Exam 2
1/106
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
107 Terms
Components of Blood and Proportions
formed elements = 45%
RBCs/erythrocytes
WBCs/leukocytes
platelets/thrombocytes
plasma = 55%
mainly water
Functions of Blood
transportation
protection
homeostasis
Transportation
O2, CO2, nutrients, wastes, hormones
supply must meet bodily demands
RBCs transport O2, CO2, H+
Protection
immune responses, blood clotting
protect from pathogens
WBCs
Homeostasis
thermoregulation
pH control
maintaining fluid volume
Components of Plasma
water = 90%
proteins = 8%
respiratory gases
nutrients
waste products… nitrogenous waste, pollutants
electrolytes
hormones
Structure and Function of Erythrocytes
shape and why it is advantageous
biconcave discs… circular + flat with indentation on each side
good b/c increased surface area to carry more
structure (not a true cell)
no nucleus, no mitochondria
why it can generate ATP anaerobically, why advantageous
good b/c the cell won’t eat its own cargo/O2
ex: if a ice cream truck driver ate all of the ice cream, there would be none to give out to customers
Hemoglobin
4 globin chains
hold CO2 waste
made of proteins
4 heme groups
made of iron
hold O2
different names based on what is attached:
oxyhemoglobin = holds O2, in arteries, ruby red
deoxyhemoglobin = holds H+, dark red
carbaminohemoglobin = holds CO2
Oxyhemoglobin
holds O2
found in arteries… oxygenated blood
ruby red blood
Carbaminohemoglobin
holds CO2
found in veins… deoxygenated blood
Deoxyhemoglobin
holds H+
found in veins… deoxygenated blood
Erythropoiesis
begins as stem cell → becomes reticulocyte after 15 days → matures into erythrocyte within 2 days of release
Reticulocyte Count
1-2% of all RBC in blood sample
important b/c demonstrates proper production of RBCs and function of bone marrow
Homeostatic Control of Erythropoiesis
stimulus = hypoxia… due to low RBC, low hemoglobin, low O2 availability
kidney released ERYTHROPOIETIN or EPO
erythropoietin stimulates red bone marrow to produce RBCs
more RBCs released into bloodstream
body can carry more O2
back to homeostasis
Causes of Hypoxia
low O2 availability… living at high altitudes
low hemoglobin to carry O2… anemia
low RBC count
Production Process of RBCs
low O2 levels in blood
kidneys produce erythropoietin/EPO
EPO in blood triggers erythropoiesis in bone marrow
new erythrocytes enter bloodstream after 120 days
Destruction Process of RBCs
hemoglobin scrapped by spleen/liver and bone marrow
broken into heme and globin units
heme breakdown creates bilirubin by-product, iron is stored in liver
globin is turned into amino acids back into blood
Red Blood Cell Count
4-6 million RBC/mm3
Reticulocyte Count
1-2% of all RBC in blood sample
indicate proper function of bone marrow and production of RBCs
Hematocrit
female = 42 ± 5%
male = 47 ± 5%
measures how much of blood volume is made up of RBCs
Hemoglobin Concentration
female = 12-16 grams/100mL
male = 13-18 grams/100mL
Differential White Blood Cell Count
4,800-10,800/uL
test allows doctor to see how many of each specific WBC is in blood
reveals immunocompromization or specific infection
Leukocyte Types + Percentages
most prevalent
neutrophils = 50-70%
lymphocytes = 25-45%
monocytes = 3=85
eosinophils = 2-4%
basophils = 0.5-1%
least prevalent
NEUTROPHIL LYMPHOCYTE MONOCYTE EOSINOPHIL BASOPHIL
NEVER LET MONKEYS EAT BANANAS
Neutrophils
50-70% of WBCs
specialized to kill bacteria by PHAGOCYTOSIS
1st soldier on the battlefield
numbers increase with bacterial infection
MAIN FUNCTION = eat/engulf bacteria invaders
Lymphocytes
25-45% of WBCs
can carry out immune response via cell attack or antibody production
mostly in spleen and lymph nodes
T and B cells
MAIN FUNCTION = direct cell attack (T cells) and antibody production (B cells)
Monocytes/Macrophages
3-8% of WBCs
in blood = monocyte
outside of blood = macrophage
PHAGOCYTIZE INVADING PATHOGENS AND DEBRIS
MAIN FUNCTION = leave blood + eat invaders/debris
Eosinophils
2-4% of WBCs
use digestive enzymes to kill parasitic worms
numbers increase w/ allergic reaction or parasitic infection
MAIN FUNCTION = secrete digestive enzyme to kill parasitic worms
Basophils
0.5-1% of WBCs
release histamine → dilates vessels → increased blood flow to tissue → allows WBCs to get to and fight infection + inflammation
MAIN FUNCTION = secrete histamine to dilate vessels + allow for more WBCs to enter and fight infection
Antigen Receptor
“looks” of cell
protein bumps on surface of cell membrane
used for identification
Antibody
WBC that detects if antigen/cell belongs in body
matches antigen = identification that cell belongs
no match = sign to destroy, foreign
Type A Antigens + Antibodies
antigens = A
antibodies = B
Type B Antigens + Antibodies
antigens = B
antibodies = A
Type AB Antigens + Antibodies
antigens = A + B
antibodies = none
Type O Antigens + Antibodies
antigens = none
antibodies = A + B
Blood Types Compatible with A+
A+
A-
O+
O-
Blood Types Compatible with A-
A-
O-
Blood Types Compatible with B+
B+
B-
O+
O-
Blood Types Compatible with B-
B-
O-
Blood Types Compatible with AB+
AB+
AB-
A+
A-
B+
B-
O+
O-
Blood Types Compatible with AB-
AB-
A-
B-
O-
Blood Types Compatible with O+
O+
O-
Blood Types Compatible with O-
O-
Universal Donor
O-
can be donated to all because it has no antigens
no antigens = no antibodies will kill it
Universal Recipient
AB+
has all of the antigens so it has no antibodies against antigens
all antigens = can accept any blood without it being a harm
Rh Factor and Positive or Negative Classification
Rh+ = has the antigen
Rh- = does not have the antigen… only will have antibodies if exposed before to Rh+
Rh- Woman Pregnant with Rh+ Children
Rh- mother has no antibodies against Rh factor because no previous exposure
Rh- mother gets pregnant and baby has Rh+ blood
during delivery, Rh- mother is exposed to Rh+ blood
Rh- mother develops antibodies
without rhogam:
Rh- mother gets pregnant with second baby with Rh+ blood
mother now has antibodies which attach baby’s blood… hemolytic anemia
with rhogam:
Rh- mother gets pregnant with second baby with Rh+ blood
mother takes rhogam
rhogam weakens immune system (B cells)
baby’s blood is not attacked + healthy pregnancy occurs
Steps of Hemostasis
process by which the body stops leakage of blood from a damaged blood vessel
vascular spasm
platelet plug formation
coagulation
Vascular Spasm
smooth muscle contracts
immediate response to slow leakage
vessel walls tighten to try to line up ripped edges together
Platelet Plug Formation
platelets adhere to rip and become sticky
more platelets aggregate + stick on… positive feedback loop
platelets glue together edges of ripped vessels
Coagulation
mesh is created using fibrin
mesh stabilizes plug + creates a clot
clot seals off blood vessel
glue dries ripped vessel walls together
Three Phases of Coagulation
two pathways to prothrombin activator
common pathway to thrombin
common pathway to fibrin mesh
Two Pathways to Prothrombin Activator
intrinsic = within blood vessel
extrinsic = in tissue around blood vessel
Common Pathway to Thrombin
prothrombin activator converts prothrombin to thrombin
Common Pathway to Fibrin Mesh
thrombin converts fibrinogen into fibrin
fibrin can now be used to form mesh + plug blood vessel
Clot Retraction
30-60 mins after injury
actin and myosin within platelets contract
pulls torn edges of vessel closer together
Fibrinolysis
breaks down clot once healing has occurred
plasmin digests fibrin
about 2 days after clot formation
Fibrin-Digesting Enzyme or “Clot Buster”
PLASMIN
Why Patients with Advanced Kidney Disease are often Anemic
poor kidney function → low EPO production → low creation of RBCs in bone marrow → ANEMIA
Hemophilia and why Aspirin Should Not be Taken
hemophilia = thin blood, low clotting
should not take aspirin because it inhibits platelet plug formation
simple: hemophiliacs already have thin blood, they don’t need it even thinner and unable to clot
Anemia
blood’s O2 carry capacity is too low
broad categories:
blood loss
low RBC production
rapid RBC destruction
Anemia due to Blood Loss
hemorrhagic anemia
can be acute (bleed from wound) or chronic (bleed from ulcers)
once bleed is resolved, erythropoiesis should restore RBC count
Anemia due to Low RBC Production
potential causes:
lack of raw materials… low amino acids or iron
red bone marrow failure
examples:
iron-deficiency anemia… diet is insufficient or cannot absorb
renal anemia… kidneys do not produce enough EPO
aplastic anemia… red marrow destroyed or inhibited
Anemia due to Destruction of RBCs
hemolytic anemia… RBCs rupture prematurely
potential causes:
abnormal hemoglobin
mismatched blood transfusion
infection
examples:
sickle-cell anemia
thalassemia… one of globin chains is absent/faulty… thin Hb deficient RBCs made
Sickle Cell Anemia
deformed RBCs that can rupture easily and get stuck in smaller vessels
O2 deficiency causes pain, gasping for air
NEED TRANSFUSION IN CRISIS
s/s = pain, fatigue, gasping for air
Effects of Leukemia on Production of WBCs, RBCs, and Platelets
overproduction of cancerous WBCs → reduced production of RBCs + platelets
fewer platelets → poor clotting → hemorrhage
WBCs produced are ineffective → immunocompromised
fewer RBCs → anemia
Lymphatic System Functions
return interstitial fluid and leaked plasma proteins back to blood
provide structural basis of immune system
Lymph Vessels vs Blood Vessels
capillaries
lymph capillaries are more permeable
lymph capillaries have one-way minivalves
collecting vessels
collecting vessels in skin travel with superficial veins
collecting vessels deep travel with arteries
nutrients are supplied from branching vasa vasorum
Lymphatic Vessels
direction of flow
one direction from TISSUE TO HEART
presence of nodes + collecting vessels
capillaries → collecting vessels → trunks and ducts
Flow of Lymph from Interstitial Fluid to Subclavian Veins
5 different trunks
2 main ducts
veins that empty the lymph
5 Lymphatic Trunks
paired lumbar = drains lower back + legs
paired bronchomediastinal = drains respiratory + thoracic
paired subclavian = drains arms
paired jugular trunks = drains head + neck
single intestinal trunk = drains abdomen
2 Main Lymphatic Ducts
right lymphatic duct
thoracic duct
empties lymph into venous circulation at junction of internal jugular and subclavian veins on own side of body
Mechanisms Helping Flow of Lymph
pulsation of nearby arteries propels lymph
skeletal muscle pump
respiratory pump
valves in vessels
NO SYMPATHETIC CONSTRICTION… NO MUSCLES IN WALLS
T Cells
kill viruses + bacteria
manage immune response
destroy + attack foreign cells by chemical injection + lysis
B Cells
produce antibodies
produce plasma cells which secrete antibodies
Macrophages
phagocytize foreign substances and help activate T cells
Structure and Function of Lymph Nodes
function = FILTER LYMPH
macrophages destroy microorganisms + debris
immune function = lymphocytes are activated + mount an attack
remove viruses/bacteria/invaders b4 they reach the heart
embedded in connective tissue, in clusters along lymphatic vessels
near body surface in inguinal, axillary, and cervical body regions
Afferent and Efferent Lymph Node Vessels
few efferent vessels, more afferent vessels → creates slow flow of lymph for better filtration + consumption of pathogens
lymph enters, travels through sinuses, exits node
Inflamed Lymph Nodes
have to filter many pathogens → inflamed and tender → swollen glands
PAIN IS A GOOD SIGN… means inflammation is present
Cancerous Lymph Nodes
nonpainful, swollen is a sign of cancerous
lymphoma
Spleen
largest lymphoid organ
functions:
site of lymphocyte proliferation and immune response
cleanses blood of aged cells + debris
stores breakdown products of RBC for reuse
stores blood platelets
contains lymphocytes, macrophages, and erythrocytes
structure:
white pulp = lymphocytes
red pulp = blood vessels
JUNKYARD SALVAGING DEAD CELLS FOR PARTS
Thymus
increases in size with age → stops growing during adolescence → atrophies
most active during childhood
contains lymphocytes and macrophages
site of T-cell maturation
Tonsils
ring of lymphatic tissue around the pharynx
first line of defense against pathogens
crypts in tissue trap and destroy bacteria
Innate Defenses
BORN WITH THESE DEFENSES
surface barriers (skin and mucosa)
internal defenses (cells + chemicals)
Adaptative Defenses
NOT BORN WITH, ADAPT/PICK UP AS YOU GROW + ARE EXPOSED
humoral immunity
cellular immunity
First Line of Defense: Non-Specific Surface Membrane Barriers
SERVE AS A PHYSICAL BARRIER AGAINST MICROORGANISMS
role of skin
skin is tough and resistant to many toxins and enzymes
hairs can trap and filter particles
role of mucous membranes
mucous can trap microorganisms and sweep upward
other
various chemicals within body can kill bacteria
enzymes in stomachs kill different microorganisms
Second Line of Defense: Non-Specific Internal Defenses
different types of phagocytes + mechanism
neutrophils + macrophages
phagocyte adheres to pathogen → forms capsule and engulfs → enzymes digest the particles → exocytosis removes the residual material
natural killer cells
specialized T cels
nonspecific
secrete enzymes + chemicals to kill cells
perforin chemical makes holes in cell membrane → cytotoxin enters… “need to make holes in wall before you throw grenade in”
inflammatory response → process + signs
basophils release histamine → vasodilation of local vessels → increased capillary permeability → plasma and WBC leak out
benefits = sets stage for repair, disposes of pathogens
s/s = warmth, pain, redness, swelling
antimicrobial proteins
complements = emergency response activator… label cell for phagocytosis and attract phagocytic cells, forms damaging holes in plasma membrane
interferons = invaded cell produces interferons → go to neighbor cell → warns it that an invader is coming → neighbor cell goes into lockdown
fever
abnormally high body temperature
WBCs release pyrogens that reset hypothalamus thermostat
increased temp inhibits bacterial growth + enhances repair
s/s = discomfort, fatigue, dehydration
NEED A FEVER TO SPEED UP IMMUNE PROCESS
Third Line of Defense: Adaptive Defenses
specific: target and kill only virus
systemic: protect whole body
memory: do not need to make new ones in response to repeat exposure
B Cells
contact extracellular antigen → create plasma cells → release antibodies → prepare antigen for destruction
Antigen-Presenting Cell
comes around when it discovers a threat
attaches to antigen receptors on infected cells → collects intel → migrates to lymph node → tells B cells to make antibodies to match viral antigen
dendritic cells, macrophages, and B cells
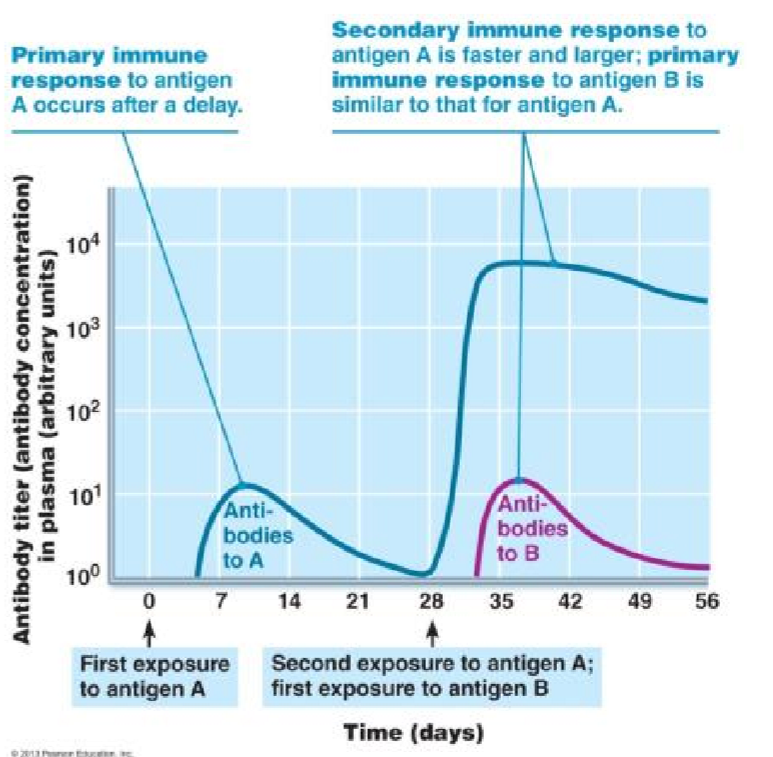
Graph of Antibody Concentration in Response to Primary and Secondary Exposure
secondary immune response is quicker, stronger, and longer lasting
Lymphocyte Maturation
immunocompetence = able to recognize a specific antigen by binding to it
self-tolerant = unresponsive to self-antigens… doesn’t attack own body cells
B cell maturation in BONE MARROW
T cell maturation in THYMUS
origin = B and T cells originate in bone marrow from stem cells
maturation = T cells go to thymus, B cells stay in bone marrow + mature
seeding = mature lymphocytes seed lymphoid organs and circulate through blood + lymph… still naive
antigen encounter + activation = activated after encountering an antigen
proliferation/differentiation = multiply and can become plasma or memory cells, then circulate body
Differences Between Primary and Secondary Immune Responses
secondary response is FASTER, LARGER, AND PROLONGED
already has memory cells that can quickly react → do not need to identify and then produce plasma cells
Humoral Immunity
B-lymphocytes
antibody-mediated, protect against extracellular antigens
B lymphocyte is activated after encountering matching antigen → B cells clone themselves into plasma cells (release antibodies) and memory cells (increase response rate during next exposure)
Active Naturally Acquired
active = you are making antibodies
infection + contact with pathogen → body becomes infected and eventually builds protection
ex: chicken pox parties
HIGH RISK
Active Artificially Acquired
active = you are making antibodies
vaccine; dead or weakened pathogens activate T + B cells
ex: COVID vaccine
LOW RISK
Passive Naturally Acquired
passive = someone else makes antibodies for you
antibodies passed from mother to fetus via placenta, antibodies passed from mother to infant via breastmilk
Passive Artificially Acquired
passive = someone else makes antibodies for you
injection of exogenous antibodies
ex: antivenom, rabies, tetanus shot
Vaccines
exposure to dead or weakened pathogen → body builds immune response → if exposed to active pathogen, body has secondary response
Cellular Immunity
T-lymphocytes
activated by antigen encounter
kill directly or release chemicals that regulate other components of immune system
protect against intracellular antigens
Helper T Cells
help activate T and B cells
activate macrophages
recruit other immune cells