Part 4: Calcium Balance
1/16
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
17 Terms
Why is calcium critical for normal physiology
six reasons
Intracellular signaling
Hormone secretion
Recall insulin lecture and how calcium entry increases insulin
Blood clotting
Neural excitability
Muscle contraction
Building & maintaining bone
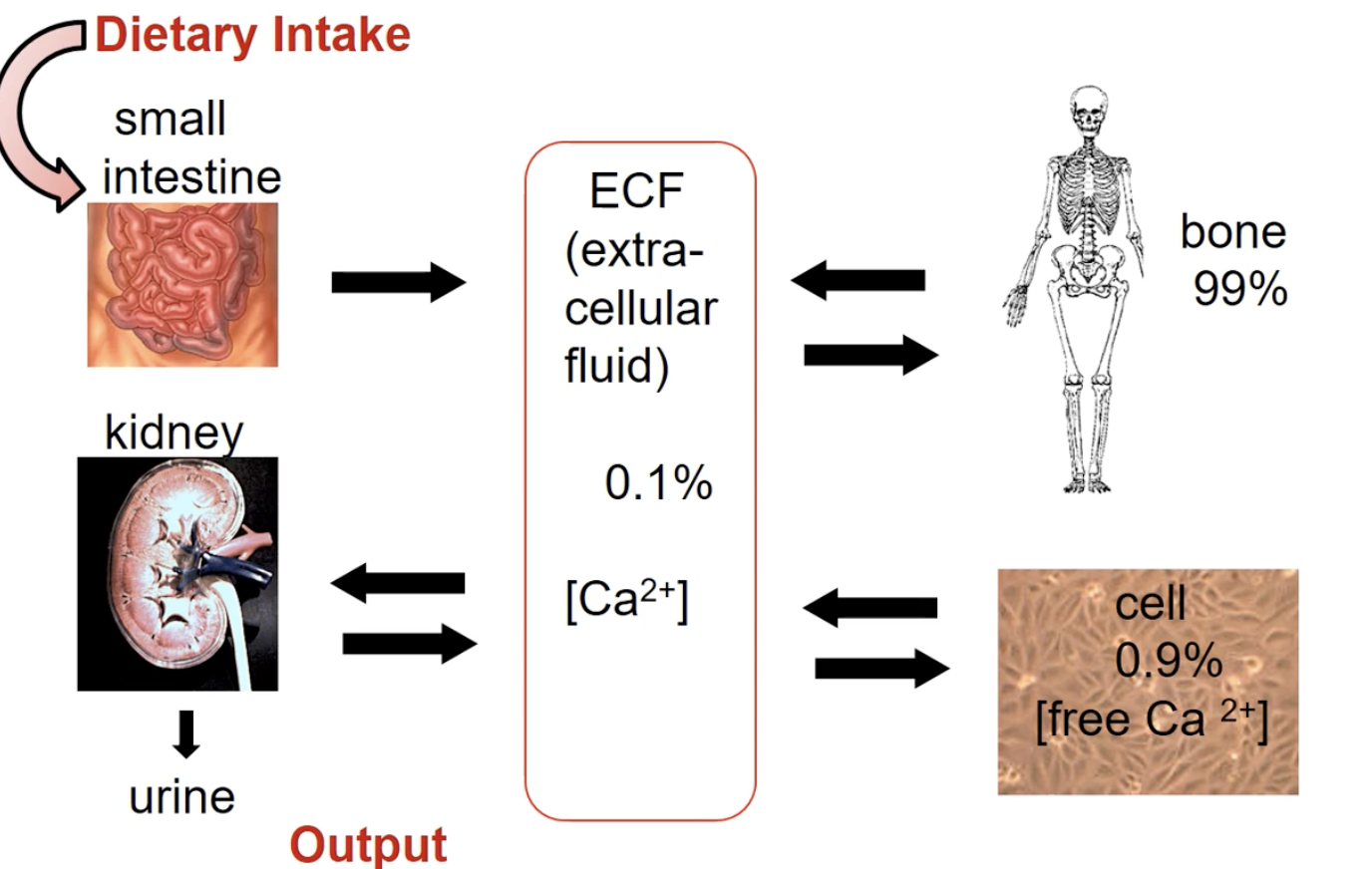
Three locations of calcium
Two places where it is found in the body + percentages
What is special about calcium and its movement?
extracellular matrix
extracellular fluid
intracellular Ca2+
Bone: 99%
Cell: 0.9%
Extracellular fluid: 0.1%
Movement
Cells and bones and output and input with ECF
Dietary intake to small intestine where it gets absorbed and into the ECF and into bone/cells
Out calcium through kidney and out in the urine
What is a unique characteristics of bone
that most people get wrong? Why do we really need this characteristics of bone for everyday life?
Where is the calcium stored in the bone
not static, constantly being formed and reabsorbed
Purpose: to break away old bone to replace with new bone
Especially for repair or micro fracture repair
Calcium is stored in crystals called hydroxyapatite (calcium + phosphate)
Small portion released ionized and readily exchangeable with the ECF
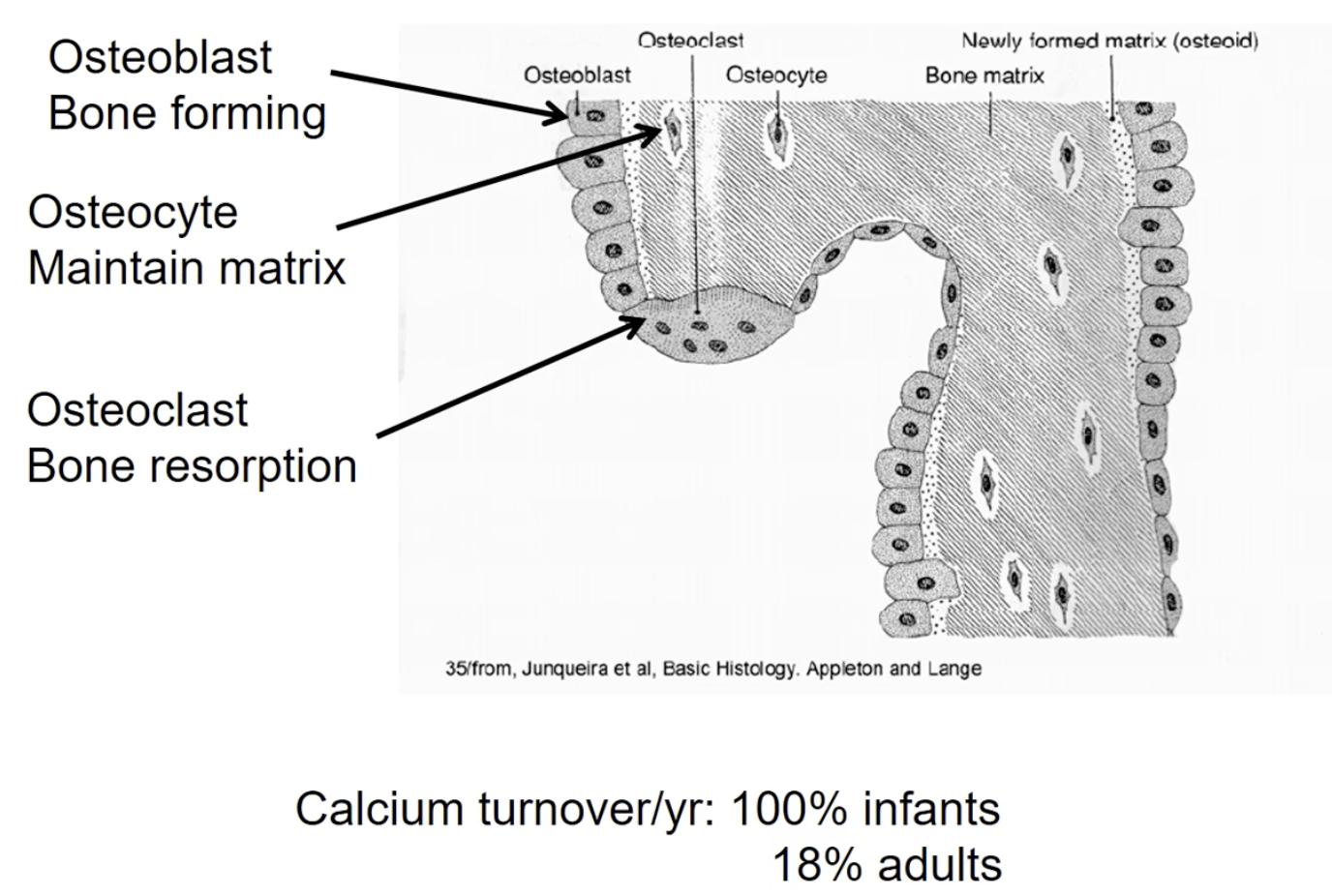
Three cells that make up bone
and their function
How is bone made
Percentage turnover for infants vs adults per year
Osteoblasts: (Hint: B for build) Bone forming cells - laying down matrix
Osteoclasts: (hint: C for cut) Break down bone
Multinucleated - fusion of multiple cells together and therefore really big
Osteocytes: (hint: Sites of maintaining) Maintain bone. (These are previously osteoblasts that are completely surrounded by bone matrix → Therefore just maintain bone in its immediate vicinity
Tract cell
Making bone = creating calcium phosphate complexes)
(calcium crystallization)
Percentage turnover per year
infants: 100%
Adults: 18%
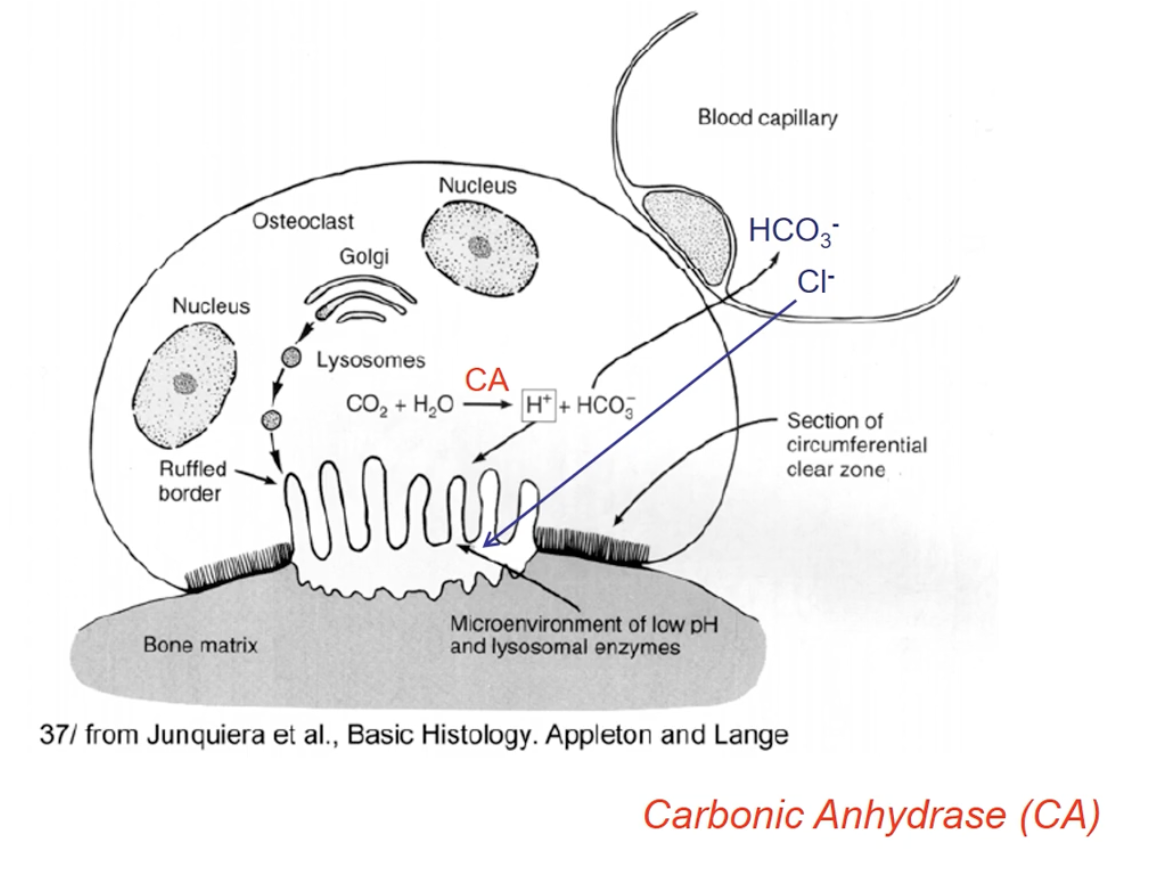
How do osteoclasts break down bone
a.k.a bone resorption
Process
Include the important equation involved
Secretes HCL and proteases
proteases that function well at lower pH and break down the case bone
Breaking down forms a calcium pool which enters the bloodstream
Important equation
Carbonic anhydrase enzyme uses carbon dioxide and water to form free protons and bicarbonate
Bicarbonate goes to the blood capillary
Blood capillary brings in Cl, and proton and Cl form HCl
HCl dissolves the bone first, and then the proteases breaks it down
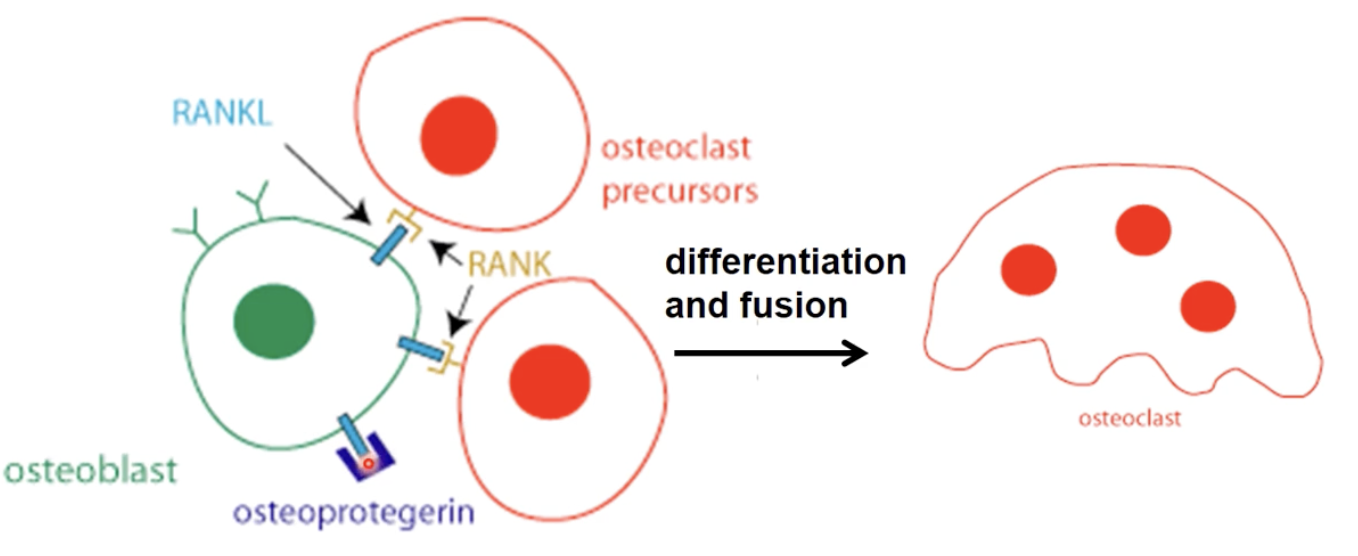
How does osteoblasts and osteoclasts communication with each other?
give a timeline of how it promotes osteoclast formation
How can it be inhibited?
Initially the osteoblasts are restoring bone
Osteoclast precursors have receptors
RANK: receptor activator of nuclear factor kappa B
Osteoblasts have ligands that can bind to the receptors
RANKL: RANK ligands
When the osteoblasts receptors and osteoclasts bind together, the ligand activates the osteoclasts receptors to bind together by differentiation and fusion to form the large osteoclast
Osteoclasts resorbes bone
Inhibiting
OPG (osteoprotegerin) will be secreted by osteoblasts to block RANKL/RANK interactions and no resorbing occurs by binding to the ligand
What is osteoporosis
a condition where there is more bone resorption
What is Denosumab drug?
helps prevent bone loss
A monoclonal antibody
Binds to RANKL to minic OPG and the ligand cannot bind to the osteoclasts
What three hormones control plasma CA2+ levels
jus list them
What are the three target site
Hint: remember how calcium flows around in the body and where it goes
PTH: parathyroid hormone
Calcitriol
Calcitonin
Sites
Bones
Kidneys
Digestive tract
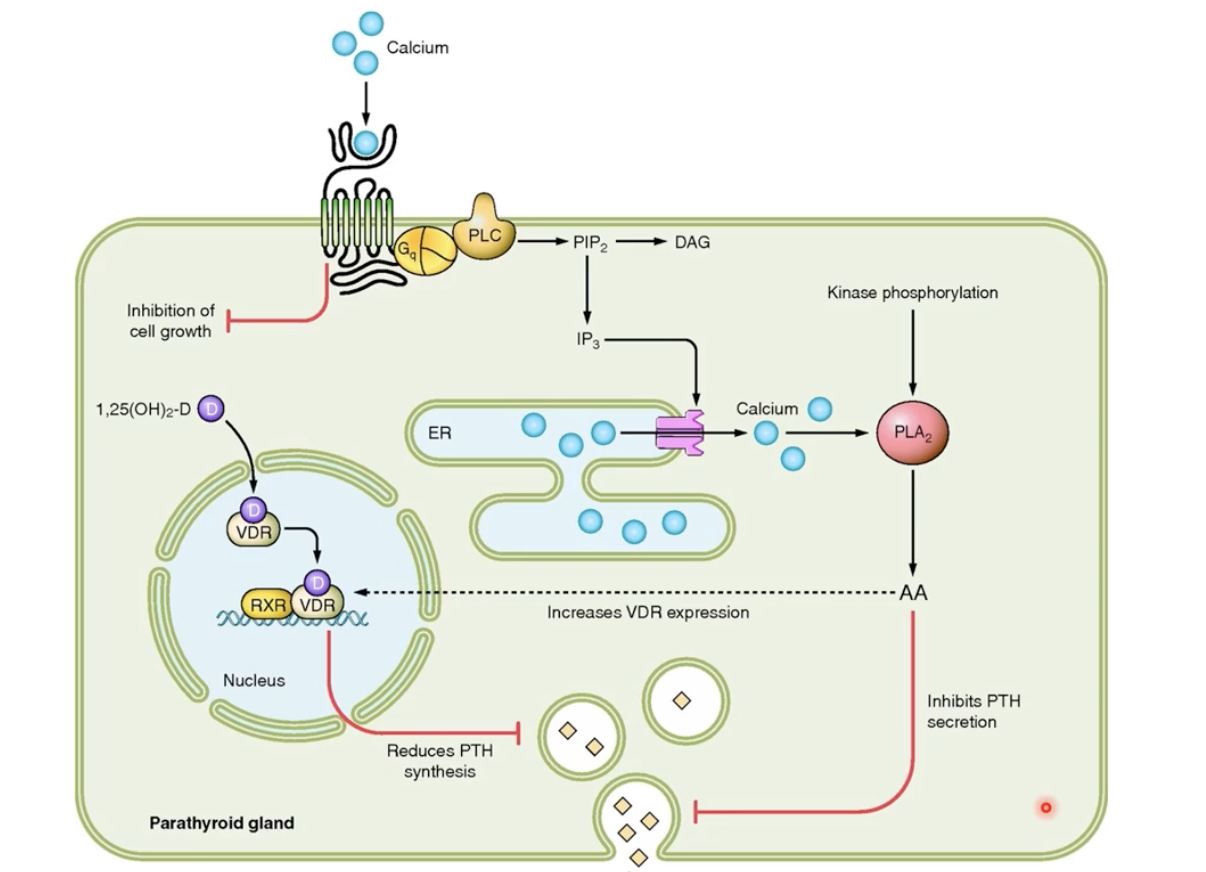
Parathyroid hormone/PTH
What gland involved
Location
Process within their cells
Function
What targets sites and what does PTH tell them to do?
Stimulus
release from the parathyroid glands
Four of them, very tiny, found on the back of the neck, stuck on the the thyroid gland
Process in cells
GQ protein, as long as there is calcium that acts as ligand, results in kinase phosphorylation that inhibit PTH secretion
Kinase phosphorylation also increase vit D3 receptor which prevents the synthesis of the PTH hormone as well
Function: to increase plasma CA2+ concentration
For bone: in osteoblasts increasing cAMP, to increase the release RANKL and decrease OPG (that inhibiting it)
For kidneys: reabsorb the Ca2+ found inside the urine back into the blood
Calcitriol synthesis
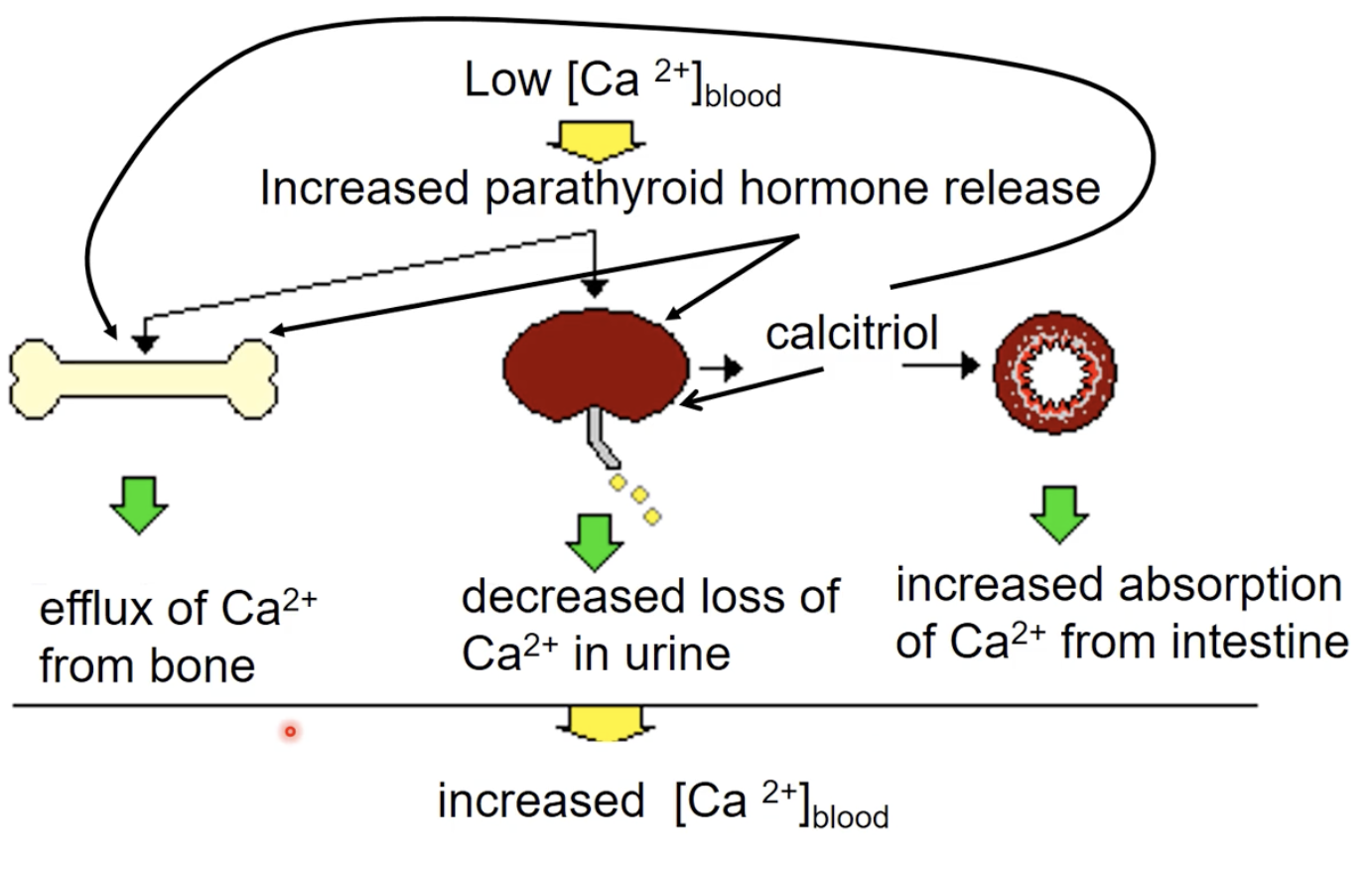
Stimulus low plasma CA2+
Very sensitive: very small range (around 1.2 concentration)
Calcitriol
another common name for it
Which organs help in the development of the hormone
Main function
Targets which organs and what does it do to each?
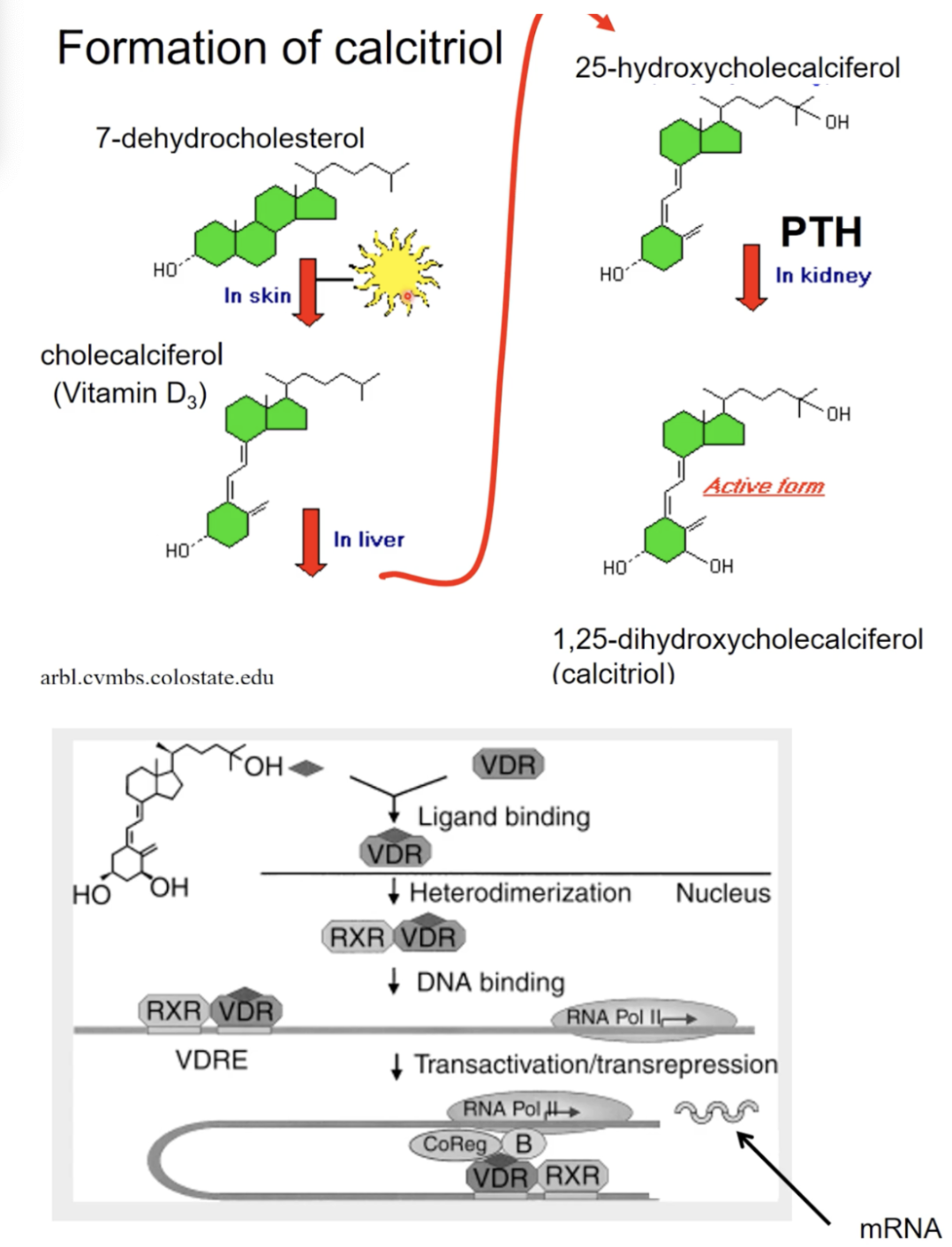
How is calcitriol formed?
Process
The process of calcitriol signalling to target organs
also known as 1,25-dihydroxycholecalciferol
Organs
Skin
Liver
Kidney
Function to increase serum (in the blood) calcium
Target organs
Main affect: Intestines: increase Ca2+ intake (affects this the most)
bone: some mobilization (little effect)
kidney: reabsorption of the Ca2+ back into the blood (little effect)
Formation of calcitriol
In skin have cholesterol precursors for vit D3, the cholesterol gets concerted into vit D3 due to the presence of UV light
The vit D3 further changed into 25-hydroxycholecalciferol in the liver
PTH in the kidney activates the cholesterol into calcitriol or vit d3 hormone
Signalling process
Calcitriol diffuses through the membrane to binds to the vit D nuelcear receptor
Forms a heterodimer with another receptor, the retinoic acid receptor
Heterodimer goes into the nucleus to find the vit D response element
Stimulate new genes being formed to form more CA channels and binding proterins and transporters in the kidneys and intestines to help absorb or reabsorb calcium into the bloodstream
Three things that can be done to correct a calcium deficit
what is the main goal
What do you want the target organs to do
What hormones are involved and how are they involved
main goal: increase Ca2+ concentration in the blood
Bone: increase resorption
Increase PTH
Kidney: retain Ca2+ and prevent loss
Increase PTH which also increases calcitriol
Intestine: increase CA2+ absorption
calcitriol by the help of the increase of PTH
How is blood phosphate controlled?
recall what is phosphate in relation to calcium
Why is it important to controll phosphate during the controlling of calcium
What are the effects of the two hormones on phosphate control in certain target organs (2 target hormones for each)
Why are the effects slightly different for each hormone (when is the hormone activated in terms of time)
Blood hydroxyapatite crystals have both calcium and phosphate
When calcium breaks down, phosphate also gets broken down
Hormones
PTH: immediate need of breaking of bone and therefore a lot lot LOT of phosphate
increase phosphate release in the bone
Decrease phosphate reabsorption in the kidney (don’t need a lot being reabsorbed because they would results in too much phosphate in the blood)
Calcitriol: hormone is there for day to day life; therefore constantly need calcium
Increase phosphate absorption by intestine
Increase reabsorption by kidney
Summary of key points of the hormones
PTH mobilizes calcium from bone: osteoclasts via RANKL and OPG mechanism (indirectly through
Osteoblasts)
PTH enhances renal reabsorption of Ca2+ (and kicks out phosphate!)
Calcitriol - PTH enhances the production of Calcitriol
Both work at Bone/Kidney/Intestines to increase absorption!
Calcitonin
Where is it secreted from
What unique characteristics does it have in relation for secreting CA2+
What type of hormone is it
What triggers its release
Main function of calcitonin
When in parts of life is this most important?
How does it affect the target organs
secreted from C cells of the thyroid gland
C cells have Ca2+-sensing receptors
A peptide hormone
Release triggered by high plasma Ca2+ concentration
Function: decreases calcium levels to protect the skeleton from Ca2+ loss
Important in pregnancy and lactation
Target organs
reduces activity of oseoclasts in bone
Stimulate osteoblasts in depositing calcium
Inhibit the reabsorption of Ca2+ by kidneys
What happens in calcium homeostasis is not maintained?
Hypercalcemia (TOO MUCH):
GROANS (constipation)
MOANS (psychic moans = fatigue, lethargy, depression)
BONES (bone pain)
STONES (kidney stones)
Psychiatric OVERTONES (including depression and confusion) ++Weakness
Hypocalcemia (TOO LITTLE)
C= Convulsions
A = Arrhythmias
T = Tetany
S = Spasms, Seizures, & Stridor
> People can die from this
Summary slide for calcium balance
Cal+ homeostasis is affected by:
Dietary intake
Urinary output
Distribution in bone, cells, and ECF
Decreased Ca+ stimulates PTH
Promotes Cal resorption from bone, enhances renal Cal reabsorption, and increases Ca?+ through its effect on calcitriol