Lecture 34: Chest Trauma and Pneumothorax II
1/42
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
43 Terms
Blunt Chest Trauma (BCT)
• Mechanism: force applied over relatively large area of chest wall
• Minor chest wall contusions to fatal intrathoracic injuries
• 25% of all trauma related deaths in U.S.
• Motor Vehicle Accident (MVA)
• Ejections from motorcycles
• Falls
• Violence & assaults
Most common mechanisms of BCT
Blunt Chest Trauma (BCT)
• Mild pain to severe dyspnea, hypotension, cardiac arrest
• Majority of injuries: chest wall contusions & rib fractures
-abrasions, swelling, seat belt marks, paradoxical motion
-distended neck veins, trachea position
1-7
True Ribs
8-12
false ribs
11-12
floating ribs
3-9
typical ribs
4-9
ribs that are most commonly fractured
1 and 2
Fracture of ribs ___________ suggest significant force
CT
-imaging that is more sensitive to rib fractures
-consider if significant trauma, multiple rib fx, intraabdominal or intrathoracic injury
Analgesics
treatment for a rib fracture with no pulmonary injury
Multiple rib fx
Elderly
Chronic lung disease
Severe co-morbidity
Intractable pain
Underlying lung, intrathoracic or intraabdominal injury
when would a rib fx cause you to be admitted?
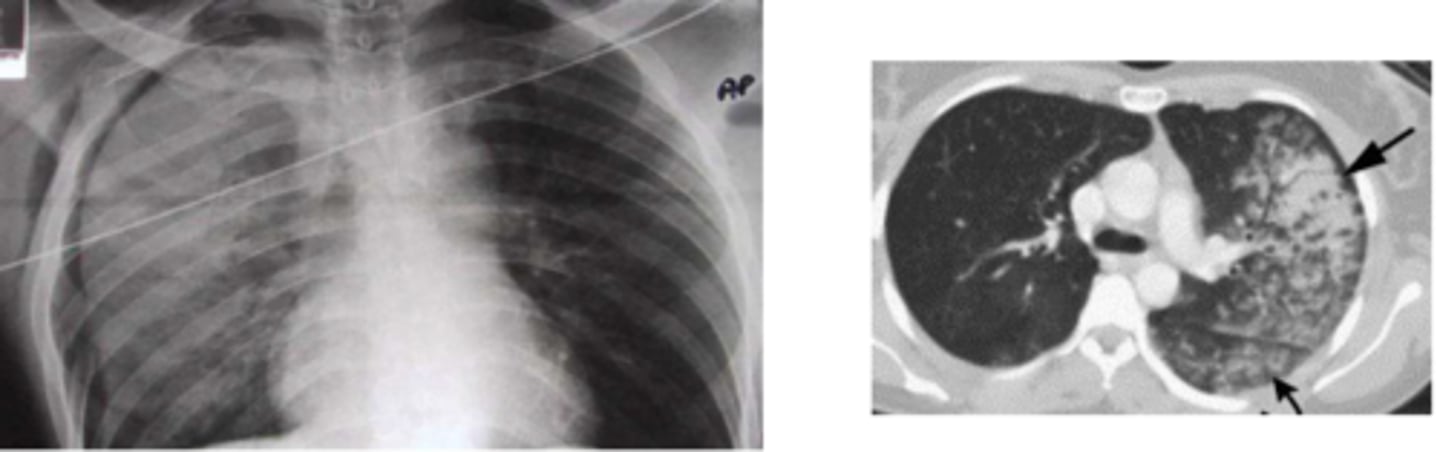
Pulmonary Contusion
• Most common injury to pulmonary parenchyma in BCT
Pulmonary Contusion
• Damage to alveolar-capillary membrane, /\ membrane permeability
• Collection of blood & edema in alveoli
• V/Q mismatch
• Hypoxia, hypercarbia, acidosis
Pulmonary Contusion
Clinical Features
• Dyspnea, tachypnea, pain common
• Tenderness, ecchymosis, deformity, crepitus of chest wall
• Crackles on auscultation***
• Large - tachycardia, cyanosis, hemoptysis
Pulmonary Contusion
• Opacification / consolidation under area of BCT
• CXR findings lag behind clinical findings (coming and going!)
• Often not present initially - progress over 6-12 hrs
Pulmonary Contusion
-Oxygenation
-Pain control
-Admission
-Avoid Excessive IV fluid
treatment of a pulmonary contusion
Flail Chest
-3 or more adjacent ribs, each fractured in 2 or more places
• Chest wall unstable & segment lacks continuity with rest of thoracic cage
Flail Chest
-Severe disruption of normal chest wall movement
-asymmetrical & uncoordinated
-Not seen with PPV, only spontaneously breathing
Flail Chest
• Respiratory compromise related to degree of underlying lung injury - severe pulmonary contusion common
• Pain & mechanics can lead to hypoventilation, atelectasis & hypoxia
• Severe pain, tenderness, crepitus, bruising
• Paradoxical motion (sometimes) absence does NOT exclude the diagnosis
Contrast-enhanced CT
what imaging is usually indicated for a flail chest?
• Oxygenation, ventilation, pain control
• Manual stabilization initially
-CT Scan
• Positive pressure ventilation
• Pain Control
• Surgery to stabilize the flail segment
treatment for flail chest
Motor Vehicle Accident
most common cause of sternum fracture
Injury to Intrathoracic/Mediastinal Structures
biggest concern in regards to a sternum fracture
Lateral
which xrays have a higher sensitivity for sternum fractures
• Pain control, ice
• Displaced fractures may require reduction
treatment of sternal fractures
6-12 hour observation & 6-12 hour EKG
observation recommendations for a sternum fracture
-Brachial plexus injury
-Vascular injury
-Pneumothorax
-Non-union
possible complications of a clavicle fracture
Clavicle Fractures
• Swelling, ecchymosis & tenderness over site. +/- Crepitus
• Skin tenting; open fx possible
• Loss of normal contour of shoulder/clavicle
• Extremity held close to body, supported by other hand
-Sling, Ice, Pain control
-Surgery (possibly)
treatment of a clavicular fracture
Costoclavicular ligament
most important stabilizer of the sternoclavicular joint
Superior Mediastinum
-immediately posterior to sternoclavicular joint
-contains great vessels, trachea, and esophagus
Sternoclavicular Joint
least commonly dislocated major joint in body
1st degree (Grade I) & 2nd degree (Grade II) joint injury
Type of SC Joint Injury:
• Sprain or subluxation of SC joint
• Stretching, incomplete tears of the SC & CC ligaments or rupture of one ligament
• Clinical findings –swelling & tenderness over SC joint
• Treatment - Ice, analgesic, sling & follow-up
3rd degree (Grade III) joint injury
Type of SC Joint Injury:
• Rupture of SC & CC ligaments with complete dislocation of clavicle from manubrium
• Significant forces required - MVC, contact sports (rugby & football) are most common
• 2 types possible – anterior and posterior
Anterior Dislocations
mot common 3rd degree (Grade III) SC Joint Injury
Sternoclavicular Joint Injury
• Extremity may be foreshortened; usually supported across the trunk by opposite arm
• Shoulder appears shortened & rolled forward
• SCJ swollen & tender to palpation
Anterior Dislocation
Medial clavicle prominent & palpable anterior to sternum
Posterior Dislocation
-pain more severe
• Clavicular notch of sternum may be palpable
• Possible associated complaints**
• Hoarseness, dysphagia, dyspnea, weakness/ paresthesias of UE
• Intrathoracic or mediastinal injuries in 30%
• Airway complications rare
Posterior
in a __________________ dislocation, the neck is often flexed toward the injured side
With traction maintained, push clavicle into place by inward pressure over medial
describe reduction of SC joint with an anterior disolcation
-Clavicle grasped near medial border (towel clip) & pulled anteriorly
-Local anesthesia should be utilized
describe reduction of SC joint with a posterior disolcation