arterial blood gases and acid-base balance
1/58
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
59 Terms
normal range for pH
7.35-7.45
PaCO2 range
35-45
paCO2 what is associated with
respiratory/lungs
paO2 range
80-100 mmHg
what is HCO3 range
22-26
what is HCO3 associated with
metabolic/kidneys
what happens to BE as bicarb decreases
BE more negative
what happens to BE (base excess) as hco increases
BE becomes more positive
what is equation for PaCO2
see equation

what does hypoventilation do to co2
elevated CO2
what does hyperventilation do to CO2
decrease— drives rxn to the left

what are factors that affect PaO2
ventiliation (breath depth and rate)
lung capacity
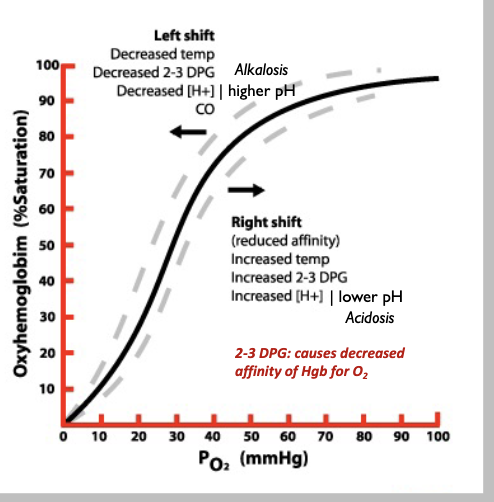
oxyhemoglobin dissociation curve (the higher on the curve, the more o2 there is to bind to Hbg)
what are key takeways from oxyhemoglobin dissociation curve
once o2 binds one heme, its easier to bind the next
normal half sat is at 26 mmHg
shifting to left means Hb has higher affinity (need a lower half sat to get 50% Hb bound to o2), right shift means half sat increase or Hb has lower affinity
can body handle acid or base better
acidosis a bit better
where is half sat lower (left shift) /higher Hbg affinity?
lung capillaries— hang on to that O2
area of high O2 content
where is O2 low/lower affinity of Hgb of O2
tissues, organs
what is FiO2
fractional percent of oxygen in air
what is PF ratio
ratio of PaO2 to FiO2
normal is 400 to 500, mild resp distress is 300
what is normal FiO2
21%
how is arterial bicarb calculated
using H-H equation- measured pH and PaCO2
should be close to serum bicarb on the BMP
what does elevated serum bicarb mean
alkalosisw
what does decreased serum bicarb mean
acidemia
what does raised anion gap mean
anion accumulation
too much acid in body— lactic acidosis, ketoacidosis
the acid is sequestered by bicarb but the anions acculmulate
what is venous oxygen saturation used to measure
oxygen delivery/uptake by tisues
can compare with arterial sat— if SaO2 and SvO2 are good then lungs AND heart ok
what is O2 sat ? what is normla value?
oxygen sat of hemoglobin
>95%
why are arterial samples pref over venous blood gas samples
venous only represents local tissue perfusion
venous tissue can’t show why gas levels abnormal
ABG show if lung, heart or tissue failing
PaO2 show how well lungs got oxygen in
PaCO2 show how well lungs removed CO2
arterial blood is same everywhere in the body
how is CO2 produced in the body
carb/fat metabolism— produces waaaay more
protein/tissue metabolism
what does high serum lactate show
anaerobic metabolism— there ia problem going on
what are buffers for acid-base homeostasis
bicarb.carbonic acid system
phosphates
proteins
resp regulation
rate/depth of breathing
renal regulation
bicarb filtration by glomerulus and reabsorption
excretion of nonvolatile acids
distal tubular hydrogen ion secretion
what is acidosis vs acidemia
acidosis is process LEADING TO acidemia (which is the state of having low blood pH)
what are two main cuases of acidemia
resp (hanging on to CO2)
metabolic (decreased serum HCO3)
what are two causes of alkalosis
resp (excessive loss of CO2)
metabolic (rention of bicarb)
what disorder is pCO2 under 35
resp alkalosis
what is quick acting buffer
bicarb/carbonic acid system
what oes pCO2 over 45 mean
resp acidosis
what does HCO3 under 22 mean
metabolic acidosis
what does hco3 over 26 mean
metabolic alkalosis
how is resp alkalosis compensated for (means too little CO2)
decreasing bicarb
how is resp acidosis (too much co2) compensated for
increasing bicarb
how is metabolic acidosis (too little bicarb) compensated for
decrease Co2
how is metabolic alkalosis (too much bicarb) compensated for
increase pCO2
what is dif between acute and chronic a/b disorder
acute means the body is in the process of compensation and pH is returnING to normal.
chronic means pH is normal but the compensation is ongoing
what is correction vs compensation
correction is where the dysfunctional organ can self-correct— ex with resp alkalosis, able ot increase pCO2.
compensation is when the other organ has to help restore pH, so in resp alkalosis hte kidneys have to decrease bicarb
how long for resp compensation of metabolic disorders to take affet
hours
how long metabolic compensation of resp problems to take affect
3-5 days
what is an example of chronic disorder
COPD
always have high pCO2, kidneys ALWAYS working
so pH is normal but not normal phys
what does AG over 20 mM/L mean regardless of pH or HCO3
priamary metabolic acidosis
what does MUDPILES stand for in regards to causes of anion gap
methanol (tox)
uremia (renal fail)
diabetic ketoacidosis
prop glycol/paraldehyde (tox)
Intoxication (alcohol)
Lactic acidosis
Ethl glycol (tox)
Salicylates (tox)
more bc acid is ADDED to the blood
what are causes of nonanion gap metabolic acidosis
Gi bicarb loss (d, pancreatic fluid drainage, ileostomy— intestines removed and bag to collect feces, its like diarrhea when high output)
renal bicarb loss (carb anhydrase inhibitors)
impaired adrenal acid excretion
Iatrogenic (HCl given in excess, poor TPN, excess NaCl)
post hypocapnia (hyperventiliating— lungs correct hyperventilation so more CO2, but means there is a time where kidneys not normalized yet so still acidic)
more because of LOSS of bicarb lost
what disorder does chloride responsive vs resistant represent
metabolic alkalosis
what is dif between Cl resistance vs responsive
responsive— chloride fixes kidney inability to excrete bicarb
the body reabsorbs Na with another anion besides Cl if defic— so means HCO3 will be reabsorbed
why is hypokalemia also associated with metabolic alkalosis
bc can’t retain Na, so use bicarb to pump back into stomach
what are chloride responsive metabolic alkalosis conditions
GI losses— vommitting, nasogastic sunction, Cl loss in diarrhea
diuertics
excess bicarb (TPN, PO, IV— iatrogenic)
post hypercapnia
chloride resistance conditions
mineralocortiod excess (hyperaldosteronism— hang onto Na no matter waht, cuhsing, exogenous mineralocort)
severe hypokalemia, hypomag (mag important to K transport)
bartters or gitelman’s syndrome
cauese of respi acidosis (not breathing fast— more CO2)
CNS— stroke
drugs—opiatives, sedatives
pulmonary— asthma/copd, pneumonia
neuromsuclar— brainstem injury, neuromuscular blocking drugs, myasthenia gravis
causes of resp alkalosis (hyperventilation— not enough CO2)
CNS— resp stim— anxiety/pain, fever, salicylate, stimulants
pulomary— embolus (not enough perfusion), asthma
preg— hypoxemia
why mineralcortiocoids cause metabolic alkalosis