Aural Rehab Midterm
1/82
Earn XP
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
83 Terms
Goals of aural rehab
Alleviate the difficulties related to hearing loss (i.e. hearing aid will provide audibility of speech sounds to help with word recognition
Lessen the consequences (if we can’t remove the problem, we can try and lessen)
Services included in AR plans
diagnosis and quantification of hearing loss
provision of appropriate hearing devices
training in the use of hearing devices
communication strategies training
vocational counseling
noise protection
counseling and instruction for family members
Who provides AR?
SLPs
Audiologists
Otolaryngologist (restore hearing for some)
Teacher of Deaf/Heard-of-Hearing
Basic configuration of hearing loss
refers to the extent of the hearing loss at each frequency and gives an overall description of the hearing loss
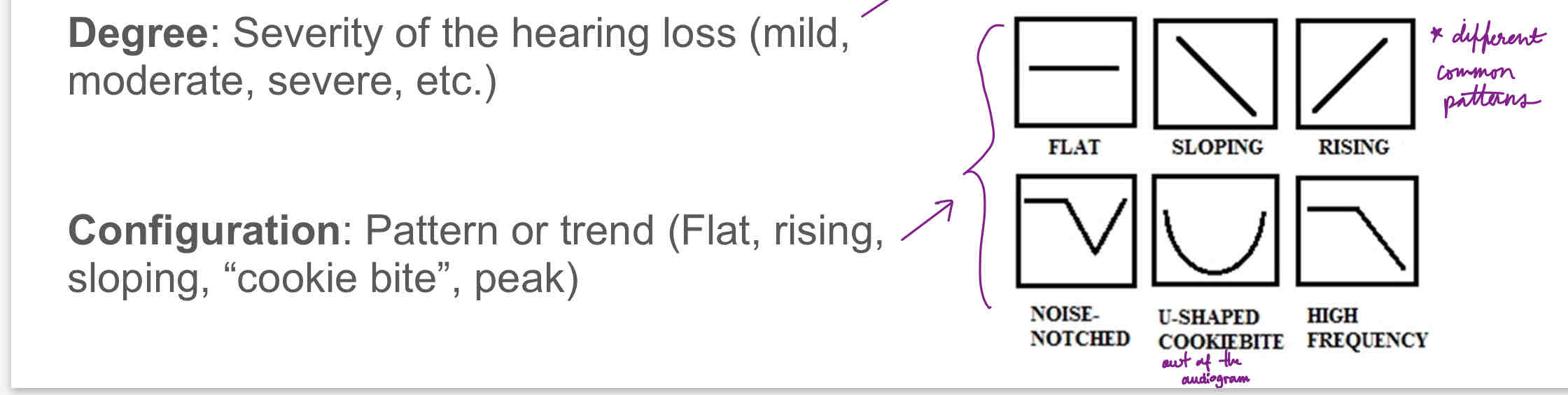
How is HL categorized?
Degree, onset, causation, and time course
Sensorineural hearing loss
a type of hearing loss that has cochlear or retrocochlear origin; stems from a disturbance in the inner ear, CN VIII, brainstem, midbrain, or auditory cortex
Conductive hearing loss
results from an obstruction within the outer or middle ear
Mixed hearing loss
a hearing loss that has both conductive and a sensorineural component
Degree of hearing loss
normal: PTA 25 db HL or better, for children: 15 dB HL
mild: PTA: 26-40 db HL or better, for children: 16 dB HL
moderate: PTA 41-55 db HL
moderately severe: PTA 56-70 dB HL
severe: PTA 71-90 db HL
profound: PTA is poorer than 90 db HL
Difference between symmetrical and asymmetrical hearing loss
symmetrical hearing loss means the degree and configuration of hearing loss are the same in each, asymmetrical means the two ears differ
Tinnitus
the perception of sound in the head without an external cause, 35-50% of people with hearing loss also report tinnitus
causes: cerumen, Meniere’s disease, ototoxic drugs (cisplatin, aspirin), noise, acoustic neuroma
currently no FDA approved therapeutics for tinnitus
Older adults and special considerations
be sensitive to health factors that may interfere with communication:
including loss of vision
stroke, memory loss
Arthritis or muscle weakness may impact listener’s ability to manipulate hearing aid battery
Dementia + Alzheimer’s disease may impact ability to manipulate hearing aids
some studies show for Alzheimer’s patients that the ability to hear what goes on around them helps them stay in tune with their surroundings for a longer period of time
should patients in assistive care facilities and/or nursing homes be fitted with HA?
some may choose ALDs for phones, TV, doorbells
some fear techonology - it’s best to keep it simple for them
include family members or caregivers
Age of onset of hearing loss
20s: may impact job choices or college major
40s: may change outlook in regards to making a career change
60s: may lessen interest in traveling, going to classes
Psychological adjustment
patients may need to process coming to terms with their hearing loss - may experience shock, disbelief, depression, anger, guilt, acceptance
Prelingual
hearing loss occurs before language has developed, usually before 2 yrs old
Perilingual
hearing loss occurs before language has “solidified,” usually after 2 yrs and before 5 yrs old
Postlingual
hearing loss occurs after 5 yrs of age, after language foundation has fully developed; can be broken down into:
prevocational (5-17)
early working age (18-44)
later working age (45-64)
retirement age (65+)
Congenital
implies the hearing loss was present at birth
Acquired
implies the hearing loss was incurred after birth
Assessing communication handicap
interview
questionnaire
daily log
group discussion
structured communication interaction
Interview
open-ended, similar to case history, but with more generous listening, semi-structured conversational format
advantage: rapport established with patient, lots of flexibility in follow-up questions
disadvantage: can’t qualify with outcome assessments
settings discussed: home, social settings, school workplace
Questionnaire
pre-selected set of questions, can be open-set (qualitative data) or closed set (quantitative data)
advantage: most are easily quantified for outcomes assessment
disadvantage: some questions do not apply to patients (ex: how well do you hear at church? But the patient doesn’t attend)
need to choose an appropriate questionnaire, not universal
some are also designed for communication partners, ex: HHIA-SP
ex: COSI, HHIA
Daily log
patient self-monitors behaviors of interest related to hearing difficulties
advantage: patient may be getting instinct through this process
disadvantage: must make it highly specific or patients may come back with nothing or notebooks full of irrelevant details
provide them something that includes detailed instructions, short number of items, be specific
Group discussion
a class or group of people (and significant others) that contributes to a list of problems common to many DHH individuals, ex: group AR classes for adults
advantage: DHH and partner realize that they are not alone
disadvantage: DHH individuals may not take advantage of group classes
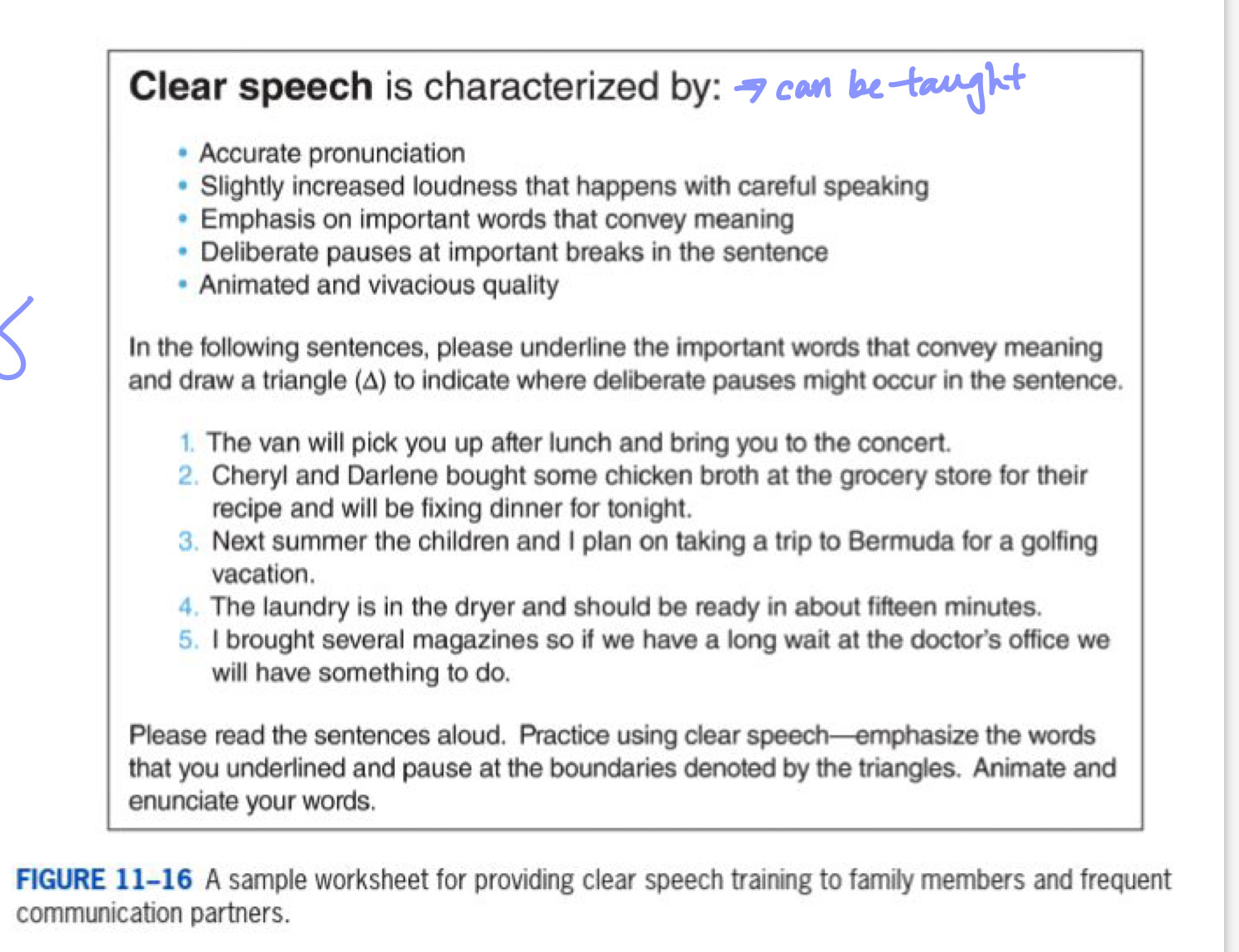
Communication strategy
course of action taken to enhance communication
Facilitative strategies
actions taken to prevent a communication breakdown, ex: arranging seats in a circle to assist speech-reading, good lighting, closed doors, etc.
Repair strategies
corrective actions once a breakdown has occurred, ex: asking for clarification, when in doubt - write it out, move to quiet spot
specific repair strategies
they request the listener to:
repeat the part or all of the message
confirm the message
choose between two candidates
simplify the message
these are preferred to continue good conversational fluency
Nonspecific repair strategies
huh?
what?
pardon?
these responses should be avoided because they are not specific enough on what parts of the initial message was not received
Talker
the person speaking and using good strategies for clear communication, ex: please speak slowly and clearly
Message
what type of message is being communicated, ex: boring text vs. intriguing story, ex: DHH person uses strategies to limit possible response from communication partner —> do you like watching comedies or drams?
Environment
difficult/adverse listening environments: poor lighting, noise, echo, distance; DHH person can:
move to quiet places
move closer to the speaker
find good lighting, away from glare
avoid highly reverberant rooms ex: gyms
Listener (heard-of-hearing person)
good or bad speech reader (may be culturally related such as not looking at the face, degree of hearing loss/residual hearing, acceptance of loss)
factors that influence with the reception of message:
relaxation
strategies that counteract maladaptive behaviors
appropriate expectations
self-advocacy
anticipating potential vocabulary
degree of hearing loss, consistent use of hearing devices
Who is a candidate for hearing aids?
anyone with hearing loss or hearing difficulty who is motivated
Basic components of hearing aids
microphones (transmitter) - picks up sound and converts sound to electrical signal
amplifier - increases the strength of the electrical signal, done with a computer chip to digitize and multiply the signal to place sound into audible range
receiver - small loudspeaker that converts the electrical signal back to an acoustic signal
battery - provided the energy to power the system
Specialized features of HA
volume control
tele-coil
directional microphones
multiple programs, remote control
noise reduction algorithms
feedback cancellation algorithms
frequency compression.transposition
tinnitus reduction/masker
Completely in canal
Cons: CIC are small, options often are not available such as: on/off switch, volume control, and telecoil
Pros:
easy to insert and remove
better sound quality some people report
reduction of feedback, improved sound localization
virtually invisible if cosmetics is important to the DHH person
In-the-ear or in-the-canal
hearing aids that fit into the concha of the ear
Pros:
usually has room for volume control and directional microphones
custom fitted to the user’s ear
closeness of the receiver to the tympanic membrane means less gain is required to provide adequate amplification for certain levels of hearing loss
Cons:
can magnify an occlusion effect for those with good hearing in the lower frequencies
subjected to ear wax build up
user’s voice can sound distorted or too loud
Behind the ear BTE
hearing aids that are worn over the pinna and coupled to the ear by means of an ear mold, most appropriate for infants, toddlers, children
Pros:
provides the most gain without feedback
best when high levels of gain needed
allows for directional microphones
can be hardwired to an assistive listening device
Cons: cosmetically may be an issue for people who do not want their HA to be visible
Bone conduction or BAHA
style used in cases of conductive hearing loss such as aural atresia, chronic drainage, challenging fit etc. —> can be worn on a headband for children or those who don’t want surgery
Pros:
can help by pass problems of feedback, occlusion effects, cerumen buildup
Cons:
high cost
surgery
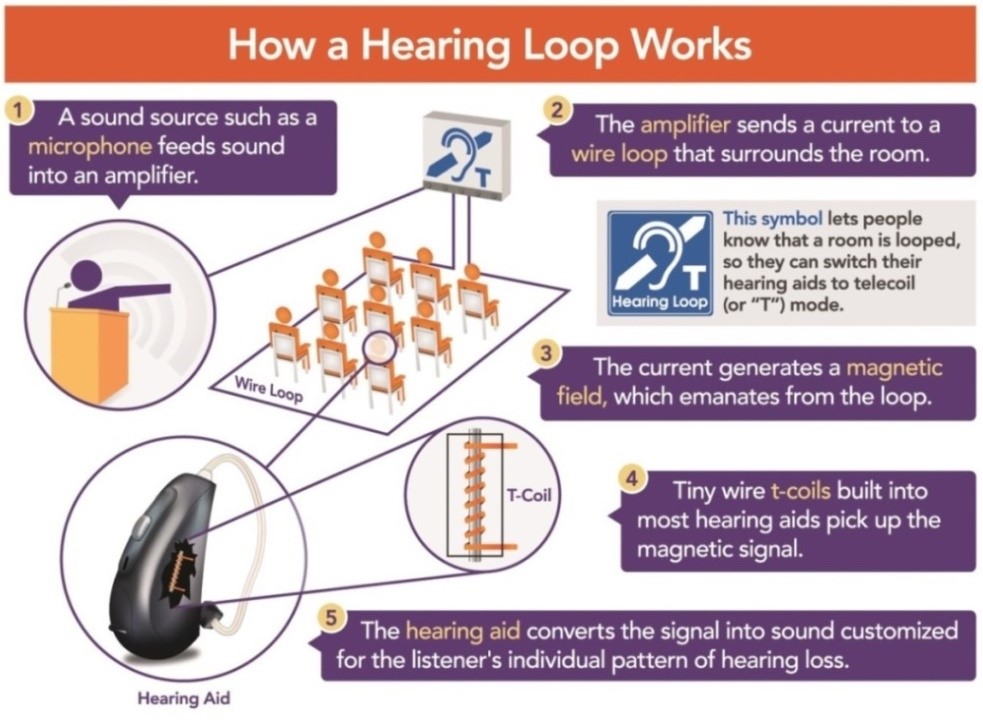
Tele-coil
a small coil inside HA - works as a small receiver which picks up signals from a loop system that acts as an electromagnetic field. HA with an activated telecoil can convert this electromagnetic field into a sound signal
listens to magnetic signal instead of the sound
magnetic signal can be from a telephone, CD, TV, personal ALD, headphone, loop
advantage is improved signal-to-noise
usually on BTEs
may have to ask or demand for tele-coil
Directional microphone
allows for better signal-to-noise ratio for sound source in front of listener
manual or auto selection
has selectable modes such as:
quiet situations: pick up everything
noisy situations: block background noise from sides and back of head
Tinnitus masker
An electronic hearing aid that generates and outputs noise at low levels for the purpose of masking an individual’s tinnitus
Feedback reduction
Algorithms that stop the output from a hearing aid receiver from re-entering the microphone, which can send the system into oscillation and create a squealing noise if it goes through
Wireless connection to devices (phones/TV)
When sound is transmitted from the sound source to the individual by means of radio waves or infrared signals, the wireless system picks up the audio signal through a microphone or by direct electrical plug-in. Sound is then converted into an electrical signal by a transmitter and delivered through the air to a receiver worn by the user
Remote microphone hearing assistance tech RMHAT
When a microphone is placed close to the talker’s mouth, where the decibel level of the acoustic speech signal is well above that of interfering noise and reverberation. The resulting high quality signal is delivered to the listener via a personal FM receiver or sound field loudspeaker
Monaural vs binaural
Binaural is recommended in most situations for reasons, especially if the hearing loss is moderate or severe. Even though two hearing aids are more expressive than one and may require more effort to maintain, binaural amplification fitting offers many advantages over monaural fitting, such as:
improvement in background noise, HA can detect non-speech and silence it
localization is easier
avoid possible deterioration of unaided ear
keep ear stimulated (for possible cochlear implant)
Head shadow
With one hearing aid, sound coming from the unaided side of the head may be attenuated by as much as 12 to 16 dB, especially high-frequency sounds. Use of two hearing aids allows sound to be received on both sides of the head
Loudness summation
When sound is received by both ears, a summing of the two signals results. Thresholds for sound may improve by 3 dB or more compared with monaural thresholds in either ear
Binaural squelch
Listening performance will be better in noise when the user wears two hearing aids instead of one. The improvement in signal-to-noise ratio may be 2 or 3 dB
Localization
People with normal hearing are sensitive to interaural differences in a sound’s intensity and phase and this allows them, in part, to perceive the direction and the location of a sound source and to segregate one sound source from another. A monaural hearing aid fitting disrupts these cues, whereas binaural hearing aids serve to preserve this localization ability
What is involved with HA verification, and why is it necessary?
It is the means to determine that the hearing aid meets a set of standards, including standards of basic electroacoustics, real-ear electroacoustic performance, and comfortable fit. Other steps involve:
verify sound quality is good (ask questions and listen to hearing aids)
verify patient doesn’t have feedback (can run a feedback test and activate feedback cancellation)
verify for comfortable fit
teach patient or parent how to use, insert batteries, change volume or program, clean hearing aid and ear mold
review warranty (loss and damage + repair)
how to adjust to new sounds, physical fit of device
how often to ear (in case of infants/children, ASAP and for all waking hours)
use of probe microphone
What is involved with HA validation, and why is it necessary?
Determines the extent to which hearing-related disability has been reduced by an intervention, such as receipt of a hearing aid. Other steps involved include:
“aided” audiogram (limited benefit measured by audibility of pure tones), not always the most reliable strategy
Speech in noise testing (most important “aided” testing)
Outcome measure: questionnaires, COSI, HHIA
Subjective benefit/Validating fit of devices
Seven categories of self-report outcome data. Choice of a particular self-assessment scale might be based on which of these seven categories you are interested in assessing
Benefit
The change in hearing-related disability that has resulted from the use of amplification
Satisfaction
An overview of the physical, psychological, and financial changes that have resulted from the use of amplification
Use time
Often related to the severity of the hearing loss and contextual factors, but is an incident of how helpful and beneficial the hearing aid is for the patient
Residual activity limitations
The hearing-related difficulties that the patient continues to experience despite the use of amplification (where/when are you still having difficulties?)
Residual participation restrictions
Limitations that prevent an individual from fulfilling a role in life (ex: volunteering at a soup kitchen, business meeting, etc.)
Impact on others
Usually determined by a frequent communication partner (not many instruments are available for this purpose), family members, etc.
Quality of life
Including improvements in social life and mental health
Hearing assistive technology systems
They are listening, alerting, and/or signaling devices that facilitate patients’ communication with the environment or enhance their personal safety through the use of auditory, visual, or tactile modalities; encompass assistive listening devices and other assistive devices. Basic components include:
microphones
amplifier
receiver
battery
Loop systems
Works by running a wire around the circumference of a room or table that conducts electrical energy from an amplifier and thus creates a magnetic field, which induces the telecoil in a hearing aid to provide amplified sound to the user
TV ears
Amplified telephones and devices for the television set
Impact of speech perception in a room
power of sound source
how loud is the voice
distance from the sound source
how far away is the listener from the speaker
reverberation (echo)
how many smooth or hard surfaces
background noise
signal-to-noise ration or S/N
Signal-to-noise ratio (S/N)
The level of a signal relative to a background of noise
ex: when I am 1 m away, my voice (the signal) is 78 dB SPL. IF the background noise is 60 dB SPL, then the S/N is 78/60 or +18 S/N
Ratio needed for DHH individuals
DHH students need on average +20 S/N to function at the same level as students with typical hearing can function at 0 S/N; adults with mature auditory systems, larger vocab/ability for auditory closure, don’t need as much
Impact of residual hearing on speech reading
Even a small amount of hearing can significantly improve the ability to lip read, individuals with hearing loss must rely even more heavily on visual cues to supplement what they miss with their ears
Benefit of visual + auditory input
Even people with typical hearing use visual information for cues as to the meaning of an utterance
Some words can mean something entirely different if said with a smile, or even with different emphasis
Analytic vs synthetic training
analytics (bottom up) - students learn to recognize individual speech sound movements; identify whether the word contained a specific speech sound in its initial, medial, or final position (without having to identify the word itself), etc. TRAIN THE EYES
Synthetic (top down) - students try to use the “whole” to get the gist of the message. They use whatever information is available - auditory, visual, contextual cues, etc.. The instructor may give a category, such as, “National Holidays,” so that context narrows down the possibilities. The point is for the speech reader to recognize the general meaning, even if he or she does not know each individual word that was said.
Visual perception
The speech reader must be able to perceive the invidious speech sound movements
Visual memory
The speech reader must retain the string of speech movements in memory so it can be processed
Visual closure
The average spoken message includes more phonemes per second than the eye can follow. The speech reader must be able to “fill in the blanks” when information is missing
Visual figure-ground
The speech reader must be able to ignore extraneous visual information and focus on the face
Visual attention
The speech reader must be able to pay attention to the available visual cues. This requires concentration
Group AR general factors
length of program
Class format
Individual or group therapy sessions (ACE has both)
Ground rules
Examples can include:
Only one person speaks at a time
Let us know when you are finished speaking by nodding your head
Everything said in this room is confidential
Be specific and use examples
Topics
Stay on topic and focus on the question or issue under discussion, jumping from topic to topic can lead to communication breakdowns
Who should attend?
DHH person and partner together
Speech reading
Involves integrating what is seen with what is heard
Incidence of HL is the US + Incidence of congenital HL
The Hearing Loss Association of America is the nation’s leading organization representing the 48 million Americans with hearing loss. About 2-3 out of every 1000 children in the US are born with a detectable level of hearing loss in one or both ears.
Incidence of HL in the US
Incidence of congenital HL