AORTIC DISORDERS
1/25
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
26 Terms
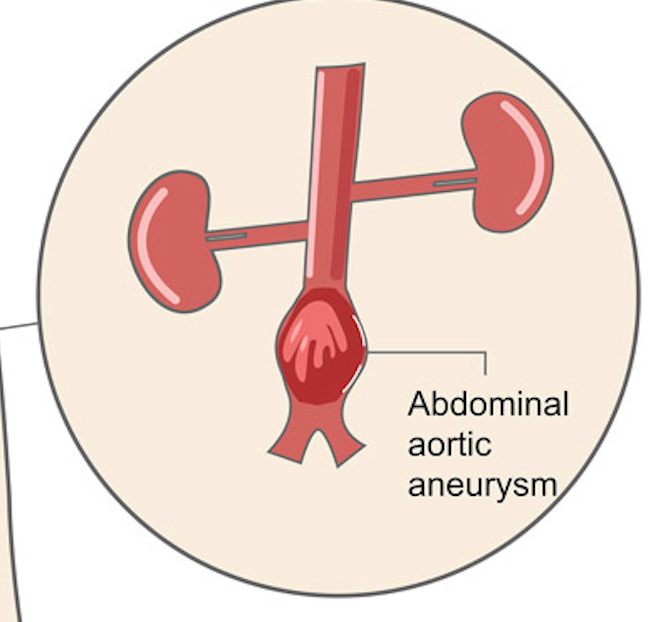
ABDOMINAL AORTIC ANEURYSM
• Localized dilation/outpouching ≥50% larger than normal
• Caused by weakening of the arterial wall
• Most occur below the renal arteries
• Risk of rupture ↑ with size (>6 cm = high risk)
AAA Symptomatic
• Abdominal/back/chest pain (tearing, stabbing)
• Pulsatile abdominal mass (classic!)
• “Blue toe syndrome” (embolization)
Abdominal Aortic Aneurysm Rupture
Sudden severe pain + hypotension + Tachycardia + ↓ urine output
EVAR (Endovascular Aneurysm Repair)
Minimally invasive
Insert graft via the femoral artery
Endoleak
asymptomatic complication following endovascular aneurysm repair (EVAR), where blood leaks back into the aneurysm sac, risking rupture
EVAR Post-Op
Graft patency (check pulses!)
Renal perfusion (urine output)
No heavy lifting for 6 weeks
Monitor pulses
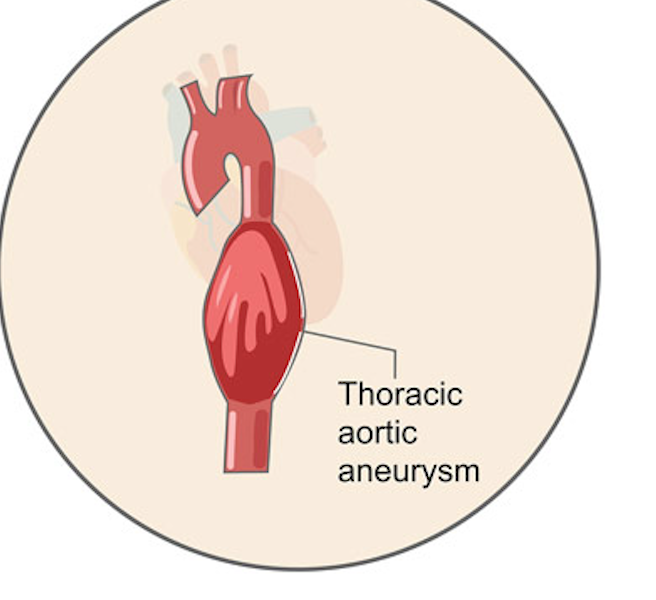
THORACIC AORTIC ANEURYSM
Deep chest pain radiating to the back
Can compress surrounding structures
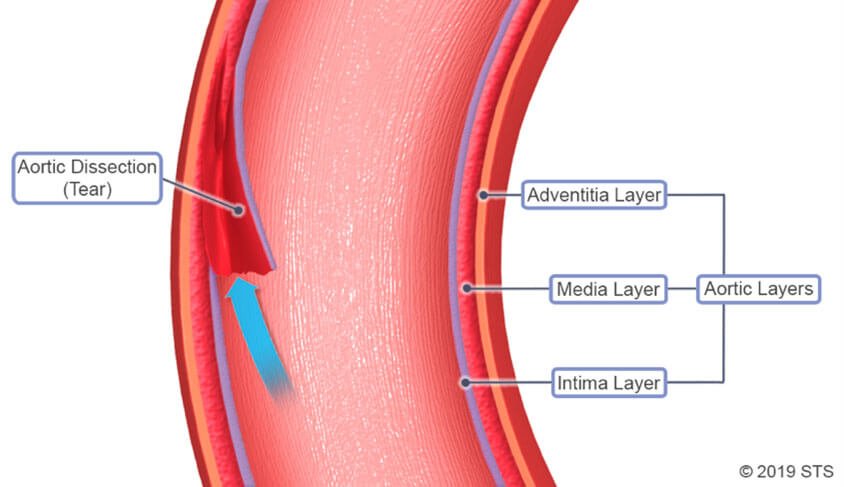
AORTIC DISSECTION
occurs when a tear in the inner layer (intima) of the aorta allows blood to surge into the middle layer (media), creating a false lumen that splits the aortic wall
• NOT an aneurysm
• Tear in intima → blood enters wall → false lumen
• Worsens with each heartbeat
Risk Factors AORTIC DISSECTION
• Chronic Hypertension (BIGGEST)
• Genetic disorders (Marfan, Ehlers-Danlos)
• Male gender
Type A AORTIC DISSECTION
EMERGENCY
Ascending aorta
Requires surgery
Type B AORTIC DISSECTION
Descending aorta
Often medical management
Clinical Manifestation AORTIC DISSECTION
• Sudden “tearing/ripping” pain
• Chest or back pain
• Unequal BP between arms
• Pulse deficits
• Neuro deficits (if arch involved)
Complications For AORTIC DISSECTION
Cardiac tamponade
Aortic rupture → death
Organ ischemia
Medical Management Type B AORTIC DISSECTION
↓ HR and BP (reduce shear stress)
Medications for AORTIC DISSECTION
Beta Blockers (FIRST LINE)
• ↓ HR → ↓ force on aorta
IV Antihypertensives (ex: Nitroprusside)
• Rapid BP control
Pain meds (opioids)
• ↓ sympathetic response
Nursing Interventions for AORTIC DISSECTION
Lower BP ASAP
Continuous BP + EKG monitoring
AORTIC DISSECTION Procedures
TEVAR (endovascular repair) Thoracic Endovascular Aortic Repair
A small incision is made in the groin, allowing a surgeon to guide a stent-graft through the femoral artery into the thoracic aorta to seal the damaged area, often using imaging to guide placement.
AAA
• Often silent
• Pulsatile mass
• Rupture = shock
TAA
• Chest/back pain
• Compression symptoms
AORTIC DISSECTION
• Sudden tearing pain
• Unequal BP
• Type A = surgery NOW
AAA Rupture
Sudden hypotension + known AAA
Saccular Aneurysm
These are round, pouch-like, or "berry-shaped" outpouchings that develop at arterial junctions in the brain,
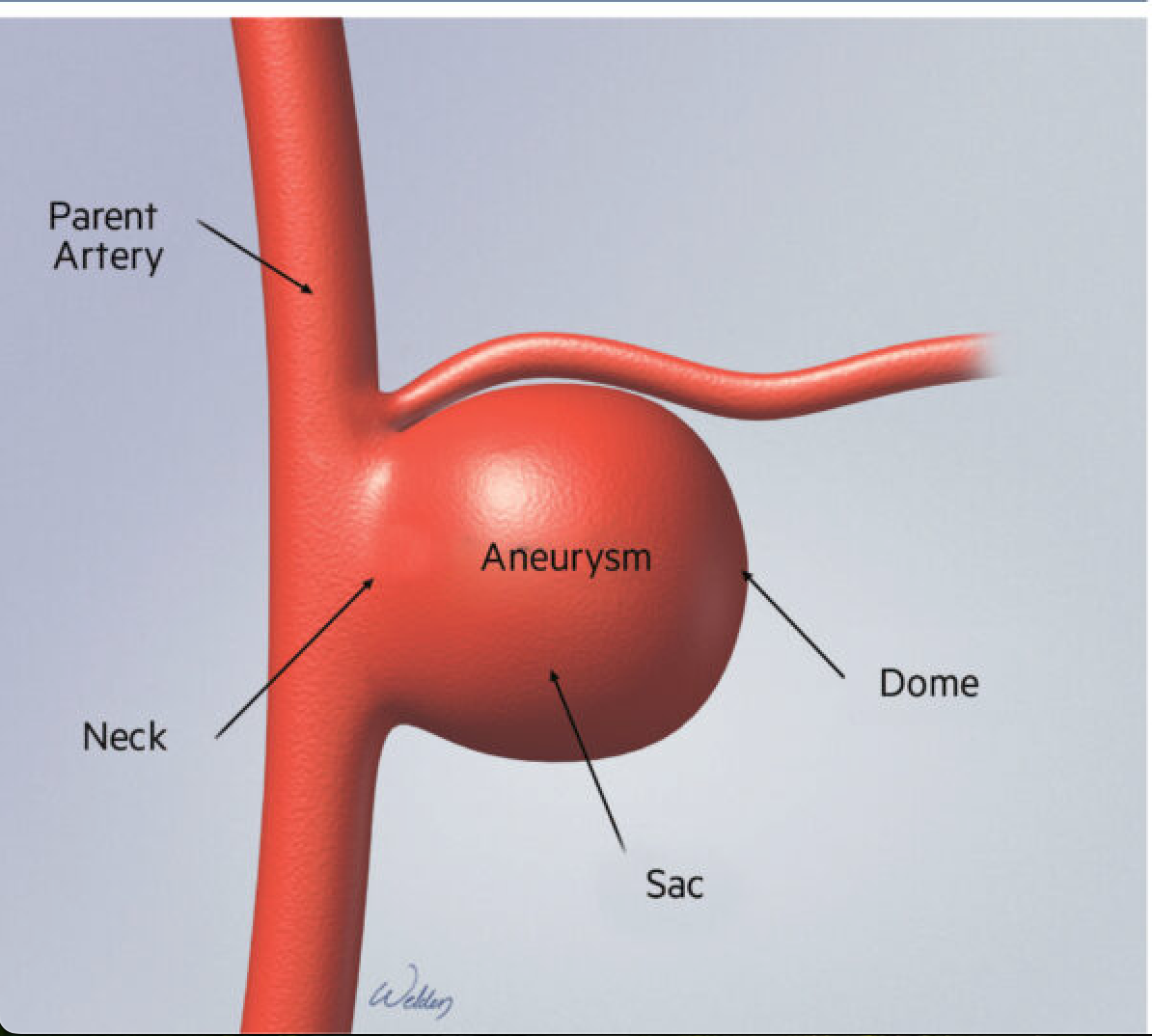
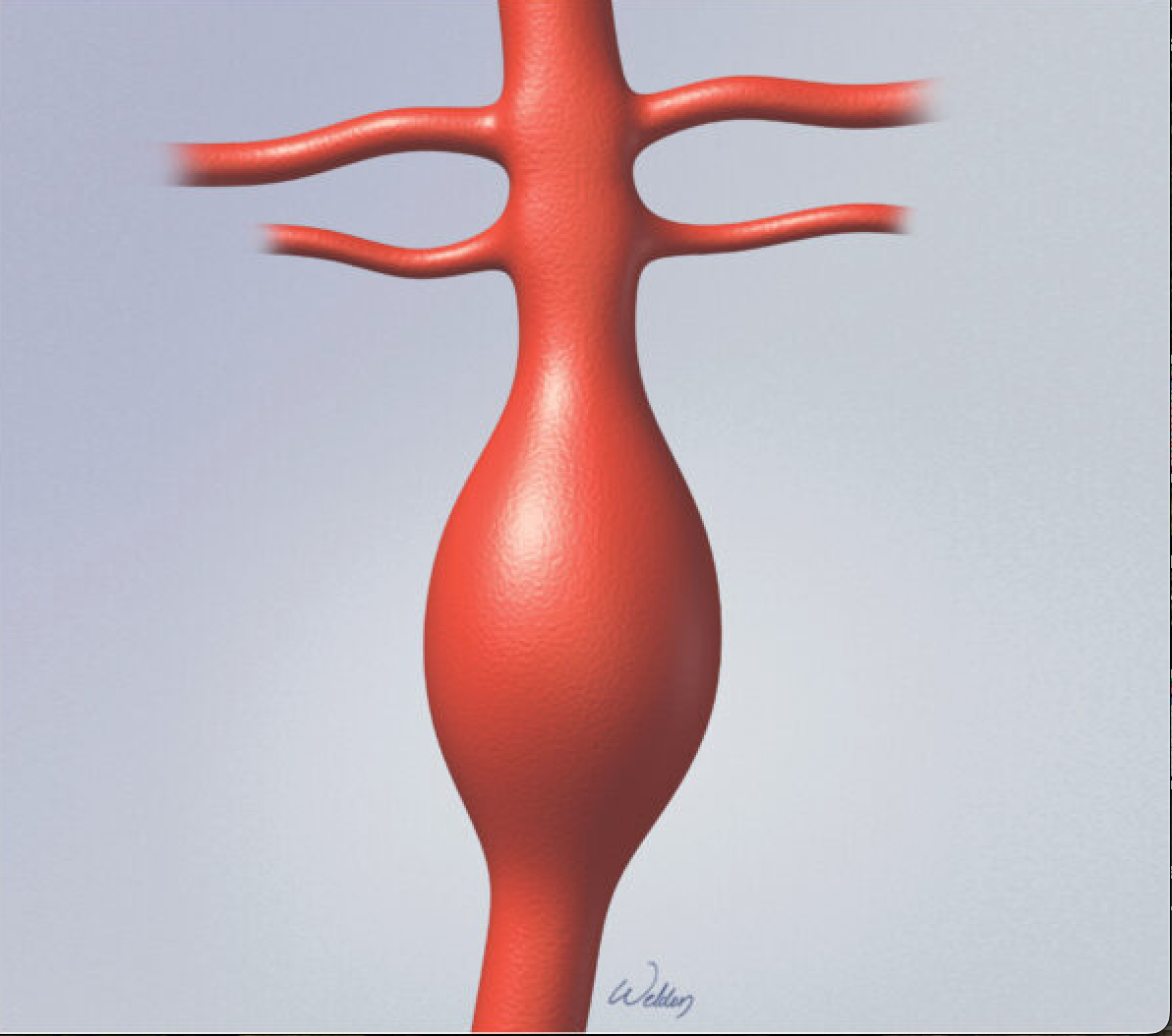
fusiform aneurysm
a type of blood vessel dilation where the entire circumference of the artery wall stretches and enlarges, forming a spindle-shaped ballooning
commonly occur in the aorta or cerebral arteries
AAA <5.5
Conservative management
Open Aneurysm Repair
Large abdominal incision / synthetic graft to the aorta above and below the aneurysm
higher risk option
aortic cross-clamping proximal and distal to an aneurysm
Aortic Dissection Onset
Acue - first 14 days
Subacute - 14-90 days
Chronic - > 90 dayes