Cardiopulm Bootcamp
1/77
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
78 Terms
Which of the following is the MOST LIKELY treatment?
a. bicarbonate infusion to decrease metabolic acidosis
b. have the patient breath into a rebreathing mask to decrease respiratory alkalosis
c. fluid and saline infusion to decrease metabolic alkalosis
d. use of supplemental oxygen to decrease respiratory acidosis
d. use of supplemental oxygen to decrease respiratory acidosis
Which of the following exercises would be MOST LIKELY recommended for this patient?
a. inspiratory muscle training
b. pursed lip breathing exercises
c. segmental breathing exercises
d. incentive spirometry
b. pursed lip breathing exercises
the PT decided to use postural drainage for airway clearance. the PT positions the patient in a seated position leaning forward over a folded pillow. based on this position, which lobe is MOST LIKELY being drained?
a. posterior apical segments of upper lobe
b. anterior apical segments of upper lobes
c. superior segments of the lower lobes
d. anterior basal segments of lower lobes
a. posterior apical segments of upper lobe
Postural Drainage
bronchus of the involved lung segment is perpendicular to the ground using gravity, these positions assist the mucociliary transport system in removing excessive secretions from the tree
postural drainage indication
pulmonary complications
weak/elderly patients
atelectasis, pneumonia, COPD
maintain each position for 5-10 minutes
secretions cleared by coughing or suctioning
superior segment of lower lobe postural drainage
prone lying on a bed with two pillows under the pelvis
posterior apical segments of the upper lobes postural drainage
sitting on a chair, leaning forward over a folded pillow
anterior segments of upper lobes postural drainage
supine lying on a bed with pillows under the knees
anterior apical segments of the upper lobes postural drainage
sitting in a recliner leaning slightly backward
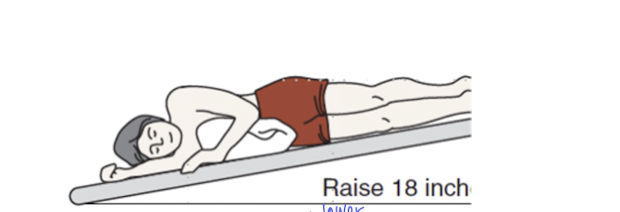
a clinician is educating the patient’s parents on postural drainage. the clinician places the patient in a position, as shown in the image below. Which of the following segments of the lungs is MOST LIKELY being drained?
a. right lateral basal segment
b. right middle lobe
c. left lingular segment
d. left lateral basal segment
d. left lateral basal segment
contraindications to postural drainage - precautions
pulmonary edema, hemoptysis, massive obesity, large pleural effusion, massive ascites
contraindications to postural drainage - relative contraindications
increased intracranial pressure, hemodynamically unstable, recent esophageal anastomosis, recent spinal fusion or injury, recent head trauma, diaphragmatic hernia
a patient with chronic congestive heart failure was recently admitted to the hopsital. Which of the following plans for prophylactic respiratory care is most likely to be contraindicated?
a. frequent turning and positioning ever 2 waking hours
b. gentle percussion 2 times per day
c. vigorous chest vibrations, with the foot of the bed elevated 4 times per day
d. gently coughing and deep breathing exercises every 4 hours
c. vigorous chest vibrations, with the foot of the bed elevated 4 times per day
Age Predicted Heart Rate
HR max = 220 - age
HR max = 207 - 0.7xage
Karvonen’s formula
heart rate reserve multiplied by the percentage of intensity plus resting heart rate
HR Reserve = HR max - HR Rest
an older adult presents with limited endurance but has no history of cardiopulmonary disease. An exercise tolerance test is negative for coronary artery disease. Which of the following is MOST APPROPRIATE initial aerobic exercise intensity for this individual
a. 90-100% HR max
b. 60-70% HR max
c. 40-50% HR max
d. 30-40% HR max
b. 60-70% HR max
a clinican is supervising a patient with a history of cardiovascular disease during an exercise session.
Baseline vitals: HR = 72 bpm, SpO2= 98%, BP 116/78 mmHg
Which of the following findings would be considered MOST LIKELY to require termination of exercise?
a. systolic BP increases to 160 mmHg
b. diastolic BP drops to 74 mmHg
c. HR drops to 60 bpm
d. HR increases to 110 bpm
c. HR drops to 60 bpm
Exercise Hypertension
SBP >240 mmHg
DBP >110 mmHg or until controlled
systolic hypotension
>10 mmHg drop of SBP is CAUTION
>20 mmHg drop fo SBP is STOP
unusual heart response
too rapid increase in HR
failure to increase in HR
decrease in HR with increased exercise intensity/duration
exercise termination symptom criteria
significant anginal response
severe leg claudication
undue dyspnea
excessive fatigue
dizziness
exercise termination criteria signs
pallor
cold sweats
ataxia
new murmur
pulmonary rales
onset of significant third heart sound
ECG abnormalities exercise termination
second or third degree heart block
onset of right or left bundle branch block
acute ST changes
Cardiac Rehab Acute Phase
monitoring phase
begins when patient is medically stable
cardiac rehab acute phase: exercise prescription
patient education
hemodynamic and ECG monitoring
Cardiac Rehab Subacute Phase
conditioning phase
begins as early as 24 hours after discharge up to 6 weeks
Cardiac Rehab Subacute Phase : exercise prescription
50-70% HR max
Cardiac Rehab Training Phase (Phase III)
intensive rehab
~5-6 from discharge extends indefinitely
Cardiac Rehab Training Phase exercise prescription
70-85% of HRmax
resistance training begins
Cardiac Rehab Conditioning Phase (Phase IV)
maintenance or prevention
lasts up to 6-12 months
exercise prescription same as phase III
Phase I and II FITT
no resistance training
F - short sesions, 2-3 times a day
I - 50-70% HR max
T - 10-15 minutes (phase I), 30 minutes (phase II) per session
T - ADLs, supervised ambulation
patients commonly undergo a symptom limited maximal stress test at 4-6 weeks post MI
a patient is undergoing cardiac rehabilitation post complicated myocardial infarction in the hospital. on day 2, the clinician wants to progress the patient to sitting. Which of the following is an APPROPRIATE INITIAL task for this patient?
a. make the patient stand and do weight bearing activities
b. make the patient sit on the upright chair during visitor time
c. make the patient sit on reclining chair and check vitals
d. patient is not ready for upright posture yet
c. make the patient sit on reclining chair and check vitals
Phase III FITT
F - 2-3 sessions/week
I - 70-85% of the peack achieved on the test (HR max)
T - 30-60 minutes with 5-10 min of warm up and cool down
T - single mode of training (walking) or multiple modes (treadmill, cycle, ergometer)
Strength Training Phase III Guidelines
begin with the use of elastic bands and light hand weights (1-3 pounts) or 30-50% of max weight used to complete 1RM
begin with 8-10 reps, progress to 12-15 reps
avoid upper extremity resistance as soft tissue is healing
a patient with uncomplicated myocardial infarction has been discharged from acute care. Which of the following activities would be MOST APPROPRIATE during early phaes 2 rehab?
a. 30 minutes walking at 3 mph with no incline
b. 15 minutes of elastic band training with yellow elastic bands
c. 15 minutes upper limb workout with 2lb hand weights
d. 30 minutes walking at 5 mph with 5% incline
a. 30 minutes walking at 3 mph with no incline
Phase IV
location: community centers, YMCA, clinical facilities
exercise: clinically stable angina, medically controlled arrhythmias during exercise
progression: 50-85% of functional capacity, 3-4/week, 45 minutes or more/session
discharge: typically, 6-12 months
Cardiac Rehab Educational Component
disease process and prognosis
individual’s risk factors and recommendations for behavior modification
general activity guidelines: role of exercise, activity pacing, HEP
medications
nutrition and prescribed diet
self monitoring techniques
what to do in an emergency
a patient with a BMI of 31 kg/m has been walking 3 days/weel for 20 minutes, for the past 3 weeks. Which of the follwoing modifications is MOST APPROPRIATE to achieve the goal of weight loss?
a. walk 6 days/week at current walking speed and increase the duration to 45 minutes
b. increase the walking speed and keep duration at 20 minutes
c. walk 5 days/week and decrease duration to 10 minutes
d. decrease the walking speed and increase the duration at 25 minutes
a. walk 6 days/week at current walking speed and increase the duration to 45 minutes
Weight Reduction Guidelines for Obesity
minimum: 250-300 min/week required
frequency: greater than 5 days/week to maximize caloric expenditure
intensity: initially moderate - 40-60% VO2, progression to >60%
time: 45-60 min/day
type: moderate exercise - aerobic, resistance, and flexibility
Sinoatrial Node
pacemaker
initiates depolarization
atrioventricular node
passess depolarization to ventricles
brief delay to allow for ventricular filling
bundle branches
to left and right ventricle
purkinje fibers
throughout ventricles
electrocardiogram
records the electrical activity of the heart
P wave (ECG)
atrial depolarization
QRS complex (ECG)
ventricular depolarization and atrial repolarization
T wave (ECG)
ventricular repolarization

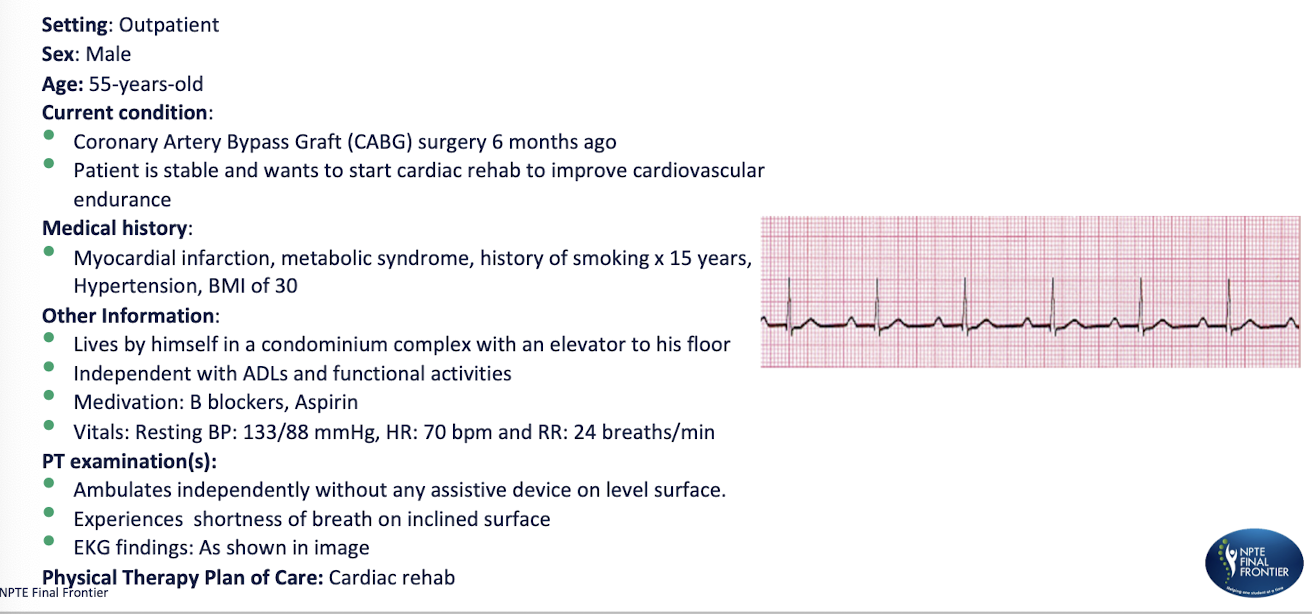
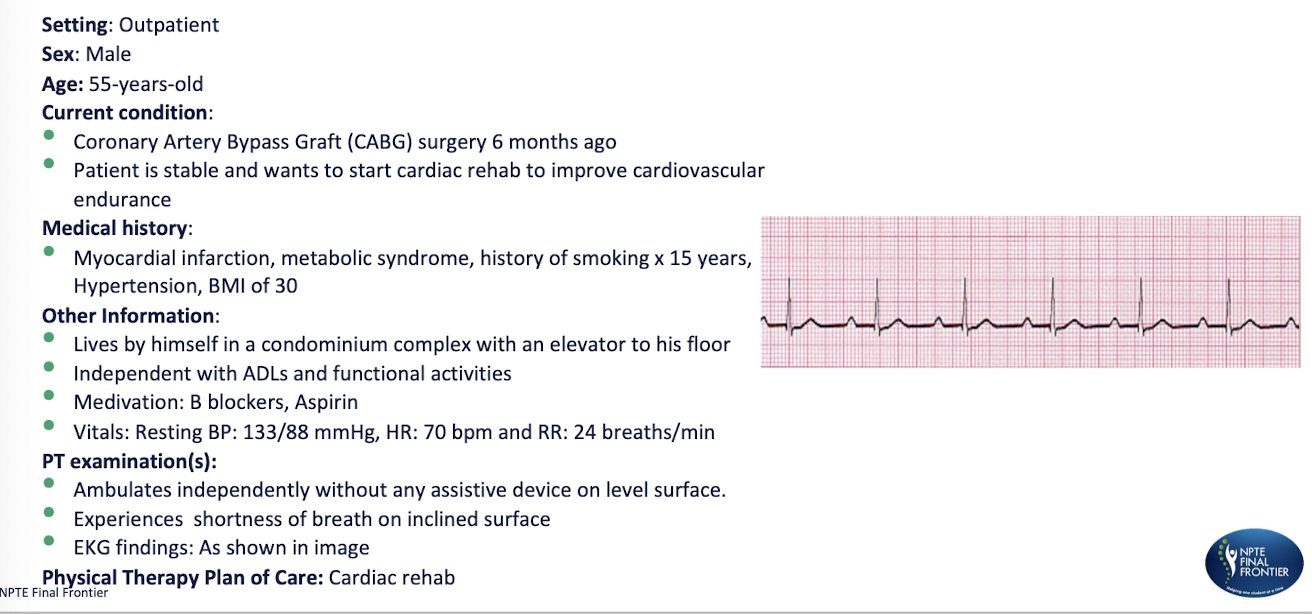
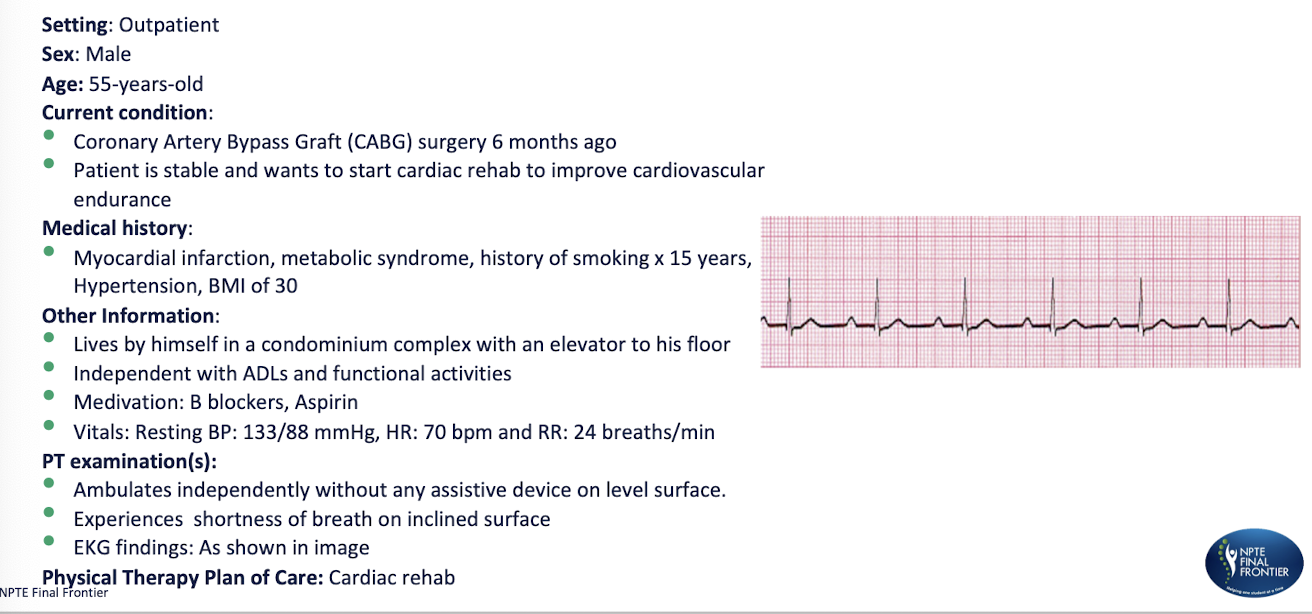
A PT examines the output from a single lead ECG of a patient in an inpatient clinic. the 6 second ECG strip is shown in picture below. What should the PT determine the heart rate of the patient as?
a. 110 bpm
b. 70 bpm
c. 90 bpm
d. 60 bpm
c. 90 bpm
AV Block: 1st degree heart block
delay in conduction
AV Block: 2nd degree
partially blocked conduction
AV Block: 3rd degree
fully blocked conduction
1st degree AV nodal disease
PR interval > 0.2 seconds
each P is followed by a QRS
seen also in athletes, with increased vagal tone (activity)
generally won’t progress benign condition
2nd degree block
Mobitz or Wenckebach
dropped QRS
increased time between P and QRS start - increasing PR interval before the QRS is dropped, cycle repeated
pattern can be discerned
disease of the AV node
2nd degree block type 2
Mobitz type II
PR intervals constant and QRS dropped intermittently
no discerned pattern
disease of the bundles of his and purkinje fibers
3rd degree AV block
the atrial rate is independent of the ventricular rate (P wave and QRS march out separately)
no relationship at all, of the PR intervals
the PR interval is constantly changing and the QRS is usually wide and bizarre because it is ventricular origin
While walking on a treadmill the PT sees the ECG pattern, as shown. What is the MOST APPROPRIATE diagnosis?
a. first degree heart block
b. Mobitz type I heart block
c. Mobitz type II heart block
d. third degree heart block
a. first degree heart block
Based on the diagnosis condition what would be the MOST APPROPRIATE response by the phyiscal therapist?
a. stop the treadmill session immediately and contact the cardiologist
b. continue exercising at the current intensity without any modifications
c. lower the exercise intensity and monitor patient closely
d. have the patient rest, then reassess before resuming exericse
b. continue exercising at the current intensity without any modifications
the patient did not come for PT for 3 consecutive visits. On following up with the patient’s caretake they mentioned thart the patient was taken to the ER as they were experiencing increased SOB at rest and cough with no evident peripheral edema. Which of the fllowing is MOST LIKELY cuasing the patient’s symptoms?
a. biventricular heart failure
b. right sided heart failure
c. cor pulmonale
d. left sided heart failure
d. left sided heart failure
myocardial ischemia
decreased blood supply
ST segment depression
T wave flattened or inverted
myocardial infarction
complete occlusion of blood supply and cell death
ST segment elevation
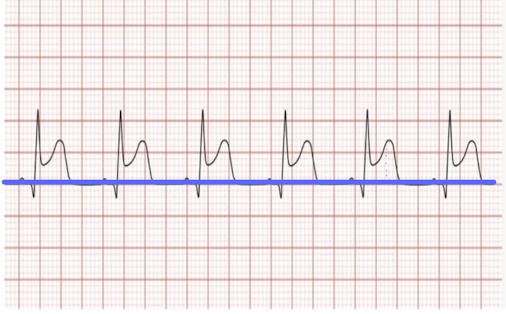
A patient is walking on a treadmill with ECG leads attached. The PT observes the ECG as shown in the image below. What is the MOST LIKELY diagnosis and intervention?
a. myocardial ischemia that has an elevation of the ST segment greater than 1 mm and the PT should stop the protocol
b. myocardial infarction that has an elevation of the ST segment less than 1 mm and the PT should stop the protocol and call 911
c. myocardial ischemia that has an elevation of the ST segment less than 1 mm and the PT should stop the protocol
d. myocardial infarction that has an elevation of the ST segment greater than 1 mm and the PT should stop the protocol and call 911
d. myocardial infarction that has an elevation of the ST segment greater than 1 mm and the PT should stop the protocol and call 911
atrial tachycardia rate
100-250 bpm
atrial flutter rate
250-350 bpm
atrial fibrillation rate
400-600
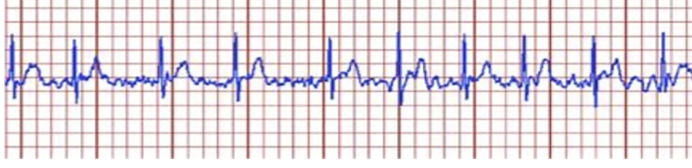
a physical therapist is ambulating a patient and they report palpitations, SOB and fatigue. What should be the interpretation and immediate action according on the ECG strip shown below?
a. ventricular fibrillation, call for a defibrillator
b. premature ventricular contractions; take them to their bed and monitor for changes in ECG
c. atrial fibrillation; stop exercise and report the physician
d. 3rd degree heart block; activate emergency
c. atrial fibrillation; stop exercise and report the physician
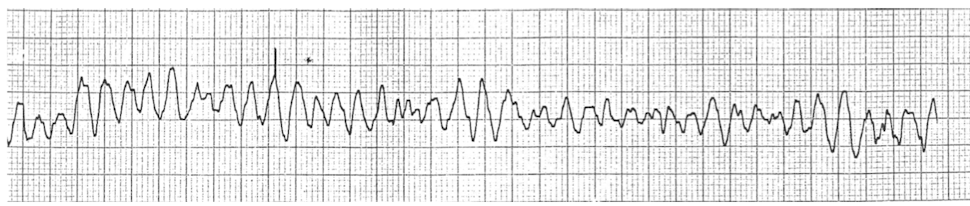
while exercising a patient on the treadmill, the PT notices the ECG as shown in the image. What should their INITIAL response be?
a. continue walking at same intensity
b. continue walking at lower intensity
c. stop the treatment and monitor ECG for 10 minutes
d. activate the emergency system or call 911
d. activate the emergency system or call 911
premature ventricular contraction
heartbeat initiated by purkinje fibers; skipped beat or palpitations
ventricles contract before the atria, cannot be filled optimally
no P, wide bizarre QRS
PVCs that occur 3 or more in a row - ventricular tachycardia
bigeminy
1 normal beat followed by 1 PVC
trigeminy
2 normal beats followed by 1 PVC
multifocal PVC
more than 1 PVC is present and 2 do not appear similar in configuration
STOP exercise and immediately refer (call 911)
couplet
2 consecutive PVCs together with no normal beat between them
stop exercise
if 2 or more couplets, immediately refer (call 911)
Ventricular Tachycardia
3 or more PVC in row
stop and call 911
physical therapist is working with a patient who is 4 months post myocardial infarction, in a cardiac rehab facility. Upon increasing the workload, the PT observes a unifocal PVC on patients ECG. which of the following is the MOST APPROPRIATE action by the PT?
a. continue to exercise and increase intensity
b. stop exercise because patient is undergoing ischemia
c. keep exercising at lower intensity; consultation with physician is not required here
d. stop exercise and consult with phyisican before starting any exercise
c. keep exercising at lower intensity; consultation with physician is not required here
a clinician is auscultating a patients lungs. During auscultation the clinician hear low pitched gurgling and snoring sounds. Which of the following sounds is the clinician MOST LIKELY hearing?
a. vesicular
b. wheezes
c. bronchial
d. rhonchi
d. rhonchi
a patient with dyspnea on exertion and has an FEV1/FVC ratio of 65%. They report chest tightness and frequent coughing. Which lung volume would be decreased compared to a patient with a healthy pulmonary system?
a. functional residual capacity
b. residual volume
c. total lung capacity
d. expiratory reserve volume
d. expiratory reserve volume
when a physical therapist auscultates the paitent’s heart, they hear an S4 sound. When can this heart sound be heard and what condition does it MOST LIKELY indicate?
a. abnormal sound heard in early diastole; congestive heart failure
b. abnormal sound heard in late diastole; congestive heart failure
c. abnormal sound heard in early diastole; myocardial infarction
d. abnormal sound heard in late diastole; hypertension
d. abnormal sound heard in late diastole; hypertension
a patient demonstrates an increased residual volume on pulmonary function testing. Which of the following conditions is MOST LIKELY responsible for this finding?
a. parkinson disease
b. pregnancy
c. scoliosis
d. emphysema
d. emphysema
a physical therapy initiates aquatic therapy at chest depth water level for a patient with general reconditioning. which cardiovascular response is most likely to occur during immersion?
a. decreased venous return
b. increased heart rate
c. increased venous return
d. decreased stroke volume
c. increased venous return