Reproductive anatomy + pathology
1/17
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
18 Terms
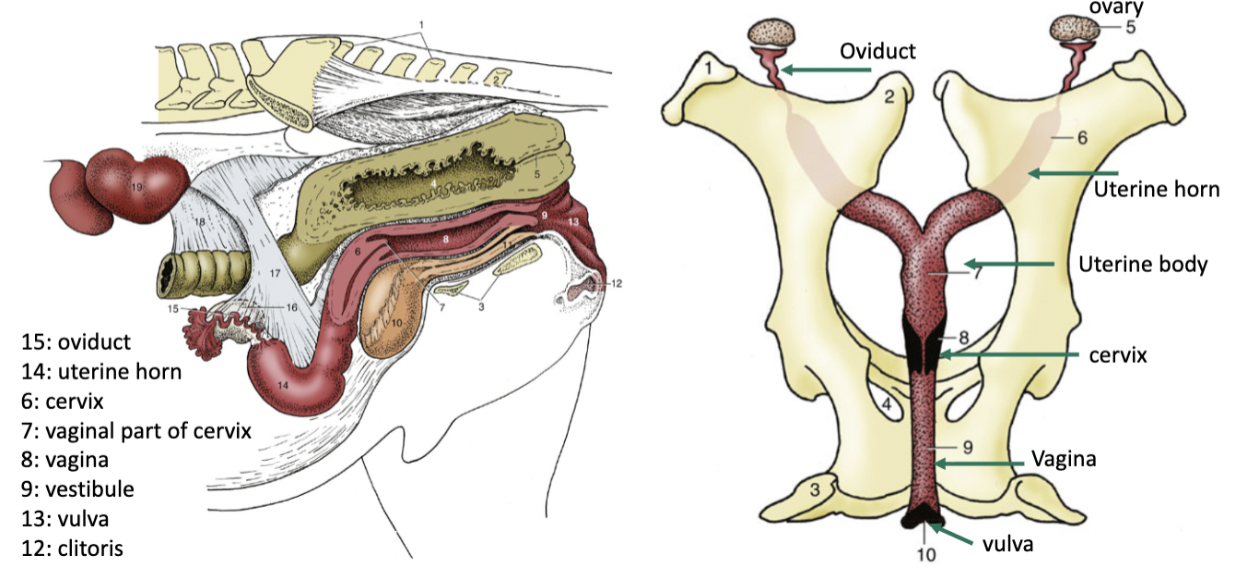
Equine Female reproductive tract
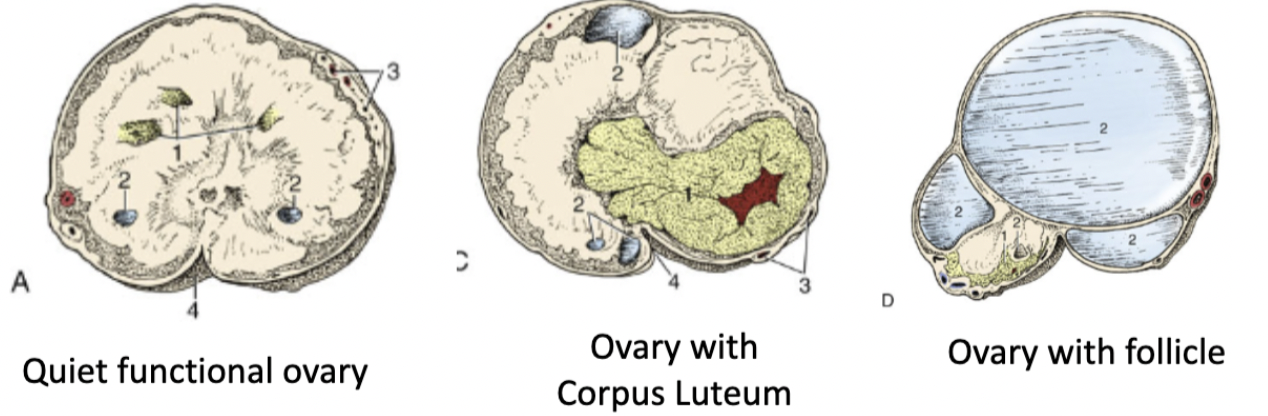
3 ovary stages
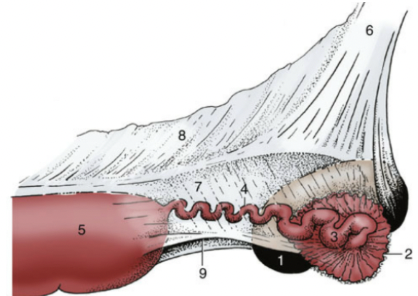
Oviduct
Infundibulum: made up of many fimbriae (little fingers) that surround the ovary, collecting the ovulated egg
Isthmus (4): “tortuous”, narrow tube that the ovulated egg travels through to get to the uterus
Where fertilization occurs (egg + sperm)
Junction of the isthmus and uterus only allows fertilized eggs to enter the uterus (5)
recognition of pregnancy
Fertilized egg makes it to the uterus ~6 days after fertilization
The conceptus is very mobile, and we believe the movement and frequent contact with the endometrium (inner lining of the uterus) aids in Maternal Recognition of Pregnancy
Prevents Corpus Luteum from regressing on the ovary, which maintains pregnancy
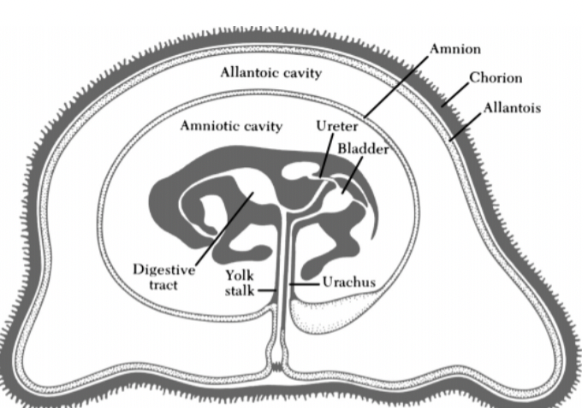
Placentation
The equine conceptus is highly unusual in that it does not form a blood connection with the mare until around 40 days of pregnancy, & takes until day ~150 to complete
Placental attachment to the uterine wall is
Epitheliochorial: The chorion portion of the fetal membranes is in contact with the mare’s uterine lining
Diffuse: The chorion has contact with the uterine lining all over, not only in specific locations
3 membranes: amnion, allantois, chorion
Gestation
Pregnancy is diagnosed either by hand via rectal palpation or by ultrasound
By hand – 25-30 days of pregnancy
Ultrasound – 11-14 days of pregnancy, fetal heartbeat by day 28
Mares are pregnant for 335-340 days
Range from 300-385
Can be longer if the mare has a low plane of nutrition, in cooler weather, and if carrying a mule as opposed to a foal
Parturition
Act of giving birth: “Foaling”
Signs of foaling include:
Udder distension: 2-6 weeks prior
Relaxation of muscles & ligaments around the pelvis: 7-10 days prior
“Waxing”: 2-4 days prior
Separation from the herd: in the hours prior
stages of parturition (3)
Abdominal discomfort, restlessness, uterine contractions
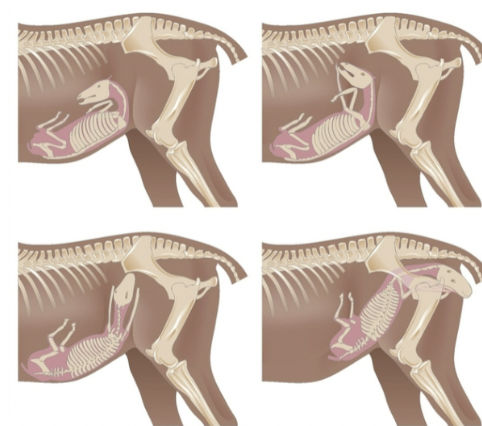
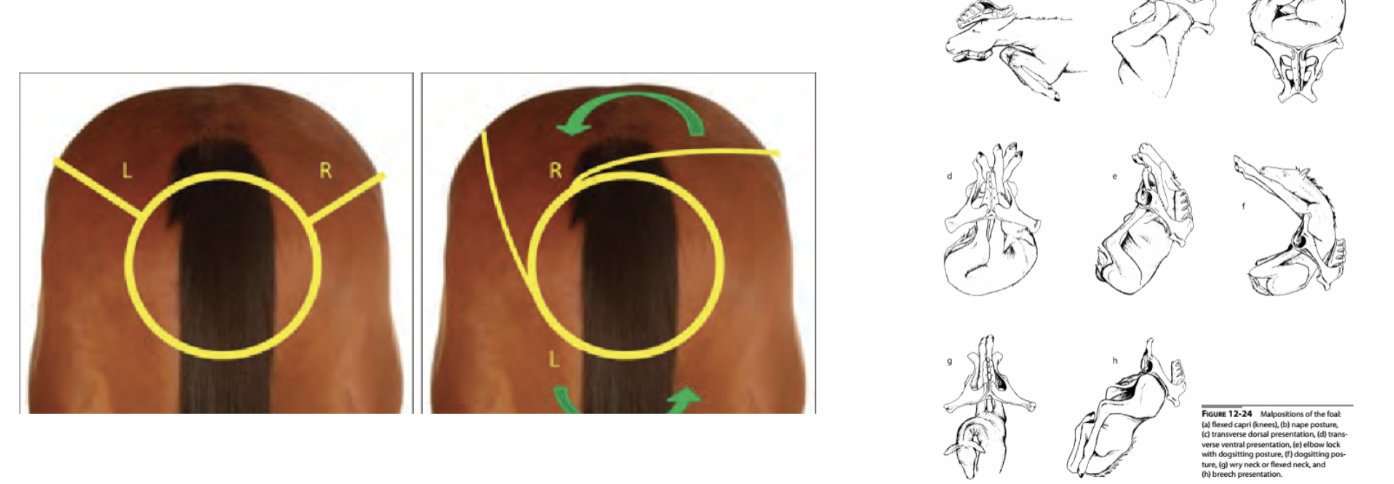
Fetal positioning
Begins with fetal membrane rupture & release of amniotic fluid – “water breaking”
Abdominal contractions, birth of foal
Typically 15-30 minutes
Amniotic membrane should break when born
Passing of fetal membranes
Within 3 hours
Placentitis
Vaginal discharge & premature “bagging up”
Ascending – infectious organisms travel up the repro tract
Poor vulvar conformation
Hematogenous – where bacteria circulate through the bloodstream
Placenta can be affected diffusely (all over) or localized infection
Can lead to detaching of the placenta or can lead to issues at parturition & can be difficult to break
Check routinely throughout pregnancy via ultrasound
Hippomanes
Amorphous pieces of allantoic material that is often delivered along with the fetus
Form like an enterolith – fluid and particulates collect around a central nidus
Mostly comprised of mucoproteins and calcium phosphate
Are typically beige-brown-green in color, firm, and up to several centimeters in diameter
Not pathologic
Twins
Terminate one (or both) if <35 days
Pinch
Issues with twins
Rarely both born full term, & alive
Likely to have retained membranes
Likely to have a dystocia
Premature Chorioallantois Separation
Red Bag
Outer fetal membranes (chorion + allantois) separate from the uterine lining before the amnion ruptures
Can quickly result in the foal not getting enough oxygen & dying via suffocation
True emergency
Caused by placentitis, twins, fescue toxicity, or for no reason at all
Dystocia
Foaling problem that does not allow the mare to give birth on her own
Mare causes vs fetal causes
Serious problem, often fatal for the mare &/or for the foal
Must consider cleanliness as well as gentleness when assisting a mare
The vulva, vagina, and uterus can be easily traumatized
Most should be addressed by a veterinarian or an experienced caretaker
Mare + Foal causes of dystocia
Mare causes
Uterine atony – failure of the uterine muscles to contract
Uterine torsion – uterus that has twisted on its axis, cranial or caudal to the cervix
Foal causes
Malposition
Fetal malformation
Addressing a Dystocia in a Standing Mare
Clean the external vulva and surrounding tissue well with iodine and warm water
Cleanliness is essential to prevent infection of the mare’s reproductive tract
There is no such thing as too much lubrication!
General rule is that if traction (pulling) requires more strength than that of two strong men, an alternative method should be considered
Often requires the use of obstetrical chains to aid in grip and traction
Addressing Dystocia: secondary options
Controlled Vaginal Delivery
Mare must be anesthetized
Hoist the mare’s hindquarters to push the GI tract cranially
Cesarean Section
Delivery of the foal by an abdominal and uterine incision
Fetotomy
When cesarean section is not an option
Fetus is cut into manageable pieces within the uterus, to be delivered vaginally with assistance
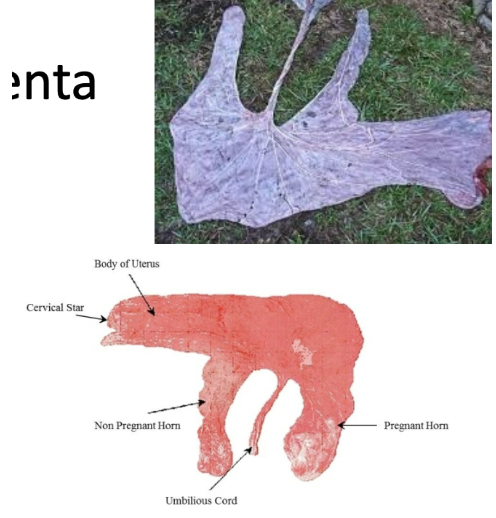
Examining placenta
Must examine the fetal membranes after every delivery
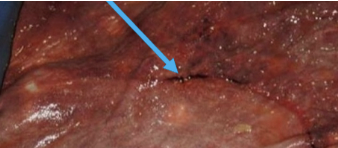
Normal birth: fetal membranes ruptured by the foal in “cervical star” – a weakened area of the chorioallantois
Should appear as the letter “F”, representing the two uterine horns and the uterine body
Retained placenta
Any missing pieces that have remained in the uterus, or if the entirety of the fetal membranes have not passed within 3 hours, the membranes are considered to be retained
Can be treated with oxytocin administration to promote uterine contractions in early cases
Must be treated with antibiotics and anti-inflammatories in cases >8 hours
Predisposes mares to laminitis