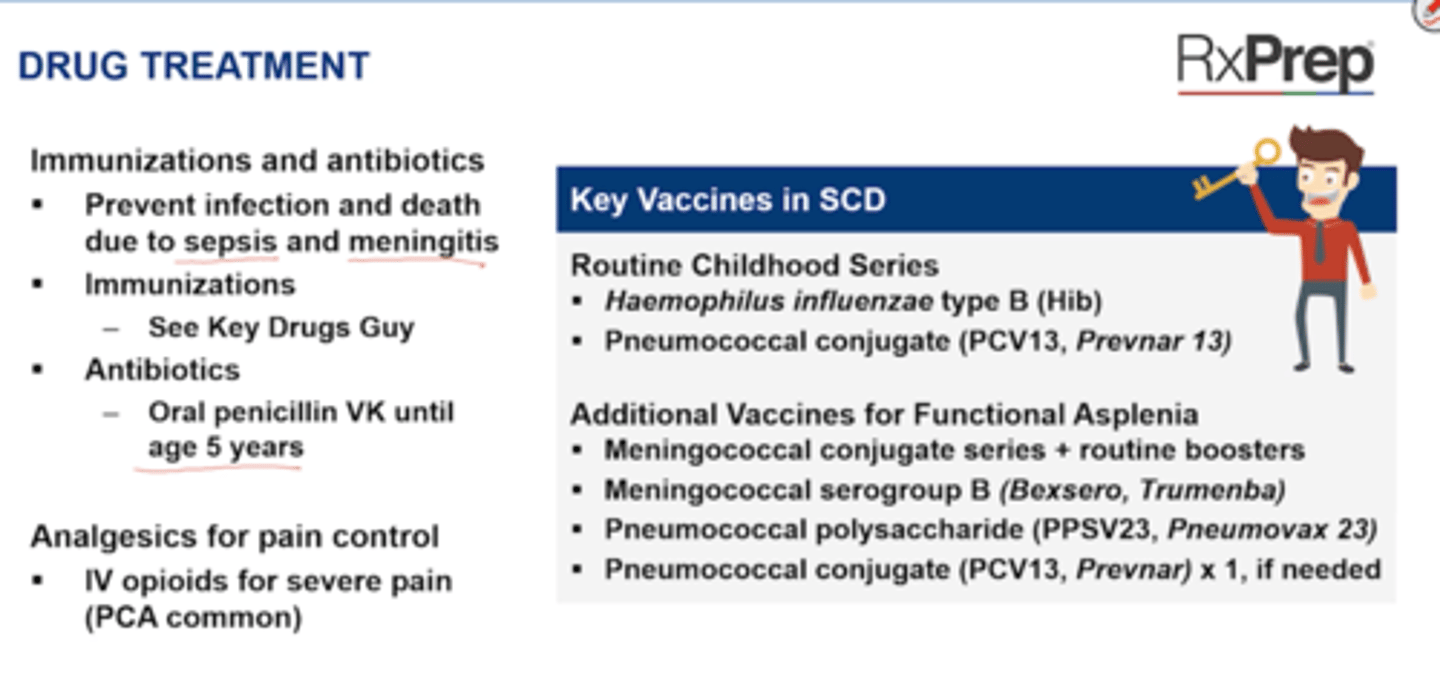
Drug Treatment - Key vaccines in Sickle Cell Anemia
Routine Childhood series
+ Haemophilus influenzae type B (Hib)
+ Pneumococcal conjugate (PCV13, Prevnar)
Additional Vaccines for Functional Asplenia
+ Meningococcal conjugate series + routine booster
+ Meningococcal serogroup B (Bexsero, Trumenba) --> At age > 10
+ Pneumococcal polysaccharide (PPSV23, Pneumovax23) --> at age > 2 years, booster 5 years later and at age > 65
+ Pneumococcal conjugate (PCV13, Prevnar) x1 in any patient > 6 years of age, if never received as part of routine childhood series
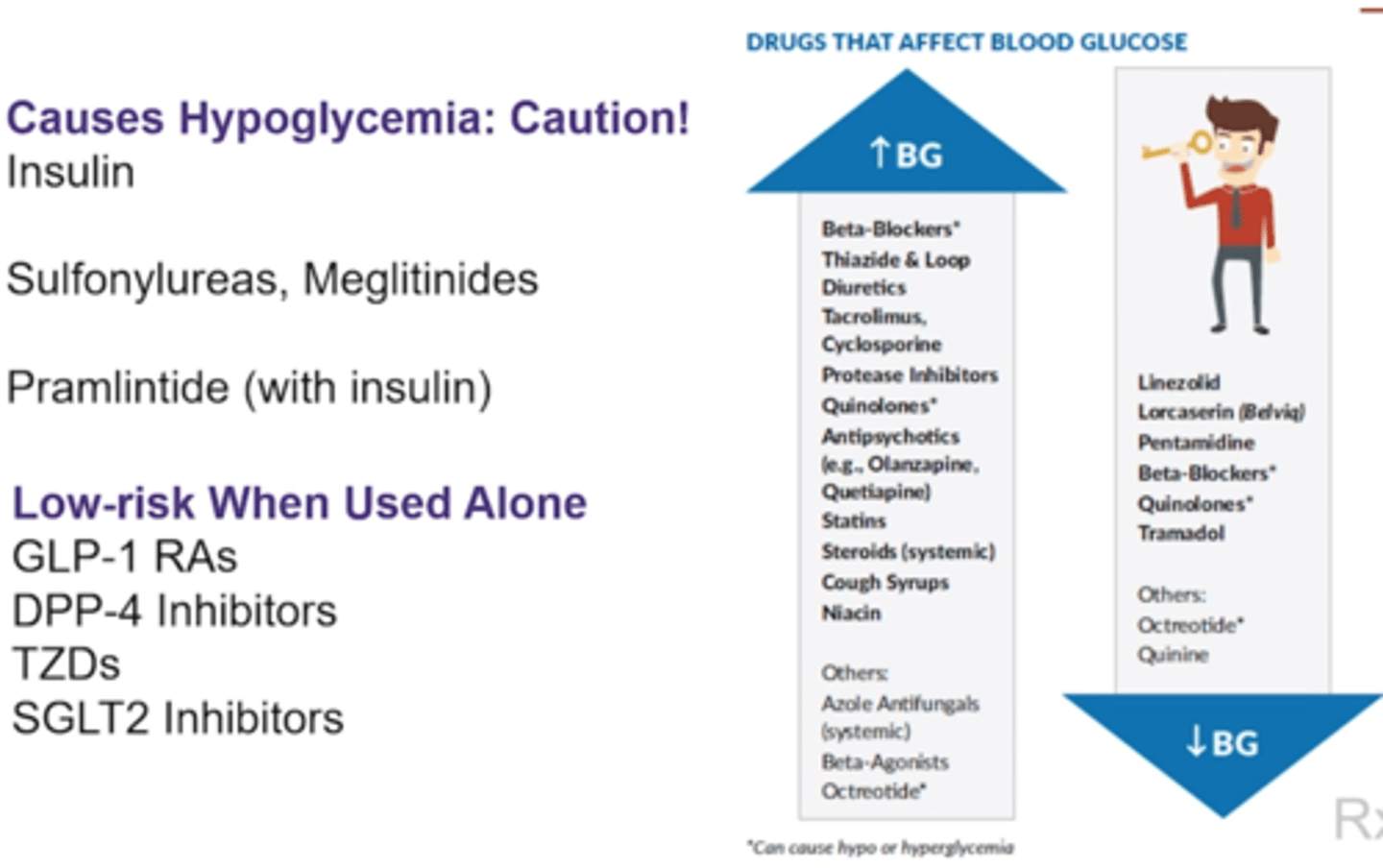
What key drugs cause hyperglycemia?
Key Drug Guy p644
- Beta-blockers (causes hypoglycemia too)
-Cough syrups (OTC and Rx)
-Diuretics (thiazides/loops)
-Immunosuppressants (cyclosporine, tacrolimus)
-Niacin
-Protease inhibitors (-navir)
-Quinolones (causes hypoglycemia too)
-Second gen atypical (clozapine, olanzapine, quetiapine)
-Statins
-Systemic Sterioids
DILE drugs
Hydralazine - HTN (vasodilator)
Procainamide - Class 1a antiarrhythmic Na channel blocker
Methyldopa?
Amiodarone (not as often, class 3 k blocker)
Quinidine (afib class 1a)
Procainamide (afib 1a)
Minocycline - Tetracycline
Methimazole - used as T4 inhibi for hyperthyroidism (less liver tox than PTU)
PTU - hyperthyroid drug
Isoniazid (INH)
Metoprolol tartrate IV conversion
Metoprolol tatrate IV is not equivalent to PO (IV:PO ratio is 1:2.5)
Carvedilol Conversion
Carvedilol (coreg) is 1 BID:3.2 qd CR tab
Steroid equivalency (hydrocortisone, prednisone, methylprednisolone, dexamethasone)
Lithium calculations
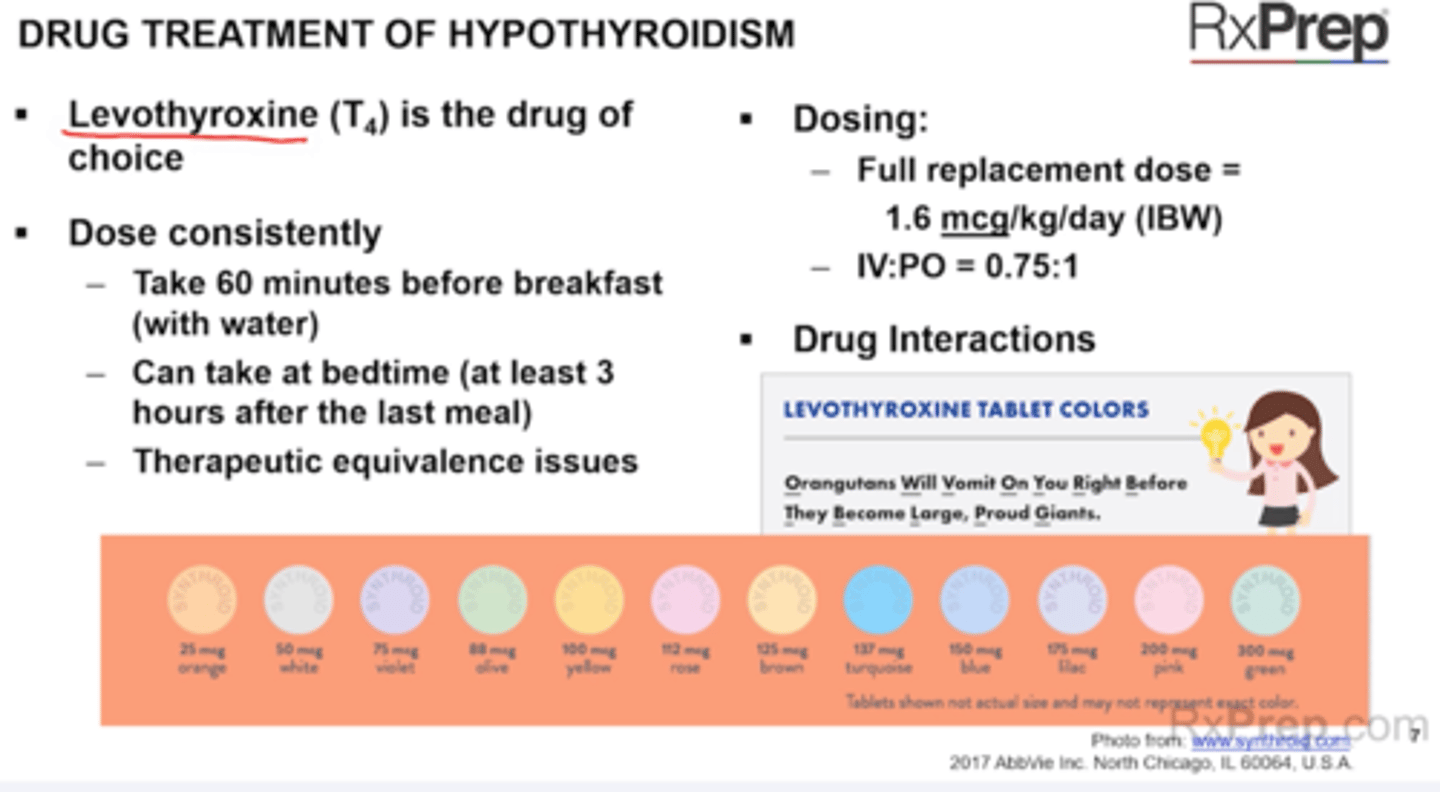
Levothyroxine tablet colors
Full replacement dose = 1.6 mcg/kg/day IBW
IV:PO = 0.75:1
CAD patients (MI, UA) take 12.5-25 mcg/day
Orangutans will violet on your rose before they become lilac, pink giants
Orange = 25 mcg
White 50 mcg
Violet = 75 mcg
Olive = 88 mcg
Yellow = 100 mcg
Rose = 112 mcg
Brown = 125 mcg
Turquoise = 137 mcg
Blue = 150 mcg
Lilac = 175 mcg
Pink = 200 mcg
Green = 300 mcg
HF doses to know
1. ACEi (REQLC)
+ Rapamil (Altace) = 10 mg QD
+ Enalapril (Vasotec) 10-20 mg BID
+ Quinpril (Accupril) (A 20 mg BID
+ Lisinopril (Prinivil, Zestril)- 20-40 mg QD
+ Catopril (Capoten)- TID
2. ARBs
+ Losartan (Cozaar)
- Target dose: 50-150 mg QD
+. Valsartan (Diovan)
- Target dose: 160 mg BID
Goes from 50-150 qd, then 160 BID
3. ARA
+ Spironolactone (Aldactone)
- Target dose: 25 mg QD or BID
4. Digoxin
- 0.125-0.25 mg PO QD
Target levels of 0.5-0.9 ng/mL
5. Beta Blockers
Beta-1 Selective Beta Blockers
+ Bisprolol
+ Metoprolol succinate ER (Toprolol XL)
- Target dose 200 mg
Non-selective Beta Blocker and Alpha=1 Blocker
+ Carvedilol (Coreg)
Target
< 85 kg = 25 mg BID
> 85 kg = 50 mg BID
6. Ivabradine
Target: resting heart rate between 50-60 BPM
ACS Benefits of BB (given w/i 24 hours and continue outpatient)
Beta Blockers
+ Oral, low dose BB (Beta-1 selective blockers without ISA preferred) should be started within the first 24 hours
Beta-1 Selective Agents (AMEBBA)
+ Atenolol (Tenormin)
+ Metoprolol (tartrate - Lopressor IV, succinate Toprolol XL)
+ Esmolol IV (Brevibloc)
+ Bisoprolol
+ Betaxolol
+ Acebutolol (has ISA) NO!
If have HFrEF use bisoprolol, metoprolol succinate, or carvedilol)
Might need to use IV BB - metoprolol Tart, Esmolol, Labetolol
ACEi = start in 24 hr
+ PO ACEi should be started within first 24 hours and continued indefinitely in all patients with LVEF <40%
+ Don't use IV ACE in first 24 hrs d/t risk of Hypotension (Enalaprilat - vasotac)
+ Can use ARB if ACEi intolerant
+ ALL PATIENTS SHOULD BE ON AN ACEi = ASCVD
Ascites treatment ratio
Ratio of 40 mg furosemide to 100 mg spironolactone to maintain potassium balance
40 lasix : 100 spiro
G6PD deficiency drugs
Nitrofurantoin
Bactrim
Opioid conversion
Bipolar Disorder
Drug treatment
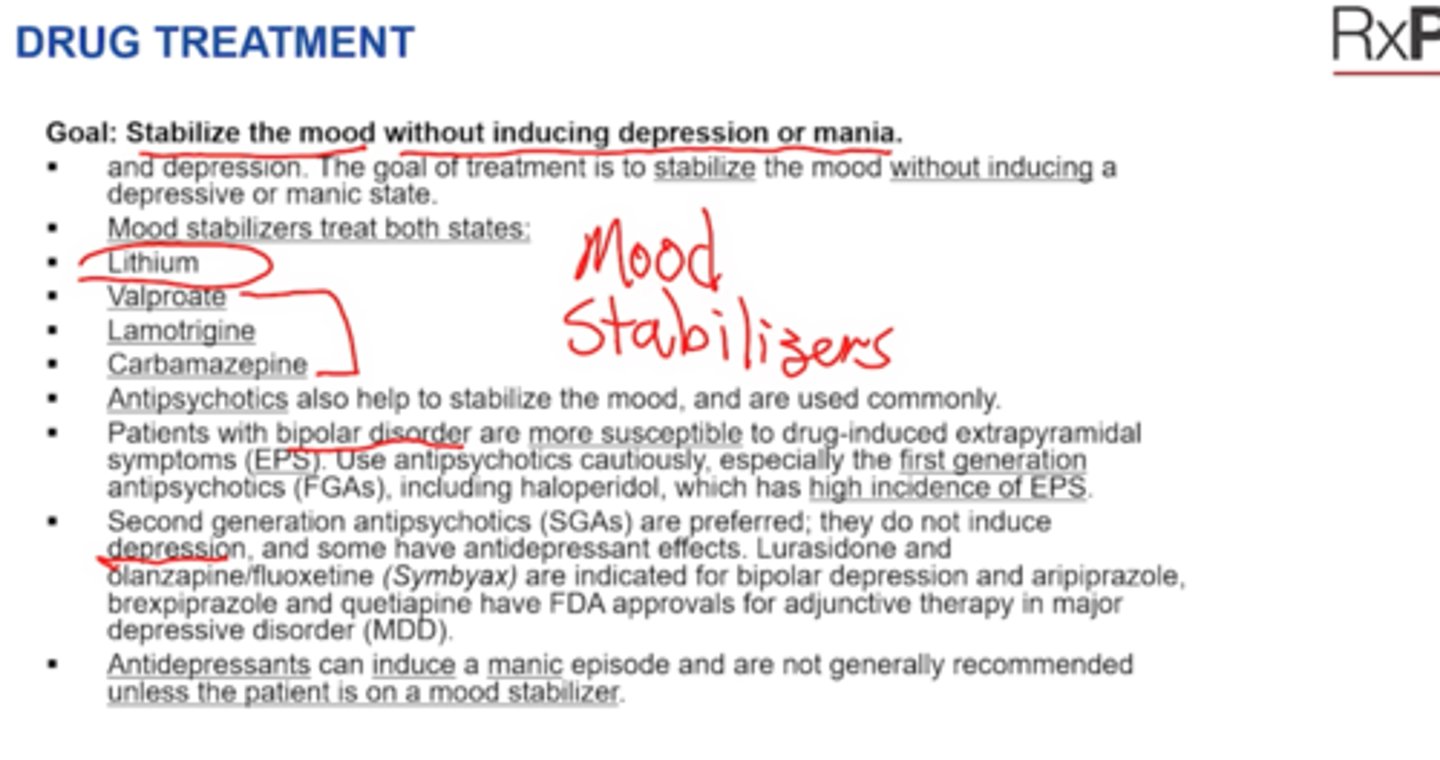
Bipolar Disorder
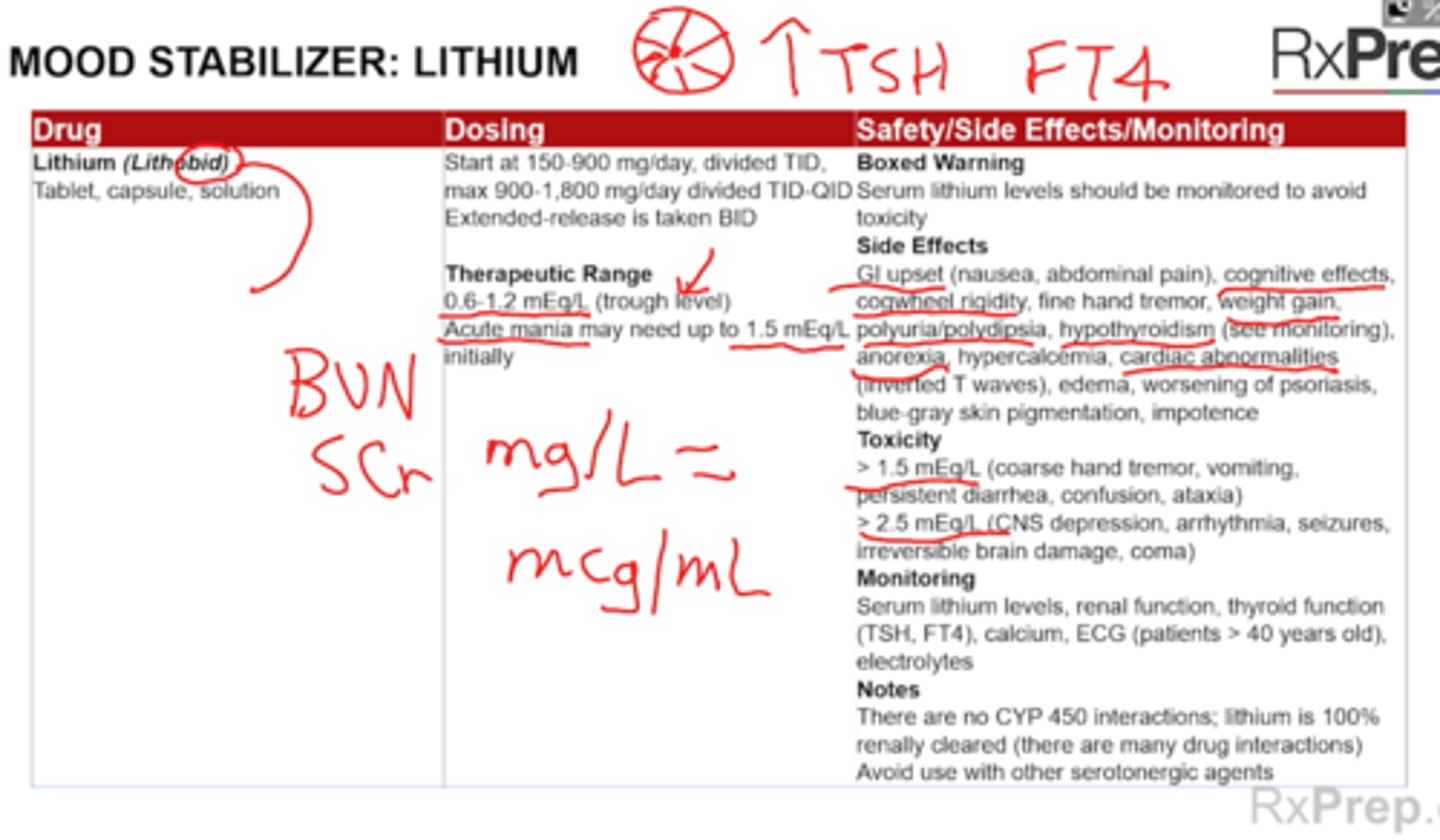
Lithium
Drug treatment
5 mL Lithium citrate syrup = 8 mEq of lithium ion
8 mEq of lithium ion = 300 mg lithium carbonate tabs/caps
Pharmacogenomics
Definitions
Study of inherited variations of genees to deterimine a patients response to a drug
Dominant vs recessive
+ Dominant needs 1 copy
+ Recessive needs 2 copies
Nucleotide = basic structural unit of DNA named based on nitrogenous bases (AGTC)
+ Gene = stretch nucleotides that codes for a single protein
+ DNA = genetic material that is the main componenet of chromosome (double helix)
+ Chromosome = made up of many genes that cary the genetic info
+ SNP (single nucleotide polymorphism = change in single nucleotide in a genetic sequence
Required/Strongly Recommended Genomic Testing
Pharmacogenomics
Key Drug Guy p
HLAB Genes
Abacavair (Ziagen) and combo products (Triumeq) --> HLAB*5701 = increase hypersensitivity risk
Azathioprine --> TPMT; decreases activity = increases myelosupression
Carbamazepine (Tegretol) --> HLAB*1502 = increase hypersensitivity risk
Allopurinol is HLA-B
Cetuximab (Erbitux) and panitumumab (Vectibix) --> KRAS neg, if neg = avoid poor response
Trastuzumab (Herceptin), ado-trastuzumab emtanside (Kadcyla), Iapatinib (Tykerb) and pertuzumab (Perjeta) --> want HER2 pos; if neg = avoid not effective
Warfarin - VKORC1
Metabolized by 2C9, S is more potent than R
Pharmacogenomics
Study Tip Gal
Does a positive or negative require action
POSITIVE:
1) HLA-B testing = hypersensitivity increased risk = avoid drug (Abacavair, Triumeq), Carbamazepine (Tegretol)
2) KRAS mutation positive = poor response to drug = avoid (Cetuximab, panitimumab)
NEGATIVE
1) HER2 negative = avoid HER2 inhibitors HERceptin/Trastuzumab
Pharmacogenomics
Consider genetic Testing
Ex: clopidogrel (Plavix) - test for CYP2C19 (used for ACS, PAD, stroke)
1 allele is normal
Poor metabolizers 2C192 and/or 2C193 alleles) will not convert drug to active form = higher CV event rates
Consider alternative therapy
Pharmacogenomics
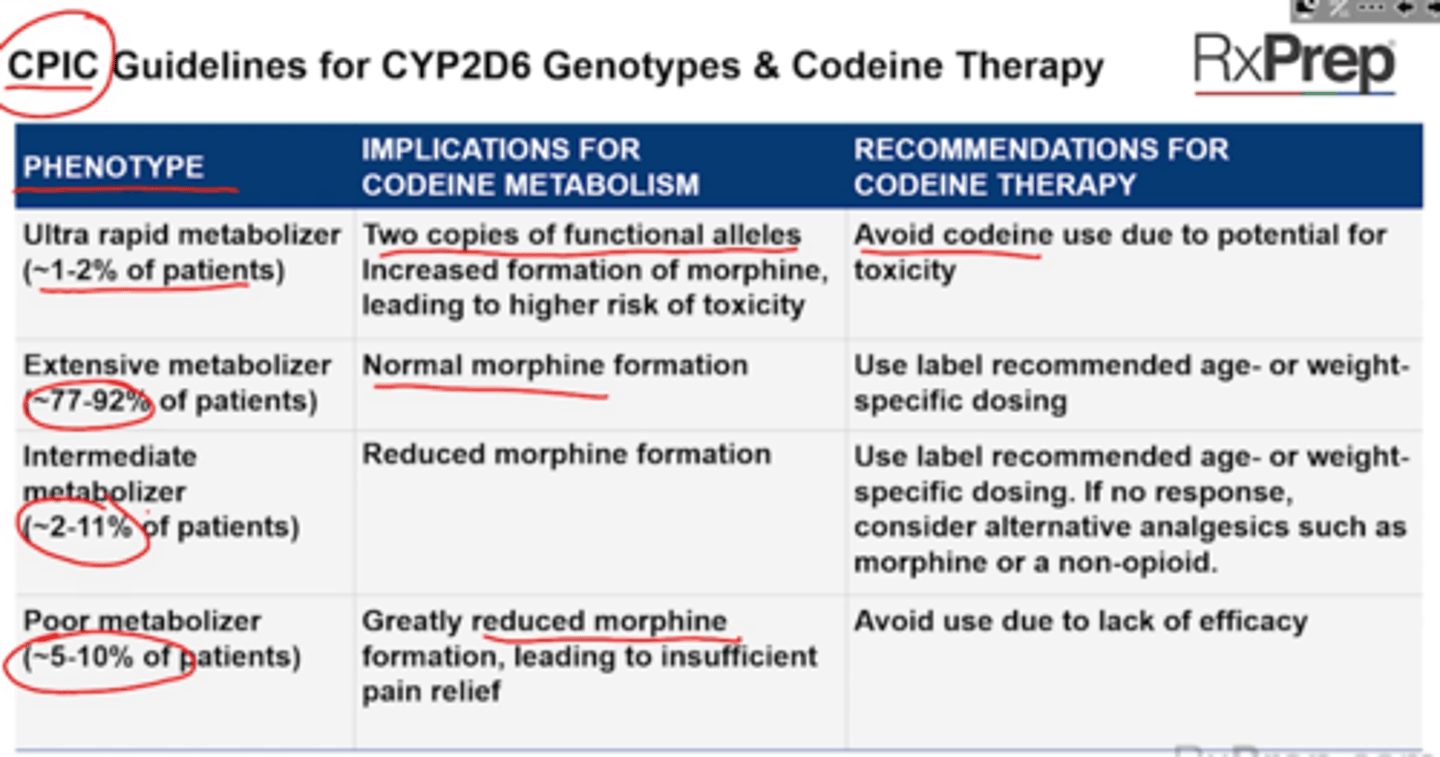
CPIC Guidelines for CYP2D6 Genotypes and Codeine
Ultra rapid = avoid due to toxicity risk (increased morphine formation = higher tox= respiratory depression or death)
Extensive metabolizer = use label recommended age or weight specific dose (normal morphine formation)
Intermediate metabolizer = reduced morphine formation - use label recommended, if no response use alternative
Poor metabolizer = greatly reduced morphine = avoid use b/c lacks efficacy