L33: Intraoperative care and support of anaesthetised animal
1/46
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
47 Terms
How is oxygen delivery maintained DO2
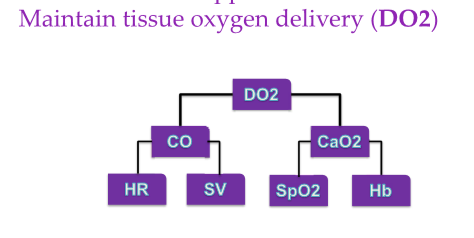
What is cardiac output reduced by
Extremes of HR and disturbances of rhythm
Poor stroke volume
Poor ventricular filling (low preload)
Poor myocardial contractility
High vascular resistance (afterload)
What is bradycardia like in different the dog cat and horse
Dog; <40 bpm
Cat: <90 bpm
Horse: <25 bpm
What can cause bradycardia
High vagal tone
Electrolyte and acid base disturbances (high K+)
Hypothermia
Drugs (potent mu agonist opioids, a2 agonists)
Baroreflex response to hypertension
Bradyarrhythmias
How do you treat bradycardia and bradyarrhythmias
Check monitored parameters and anaesthetic depth
Remember a2 agonist associated bradycardia
Be aware of raised intracranial pressure as a cause
Atropine 0.02-0.04 mg/kg IV
Glycopyrrolate 0.005-0.01 mg/kg IV
What are the bpms on tachycardia for dog cat and horse
Dog: >180
Cat: >220
Horse: >50bpm
What can cause tachycardia
high circulating catecholamines
pain, hypertension, hypovolaemia, hypoxia, hypercapnia
Hyperthermia
Anaemia
Drugs
Sympathomimetics, parasympatholytics
Tachyarrhythmias
How do you treat tachycardia and tachyarrhythmias
Check monitored parameters and anaesthetic depth
Rule out or treat underlying cause
what are some types of supraventricular arrhythmias
AV block
Define cause
Atropine or glycopyrrolate
Atrial fibrillation
Unusual to develop during anaesthesia

In what ways can ventricular arrhythmias occur
Can occur singly or in runs, or as ventricular tachycardia which may be paroxysmal
How do you approach/treat ventricular arrhythmias
Try to determine cause and fix it
Hypercapnia
Hypoxia
electrolyte imbalance
Treat if haemodynamically significant
Assess pulse quality and rate
Assess blood pressure
SpO2, mucous membrane colour and CRT
if you decide to treat ventricular arrhythmias what do you use
Lidocaine first choice
1-2 mg/kg slow IV bolus (dog and horse)
0.5 mg/kg IV bolus (cat)
Followed by CRI at 25-100 ug/kg/min
maximum dose (over 10 minutes)
Dogs; 4 (-6) mg/kg
Cats; 2 mg/kg
Cats sensitive to lidocaine toxicity, may start treatment with beta blocker instead
How do you treat underlying hypovolaemia/hypotension
Reduce depth of anaesthesia if possible
Give IV fluids (bolus if necessary)
inotropes/vasopressors
what fluids are commonly given during anaesthesia
Crystalloid fluids for relative hypovolaemia
How do you know which fluid type to use
Depends to some extent on nature of deficit but CSL most common as its balanced
Different rates suggest between 2-10 mL/kg/hour
Commonly 5ml/kg/hour
May need rapid bolus in emergency situation (5-10mL/kg)`
What are colloids good for
If TP <35g/l or if better IV filling needed
Plasma
FFP, FP as above or if clotting factors required
Fresh whole blood (FWB)
Packed red blood cell (PRBC)
Human serum albumin (HSA)
What are the typical blood volumes for dogs and cats
dog: 80-90 mL/kg
cat: 50-60 mL/kg
What fluids do you give for 10% total blood volume loss
crystalloids
What fluids do you give for 10-25% total blood volume loss
Colloid
What fluids do you give for >25% total blood volume loss
Blood
What fluid do you give if PCV is <20% or Hb <7 g/dl
Blood or PRBCs
What are some examples of inotropes
Dopamine
Dobutamine
What are the high, mid and low rate for dopamine
Low rate: 2-5 ug/kg/min- DA receptor
Mid range: 5-10 ug/kg/min- b1 receptor, positive inotrope
high rate: 10-15 ug/kg/min- affect a1 receptors, vasocontriction
What are some side effects of dopamine
what animals is dopamine usually used in
arrhythmogenic
Dogs and cats
Where does dobutamine act and what is its use
Acts mainly on B1 receptors
Positive inotrope with minimal vascular resistance
Mild chronotropic
Less arrhythmogenic
dose of 0.5-10 ug/kg/min
horses
what are some types of vasopressors
noradrenaline
phenylephrine
ephedrine
vasopressin
What does noradrenaline do
B1 and a1 adrenergic effect
Positive inotrope and vasopressor
Increase CO and SVR
Reduced liver, muscles and renal and skin perfusion
Dose 0.1-1.0 ug/kg/min
what does phenylephrine do
a1 adrenergic effect
Vasopressor
Increased SVR
Reduced splanchnic perfusion
Dose 0.002-0.02 mg/kg IV or 1-3 ug/kg/min
What does ephedrine do
Stimulates endogenous noradrenaline release
a and b adrenergic effect
subsequent boluses have diminished effect
Reduced splanchnic and renal perfusion
Increased HR, MAP, CO
Dose: 0.02-0.05 mg/kg IV/IM
what does vasopressin do
Potent vasopressor on V receptors
Increased SVR
Reduced splanchnic perfusion
What are some conditions that need respiratory support
hypoventilation
Hypercapnia
Hypoxaemia
what is hypercarbia
increased CO2
Normal range 35-45 mmHg
May occur due to
Hypoventilation
Rebreathing of exhaled gas
increased BMR
What are some good effects of hypercarbia
Increased symp tone
Circulatory stimulation
Stimulates respiratory centre
What are the downsides to hypercarbia
Tachycardia
Hypertension
Cardiac arrhythmias
Increased intracranial pressure
CV depression at high levels
Resp acidosis
vasodilation
Define hypoxaemia
Arterial PO2 <60 mmHg or SpO2 <90%
What can cause hypoxaemia
Decreased FiO2
Hypoventilation (on air/O2 air mix)
V/Q mismatch and shunt
CV depression
Diffusion barrier
anaemia
Increased O2 demand
Pyrexia, Increased BMR, shivering
How can you help in cases of hypoxaemia and hypercapnia
check anaesthetic depth
check airway
increase FiO2 if possible
Ensure no rebreathing CO2
Ventilate
intermittent positive pressure ventilation
Consider use of PEEP
consider recruitment manoeuvre in horses
Consider salbutamol in horses
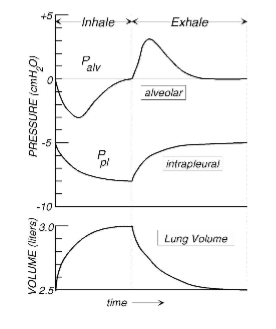
What are the mechanics of ventilation/spontaneous breathing
Inspiration
expansion of thorax
Generating negative intrapleural pressure
draws air into lungs
Expiration
Intrapleural pressure rises as thorax contracts
but intrapleural pressure remains negative throughout respiratory cycle
negative intrapleural pressure necessary for normal thoracic pump and cardiac output
What are the effects of IPPV
Intrapleural pressure remain positive/above zero throughout resp cycle
Decreased venous return decreased cardiac output
Worse with high pressures and long inspiratory times
Worse in hypovolaemia animals or those in heart failure
what are the IPPV guidelines
Tidal volume 10-15 mL/kg
Rate 10-20 breaths/min (horses 6-10 b/min)
Inspiratory: Expiratory ratio 1:2-1:3
End tidal CO2 35-45 mmHg
Peak inspiratory pressure (PIP) <20cm H20 (20-40 cm H20)
Positive end expiratory pressure (PEEP) <5cm H20
What reflex causes increased intracranial pressure
Cushings reflex
What is the purpose of increased intracranial pressure : Cushings reflex
Impending death
Last attempt to maintain cerebral perfusion
What is in cushings triad
Increased blood pressure
bradycardia
Resp changes if not ventilated
How do you treat increased intracranial pressure
Hyperventilate as emergency measure (if anaesthetised)
Mannitol- osmotic effects
also reduce blood viscosity → blood flow and oxygen delivery
Hypertonic saline → osmotic effects
Furosemide → may be synergistic with mannitol
does shivering and pain increased oxygen demand
yes increased demand in recovery
what are the effects of hypothermia
MAC reduction (~5% every C)
Alters pharmacokinetics and pharmacodynamics of anaesthetic drugs → prolonged recovery
Organ system dysfunction (CV, resp, CNS)
Increased blood loss → increase clotting times
Shivering increases oxygen demand in recovery
increased incidence of SSI (human)
Delayed wound healing
Humans report hypothermia as not it to have
How can you treat/give temperature support
Rebreathing circuits and HME
Warm operating theatre
Passive techniques
Towels, bubble wrap, reflective blankets
Active techniques
Electric heated blankets, forced warm air blankets, heat lamps, IV fluid warmers, warm abdominal lavage fluids, circulating warm water pads