PERCEPTION EXAM 3 - the bodily senses
1/65
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
66 Terms
WHAT is SOMATOSENSATION? What are its 2 COMPONENTS?
The body senses
Somesthesis
Propioception
WHAT is SOMESTHESIS? HOW does it MANIFEST (5 ways)?
Cutaneous (SKIN) sensitivity
Light pressure
Deep pressure
Coldness
Heat
Pain
WHAT is PROPRIOCEPTION? WHAT are its TWO subsenses?
Bodily awareness without visual confirmation–knowledge of spatial position & movement of the body
Kinethesis (knowledge of spatial position/movement)
Vestibular (balance)
What 3 RECEPTORS are provided on/through SKIN?
Chemoreceptors–chemical energy (chemical irritation–itch, burns)
Thermoreceptors–thermal energy (heat/cold)
Mechanoreceptors–mechanical energy (pressure)
What are the 3 MAJOR CHARACTERISTICS of the SKIN? WHAT are its 3 ROLES in the body?
MAJOR CHARACTERISTICS:
Largest organ of human body
Defines individuals
Can be hairy or hairless
ROLES IN THE BODY:
Roles in temp. Regulation
Protection
Respiration
What are the 3 LAYERS of the SKIN?
Epidermus (outer)
Dermus (inner)
Subcutaneous tissue
What 5 ENERGIES (stimuli) do SKIN RECEPTORS detect?
Light touch
Deep touch
Heat
Cold
Pain
WHAT KIND of RECEPTORS on the skin respond to TOUCH (light/deep pressure)? What do they RESPOND TO? What are their 2 KEY characteristics?
MECHANORECEPTORS respond to SKIN DISPLACEMENT (mechanical stimulation of body surface)
SENSITIVE —.000004 inch displacement triggers a response
ADAPTIVE for passive stimulants, but not active, touch–i.e. wearing clothes
WHAT KIND of RECEPTORS on the skin respond to TEMPERATURE (2 TYPES)? What do they RESPOND TO? WHAT 3 BODILY PROCESSES does it affect? What are their KEY characteristic?
THERMORECEPTORS respond to CONSTRICTION/DILATION of blood vessels (THERMAL STIMULATION)
AFFECTS 3 BODILY PROCESSES (Blood flow, perspiration, and piloerection)
ADAPTIVE: Psychological zero (range of thermal indifference)
WHAT KIND of RECEPTORS on the skin respond to PAIN? WHAT are they responding TO? WHAT are pain receptors 2 KEY CHARACTERISTICS (evolutionarily and otherwise)?
NOCICEPTORS respond EXTREME MECHANICAL/THERMAL STIMULATION
Biologically advantageous–pain results from potentially dangerous stimuli
DOES NOT show adaptation
What 6 STRUCTURES conduct TRANSDUCTION (& hold receptors) in the SKIN SENSES?
Merkel's disc
Free nerve endings
Meissner's corpuscle
Hair follicle receptors
Pacinian corpuscle
Ruffini's end organ
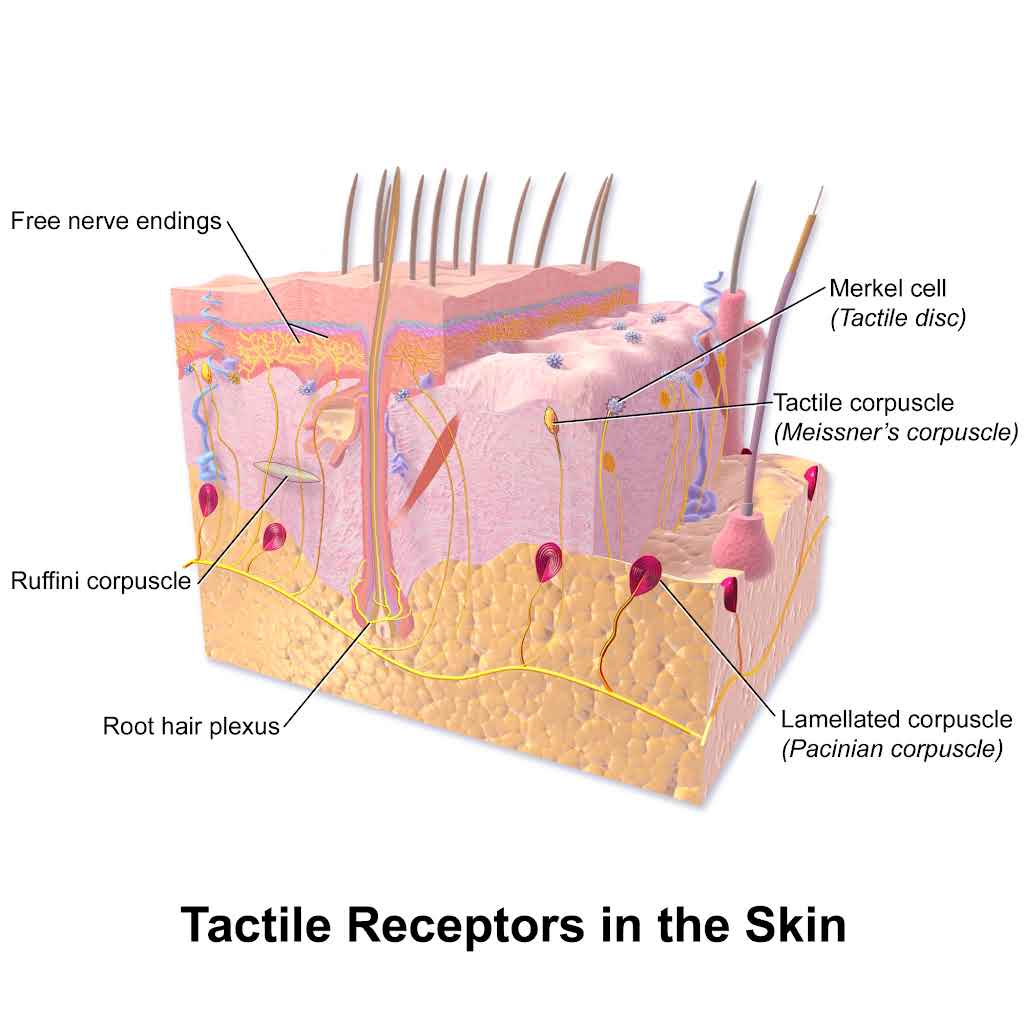
What does the MERKEL’S DISC sense/transduce?
Sustained touch/pressure
What 5 SIGNALS do FREE NERVE ENDINGS sense/transduce?
touch, pressure, stretch, pain, temperature
What does the MEISSNER’S CORPUSCLE sense/transduce?
Texture changes
What do HAIR FOLLICLE RECEPTORS sense/transduce?
Position of hairsWhat does the PACIAN CORPUSCLE sense/transduce?
What does the PACIAN CORPUSCLE sense/transduce?
Deep pressure
What does the RUFFINI’S END ORGAN sense/transduce?
Sustained pressure
What 2 FACTORS determine how TOUCH is DETECTED?
Spatial resolution (high vs low)
Receptive field (large vs small)
What 2 KINDS of RECEPTORS detect LIGHT & DEEP PRESSURE energy?
Fast-adapting receptors
Slow-adapting receptors
What are the 2 KEY CHARACTERISTICS of COLD receptors (abundance & what temps they fire)? WHAT survival PHENOMENON do COLD receptors produce?
Cold receptors are 3.5 times more numerous.
Fire below 41˚F to 109˚F, also fire 113˚F
PARADOXICAL COLD (cold sensation in response to extreme heat)
What are the 2 KEY CHARACTERISTICS of HEAT receptors (transmitters & what temps they fire)? WHAT survival PHENOMENON do HEAT receptors produce?
Transmitted by C fibers
Fire 82˚-117˚, also fire below 59˚
PARADOXICAL HEAT (Heat sensation in response to extreme cold)
WHAT 2 FIBERS make up PAIN?
A-delta fibers (myelinated)
heat and pressure—FIRST wave of pain (sharp/localized)
10x faster than nonmylinated fibers
C fibers (nonmylinated)
slower—SECOND pain (throbbing/aching)
What is CIPA? What CAUSES it? What does this MEAN (life implications & morality rate)? What do patients REQUIRE?
Congenital Insensitivity to Pain with Anhidrosis (CIPA)—Rare genetic condition resulting in no free nerve cell endings–Patients cannot detect pain, warmth, or cold
Numerous accidental self-inflicted injuries/burns
Half of all CIPA children die before the age of 3 because of overheating
Requires consistent monitoring for injuries and temperature
WHAT do we use to measure SKIN RECEPTOR SENSITIVITY? HOW can they differ (2 ways)?
SPECIFIC RECEPTIVE FIELDS—Larger receptor field = less specificity
DIFFERNECES:
field SIZES
receptor DENSITIES
HOW do we measure RECEPTOR SENSITIVITY? WHAT does it MEASURE? What SCHOOL of PSYCHOLOGY does it belong to?
The two-point threshold procedure
Measures ABSOLUTE THRESHOLD of detection of different parts of the body—LARGER receptor field = HIGHER absolute threshold/baseline for detection
“Did you feel one point or two?”
Psychophysics
Where are we MOST sensitive to touch? WHY? What 3 PARTS OF THE BODY?
THE EXPOLORATORY AREAS–SMALL reception fields with HIGH receptor density
Fingers
Feet
Genitals
How does the SKIN SENSES CODE energy (D.I.L.T)?
Duration: onset/offset of firing–well identified
Intensity: NUMBER of neurons fired/firing rate
More intense stimuli = more vigorous firing rate
Location: determined by which receptors fire
Type: identified by type of receptor stimulated (Primary Receptors)
What do TOUCH RECEPTORS detect to LOCALIZE energy? What does this MEAN for the receptors?
By detecting MOVEMENT
Receptors = DIRECTIONALLY SENSITIVE
How do PAIN RECEPTORS LOCALIZE energy? WHAT FACTOR creates a DIFFERENCE?
Depends!
Sharp pain = well located
Dull/referred pains = poorly located
WHY does TEMPERATURE RECEPTOR LOCALIZATION tend to be POOR?
Spatial localization tends to be poor because of spatial summation of receptor firing—many receptors fire together & signals blur into one combined message instead of a precise one.
What are the 2 TRANSMISSION pathways for TOUCH?
Dorsal-column-medial-lemniscal pathway
Spinothalamic pathway
What is the DORSAL-COLUM-MEDIAL-LEMNISCAL PATHWAY of TOUCH TRANSMISSION (3 steps)?
A-beta fibers: fine touch/pressure information
Smaller and more numerous receptive fields (more precise)
[moves] Contralateral to ventrobasal complex
What is the SPINOTHALAMIC PATHWAY of TOUCH TRANSMISSION (3 steps)?
A-Delta and C fibers: myelinated, fast axons for sharp pain (temperature and touch as well)
larger receptive fields with spatial summation
[moves] Contralateral to ventral posterolateral nucleus
What is THE GATE CONTROL THEORY OF PAIN? HOW do signals TRAVEL in BOTH COMPONENTS of the theory? WHAT STRUCTURE is the “gate”?
Pain Signal Transmission results from Bottom-up AND Top-Down Processes
Spinal cord → Substantia gelatinosa (SG) of the dorsal horn = the GATE
Bottom-up = Signals COME IN and the Spinal Cord [gate] DETERMINES IF pain signal REACHES brain
Intensity of pain and touch signals
Touch info can OVERRIDE & pain BLOCK info and its transmission to the brain, closing the “gate”
Top-down = Brain SENDS MESSAGES through DESCENDING FIBERS that STOP/AMPLIFY/REDUCE pain transmission THROUGH the “gate”–DISSOCIATING from pain
Context, situation, emotion, attentional focus
Where does BODILY SENSORY PROCESSING (CORTICAL PROCESSING) occur? WHERE is it LOCATED?
The somatosensory cortex
Located in parietal lobe
HOW are the skin senses REPRESENTED in CORTICAL PROCESSING?
Topographically (map-like)
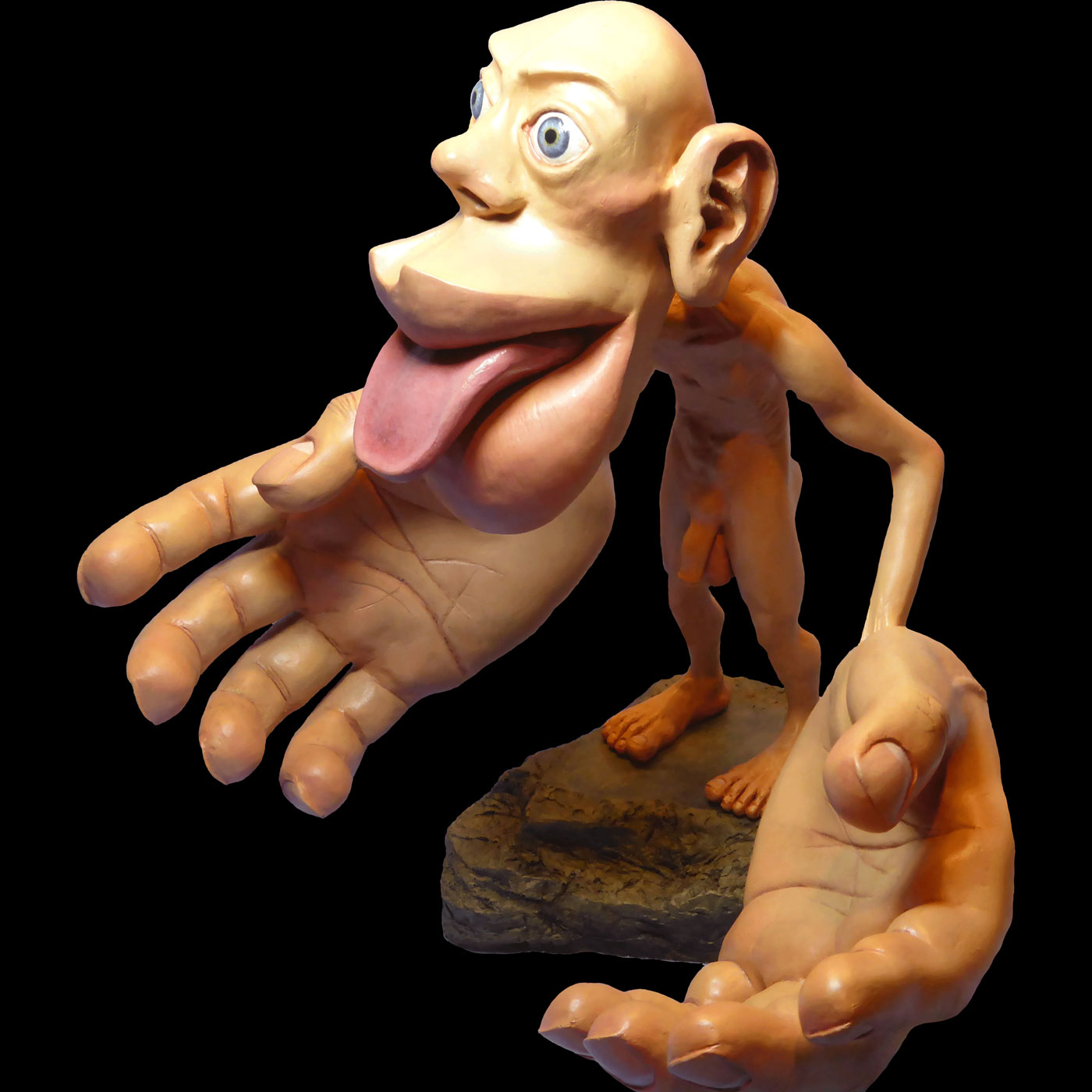
What DETERMINES CORTICAL REPRESENTATION? What IS the RELATIONSHIP between BODY AREA & CORTICAL REPRESENTATION? HOW is this relationship VISUALLY REPRESENTED?
Determined by RECEPTOR DENSITY in body parts
MORE SENSITIVE areas of the body = GREATER cortical representation
Visually represented THROUGH SENSORY HOMUNCULUS
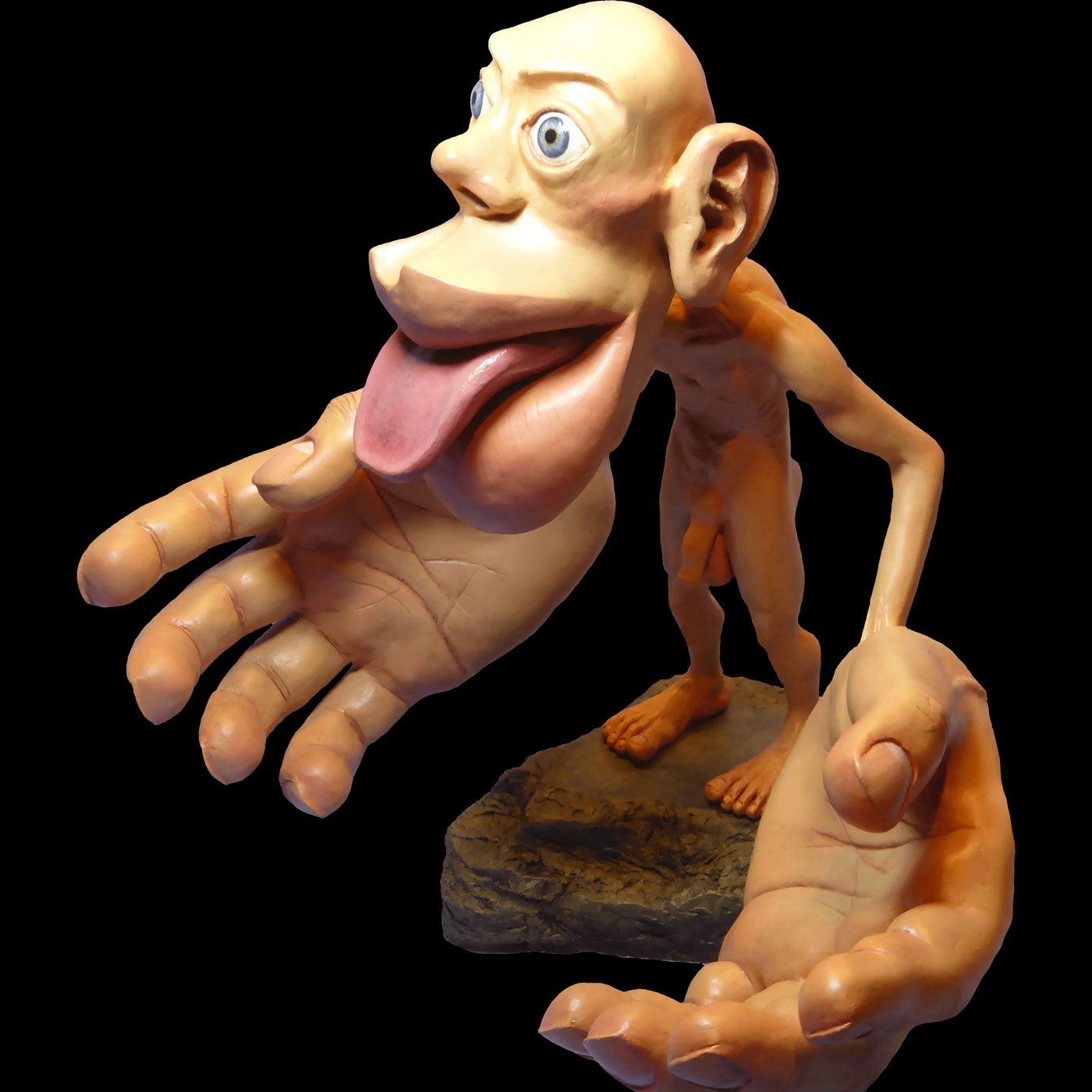
What RATIO does the SENSORY HOMUNCULUS represent?
1:1 representation of RECEPTOR DENSITY throughout the body
What is PHANTOM LIMB? WHO (percentage of what demographic) experiences it? What CAUSES it? WHEN does it occur?
An often painful sensation that an amputated/missing limb is still attached
Experienced by 60-80% of Amputees
CAUSED BY reorganization of Somatosensory Cortex
OCCURS in response to all losses: limb removal, mastectomy, tooth removal
Sometimes after gender reassignment surgery (phantom genitals)
What is a FAMOUS CASE of PHANTOM LIMB?
Derek Stein
Reported feeling pain in (phantom) left hand when its corresponding regions in somatosenory cortex started responding to ADJACENT regions linked to the face–REORGANIZATION
What is the BIOPSYCHOSOCIAL MODEL of PAIN?
Pain is influenced biological, psychological, and sociocultural factors
What 8 FACTORS affect PAIN SENSITIVITY (inter-individual variability)? WHICH component of the BIOPSYCHOSOCIAL MODEL do they fit into?
BIOLOGICAL
Genetics–genetic differences
Age–75% of older adults report persistent pains
Medical conditions
Gender–females = more sensitive
PSYCHOLOGICAL
Mental illness–report feeling more body aches
Psychophysiological pain–emotions/expectations
SOCIAL
Cultures–differing expectations
Situations–associations with pain (i.e., childbirth, athletics, initiation rites)
What 5 MEDICAL TREATMENTS affect PAIN SENSITIVITY (biopsychosocial model)?
Pharmacological interventions
NSAIDs (ibuprofen)
Acetaminophen
Opioids
Marijuana
Transcutaneous Electrical Nerve Stimulation (TENS)–providing electrical signals to neural pathways
Surgical interventions
Nerve severance
Nerve blocks
Acupuncture
What 6 PSYCHOLOGICAL TREATMENTS affect PAIN SENSITIVITY (biophysical model)?
Behavioral Management Therapy (BMT)
Psychotherapies
Biofeedback
Palliative support
Empathy & understanding
Occupational assistance
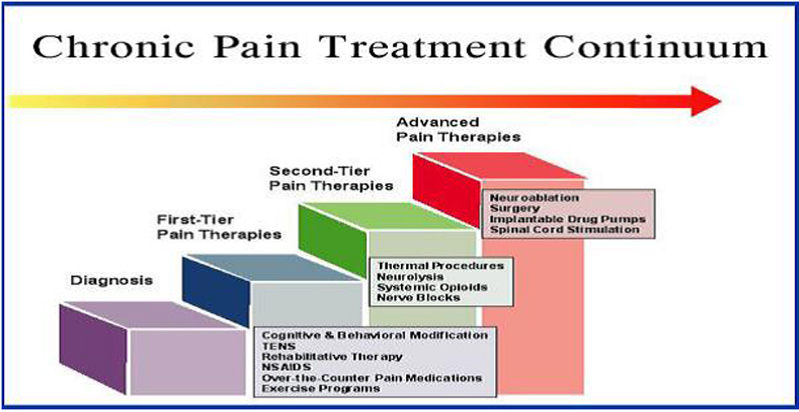
What is the 4 tier CHRONIC PAIN TREATMENT CONTINUUM?
Diagnosis
First-tier pain therapies (NASIDs/TENS/CBT/nerve blocks)
Second-tier pain therapies (opioids/neurolysis/thermal procedures)
Advanced pain therapies (neurostimulation/drug pumps/surgery/neuroablation)
What are OPIATE DRUGS? What do they TARGET? What is their MECHANISM OF ACTION?
Derivatives or synthetic variants of opium that treat pain–Mimics naturally occurring opiate system
TARGET = endogenous opiate neurotransmitter systems (Enkephalins and Endorphins)
Brain’s natural painkillers
M.O.A. = be closing the substantia gelatinosa (SG) gate–area is rich in endorphin pathway
What is ACUPUNCTURE? What does it DO? What is it HELPFUL for? What are its 3 MECHANISMS OF ACTION?
Use of needle insertions and manipulations to treat pain
Stimulates the 14 channels through which Qi (life energy) flows–NOT MUCH SCIENTIFIC EVIDENCE!
TARGET = Helpful for certain types of somatic pain (body, neck, headaches)
M.O.A.’s:
Releases endorphins
Decreased cortical activity
Placebo effect
What are 4 BEHAVIORAL PAIN MANAGEMENT methods?
Relaxation techniques for stress reduction–reduced tension
Biofeedback–giving external signals to internal events
Refocusing attention
Cognitive-behavioral therapy (CBT)
What are KINESTHESIS’S 2 STIMULI?
Internal information about the angle of limbs
Information about movement, stretch, position, etc.
What TYPE of RECEPTORS transduce KINESTHETIC energy? WHERE are KINESTHETIC RECEPTORS located? WHAT do they DETECT?
MECHANORECEPTORS located in muscles, joints and tendons throughout the body
detect the amount of stretch/compression/twisting/tension in the muscles.
What 3 STRUCTURES contain kinesthetic receptors?
Golgi [tendon] organ
Muscle spindles
Pulmonary stretch receptors
What does the GOLGI ORGAN monitor in KINESTHETIC TRANSDUCTION? WHAT does it ACT as? WHERE is it LOCATED?
Monitors changes in muscle tension
Acts as a “BRAKE” against excessively vigorous contraction
Located at muscle fiber-tendon connection.
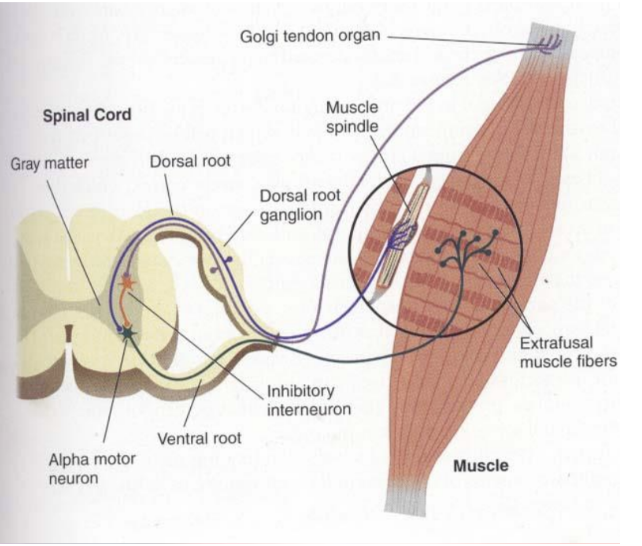
What do MUSCLE SPINDLES MONITOR in KINESTHETIC TRANSDUCTION? What does it PRODUCE?
Monitor level of stretch in muscle fibers.
Produces reflexive contractions as needed.
WHERE are PULMONARY STRETCH RECEPTORS located?
the lungs
What 5 FUNCTIONS is KINETHESIS IMPORTANT for?
Muscle memory–gain in accuracy of muscle movements with continued practice
Hand-eye coordination–integration of visual input to guide bodily movement
Fine/gross muscle movement control
Body awareness
Postural control/adjustment
What are the VESTIBULAR SENSE’S/PROPRIOCEPTION’S 2 STIMULI?
Signals for rotation, orientation with respect to gravity/acceleration through space
Changes in rotational movements of the head
What TWO MOVEMENT PHENOMENA do VESTIBULAR RECEPTORS transduce for?
Rotation
Acceleration
WHERE do VESTIBULAR RECEPTORS code for ROTATIONAL MOVEMENTS?
the Semicircular canals
What are the SEMICIRCULAR CANALS? WHERE are the canals located?
Hair cell receptors that monitor rotational movements
Loated in THREE SEMICIRCULAR CANALS of INNER EAR
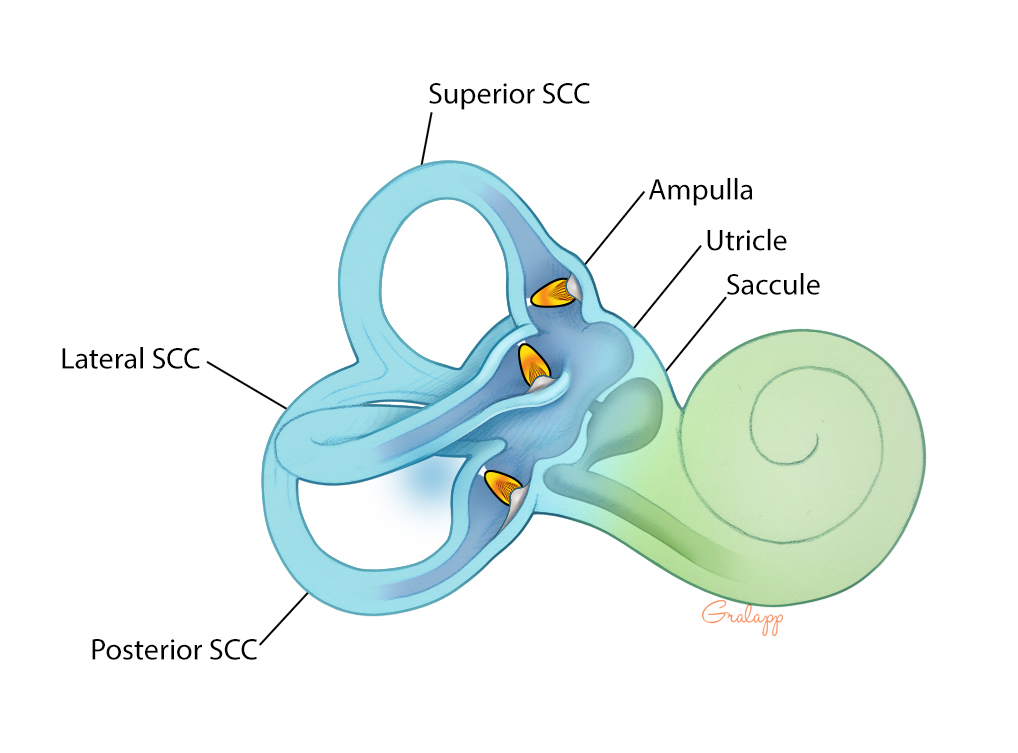
WHERE do VESTIBULAR RECEPTORS code for ACCELERATION (moving through the world)? WHAT 2 STRUCTURES compose it?
Otolith organs
Otoliths
“Ear stones”
What are the 2 OTOLITH ORGANS? WHAT HAPPENS TO THEM as they TRANSDUCE signals? WHAT 3 FACTORS affect their transduction?
Utricle
Saccule
Otoliths (“ear stones”) PRESS AGAINST VESTIBULAR HAIR CELLS
Depends on DIRECTION/TILT/RATE of acceleration
WHAT 4 THINGS is the VESTIBULAR SYSTEM (PROPRIOCEPTiON) important for?
Maintaining balance
Vestibulo-ocular reflex (VOR)–Maintains eye fixation point as we move
Postural control/adjustments–staying upright
Which way is UP
HOW do VESTIBULAR DEFICITS happen? what CAUSES it? WHO (3) is at risk? HOW (through what conditions)?
Inability to perceive one’s position/motion/altitude relative to surroundings–NOT knowing which way is UP!
Mismatch between sensory inputs (visual/vestibular)
GYMNASTS (the twisties)
SCUBA DIVERS (loss of visual inputs)
PILOTS (weather/the leans/elevator illusion)
What are some prominent deaths from spatial disorientation?
Kobe bryant & co.–helicopter crash
“The day the music died”–plane crash
Pilot JFK Jr. –plane crash
Jim Croce–plane crash
Medical jet crash in NE Philadelphia (Jan. 2025)
What 3 SYSTEMS contribute to SPATIAL ORIENTATION? What PECENTAGES do they contribute?
Vision (80%)
Vestibular (15%)
Proprioception (5%)
WHAT 5 CONDITIONS are CAUSED by VESTIBULAR DEFICITS?
Vertigo–false sensation that the person or the world is spinning
Dizziness–vertigo + unsteadiness
Meniere’s Disease–A disorder of the inner ear that can lead to dizzy spells (vertigo) and hearing loss
Motion sickness–vertigo/nausea/vomiting induced by repeated vertical movements