Neurological Alterations
1/121
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
122 Terms
What are the 2 causes of stroke?
Ischemia → inadequate blood flow to part of the brain
Hemorrhage → bleeding into the brain
Result = death of brain cells
Other terms for stroke
Brain attack (emphasizes urgency)
CVA
Impact of strokes
Loss or impairment of functions controlled by affected brain area
Movement, sensation, thinking, talking, emotions
Common disabilities from strokes:
One-sided weakness
Inability to walk
Dependence for their ADLs
Aphasia (can’t communicate)
Depression
Leading cause of serious long-term disability =
Strokes
BE FAST (stroke S&S)
B – Balance; sudden loss of balance or coordination, headache, dizziness
E – Eyes; sudden vision changes or loss of vision in one or both eyes
F – Facial drooping (uneven smile/face?)
A – Arm weakness (one arm drifts down; pronator drift?)
S – Speech difficulties (slurred, unable to repeat sentence)
T – Time to call 911 (note time symptoms started!)
BE FAST (stroke S&S)
Balance; sudden loss of balance or coordination, headache, dizziness
Eyes; sudden vision changes or loss of vision in one or both eyes
Facial drooping (uneven smile/face?)
Arm weakness (one arm drifts down; pronator drift?)
Speech difficulties (slurred, unable to repeat sentence)
Time to call 911 (note time symptoms started!)
Brain’s blood supply =
Brain is very metabolically active, requiring 750-1000 mL/min (20% of CO)
No capacity of O2 or glucose
Supplied by internal cartoid arteries (anterior) and vertebral arteries (posterior)
Connected by circle of Willis
Critical timeline for strokes/TIAs
30 seconds = neuroloigc metabolism altered
2 minutes = metabolism stops
5 minutes = cell death occurs
How does the brain protect itself?
Autoregulation:
Maintains constant blood flow despite BP changes (50-150 mm Hg)
Adjusts vessel diameter
May be be impaired after stroke (protective mechanism can be comprimised by stroke/TIA)
Brain is then dependent on systemic blood pressure
CO2 levels strongly affect cerebral blood flow
After stroke, there may be angiogenesis/collateral cirucatlion over time to increase perfusion
Why do we not lower the BP too rapidly or too much after a patient has had an acute stroke?
Brain’s ability to autoregulate (protective mechanism which adjusts vessel diameter) is damaged
Brain is now dependent on systemic BP for adequate perfusion; brain may need higher pressures to maintain function w/o autoregulation
How does CO2 affect cerebral blood flow?
CO2 is a potent vasodilator; we monitor respiratory status of stroke patients since we don’t want these patients to hyperventilate; if they have low CO2, they start having vasoconstriction which can reduce blood flow to brain
What is autoregulation?
Protective mechanism that maintains constant blood flow to brain despite BP changes (50-150 mm Hg, as in cardiac arrest)
Adjusts vessel diameter
May be be impaired after stroke (protective mechanism can be comprimised by stroke/TIA)
Brain is then dependent on systemic blood pressure
Why can hyperventilation be dangerous for stroke patient?
CO2 is a potent vasodilator; if CO2 levels, there will be vasoconstriction, which lowers perfusion to the brain.
Significance of angiogenesis/collateral circulation in stroke patients
Some stroke patients (e.g. ones that have vessel stenosis) will have more collateral circulation/agiogenesis that occurs over time that improve lateral blood flow, so when they have a full-blown stroke, they don’t have as many symptoms as somebody who suddenly gets a stroke from an embolislm.
Nonmodifiable risk factors for strokes
Age (risks double each decade after 55)
Gender (more common in men, but women die more often)
Race/ethnicity (Blacks 2x higher risk)
Family hx/genetics
Major modifiable risk factors for strokes (modifiable risk factors cause 90% of strokes)
HTN (single most important risk factor)
Heart disease (especially Afib → 25% of strokes)
Afib patients need to be on anticoagulation therapy
Obesity (metabolic syndrome)
Physical inactivity
Poor diet
Diabetes (5x higher risk)
Alcohol/drug use
Smoking (2x ischemic stroke risk, and 4x hemorrhagic stroke risk)
risk normalizes after 5-10 years if they quit; still important for patient who smoked for 30 years as they can normalize it.
What is the sing;e most important modifiable risk factor for strokes?
HTN
HHOPPDAS Major modifiable risk factors for strokes
H – HTN
H – Heart disease (Afib = 25% of strokes
O – Obesity
P – Poor diet
P – Physical inactivity
D – Diabetes
A – Alcohol/drug use
S – Smoking (2x ischemic, 4x hemorrahgic)
Transient neurologic dysfunction from focal brain/spinal cord/retinal ischemia
Has NO acute infarction (no permanent brain damage)
Symptoms typically last <t hour
Medical emergency → treat immediately
TIA
Outcomes for TIAs
1/3 have no further events
1/3 have more TIAs
1/3 progress to stroke
ABCD² Score (0-7 points)
Predicts r/o stroke after TIA
A – Age ≥ 60 years (1 point)
B – BP ≥ 140/90 (1 point)
C – Clinical features (1-2 points)
D – Duration ≥ 60 min (2 points) or 10-59 min (1 point)
D – Diabetes (1 point)
Why is TIA a medical emergency and needs immediate treatment?
TIAs are a major indication of cerebrovascular disease; these patients have a high risk of having a stroke later
Furthermore; there is no way for patient to differentiate between a stroke and TIA for sure unless they are evaluated
TREAT IT LIKE A STROKE
Common symptoms of TIAs (similar to strokes)
Amaurosis Fugax/vision loss in one eye (temporary and painless loss of vision in one or both eyes due to disruption of the blood flow to the retina; feel like current dropping over your vision)
Unilateral weakness or numbness
Sudden speech difficulty
Dizziness/loss of balance
Significance of ABCD²
0-3 = 1% 2-day stroke risk
4-5 = 4.1% risk
6-7 = 8.1% risk
Higher scores may need hospitalization and aggressive management to identify and address any underlying causes
Imporant education regarding TIAs for patients
Treat it like a stroke (subsequent episodes need to be treated as a stroke since they have same symptoms even if they had a TIA before)
TIA = risk for stroke
Aggressive monitoring/care is necessary
“Clogged pipe.” Stroke (87%) that results from inadequate blood flow from a partial or complete arterial occlusion. has two types:
Thrombotic (most common ~60%)
Embolic
Ischemic stroke
“Bursted pipe.” Stroke (13%) that results from bleeding into brain tissue. Has two types:
Intracerebral hemorrhage
Subarachnoid hemorrhage (SAH)
Hemorrhagic stroke
TIA vs stroke
TIA = ichemia w/o infarction
Stroke = infarction (cell death)
Stroke diagnosis
#1 imaging is CT and is fast/convenient (can quickly rule out hemorrhage)
If not hemorrhage on CT but has significant stroke sx, it’s probably ischemic stroke → give tPA
MRI is better, but is slower than CT
Blood clot forms in brain artery
Clot develops at site of atherosclerotic plaque
Most common stroke type (~60%)
More common in older adults
These are characteristics of what condition?
Thrombotic strokes
Risk factors for ischemic strokes (thrombotic)
HTN
DM
High colesterol
Atherosclerosis
Clinical presentation of thrombotic strokes
Often occurs during or after sleep
TIA may precede (30-50% of cases)
Stepwise progression of symptoms
Usually conscious in first 24 hrs
Symptoms may progress over 72 hrs as edema increases
Symptoms are not very severe, but worsen with time (or they can wake up fucked).
Often occurs during or after sleep (may be due to decreased BP during sleep)
TIA may precede this (30-50% of cases)
Stepwise progression of symptoms (sx worsen in stages)
Usually conscious in first 24 hrs
Symptoms may progress over 72 hrs as edema/swelling increases
Symptoms are not very severe, but worsen with time (or they can wake up fucked).
These are clinical manifestations of what condition?
Thrombotic strokes
Strokes that often have TIAs preceding them
Thrombotic strokes
Traveling clot lodges in cerebral artery
Second most common cause of ischemic strokes
Has sudden onset with severe sx (acute)
These are characteristics of what condition?
Embolic strokes
Common sources of embolic strokes
Heart conditions: Afib (most common), MI, endocarditis, valve problems
Atherosclerotic plaque breaking off; any clot that breaks off e.g. DVT
Less common: air embolism, fat from long bone fractures
Clinical presentation of embolic strokes
Usually occurs during activity
Sudden, severe neurologic deficits (no warning signs!)
Often no warning signs
Patinet usually conscious, may have HA
Symptoms may be temporary if clots breaks up
High recurrence rate w/o tx
Usually occurs during activity
Sudden, severe neurologic deficits (no warning signs!)
Often no warning signs
Patinet usually conscious, may have HA
Symptoms may be temporary if clots breaks up
High recurrence rate w/o tx
These are clinical manifestations of what condition?
Embolic strokes
Why is cardiac workup essential for all stroke patients?
Flag HTN and atherosclerosis
Flag heart conditions that increase risk for embolic strokes e.g. Afib
Bleeding within brain tissue (usually basal ganglia); increased ICP
Most lethal type of stroke
30-day mortality: 40-80%
Half of deaths occur in first 48 hrs
Most common cause = HTN
These are characteristics of what condition?
ICH
Most common cause of ICH
Chronic uncontrolled HTN
Over time, HTN damages small blood vessels over time, making them more prone to ruptue → bad things happen
Causes of ICH
HTN
Vascular malformations
Anticoagulant/thrombolytic drugs
Coagulation disorders
Trauma, tumors, ruptured aneurysms
Occurs during activity (BP spikes)
Sudden onset with rapid progression (minutes to hrs)
Severe HA, nausea, vomiting
Decreased LOC
HTN
These are clinical manifestations of what condition?
ICH
Patient with head trauma and is on anticoagulant therapy →
Must be screened for ICH; these patients are at higher risk, especially elderly patients
Clinical presentation of ICH
Occurs during activity (BP spikes)
Sudden onset with rapid progression (minutes to hrs)
Severe HA, nausea, vomiting
Decreased LOC (may be unconscious due to ICP)
Deficits are dependent on location/size
HTN
LOC comparison between ischemic stroke or hemorrhagic stroke
Ischemic strokes may have patients who remain conscious.
Hemorrhagic stroke patients often come in unconscious
Cerebellar hemorrrhages (ICH) symptoms =
More severe HA, vomiting, inability to walk, eye movement.
Putaminal hemorrhage (ICH) symptoms =
More common
Unilateral weakness, slurred speech, eye deviation
Thalamic bleeds (ICH) symptoms
Sensory loss
Motor loss
Pontine hemorrhgaes (ICH) symptoms
Most serious since this affects basic life functions
These patients may go into a coma
Complete paralysis and abnormal VS
Treatment for hemorrhagic strokes
Controlling BP
Managing ICP
Cerebrovascular and cardiac function monitoring and maintenance
Surgery to evacuate hematomas
NO BLOOD THINNERS
Bleeding into CSF-filled space between arachnoid and pia mater
Often caused by ruptured cerebal aneurysm
These are characteristics of what condition?
SAH
Aneurysm types (SAH)
Saccular (berry) aneurysms → 2-30 mm
Fusiform atherosclerotic aneurysms
Most located in circle of Willis
Stroke often caused by ruptured cerebral aneurysm
SAH
Clinical presentation of SAH
“Worst HA of my life,” thunder clap HA
Sudden onset during activity (NO WARNING SIGNS until vessel explodes)
NV, seizures
Stiff neck
Loss of consciousness (may or may not occur)
Focal neurologic deficits (blood mixes with CSF, causing irritation and increased ICP)
Neurosurgical emergency
“Worst HA of my life,” thunder clap HA
Sudden onset during activity (NO WARNING SIGNS until vessel explodes)
NV, seizures
Stiff neck
Loss of consciousness (may or may not occur)
Focal neurologic deficits
Neurosurgical emergency
These are clinical manifestations of what condition?
SAH
Risk factors for SAH
HTN
Smoking
Cocaine/stimulants
Family hx
If 2 or more first-degree relatives → need screening
Anything that increases BP (e.g. activity or stimulant drugs) =
Increased r/o hemorrhagic strokes
Major complications of SAH
Rebleeding before tx
Cerebral vasospasm (peaks 6-10 days post-bleed)
What is the significance of cerebral vasospasms in SAH?
Causes an ischemic stroke on top of the hemorrhage
Body’s compensatory mechanism to protect brain, by constricting blood vessels to slow bleeding; this backfires
Risk peaks at 6-10 days after initial bleed; SAH patients need ICU monitoring for up to 2 weeks (risk for vasospasm after origianl injury)
Tx of SAH caused by aneurysm
Surgery (clipping/coiling)
Manage vasospasms with meds → maintain adequate BP and fluid volume
Watch for rebleeding
Right brain damage (stroke) =
Left-sided deficits
Left-sided hemiplegia/hemiparesis
Spatial-perceptual deficits (trouble judging distances, navigating spaces)
Quick, impulsive bahvior
Poor judgment
Neglect of left side
HIGH FALL RISK
Left brain damage (stroke) =
Right-sided deficits
Right-sided hemiplegia/hemiparesis
Aphasia (speech/language problems)
Slow, cautious behavior
Awareness of deficits → anxiety, depression
Stroke on right side of brain =
Paralyzed left side: hemiplegia
Left-sided neglect
Spatial-perceptual deficits
Tends to deny or minimize problems
Rapid performance, short attention spain
Impulsive → safety problems
Imparied judgment
Impaired time concepts
Stroke on left side of brain =
Paralyzed right side: hemiplegia
Imparied speech/language aphasia
Impaired right/left discrimination
Slow perforamnce, cautious
Aware of deficits → depression/anxity
Impaired comnprehension related to language, math
Artery-specific manifestations of strokes
Anterior cerebral → leg > arm weakness, personality changes
Middle cerebral → arm > leg weakness, aphasia (dominant side), neglect (non-dominant)
Posterior cerebral → visual deficits, hallucinations
Vertebrobasilar → cranial nerve deficits, vertigo, ataxia, coma risk
Effect of stroke on ACA (sx)
Leg > arm weakness, personality changes
Effect of stroke on MCA (sx)
Classic stroke sx
Arm > leg weakness
Hemiparesis
One-sided sensory loss
Aphasia (dominant side)
Neglect (non-dominant)
Effect of stroke on PCA (sx)
Visual deficits
Hallucinations
Balance/coordination
Decreased LOC if brainstem is involved
Effect of stroke on vertebrobasilar artery (sx)
Cranial nerve deficits, vertigo, ataxia, coma risk
MCA stroke has what symptoms?
Classic stroke sx
Arm > leg weakness
Hemiparesis
One-sided sensory loss
Aphasia (dominant side)
Neglect (non-dominant)
Vertebrobasilar artery stroke has what symptoms?
Cranial nerve deficits, vertigo, ataxia, coma risk
ACA stroke has what symptoms?
Leg > arm weakness, personality changes
PCA stroke has what symptoms?
Visual deficits
Hallucinations
Balance/coordination
Decreased LOC if brainstem is involved
Motor deficits from stroke result from:
Destruction of motor neurons in pyramidal pathway
Pattern of recovery of motor function after stroke
Initial → flaccidity, hyporeflexia (days to weeks)
If flaccid for too long = bad, we want spasticity (spasticity means nervous system is reconnecting itself)
Progression -. spasticity, hyperreflexia develops
Gradual return of voluntary movement (proximal and gradually to distal)
Characteristics of motor deficits from stroke
Contralateral deficits (opposite side from brain lesion)
Weaknes sor paralysis (hemiparesis/hemiplegia)
Loss of skilled voluntary movement (akinesia)
Altered muscle tone
Changed reflexes
MCA stroke: upper extremity > lower extremity weakness
Position tendencies (motor deficits of strokes) nursing implications
Need to position patient’s joints correctly to avoid injury and pain
When they’re flaccid, day oen we want to position joints correctly so they don’t get injury from flaccidity
Shoulder → internal rotation
Arm → flexion contractures at hand, wrist, elbow
Hip → external rotation
Foot → plantar flexion (footdrop)
Nursing interventions for contractures (motor deficits after stroke)
When patient is flaccid; day one we want to position joints correctly to avoid pain and injury as patient gradually becomes more spastic → maintain alignment of joint
Trochanter rolls
Arm supports
Hand cones
Leg splints
High top shoes
Communication deficits of strokes
Broca’s aphasia
Wernicke’s aphasia
Global aphasia
Dysarthria
Frontal lobe damage
Understand speech BUT can’t speak fluently
Broc → broken speech
Short, effortful phrases, omits small words
Aware of problem → frustration
Example: “Walk dog” for “I will take the dog for a walk)
These are clinical manifestations of what condition?
Broca’s aphasia (nonfluent/expressive)
Temporal lobe damage
Speaks fluently BUT doesn’t make sense
Wer = word salad
Can’t understand speech
Unaware of errors
Example: “You know that smoodle pinkered…”
These are clinical manifestations of what condition?
Wernicke’s aphasia (fluent/receptive)
Describe Broca’s aphasia (nonfluent/expressive)
Frontal lobe damage
Understand speech BUT can’t speak fluently
Broc → broken speech
Short, effortful phrases, omits small words
Aware of problem → frustration
Example: “Walk dog” for “I will take the dog for a walk)
Describe Wernicke’s aphasia (fluent/receptive)
Temporal lobe damage
Speaks fluently BUT doesn’t make sense
Wer = word salad
Can’t understand speech
Unaware of errors
Example: “You know that smoodle pinkered…”
Extensive language area damage
Severe communication difficulties
Limited speaking AND understanding
These are clinical manifestations of what condition?
Global aphasia
Muscular control problem
Slurred speech, poor articulation
Language and comprehension intact
These are clinical manifestations of what condition?
Dysarthria
Describe global aphasia
Extensive language area damage
Severe communication difficulties
Limited speaking AND understanding
Describe dysarthria
Muscular control problem
Slurred speech, poor articulation
Language and comprehension intact
What type of strokes cause aphasia?
Left-sided strokes
Communication strategies for patients with aphasia
Simple sentences
Be patient; allow ample time to respond
Use gestures or pictures
Maintain calm environment
Goal is to teach patients how to communicate their own needs rather than speak for them
Consult speech therapy
Emotional/affect changes of strokes
Joker syndrome
Emotional lability (unpredictable mood swings)
Pseudobulbar affect (inappropriate crying/laughing)
Depression/anxiety
Apathy
Other stroke manifestations
Emotional/affect changes
Joker syndrome + apathy (labile, depressed, inappropriate laughing/crying unrelated to actual feelings) → loss of emotional control mechanisms regulated by brain
Teach patient it’s a neurological sx, NOT a psychological sx
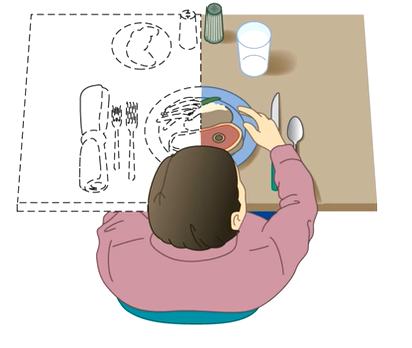
Spatial-perceptual problems
e.g. homonymous hemianopsia
Neglect syndrome (ignores affected side; may have blindness in one side or do not notice things on affected side)
Position food on unaffected half of plate
Agnosia (can’t recognize objects e.g. may not recognize fork even when looking at it)
Apraxia (can’t perform learned sequential movements e.g. not able to brush teeth)
Elimination
Urinary urgency, frequency, incontinence (usually temporary)
Constipation (immobility, weak abd muscles)
Intellectual function
Memory impairment, impaired judgment, difficulty w/ abstract thinking
Stroke patient ignores affected side; may have blindness in one side or do not notice things on affected side
Position food/ on unaffected half of plate
This is called =
Neglect syndrome
Stroke patient can’t recognize objects e.g. may not recognize fork even when looking at it. This is called =
Agnosia
Stroke patient' can’t perform learned sequential movements e.g. not able to brush teeth. This is called =
Apraxia
What problems with elimination do stroke patients have?
Urinary urgency, frequency, incontinence (usually temporary)
Constipation (immobility, weak abd muscles)
What problems with intellectual function do stroke patients have?
Memory impairment, impaired judgment, difficulty w/ abstract thinking
Spatial-perceptual alteration wher epatient doesn’t recognize a whole side of what’s going on in their body.
Homonymous hemianopsia
Diagnostic studies for stroke
Immediate priority is to determine time of sx onset (critical for tPA eligibility; must be within 3-4.5 hrs)
Imaging stu\dies
Noncontrast CT or MRI (FIRST TEST)
CT angiography (CTA)
MRI/MRA)
Cardiac assessment
ECG, echocardiography
Cardiac markers (e.g. troponin + BNPs)
Many strokes are caused by cardiac embolic
Blood tests
CBC, Plts
Coagulation studies (PT/PTT)
Electrolytes, glucose
Lipid profile
Renal and hepatic function
Lumbar puncture (if suspect SAH but CT is negative)
Look for signs of xanthochromia in CSF to indicate old blood/BRB)