anatomical landmarks #1
1/44
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
45 Terms
what are anatomical landmarks that are of prosthodontic importance?
landmarks that may be anatomical points, lines or planes related to the maxilla and the mandible extraorally and intraorally
why are landmarks of completely edentulous patients important in complete denture construction?
they are used as natural guidelines during denture construction, helping achieve aesthetic and biochemical principals
what are the extraoral landmarks?
lips
philtrum
nasolabial angle
nasolabial sulcus
mental protuberance
mentolabial sulcus
modiolus
inter-pupillary line
ala-tragus line (campers line)
outer canthus-tragus line (frankfort line)
angle of the mouth
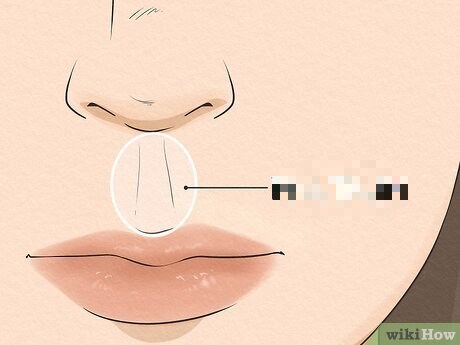
the following picture is what extraoral landmark?
the philtrum, a diamond shaped outline between the center of the upper lip and the base of the nose
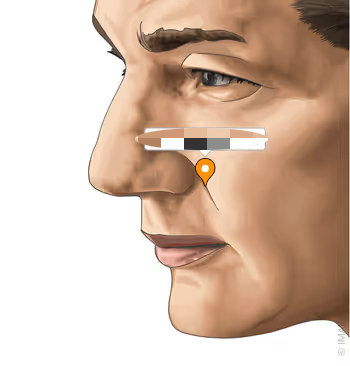
the following picture is what extraoral landmark?
the nasolabial angle, which is the intersection of the base of the lip and the upper lip
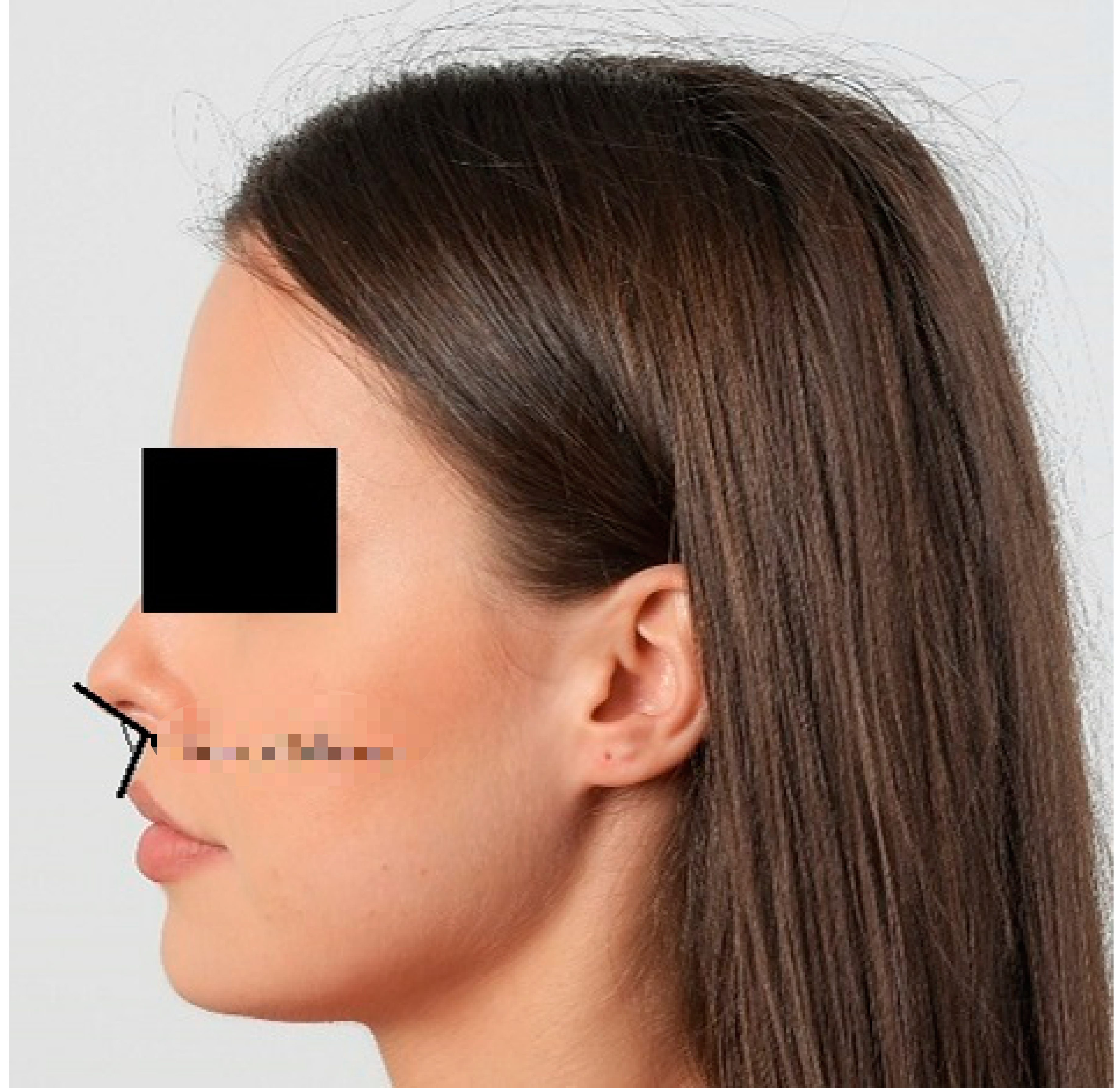
the following picture is what extraoral landmark?
the nasolabial sulcus, which is a depression that extends from the ala of the nose until the corner of the mouth in a downward and lateral direction to it
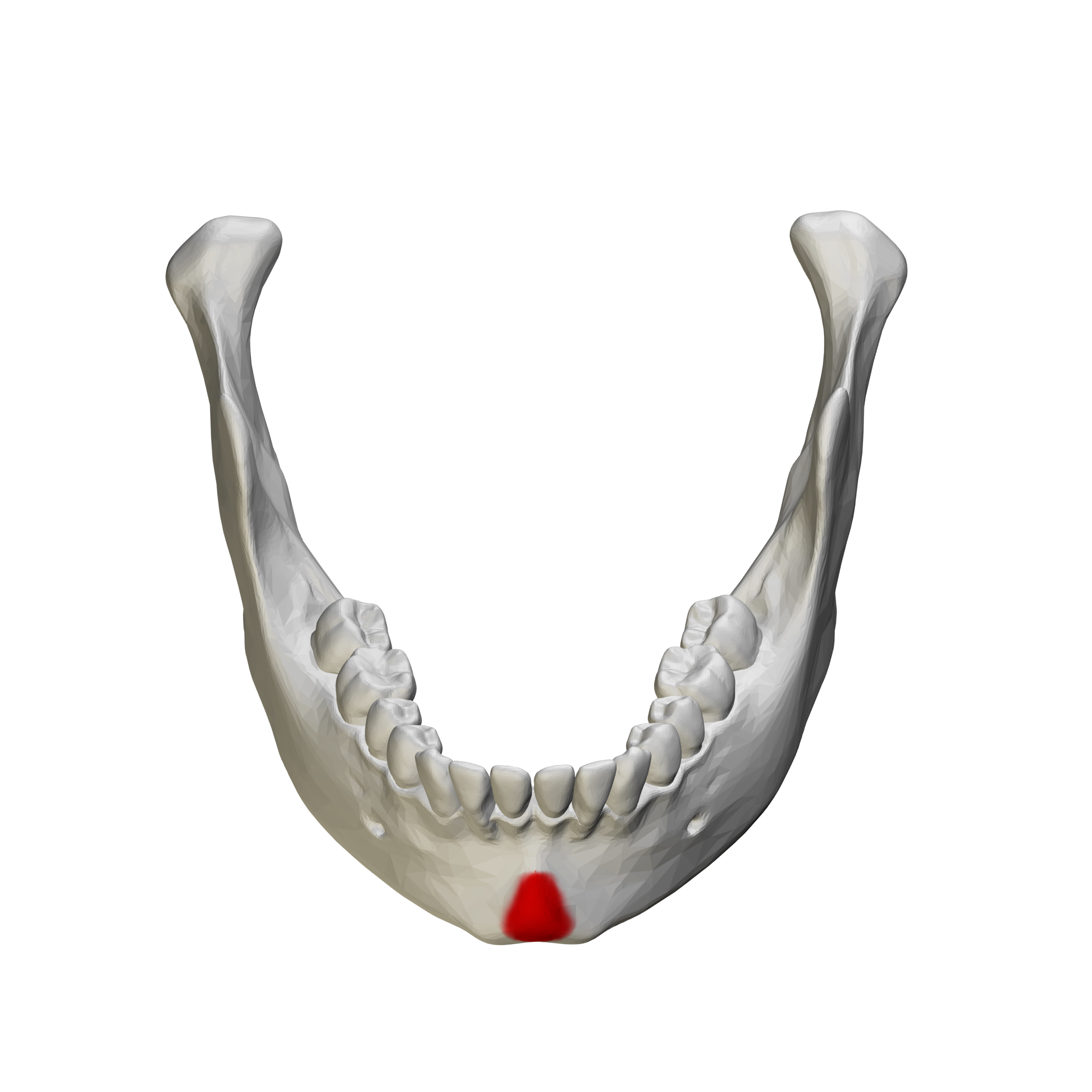
the following picture is what extraoral landmark?
the mental protuberance, which is a triangular prominence occurring in the midline near the inferior border of the mandible that forms the base of the chin
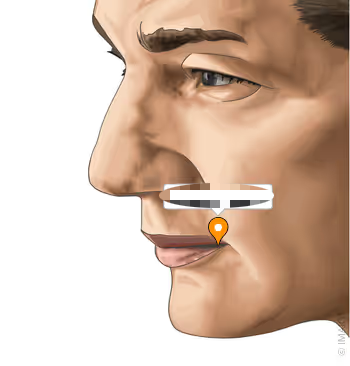
the following picture is what extraoral landmark?
the mento-labial sulcus, which is a depression that runs horizontally between the lower lip and chin
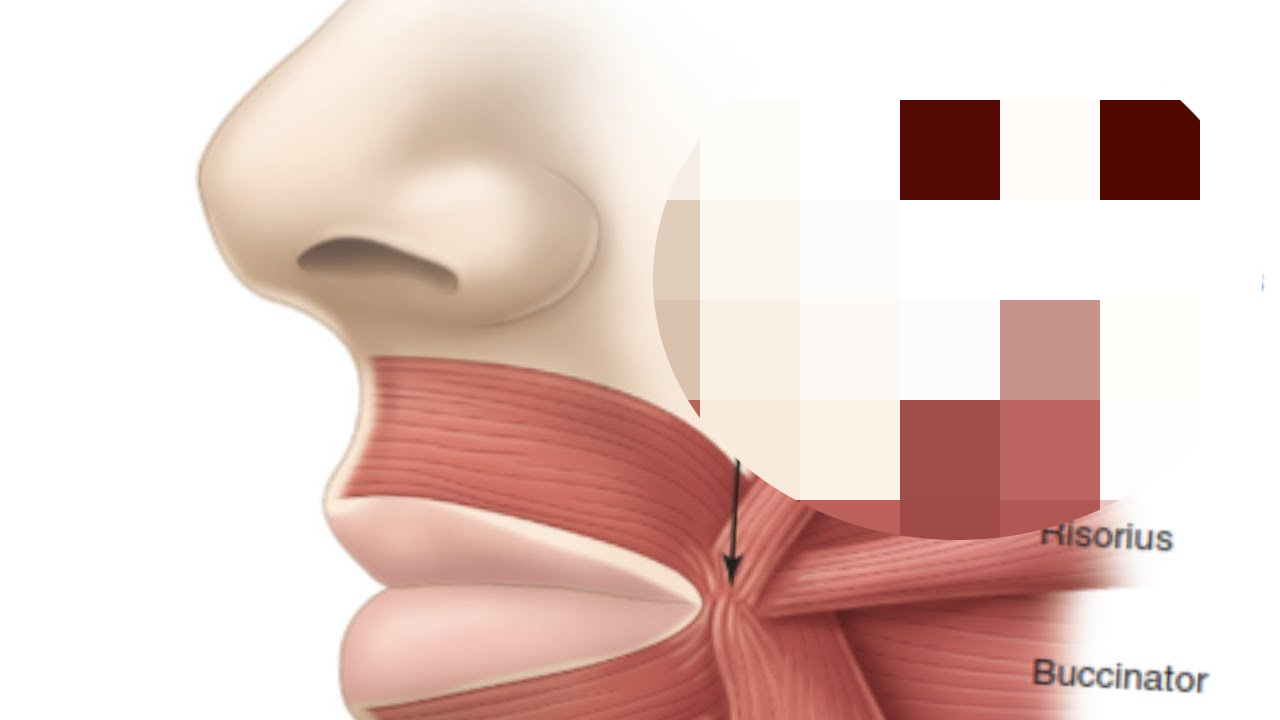
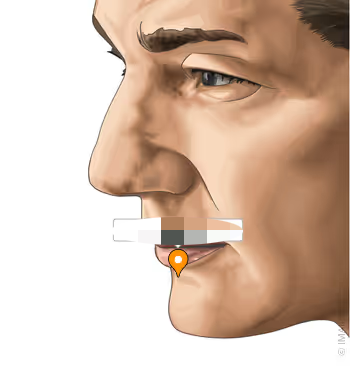
the following picture is what extraoral landmark?
the modiolus, which is a collection of facial muscle insertions located near the buccinator muscles, or near the corners of the mouth. only prominent / seen properly in edentulous patients
what is the inter-pupillary line?
an imaginary anatomical reference line drawn between the centers of the two pupils when the patient is looking straight ahead and is used in denture construction to help orient the occlusal plane horizontally and ensure facial symmetry and esthetics.
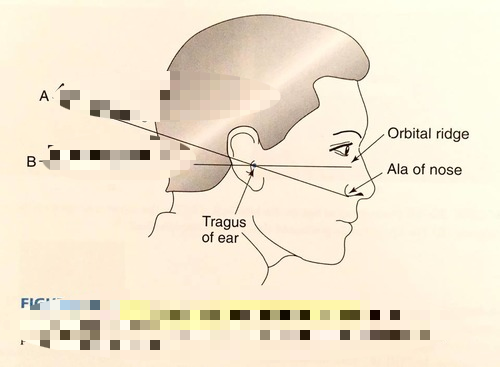
line a is what extraoral landmark?
the ala-tragus, or Camper’s, line. it is an anatomical reference line that extends from the inferior border of the ala of the nose to the superior border of the tragus of the ear
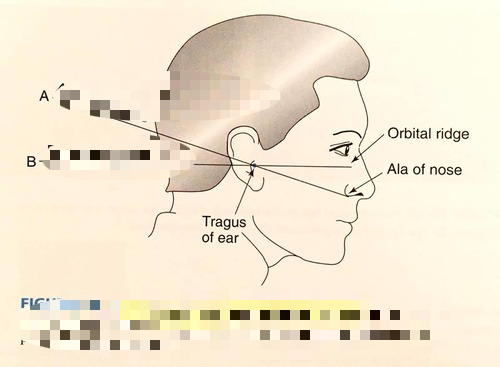
line b is what extraoral landmark?
the outer canthus-tragus, or Frankfort, line. it is an anatomical reference line that extends from the outer canthus of the eye to the superior border of the tragus of the ear
the following picture is what extraoral structure?
the angle of the mouth, which is where the lateral, corner junction where the upper and lower lips meet, marking the side limits of the oral fissure. also known as labial commissure
how are the intraoral landmarks of maxilla and mandible divided?
supporting structures, which is further divided into primary and secondary
limiting structures
relief areas
what are the supporting structures of the maxilla?
residual alveolar ridge
palatal shelf area / hard palate
maxillary tuberosity
rugae area
malar bone (base of Zygomatic process)
what are the relief areas of the maxilla?
incisive papilla
median / midline palatal raphe
canine eminence
torus palatinus
what are the limiting structures of the maxilla?
labial frenum
labial vestibule
buccal frenum
buccal vestibule
hamular notch
fovea palatinae
posterior palatal seal area
vibrating line
what should the direction of functional forces be in complete dentures?
the direction of functional forces should be directed vertically at a right angle to the supporting tissues, as vertical forces are well tolerated by the bone and soft tissues. any non vertical forces are considered damaging forces.
how should functional forces be distributed in complete dentures?
the denture base should cover the maximum possible area of the supporting tissues as spreading masticatory forces over a larger area decreases the stress per unit area, preserving the ridge and ensuring comfort
why is the residual alveolar ridge a supporting structure?
it can absorb most of the masticatory load, supporting the denture
what are the four shapes the residual ridge can be?
flat
rounded
v shaped
u shaped
what determines if the residual alveolar ridge is a primary stress bearing area?
in the edentulous maxilla when the ridge bone is highly dense and the ridge is U-shaped. it is characterized by a flat crest at a right angle to functional forces and a well developed, wide tissue area that minimizes stress per unit area
what determines if the residual alveolar ridge is a secondary stress bearing area?
when the ridge bone is low or poorly dense and the ridge form is flat or V-shaped. it is characterized by a narrow crest that is not at a right angle to functional forces and a narrow tissue area that increases the stress per unit area
what makes the palatal shelf area an ideal primary stress bearing area for the maxilla?
it is the horizontal portion of the hard palate lateral to the midline (palatine vault), covered by firmly attached keratinized mucosa and it consists of compact bone, which is strong and can resist much of the vertical loading force. it does not undergo bone resorption over time
what is the maxillary tuberosity?
the area of the alveolar ridge that extends distally from the second molar to the hamular notch. it must be fully covered by the maxillary denture as it is considered a secondary stress bearing area. it provides resistance to the forward and lateral movements of the maxillary denture, contributing significantly to denture stability.
what is the rugae area?
areas of dense connective tissue in the anterior 1/3 of the palate. they provide lateral and anteroposterior resistance, or stability, to denture movement, as well as increasing the surface area to help in retention
based on the anatomy of the rugae, when can it be a primary stress bearing area?
if the rugae are firm, moderate height, broad and anatomically located at a right angle to the vertical loading forces
based on the anatomy of the rugae, when can it be a secondary stress bearing area?
if the rugae are firmly attached, but are narrow and sloped at the anterior palatal area
based on the anatomy of the rugae, when can it be a relief area?
if the rugae are flabby or highly prominent, meaning it should be surgically removed
why should the rugae not be displaced during impressions?
to avoid tissue rebound, which can cause denture dislodgement or displacement
what is the molar bone area?
a hard area located buccally to the first molar region and is seen in edentulous patients. it is formed of compact bones and is located horizontally at a right angle to the vertical forces. depending on it’s anatomy, it can either be a supporting area or relief area. if it is hard, dense and at a right angle, it has good stress bearing potential. however, if it is sharp, prominent or thin, it should be relieved
what is the incisive papilla, and why should it be relieved?
a pad of fibrous connective tissues that lies between the two central incisors on the palatal side, overlying the incisive foramen of the nasopalatine duct, which is where the nasopalatine nerves and vessels arise. in an edentulous mouth, it may lie close to the crest of the residual ridge due to bone resorption. relief must be provided in the denture to prevent pressure on the nerve and blood supply. if pressure is applied, it can cause pain, numbness or ulceration
what is the median palatal raphe?
a relief area for the maxillary dentures. it overlies the medial palatal suture, extending from the incisive papilla to the distal end of the hard palate
what is the canine or cuspid eminence?
a relief area for the maxillary dentures. a round elevation in the corners of the mouth, representing the location of the root of the canine, which is a helpful guideline for the arrangement of the maxillary anterior teeth
what are the torus palatinus?
a hard, bony enlargement that occurs in the midline of the roof of the mouth (hard palate). it occurs in about 20% of patients. if it is large, surgical removal is required. if small or moderately sized, it should be used as a relief area
what is the hamular notch?
a narrow cleft of loose connective tissues situated between the maxillary tuberosity and the pterygoid hamulus. it is used as a boundary of the posterior border of the maxillary denture
what is the labial frenum?
a fold of mucous membrane that extends from the mucosal lining of the upper lip to the labial surface of the residual ridge
what is the buccal frenum?
a fold, or folds, of mucous membrane that vary in size and shapes. it extends from the buccal mucous reflection to the slope or crest of residual alveolar ridge
what is the labial vestibule?
extending on both sides of the labial frenum to the buccal frenum, it is bounded by the upper lip and the residual alveolar ridge. in dentures, the area that fills this space is the labial flange
what is the buccal vestibule?
the space distal to the buccal frenum. it is bounded laterally by the cheek and medially by the alveolar ridge. the area of the denture that fills this space is the buccal flange, which when properly filled, especially distally, increases retention and stability
what are the fovea palatinae?
two indentations on each side of the midline formed by several mucous glandular ducts. they act as a guide for the location of the midline and the vibrating line of the posterior border of the denture
what is the vibrating line?
an imaginary line that extends across the palate from one hamular notch to the other. the posterior border of the maxillary denture is designed to contact this area during function and at rest, forming the posterior palatal seal (PPS), which helps retain the denture and prevent dislodgement.
what are the supporting structures of the mandible?
residual alveolar ridge
external oblique ridge
buccal shelf area
what are the relief areas of the mandible?
mental foramen
genial tubercles
mylohyoid ridge
mandibular tori
what are the limiting structures of the mandible?
labial frenum
labial vestibule
buccal frenum
buccal vestibule
lingual frenum
alveololingual sulcus / lingual pouch
sublingual salivary gland area
retromolar pad area
masseter muscle area
palatoglossal arch
retromylohyoid fossa
retromylohyoid curtain
pterygo-mandibular raph