Week 11 CNS/Brain injuries/Conditions
1/122
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
123 Terms
Head injury involves
trauma to scalp, skull, and brain
Result of head injury is
mild concussion to coma to death
Traumatic brain injury (TBI)
can be open, closed, diffuse, focal
most common cause: falls
Clinical manifestations of head injury depend on
location and severity of injury
symptoms of hemorrhage are delayed until hematoma is large enough to increase intracranial pressure
can involve personality and physical function
Epidural hemorrhage refers to bleeding that are
above dura, under skull
medical emergency
rupture of middle meningeal artery
Epidural hemorrhage results in
herniation
loss of consciousness
focal neuro deficits
pupil dilation, paralysis of extremity
Subdural hemorrhage refers to bleeding that are
below dura, between dura and brain
usually venous
may be acute, subacute, chronic
Intracerebral hemorrhage refers to bleeding that are
within the brain tissue
Intracerebral hemorrhage are the result of
focused injury or system issues (hypertension→ CVA)
Concussion is
global, microscopic
widespread, homogenous impairment of brain cells
cell under-perform
no visible bleeding
confusion, irritability, disorientation, headache
Contusion is
localized, macroscopic
structural damage to cells
cells die
effects peak 18-36 hours after injury
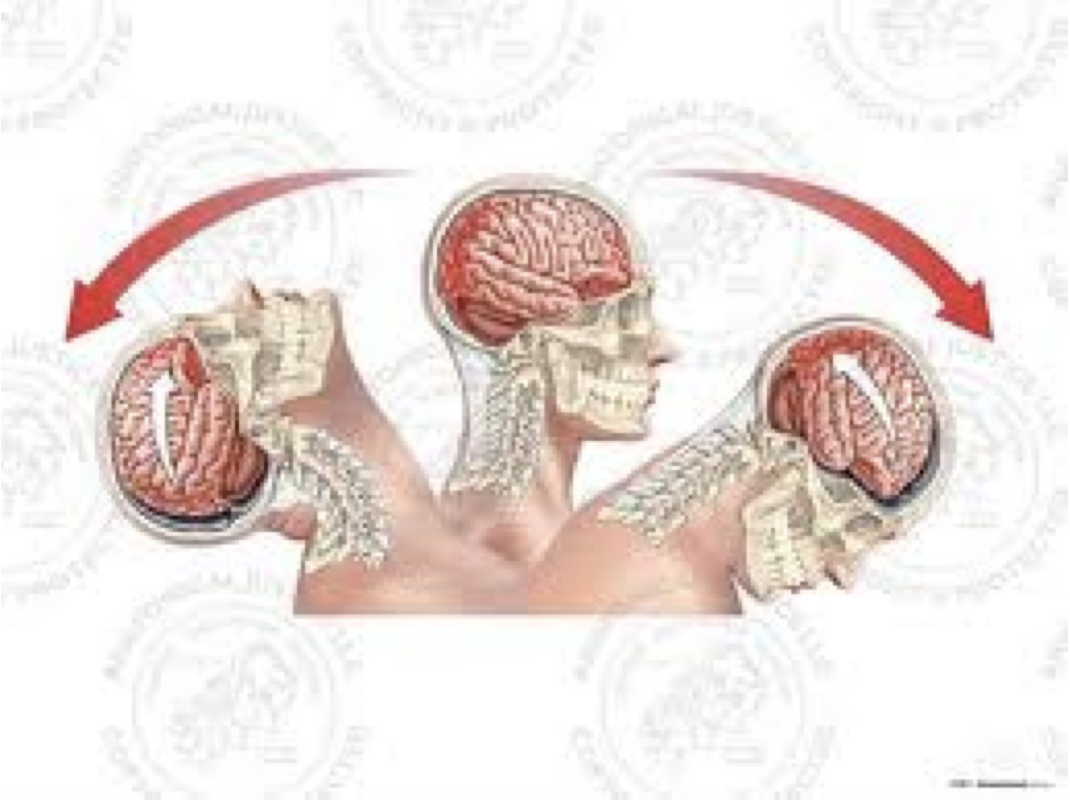
“Coup-conTrecoup”
can cause increase ICP d/t bleeding
blurred vision, disorientation, unsteady gait, vomiting, slurred speech, coma
Intracranial bolt (ICB) is
a device inserted into the skull to directly monitor intracranial pressure
identify increases in pressure quickly so treatment can be started before severe complications occur
Vomiting is associated with
increased ICP in head injuries
Coup-contrecoup
severe traumatic brain injury involving contusions at both sides
Diagnostics for head injuries
CT or MRI
identifies / evaluates injury to brain tissue
skull x rays
penetrating injuries to the skull
angiography
Medical care for head injuries
control ICP
reduce cellular demands with medically induced coma
surgical interventions
minimize secondary injury
How do you control ICP?
Intracranial Bolt (ICB)
mechanical ventilation
prevent hypoxemia bc
increased lactic acidosis→ increased vasodilation and increased ICP
cerebral vessels dilate→ increased ICP
How hypoxemia and hypercapnia affect ICP?
low O2 and high CO2 cause cerebral vessel dilation and widening of vessels mean more blood in brain’s limited space→ increases ICP
Goals of nursing care for head injury
address acute issues
prevent / treat secondary complications
prevent / treat / minimize consequences
Nursing care of head injury involves 2 steps
assess all systems for direct impact (primary compromise)
assess all systems for secondary impact (secondary compromise)
Primary compromise involves checking for
patient airway
optimal breathing pattern
optimal cerebral tissue perfusion
appropriate fluid balance
Secondary compromise involves checking for
S/S of infection
complications and consequences
Post-concussion syndrome lasts
1 week→ 1 year
Post concussion syndrome S/S
headache
dizziness
lethargy
emotional lability
fatigue
poor concentration
decreased attention span
memory difficulties
intellectual dysfunction
Monitor and notify MD if patient is showing
difficulty awakening or speaking
confusion
severe headache
vomiting
unilateral weakness
What does Intracranial surgery do?
reduce elevated ICP
remove tumor / foreign body
evacuate a blood clot
control hemorrhage
Craniectomy
removal of part of skull to allow room for swelling
Cranioplasty
repair of skull using metal / plastic plate after craniectomy
Pre op medical care for head injury
define diagnosis / surgical approach
general pre and post op considerations
medications
Pre op nursing care for head injury
document baseline neuro status
routine pre op care and education
continue with established care (diet, activity, meds)
Post op medical care for head injury
reduction of cerebral edema
relieving pain
preventing seizure
monitoring intracranial pressure
Post op nursing care
assess every hour (glasgow coma scale, respiratory, ABGs, VS, ICP)
proper positioning, depends on surgical approach
routine post op care (In and Out, bleeding? drainage?
check with MD for deep breathing and coughing
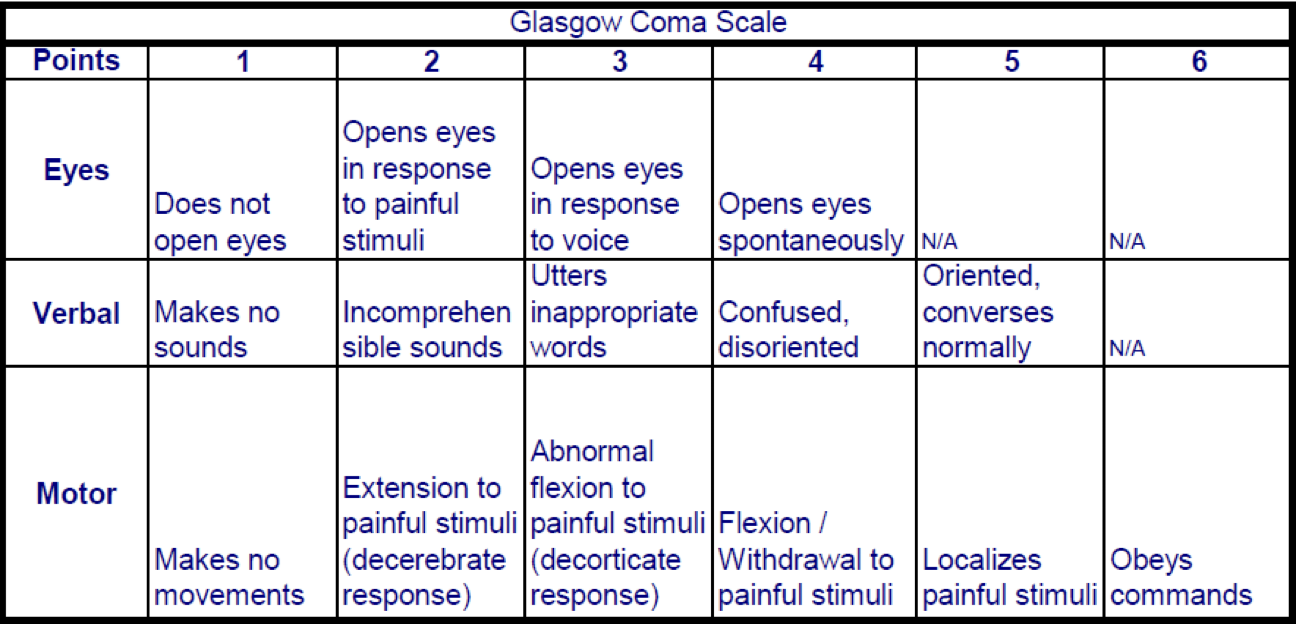
Glasgow Coma Scale (GCS)
most widely used method for evaluation of coma
Shortcomings for Glasgow Coma Scale
limited utility in intubated patients
inability to assess brainstem reflexes
Full Outline of UnResponsiveness (FOUR)
provides further neurological details
better predictor of outcome
useful for intubated patients
Glasgow Coma Scale
FOUR Score
| Points | 4 | 3 | 2 | 1 | 0 | Total Score |
System |
|
|
|
|
| ||
Eyes |
| 4 = Eyelids open or opened, tracking or blinking to command | 3 = Eyelids open but not to tracking | 2 = Eyelids closed but opens to loud voice | 1 = Eyelids closed but opens to pain | 0 = Eyelids remain closed with pain stimuli | |
Motor Response |
| 4 = Thumbs up, fist, or peace sign | 3 = Localizing to pain | 2 = Flexion response to pain | 1 = Extension response | 0 = No response to pain or generalized Myoclonus status | |
Brainstem Response |
| 4 = Pupil and corneal reflexes present | 3 = One pupil wide and fixed | 2 = Pupil or corneal reflexes absent | 1 = Pupil and corneal reflexes absent | 0 = Absent pupil, corneal, or cough reflex | |
Respiration |
| 4 = Regular breathing pattern | 3 = Cheyne-Stokes breathing pattern | 2 = Irregular breathing | 1 = Triggers ventilator or breathes above ventilator rate | 0 = Apnea or breathes at ventilator rate. | |
| |||||||
System Score |
|
|
|
|
|
|
|
Potential post op complications
bleeding and hypovolemic shock
fluid and electrolyte disturbances
infection
increased ICP
seizures
diabetes insipidus
SIADH
What is intracranial pressure?
balance of brain tissue, blood, cerebrospinal fluid
Normal ICP is
7-15 mmHg
increases in ICP can be due to
injury
brain tumors
subarachnoid hemorrhage
toxic or viral encephalopathies
Monroe Kellie Doctrine
increase in any component→ compensatory changes in other or ICP will increase

Early responses to increased ICP
change in LOC
pupillary changes
impaired ocular movements
weakness in one extremity / side
headache - constant
increase in intensity
aggravated by movement / straining
Late response to increased ICP
further deterioration of LOC
respiratory pattern alterations
loss of brainstem reflexes
pupillary, gag / swallowing, corneal
Cushing’s Triad
Hemiplegia or flaccidity
decorticate or decerebrate posturing
Cushing’s Triad is
hypertension / widening pulse pressure
bradycardia
bradypnea
Increased ICP acronym
Increasing pulse pressure
Changes: LOC, respiratory, speech, heart rate
Pupils, Puking, Pain, Posturing
Decorticate posturing indicates severe damage to
the brain at corticospinal tract
serious, but more favorable than decerebate posture
may progress to decerebrate posture, or the two may alternate
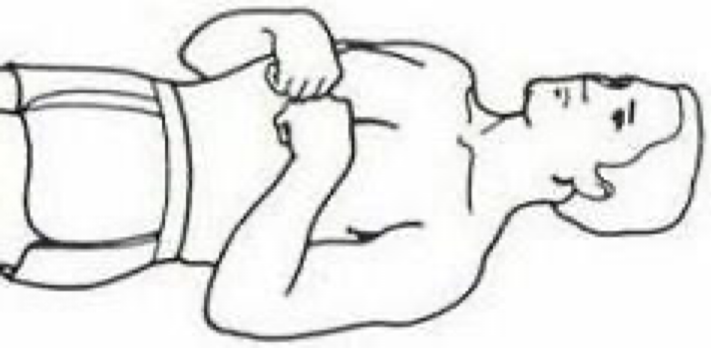
Decorticate posturing looks like
arms adducted and flexed
hands clenched
may be uni or bilateral
Decerebrate posturing indicates severe damage to
the brain at brainstem level
worse than decorticate
Decerebrate posturing looks like
arms adducted, extended and pronated
wrists flexed
head and neck arched backwards
muscles are tightened, held rigid
Risks for compromise d/t increased intracranial pressure
cerebral perfusion
airway clearance
fluid balance / imbalance
bowel / bladder function
infection
Nursing interventions for ↑ICP r/t Cerebral Perfusion
elevate HOB to 30-45 degrees with head in neutral position & use a cervical collar if necessary
avoid extreme hip flexion
note abnormal distension
avoid Valsalva maneuver
no closed mouth coughing
ask patient to exhale when being moved or turned
avoid enemas, suppositories
avoid isometric exercises
pre-oxygenate and hyperventilate prior to suctioning
avoid high levels of PEEP
space nursing interventions
assess level of cognition, orientation, and ability to follow commands
avoid emotional distress and frequent arousal from sleep
What is the Valsalva maneuver?
a breathing technique performed by attempting to forcefully exhale against a closed airway—typically by pinching the nose and closing the mouth while straining (bearing down) for 10–15 seconds
Why do we discourage patients from Valsalva maneuver?
to prevent straining
ask patient to exhale when moving / turning and avoid closed-mouth coughing and enemas
Nursing interventions for ↑ICP r/t Airway
elevate HOB
auscultate lung fields
O2 as needed
monitor pulse ox
suction as needed
hyperoxygenation for suctioning
note nasal drainage
Why should you never suction the nares?
it can lead to brain trauma or infection
Nursing interventions for ↑ICP r/t fluid balance / imbalance
monitor vital signs, I & O, skin turgor, mucous membranes, serum and urine osmolality
monitor intraventricular fluid
observe for congestive heart failure and pulmonary edema if giving Mannitol
good oral hygiene
non-drying mouth rinse
lip lubrication
Nursing interventions for ↑ICP r/t bowel / bladder function
monitor urinary output every 2-4 hours
test urine for specific gravity and glucose
monitor bowel sounds
monitor for abdominal distension
test stools for occult blood
Nursing interventions for ↑ICP r/t infection
aseptic technique when managing the intra-ventricular catheter / direct ICP monitoring
observe character of the CSF drainage
report increasing cloudiness or blood
monitor for signs / symptoms of meningitis
fever, chills, nuchal rigidity, increasing / persistent headache
monitor temperature, labs, urine, lungs
Nursing interventions for ↑ICP r/t hyperventilation
PaCO2 range: 25-30 mm Hg
Nursing interventions for ↑ICP r/t temperature control
Prevent hyper- or hypothermia
Nursing interventions for ↑ICP r/t B/P control
High range normal essential for adequate perfusion pressure
Too high may increase ICP
Sedation
Recommended positioning for a patient with increased ICP?
elevate HOB to 30-45 degrees with head in a neutral, midline position
Why should extreme hip flexion avoided in patients with increased intracranial pressure?
it increases intra-abdominal and intrathoracic pressure, which can impede venous return from the brain and raise ICP
How should a nurse prevent the Valsalva maneuver during patient movement?
instruct the pt to exhale while being moved or turned and avoid closed-mouth coughing
What are the respiratory nursing considerations before suctioning a patient with increased ICP?
pre-oxygenate and hyperventilate the pt
What is the target PaCO2 range for therapeutic hyperventilation in ICP management?
25-30 mmHg
When administering Mannitol, what two major complications must the nurse observe for?
Congestive Heart Failure (CHF) and pulmonary edema
What are the classic signs of meningitis to monitor for in a patient with an ICP drain?
fever, chills, nuchal rigidity (stiff neck), and increasing/ persistent headache
Why should nursing itnerventions be “spaced out” for patients with increased ICP?
to prevent cumulative increases in ICP and allow the pressure to return to baseline between tasks
What should the nurse test for if the patient has a risk of compromised bowel / bladder function?
urine specific gravity / glucose, abdominal distension, bowel sounds, and occult blood in stool
Management of increased ICP include
control intracranial pressure
medications
Mannitol
Corticosteroids
Dilantin
Antibiotics
Anti-anxiety
Mannitol is an
osmotic diuretic
Corticosteroids
reduce cerebral edema
Dilantin manages
Prophylaxis seizure activity
Complications to monitor for d/t increased ICP
brains tem herniation
respiratory distress or failure
pneumonia
aspiration
pressure ulcer
deep vein thrombosis (DVT)
contractures / position
seizures
diabetes insipidus
syndrome of inappropriate anti-diuretic hormone (SIADH)
Pathology of seizures
uncontrolled, abnormal, recurring electrical discharges in brain
Causes for seizures
idiopathic
acquired
cerebrovascular disease, hypoxemia, fever, head injury / surgery, hypertension, CNS infection, metabolic and toxic conditions (renal failure, hypoglycemia), brain tumor, drug / ETOH withdrawal, allergies
Classifications of seizures
Generalized seizures: involve the whole brain
Partial (focal) seizures: begin in one part of the brain
Simple partial: consciousness remains intact
Complex partial: impairment but no loss of consciousness
Manifestations of seizures
Loss of consciousness
Excessive movement
Not all seizures cause convulsions
Loss of muscle tone
Disturbances of behavior, mood, sensation, perception
Static Epilepticus
emergency where a seizure lasts longer than 5 minutes without waking in between
Seizure assessments
Precipitating factors
Presence of an aura
Initial presentation
Type of movements
Areas of body involved
Eyes
Size of pupils
Eyes open or closed
Any deviations
Incontinence
Duration
Periods of unconsciousness
Paralysis or weakness after the seizure
Inability to speak
Movements at the end of the seizure
Post-ictal period
Cognitive status after the seizure
Nursing actions when a pt is having a seizure
Maintain and protect airway
Suction set-up available
Turn sideways
Intubation to protect airway?
Limit seizure duration
Medications
Valium (diazepam), Ativan (lorazepam), Dilantin (phenytoin)
Prevent patient/personal injury
Observe seizure activity
Neuro/cardio/pulmonary monitoring
Documentation
Nursing actions post seizure
Reorient patient when awake
Provide comfort and reassurance
Treat any injury from seizure activity
Maintain seizure precautions
Anti-seizure medication if ordered
Education
Medication
Triggers
At-home/school care
Nursing actions for a pt with history of Status ePILEPTICUS
Limit seizure duration
Medications
IV Valium (diazepam)
Ativan (lorazepam)
Dilantin (phenytoin)
Establish and protect airway
Turn sideways
Intubation may be necessary
Neuro/cardio/pulmonary monitoring
Maintain safety
Documentation
Diabetes Insipidus is
deficiency anti-diuretic hormone (ADH) secretion
fluid Drains out
result of Diabetes Insipidus
polydipsia and polyuria
low urine specific gravity
dehydration
Causes of Diabetes Insipidus
increased intracranial pressure
surgical ablation or irradiation of pituitary
infections of CNS
Syndrome of Inappropriate ADH is
excess anti-diuretic hormone (ADH) secretion
fluid Stays in
result of SIADH
fluid retention, no edema = dilutional hyponatremia
causes of SIADH
increased ICP
bronchogenic carcinoma
paraneoplastic syndrome
severe pneumonia
hemothorax
Paraneoplastic syndrome
ADH is secreted by the tumor cells
how to treat DI
replace fluid
hourly IV fluid volume dependent on urine output
replace ADH
vasopressin
Complications d/t DI
dehydration
electrolyte imbalance
unintentional weight loss
how to treat SIADH
restrict fluid intake
1200-1800mL/day to increase serum sodium
replace sodium
hypertonic saline
complications d/t SIADH
water overload
electrolyte imbalances
fluid shifts
if Na+ > 140 mEq
dehdyration
if Na+ <135
confusion
Spinal cord injuries risk factors
youth, male, drug / alcohol use