Urinary System
1/112
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
113 Terms
components of the urinary system
kidneys
ureters
bladder
urethra
associated nerves/blood vessels
functions of urinary system
regulate blood volume, blood pressure, pH, and concentration of electrolytes
reabsorb glucose and excreting wastes
release hormones (renin and erythropoitin)
activate vitamin D
location of the kidneys (+ which is lower)
between peritoneum and posterior wall of abdomen in retroperitoneal space
right is slightly lower than left due to position of the liver
cortex of kidney (+ function)
outer layer that filtrates to form urine
medulla of kidney (+ function)
inner layer that collects and excretes urine
renal pyramids (+ function)
8-18 cone-shaped subdivisions that contain kidney’s secreting apparatus and tubules
renal columns (+ function)
lines of blood vessels and fibrous material between pyramids
anchors cortex
renal papilla
location where renal pyramids empty urine into minor and major calyces
minor calyx
receive urine from each renal pyramid
major calyx
receive urine from 2-4 minor calyces
When does filtrate become urine?
When it enters calyces because no further reabsorption occurs
renal pelvis
a large cavity that receives urine from major and minor calyces and drains into ureters
renal blood flow
renal artery and vein pass into parenchyma at hilum
How does the renal artery branch to become renal vein?
Renal artery → (extensive branching) afferent arteriole → glomerular capillaries → efferent arteriole → peritubular capillaries → (extensive branching) renal vein
nephron
functional unit of kidney composed of blood vessels and tubules that collect filtrate
How many nephrons per kidney?
~ 1 million
filtration in nephron (where it occurs, describe)
mostly in renal corpuscle
most solutes of the right size (small enough) enters through the glomerular capillaries into the nephron
reabsorption in nephron (where it occurs, describe)
mostly proximal convoluted tubule (PCT)
solutes are reabsorbed into the blood that were taken out that the body still needs
secretion in nephron (where it occurs, describe)
mostly distal convoluted tubule (DCT)
unwanted stuff in blood is taken into nephron and added to filtrate
Where does H2O absorption happen?
descending loop of Henle and PCT
visceral layer of Bowman’s capsule
podocytes with pedicels that wrap around the single layer of cells of glomerular capillaries and form inner wall of capsule
podocyte
modified simple squamous epithelial cells with pedicels
parietal layer of Bowman’s capsule
simple squamous outer wall
filtration membrane
fenestrations formed by the two layers of Bowman’s capsule
Types of Nephrons
cortical
juxtamedullary
What determines the amount of water absorbed out of loop of Henle in a nephron?
length of loop of Henle and the osmotic force as you go deeper into the medulla
cortical nephrons
loop of Henle only goes into medulla a little and, since the loop is shorter, cortical nephrons can only produce dilute urine (most common nephron)
juxtamedullary nephron
loop goes deeper into medulla and, since loop is longer, lots of water is able to be pulled out, making it capable of producing concentrated urine
renal corpuscle
glomerulus and Bowman’s capsule
Which nephrons can you find a thin and thick limb of the loop of Henle in?
juxtamedullary nephrons
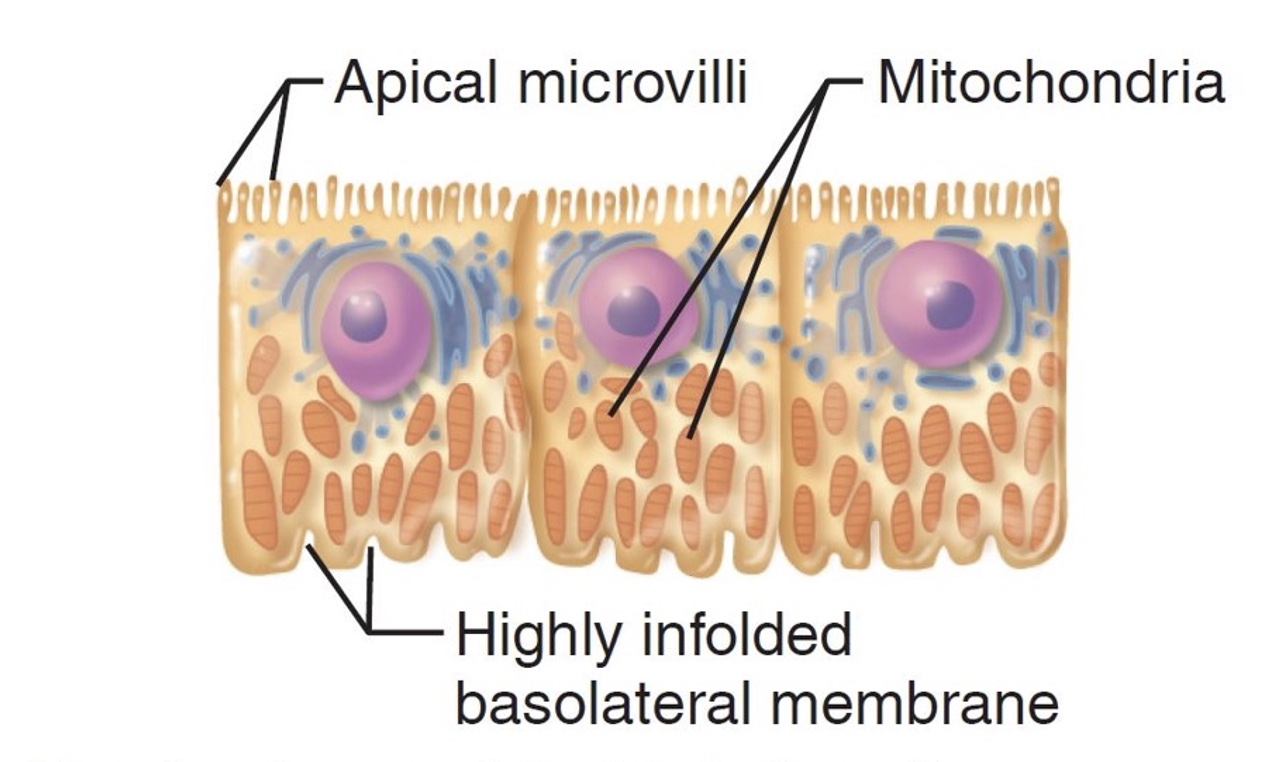
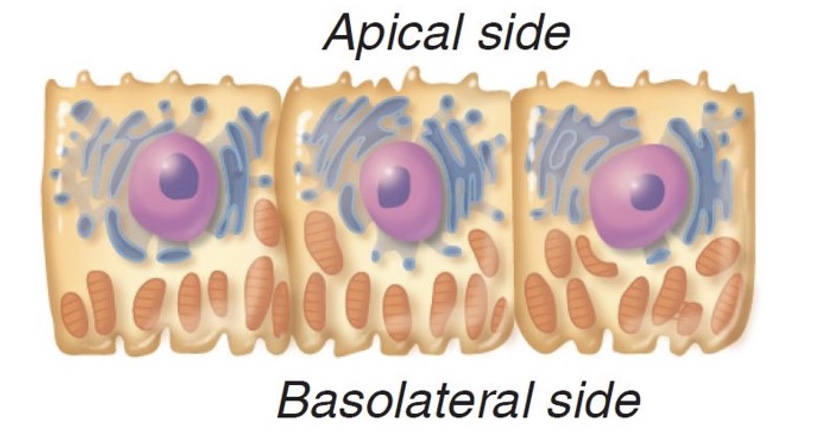
components of proximal convoluted tubule specific to it (+ type of epithelium)
has mitochondria and microvilli for reabsorption because active transport requires lots of ATP and the microvilli increase surface area and rate of reabsorption back into blood
simple cuboidal epithelium
components of distal convoluted tubule specific to it (+ type of epithelium)
sparse microvilli
simple cuboidal epithelium
components of descending nephron loop specific to it (+ type of epithelium)
also called the “thin segment” in juxtamedullary nephrons because it has high water permability
simple squamous epithelium
components of ascending nephron loop specific to it (+ type of epithelium)
also called the “thick segment” in juxtamedullary nephrons but it remains thin on some nephrons
cuboidal or short columnar epithelium
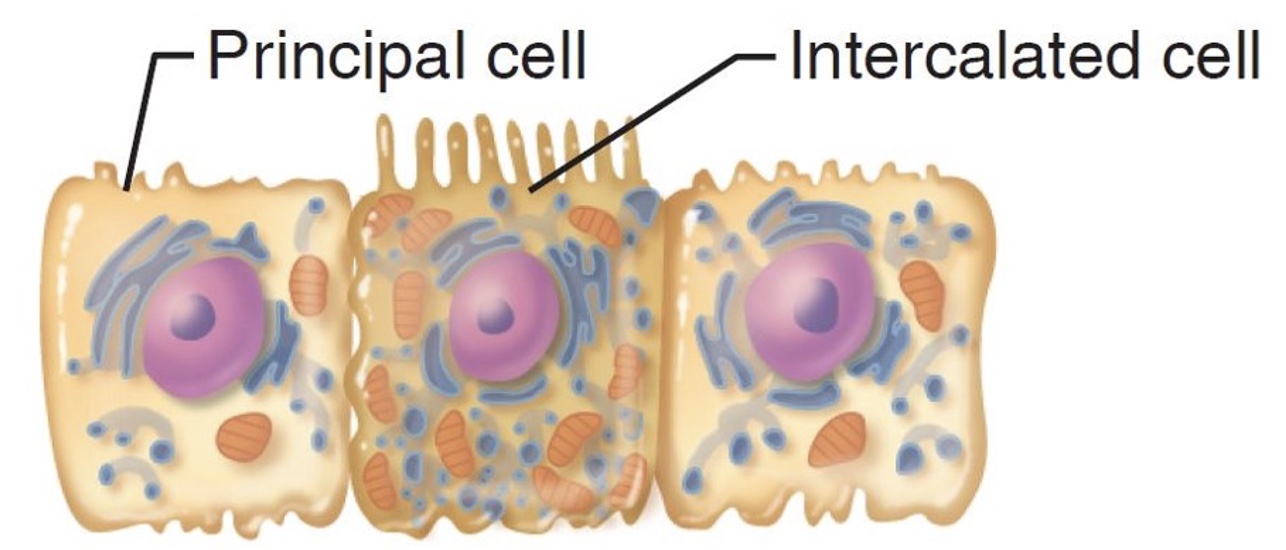
cells of the collecting duct
principal cells
intercalated cells
principal cells of collecting duct (function, hormones that affect it, appearance)
function: maintain water and Na+ balance
are affected by ADH and aldosterone
have sparse short microvilli
intercalated discs of collecting duct (function, type of epithelium, two cell types)
function: maintain acid-base balance in blood
cuboidal cells with abundant microvilli
A and B cell types
Where are these cells located?
proximal convoluted tubule

Where are these cells located?
descending loop of Henle
Where are these cells located?
distal convoluted tubule
Where are these cells located?
collecting duct
peritubular capillaries (location, function)
surround cortical nephrons
pick up water reabsorbed from filtrate and return it to blood
vasa recta (+ type of nephrons, function)
long vessels that run parallel to long nephron loops
in juxtamedullary nephrons
involved in formation of concentrated urine and picks up water reabsorbed from filtrate and returns it to blood
juxtaglomerular complex (+ function, type of cells)
made from modified portions of the most distal part of ascending limb of loop of Henle and the afferent arteriole
function: regulate rate of filtrate formation and blood pressure
types of cells: macula densa and granular cells
macula densa cells of juxtaglomerular complex (+ function)
group of tall, closely packed cells of ascending loop of Henle
act as chemoreceptors that monitor NaCl content of filtrate entering DCT
granular cells of juxtaglomerular complex (+ function)
large, smooth muscle cells surrounding afferent arterioles
act as mechanoreceptors that monitor BP
secretory granules contain renin (enzyme)
outward pressure (+ function)
hydrostatic pressure in glomerular capillaries
promote filtration
inward pressures (+ functions)
hydrostatic pressure in the capsular space
colloid osmotic pressure in glomerular capillaries
inhibit filtration
hydrostatic pressure in glomerular capillaries (+ value)
the force pushing water and small solutes out of capillaries
HPgc = 55 mm Hg
Hydrostatic pressure in the capsular space (+ value)
due to fluid pressure of filtrate in confined space with narrow outlet
Hpcs = 15 mm Hg
Colloid osmotic pressure in glomerular capillaries (+ value)
“pull” of plasma proteins
OPgc = 30 mm Hg
Net filtration pressure (+ equation, what it controls)
outward pressure - inward pressure
55 mm Hg (outward) - 45 mm Hg (inward) = NFP of 10 mm Hg
controls glomerular filtration rate
glomerular filtration rate
volume of filtrate formed by both kidneys per minute (mL/min)
myogenic mechanism
smooth muscle contracts when stretched to help maintain normal glomerular filtration rate despite regular fluctuations in BP
How does the myogenic mechanism adapt to a rise in BP?
stretches smooth muscle of afferent arteriole, causing it to contract and constrict blood flow into glomerulus (protecting it from high BP)
How does the myogenic mechanism adapt to a fall in BP?
causes afferent arteriole to relax and vasodilate
How does tubuloglomerular feedback mechanism adapt to rise in glomerular filtration rate?
increased flow causes less time to reabsorb NaCl
macula densa cells respond to elevated NaCl levels by releasing vasoconstrictor chemicals
constriction of afferent arterioles lowers GFR back to normal, allowing adequate time for NaCl reabsorption
How does tubuloglomerular feedback mechanism adapt to a fall in glomerular filtration rate?
decreased flow causes too much time to reabsorb NaCl
macula densa cells respond to low NaCl levels by releasing vasodilator chemicals
dilation of afferent arteriole raises GFR back to normal, allowing adequate time for NaCl reabsorption
Sympathetic nervous system controls at rest vs. in ECF crisis
at rest: SNS activity is low, afferent arterioles dilated
in ECF crisis: SNS fibers release lots of norepinephrine, causing vasoconstriction throughout body
vasoconstriction causes GFR to reduce urine output, increase blood volume, and increase blood pressure
tubular reabsorption (+ types)
quickly reclaims most tubular contents and returns them to blood
transcellular
paracellular
transcellular tubular reabsorption
substances move directly through tubule cell via active transport, facilitated transport, diffusion, etc.
paracellular tubular reabsorption
substances pass between tubular cells
obligatory water reabsorption
occurs in the PCT and descending loop of Henle where aquaporins are already present and water moves based on osmotic force (water follows ions)
facultative water reabsorption
occurs in collecting ducts where concentration of aquaporins depends on ADH
as ADH increases, aquaporins increase (more water reabsorbed)
transport maximum
reflects the number of transport proteins available to move that substance
when transporters are saturated with their solute, the rest is excreted in urine
hormones involved with the urinary system
aldosterone
ADH
RAAS
ANP
aldosterone functions
causes Na+ to be reabsorbed into blood by creating more Na+ channels in collecting duct
water follows Na+ out, increasing blood volume and BP
causes K+ to be secreted back into filtrate
ADH functions
facilitated H2O reabsorption
direct vasoconstriction
RAAS functions
angiotensin II is direct vasoconstrictor
aldosterone causes reabsorption of Na+ (and therefore H2O) to increase BP
ANP (atrial natriuretic peptide) functions
direct vasocontriction
secretion of Na+ and H2O into urine to decrease BP
tubular secretions
follows same steps as reabsorption but in reverse
selected substances such as K+, H+, NH4+, and creatinine from nearby peritubular capillaries are transported from IF into filtrate
types of countercurrent mechanisms
countercurrent multiplier
countercurrent exchanger
countercurrent multiplier (+ what it depends on)
interaction of filtrate flow in ascending and descending limbs of long nephron loop
depends on:
flow in opposite directions through adjacent parallel limbs
descending limb is permeable to water but not solutes
ascending limb is impermeable to water but pumps out solutes
countercurrent exchanger
blood flow in ascending/descending limbs of vasa recta provides passage exchange with IF
What is the function of both types of countercurrent mechanisms?
produce and maintain medullary osmotic gradient (300 mOsm in cortex and 1200 mOsm at tip of medulla)
How does the vasa recta maintain the medullary osmotic gradient?
by preventing rapid removal of solutes from IF and removing reabsorbed water
What is the osmotic concentration in the cortex vs the inner medulla?
cortex: 300 mOsm
medulla: 1200 mOsm
How does urea contribute to the medullary osmotic gradient?
enters filtrate in ascending limb of loop of Henle
cortical collecting ducts reabsorb water, concentrating urea left behind
in deep medulla, some of the (now more concentrated) urea leaves the collecting ducts and either enters the IF or is excreted in urine
origin or urea
NH3 is toxic to humans so the liver converts it to urea
What is the purpose of a urinalysis
used to help diagnose diseases and detect the presence of illegal substances in the body
What is used to analyze renal function?
urinalysis and blood test
composition of urine
95% water and 5% solutes
types of nitrogenous wastes in urine
urea, uric acid, creatinine
uric acid
nucleic acid metabolism
creatinine
creatine phosphate metabolism
What are the normal solutes in urine?
Na+, K+, PO4³-, SO4²-, Ca²+, Mg²+, HCO3^-
What does glucose in urine indicate?
diabetes mellitus
What does high levels of proteins in the urine indicate?
nonpathological: pregnancy or excessive exertion
pathological: hypertension, heart failure, renal disease
What does high levels of ketone bodies in the urine indicate?
starvation or uncontrolled diabetes mellitus
What does high levels of hemoglobin in the urine indicate?
transfusion reaction, hemolytic anemia, severe burns
What does high levels of bile pigments in the urine indicate?
liver disease or obstruction of bile duct from liver to gallbladder
What does high levels of erythrocytes in the urine indicate?
bleeding urinary tract due to trauma, kidney stones, infection, cancer
What does high levels of leukocytes in the urine indicate?
UTI
normal color of urine
clear or pale to deep yellow
abnormal colors of urine and potential causes
pink, brown, smoky
may result from certain foods or meds or presence of blood or bile pigments in urine
odor of urine
slightly aromatic when fresh (depends on diet) and develops an ammonia scent upon standing as bacteria metabolizes urea
What can cause abnormal odor of urine?
drugs, vegetables, disease
pH of urine (+ what can change it)
slightly acidic (~6)
acidic diet: lots of protein and whole wheat lowers the pH
alkaline diet: vegetarian diet can raise the pH
ureter (function, length, how does it perform its function)
transports urine from kidneys to bladder
25 cm in length
uses peristaltic waves, gravity, and hydrostatic pressure
How does the urine not back-flow from the bladder to the ureter?
as bladder pressure increases, distal ends of ureters close