Addiction Part 3 Opiods, Cannabis
1/20
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
21 Terms
Opioids intoxication effects
Euphoria, drowsiness, slowed breathing—It allows everything to calm down and slip away. You aren’t’ thinking so much, you merely zone out.
Death due to depressed respiration—You can die from opioids because your breathing slows down so much that you suffocate and die from it.
Opioid withdrawal effects
Nausea, chills, diarrhea, insomnia—it’s like a super bad flu for a bunch of days. But, assuming you don’t have a really bad health condition, you won’t die from it.
Biological etiological factors of opioids
Enkephalin and endorphin systems—enhance the effect of the body’s natural pain killers
It’s mainly negative reinforcement—it removes unpleasant stuff—rather than adding pleasant stuff
Three treatment methods for biological-etiology factors
Methadone
Buprenorphine
Naltrexone
Methadone
An opioid, but stronger than painkillers you have in your own home. It is a safer type of opioid because its given in monitored dosages from a medical professional
Research shows that this greatly improves the individuals overall quality of life, but a lot of people will fall out of the program because they have a tough time following the guidelines
Buprenorphine
A partial opioid agonist. It targets the same receptor sites as morphine and heroine, but it is not as strong as methadone.
When people come off of methadone, the withdrawal effects are less intense if taking Buprenorphine
Some evidence indicates that it’s an effective stop-smoking agent.
Naltrexone
Blocks you from receiving a high from an opioid, and it also seems to help with the cravings. But, if the person decides that they do want to do heroine, it’s easier for them to overdose with the naltrexone, as they won’t feel the effects, so they’ll take more of the drug.
Psychological-etiological effects of opioids
Withdrawal symptoms prompt re-use—if people are afraid of withdrawal, they will stay on the drug to avoid the withdrawal
Sensation seekers vs. emotional copers—people take the drugs both for the sensation, but also to cope with trauama and physical pain (emotional copers)
Treatment for opioids
Narcotics Anonymous—typically less effective than traditional AA
CBT—?
Harm reduction—methadone programs, helping people with housing
Ex. In places like Norway and Sweden, they have “heroine ice cream trucks” that drive around treating people
Cannabis
Contains numerous substances, unlike alcohol, which just contains alcohol
There are more than 100 different types of cannabinoids
Key types of cannabinoids in cannabis?
(Most popular) THC—the one that gets people high
(Most popular) CBD—does not get people high; its more of a relaxation effect
There is also terpenes, CBN, and CBG, which are getting more popular, though there is no research on what they do
Intoxication effects of cannabis (part 2)
Intoxication effects of cannabis (part 1)
Paranoia, hallucinations, dizziness—happens if you smoke a whole bunch
There is cannabis induced psychosis, though it’s more likely to happen if you have the genetic predisposition of schizophrenia, though if the THC levels are super potent, you can have it without the predisposition
Intoxication effects of cannabis (part 3)
Tolerance—chronic and heavy users report tolerance, especially to the euphoric high
Sensitisation—regular users often experience more pleasure from the drug after repeated use
Additional effects of THC
No evidence to date that pure THC having causes lung cancer
Some research shows that using cannabis can help people recover from a traumatic brain injury
It’s impossible to overdose on marijuana
Cannabis withdrawal effects
Irritability, appetite loss, difficulties sleeping—tends to be very mild for those who come off, although if you smoke cannabis super intensively, then you can have fairly intense withdrawal effects, though that’s still fairly rare
Biological-etiological effects of cannabis
Endocannabinoids—your body’s natural versions of THC and other cannabinoids
Sensitization—occasionally people will become more sensitized to weed overtime, but this is rare
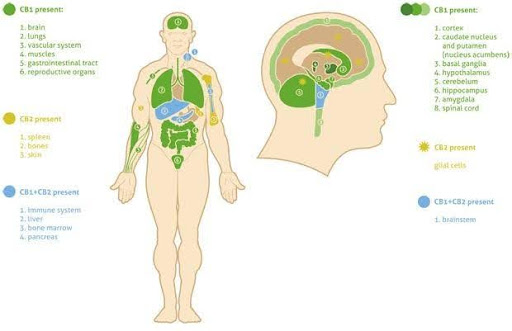
Receptor cites for cannabis
All of the coloured portions are parts of your body with a receptor cite for cannabis
Some research shows there are more receptor cites in the brain for cannabis than for GABA and glutamate, though this is not necessarily true
Treatment for biological effects of cannabis
Treat comorbid conditions—essentially, if you smoke weed because of depression, the therapist will treat the depression
Psychological-etiological effects of cannabis
Motivations for use—why are you using the weed?
Ex. Is it because you are depressed, you want to get high, or because you enjoy having it while going to concerts (if so, then keep going to the concerts without the weed, and eventually you’ll love them again)
Treatment for psychological factors of cannabis
CBT relapse prevention—when the client relapses, the therapist says that an individual just had a bad weekend which is why they relapsed. It’s just a small slip, which doesn’t mean you are fully back to the life you didn’t want to. This is in contrast to AA, as sometimes when people relapse in AA, they really spiral, because they teach it’s the end of the world.
Harm reduction—-? No notes