Endocrinology
1/51
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
52 Terms
Metabolic action of Insulin

Causes of thyrotoxicosis

Sings and symptoms of hyperthyroidism

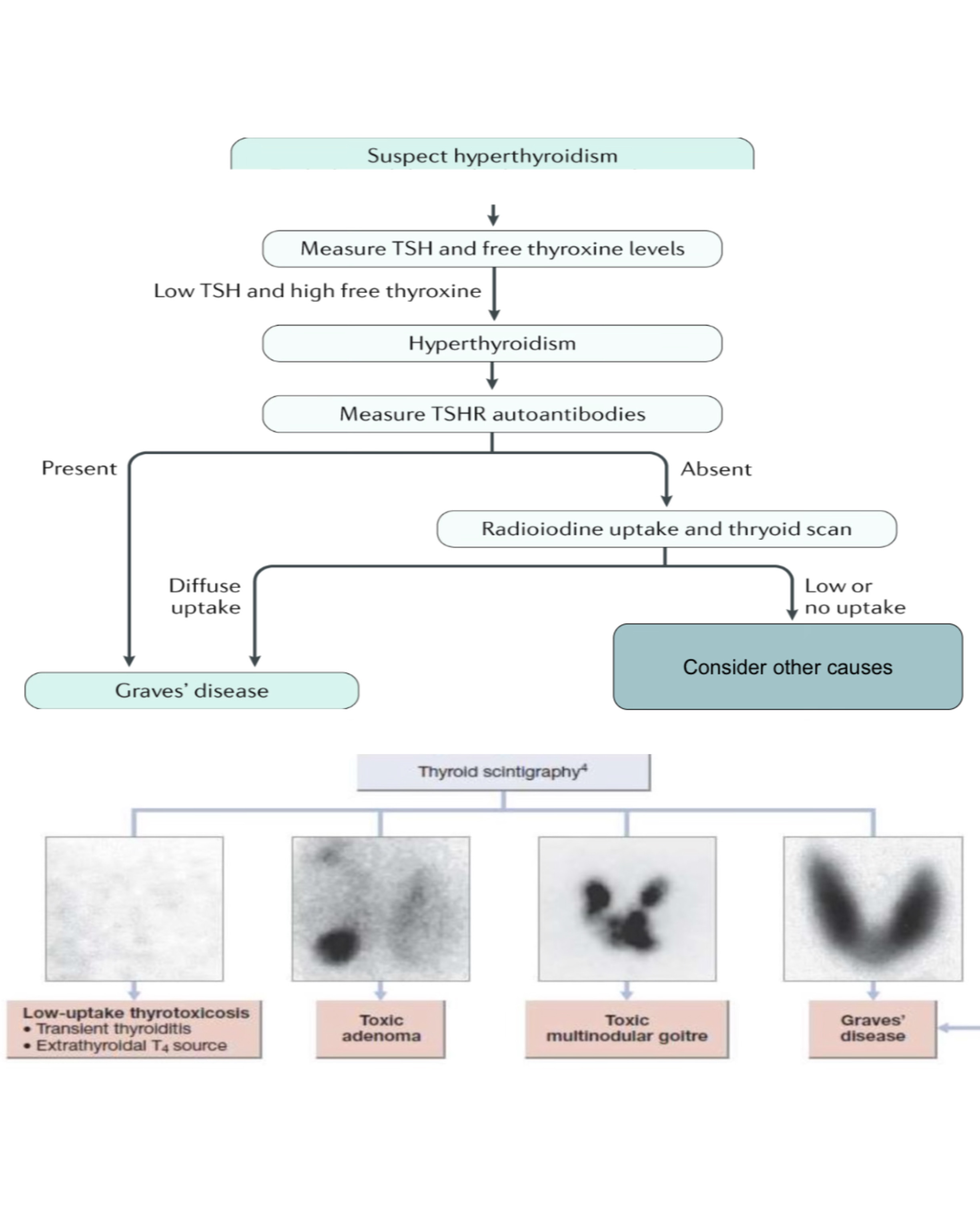
Hyperthyroidism investigation
Thyrotoxicosis Tx

Toxic adenoma

Subclinical thyrotoxicosis

Clinical features of thyroid storm (thyrotoxic crisis)

Cause of thyroid storm

Deferential diagnosis of thyroid storm
Septic shock
Upper GI bleeding
Sympathomimetic toxin ingestion
Ischemic liver disease
Pheochromocytoma
Thyroid storm treatment

Deferences between type 1,2 DM

What is the immune antigen for DM1
HLA-DR3 and HLA-DR4
Associated autoimmune with DM1
Primary adrenal insufficiency
Hashimoto thyroiditis
Vitiligo
Celiac disease
Pernicious anemia
Associated conditions with DM2
HTN
Dyslipidemia
Fatty liver
PCOS
DM should be suspended in patients with
Recurrent cellulitis
Candidiasis
Gangrene
Pneumonia
UTI
DM investigation

Microalbuminuria or proteinuria, in the absence of UTI , is an Important indicator of
diabetic nephropathy
(MODY) Maturity onset diabetes in the young

Metformin

When to stop metformin

SGL2I

GLP-1

Sulfonylureas

indications for insulin therapy in DM2
Antidiabetic treatment failed
Contraindications for Antidiabetic like end stage renal failure
Pregestational and gestational DM
Hyperglycaemic crisis
DKA characteristics
Hyperketonaemia (> 3)
Ketonuria (+2)
Hyperglycaemic (>200mg/dl)
Metabolic acidosis (HCl3<15) (ph <7.3) (H+ > 50 )
Sever DKA

DKA

Hyperglycaemic Hyperosmolar state HHS
Medical emergency in older DM2
Hypovolemia
Severe Hyperglycaemia > 600mg/dl
Hyperosolality > 320
Without ketonaemia or acidosis
Common precipitating factors for HHS
Infections
MI
Cerebrovascular events
Drugs ( glucocorticoids)
In management of HHS
Rapid shifts in osmolality avoided
Normal valve of osmolality is 280-296 DLOC if >340
IV fluid 0.9% NS 1 litre over 1 hour
( mortality are higher than DKA )
Common symptoms of hypoglycaemia
Sweating
Hunger
Anxiety
Palpitations
Tremor
Delirium
Drowsiness
Headache
Nausea
Severe hypoglycaemia management
If patient unconscious ( IV 200ml 10% dextrose over 15 minutes ) or ( IM glucagon 1mg)
Causes of Adrenal insufficiency

Adrenal insufficiency C.F and comparison

C.F of Adrenal insufficiency

Investigation Of adrenal insufficiency

Tx of primary and secondary adrenal insufficiency
glucocorticoids oral
Mineralocorticoids
DHEAS (50mg/day) given for some women with low libdo
Dose of corticosteroids must be increased in stress conditions to avoid adrenal crisis
Adrenal crisis signs and symptoms (Addisonian crisis)
Hypotension, shock
DLOC
Vomiting, Diarrhea
Severe abdominal pain
Adrenal crisis (Addisonian crisis)

Causes of hypothyroidism

Hashimoto thyroiditis
Most common cause of acquired hypothyroidism , most prevalent in women 30-50years , thyroid is firm not tender diffuse goiter
Always look for autoimmune conditions
Clinical features:
In early stage is asymptomatic then hyperthyroidism (irritable, heat , diarrhoea)
In late stage thyroid normal size or small fibrosis then hypothyroidism (cold, fatigue, constipation)
Why you need T3,T4 in follow up
Because TSH take several weeks to catch up
Confirming Hashimoto thyroiditis by
Serum antithyroid peroxidase and antithyroglobulin antibody
ECG findings in hypothyroidism
Sinus bradycardia with low voltage complexes
ST-segment and T-Wave abnormalities
Hypothyroidism Tx
Start dose of levothyroxine 50ug/day for 3 weeks
Then 100ug/day for 3 weeks
Maintenance dose 100-150ug/day
In patients with Hx of ischemic heart disease start low and go slow
dose adjustment in levothyroxine

Symptoms of hypothyroidism

Subclinical hypothyroidism

Myxedema coma clinic features
DLOC
Hypothermia
Myxedema
Hypoventilation ( hypercapnnia and hypoxia)
Hypotension ( possibly shock)
Bradycardia
Myxedema coma Causes

Myxedema coma Tx
