Chapter 12 process of birth
1/102
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
103 Terms
contraction characteristics
the power that advances labor
coordinated
cyclical
fetus stores O2 → circulation cut off w/ contraction
wavelike pattern
contraction coordination
frequency
duration
intensity
contraction frequency
beginning of one uterine contraction to the beginning of the next
how often is it happening? - mins & fractions of mins
contraction duration
beginning of a contraction → end of same contraction
how long is it? - in sec
contraction intensity
strength!
contraction cycle
increment
peak/acme
decrement
contraction increment
period of increasing strength
slowly climbing
contraction acme/peak
when contraction is most intense
watch relationship w/ FHT
contraction decrement
period of decreasing intensity
as uterus relaxes
contraction interval
resting time!
btwn contractions
notes placental perfusion
end of one contraction → beginning of another
not long enough? not enough O2! - tachysystole
FHT deceleration
uterus
a muscle!
upper 2/3 contracts
squeeezeeee
pushes fetus down
lower 1/3 less active
w/ cervix
contractions not strong enough? complications !
uterus retraction ring
physiologic
division btwn upper & lower segments
uterus during labor
upper segment becomes thicker
lower segment + cervix get thinnger & get pulled upward
cervical changes in labor
happen concurrently, but at different rates
effacement
dilation
towards end of pregnancy & start of labor
cervix
about 2in non-effaced
cervical effacement
thinning & shortening of uterus
starts a lil earlier
cervical dilation
opening
nullipara during labor
have not completed a pregnancy to at least 20wks gestation
cervical effacement often happens early in process of cervical changes
efface THEN dilates
para during labor
has given birth after pregnancy of at least 20wks gestation
cervix usually thicker than nullipara at any point in labor
efface & dilate faster
been thru it before already
cardiovascular effects of labor
during contractions 300-500mL of blood backs into systemic circulation
causes short increase in blood vol
BP increase, HR decrease
only check vitals in btwn contractions! false high & low
notice vitals are odd? check contraction timing
respiratory effects of labor
depth & rate increases
too fast? may hyperventilate
help control breathing !!
GI effects of labor
motility slows
N&V
client kept on clear liquid diet
to decrease N/V
makes emergency surgery/c-section easily accessible
still gets glucose, but won’t have a lot of food in stomach
urinary effects of labor
reduced sensation of full bladder
none w/ an epidural
if not emptied regularly, can add to pain of labor & keep fetus from descending
hematopoietic effects of labor
500-1000mL blood loss normal
can usually be tolerated w/o difficulty bc of increase in blood vol during pregnancy
if client is anemic at time of delivery, may not be able to tolerate loss
may be symptomatic or need blood
placental circulation fetal effects during labor
circulation is vital to make it thru labor
during strong contractions blood supply to placenta decreases
spiral arteries compressed
exchange occurs btwn contractions
if working properly, enough O2 will be there to tolerate interruption
fetus can have issues tolerating labor w/ placental fxn issues
diabetes, HTN, preeclampsia → decels
pulmonary fetal effects during labor
lungs filled w/ fluid in utero
as fetus nears term → production of fluid decreases to abt 65%
labor speeds lung fluid absorption
35% remains in lungs at birth
catecholamines made by fetal adrenal glands in response to labor stress help infant adapt to land living
fluid squeezed out or squeezed into tissue → less to deal w/
cardiovascular fetal effects during labor
reacts quickly to labor events
alterations seen from labor effects/fetal intolerance
FHT normally 110-160 for term
may be higher in preterm babies bc of immature parasympathetic nervous system
factors affecting labor process
powers
passage
passenger
psyche
powers & labor process
quality, force & freqency of contraction
passage & labor process
true pelvis/birth canal
passenger & labor process
the fetus itself
psyche & & labor process
anxiety
culture
expectations
support
powers & labor
contractions
pushing efforts
contractions
body trying to get baby out
not strong/frequent enough? labor can stall
should have 1min intervals in btwn
ideally 3 min apart from start of one to next
weak contractions
labor can stall
ineffective pattern
may need help - pictocin
c-section if that still doesnt work
tachysystole
contractions too close tgt
oxygenation problems
not enough time for mom & fetus to recover
contraction strengths
mild
moderate
strong
passage
route through which the fetus has to travel to be born vaginally
true pelvis
must be of adequate shape & size so baby can pass thru
if large fetus noted, measurements of pelvic outlet & baby head measured via U/S
if noted during labor (w/ baby not coming down), emergency c-section indicated
failure to progress
when baby does not come down into pelvis during labor
pelvis & labor
the birth canal passage!
bony pelvis & soft tissue of birth canal
pelvic outlet & vaginal canal
pelvic outlet
circumference of opening inside of pelvis
small? cephalopelvic disproportion happens
not large enough to accomodate head → c-section !
bony pelvis
can be measured w/ pelvimetry, but not accurate
has been replaced by clinical labor trial
cephalopelvic disproportion
when the head will not fit through the pelvis
like trying to fit a square block in a round hole
soft tissue of birth canal
cervix
pelvic floor musculature
passenger
what presents to the pelvic outlet
fetus
membrane
placenta
fetal laboring aspects
head
attitude
lie
presentation
fetal head
usually presents in cephalic presentation
optimal presentation!
shoulders must be considered in width
fetal attitude
posturing of fetal parts to one another
flexion or extention
flexed most favorable for vaginal birth
fetal lie
relationship of the spine of fetus to the mother
R, L, anterior, posterior, transitional
anterior/longitudinal lie most optimal
fetal face facing mother’s spine
typically how baby is presented
transitional lie
baby positioned back first
fetal presentation
body part of fetus that enters pelvic inlet first
what part presents first!
cephalic, breech, shoulder, transition
cephalic presentation
head-first
best positioning!
Largest single fetal part
Can change shape, molding & adapting!
Smooth, round, hard -> helps dilate cervix
Further division
cephalic presentation divisions
Vertex (flexed, most favorable)
military (neutral)
brow (partly extended)
face (fully extended)
breech variations
Frank (legs extended)
complete (all flexed & butt first)
footling (feet first)
breech presentation
pelvis first
butt/feet
More common preterm, hydrocephaly, multiple gestations, uterine abnormalitites, placenta previa
Buttocks not smooth
Head last to be born -> head suject to compression
shoulder presentation
scapula first
Preterm, hydramnios, placenta previa, abnormal uterus
C-section needed
occiput posterior presentation
baby spine facing mother’s spine
face to belly
hardest position to get baby down into outlet
wider circumference
longer labor on back, longer time pushing
increased back pain
can be bc of pelvis tilt/odd shape
may lead to C-section
back-lying labor
not normally taken by epidural
pushing sessions
FTM? about 1hr
later becomes quicker
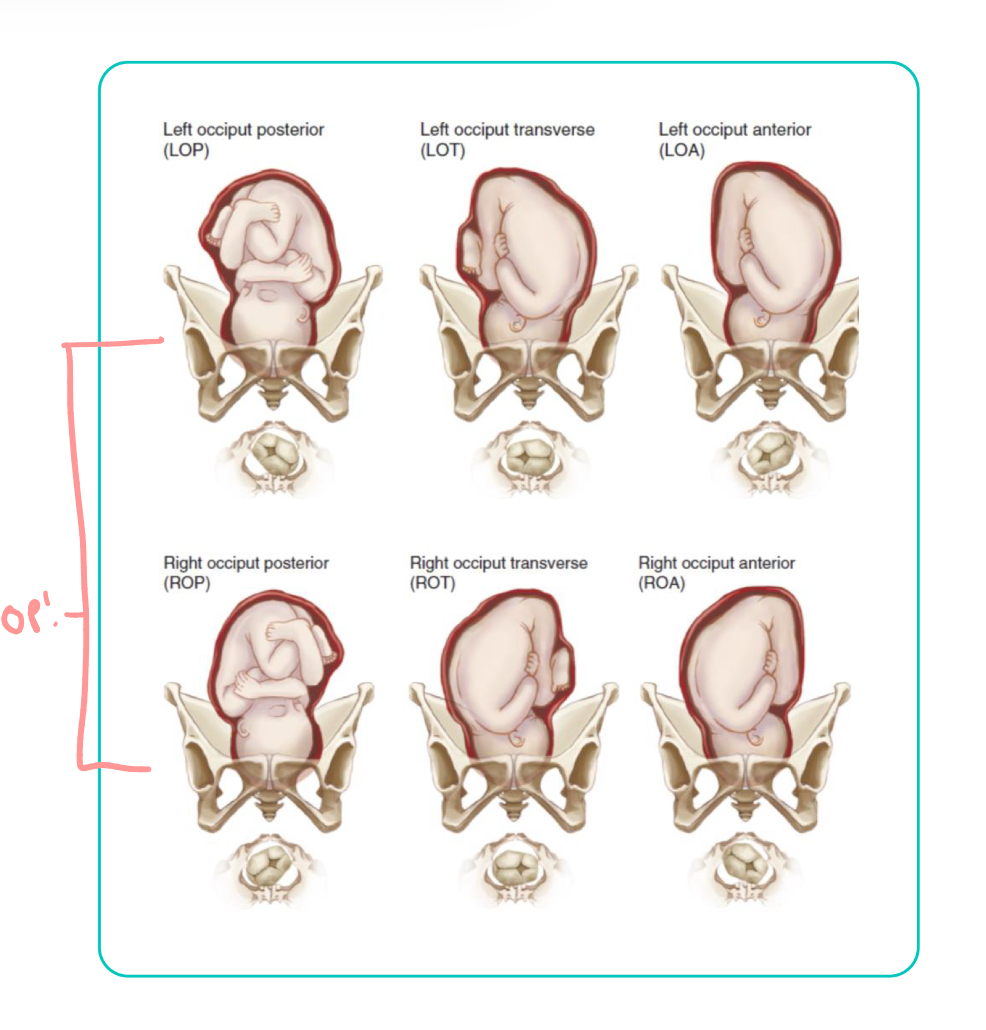
positioning indication abbreviation
3 letters!
1st: whether presenting part is toward L or R of maternal pelvis
2nd: presenting part of fetus
occiput (O), sacrum (S), mentum (M), acromion process (A), dorsal (D)
3rd: location of presenting part in relation to portions of maternal pelvis
anterior (A), posterior (P), transverse (T)
fetal position ex
all longitudinal lie w/ flexion attitude
psychological response of mother during labor
state of mind throughout birthing process is critical to positive outcomes
esp when mom is alone!
exhaused? can’t push efficiently - coaching needed
super anxious? cant relax? labor effected!
factors promoting a positive birth experience
clear info about procedures during labor
support - not being alone!
sense of master, self-confidence
trust in staff
positive rxn to pregnancy
personal control over breathing
prep for childbirth experience
false labor
has to be sent home
no tylenol in hospital, alternative means at home
can happen many times
false labor contractions
inconsistent in frequency, duration, & intensity
change in activity, like walking, does not alter contractions
may decrease them
can be triggered by dehydration
give water!
false labor discomfort
felt in abd & groin
in the front
may be more annoying than truly painful
false labor cervix
no significant change in effacement/dilation after an observation period of 1-2hrs
>39wks? may be admitted & given pictocin
true labor
only pain mgmt is epidural
true labor contractions
consistent pattern of increasing frequency, duration, & intensity usually develops
walking tends to increase frequency & strength
put on monitor first thing!
observe strength & frequency
look for FHT and distress
true labor discomfort
begins in lower back & gradually sweeps around to lower abd like a girdle
back pain may persist in some women
often feels like menstural cramps
true labor cervix
effacement and/or dilation of cervix happens
dilation itself not a sure tell
progressing is most important characteristic!
vaginal exams q1h
water is usually broken, but sometimes not
elective induction
pt has to be at least 39wks
decided by AWHONN
sooner, decided induction only bc of complications
early induction complications
preeclampsia
IUGR
poor placental perfusion
gestational diabetes
mild contraction palpation
slighty tense fundus
feels like touching finger to tip of nose
moderate contraction palpation
firm fundus
feels like touching finger to chin
strong contraction palpation
rigid, board like fundus
feels like touching finger to forehead
labor stages
first
second
third
fourth
labor stage 1
onset → 10 cm dilated
first stage labor work accomplishment
effacement & dilation of cervix
first & third stage labor forces
uterine contractions
first stage labor cervical dilation
latent phase
active phase
labor latent phase
first stage
~0-5cm
beginning of labor!
excited!
contractions okay
coming to hospital/admitting
labor active phase
first stage
~6-10cm
omfg this is killing me
water breaks
epidural initiated
increasing contractions
mad asfff
stuff is getting real
first stage labor uterine contractions
initially mild & infrequent
gradually progresses to strong intensity
3-5 contractions in 10min period
first stage labor discomfort
often begins w/ low backache & cramps like period cramps
back discomfort then sweeps to lower abd like a girdle
discomfort intensifies as labor progresses
first stage labor client behaviors
sociable, excited, somewhat anxious in early labor
becomes more inwardly focused as labor intensifies
may lose control during late active phase
often varies w/ pain-relief chosen!
labor stage 2
10cm → delivery
pushing time
second stage labor work accomplished
expulsion of fetus
second stage labor forces
uterine contractions
voluntary bearing-down efforts
second stage labor cervical dilation
10cm!
complete!
second stage labor uterine contractions
strong
5-6 contractions in 10min period
may be slightly less intense than during late first stage
may pause briefly as second stage begins
second stage labor discomfort
urge to push/bear down w/ contractions
becomes stronger as fetus descends
distention of vagina & vulva may cause stretching/splitting sensation
second stage labor client behaviors
intense concentration on pushing w/ contractions
often oblivious to surroundings & appears to doze btwn contractions
labor stage 3
delivery of baby → delivery of placenta
third stage labor work accomplished
separation of placenta
third & fourth stage labor uterine contractions
firmly contracted
third stage labor discomfort
little
sometimes slight cramp felt as placenta is passed
third stage labor client behaviors
excited & relieved after baby’s birth
usually very tired
often cries
labor stage 4
recovery!
1-4hrs
based on whats happening to mom
fourth stage labor work accomplished
physical recovery
bonding w/ newborn