Neuro PT2- Topics Related to Wheelchair Evaluations
1/117
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
118 Terms
Who uses WCs?
Any age
Any diagnosis
Any environment
Any funding source
Any life-style, life-role or vocation
Ongoing/permanent need or temporary
Match patient characteristics/needs to customize WC
Fit
Skin protection
Postural support
Function
Environment
Transportation
Durability/maintenance
Affordability
How long can it take to get a custom WC?
Typically several weeks to months, depending on patient needs and manufacturer.
~3-6 months
How often does someone get a new WC?
5 years/or sooner if needs change significantly (i.e. new dx/change in fctn)
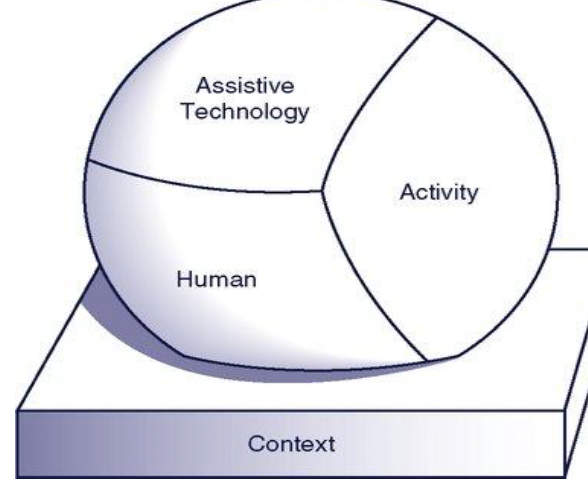
What is the HAAT Model
How assistive tech interacts with the individual and how it assists them
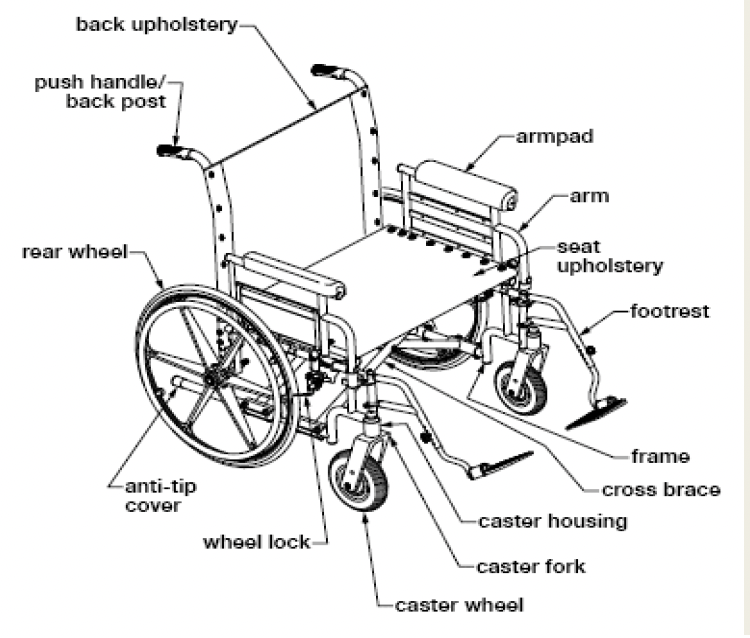
What are the parts of a WC
Standard WC height
18”x16”, 19.5” height
Hemi WC height
17.5’’ Floor to seat height
Super low WC height
Less than 17.5’’ Floor to seat height
Tall WC height
18” depth, seat height
Amputee WC axel placement
posterior axel to prevent falling fwd
Ultra light weight WC consideration
Weight, adjustable axel placement
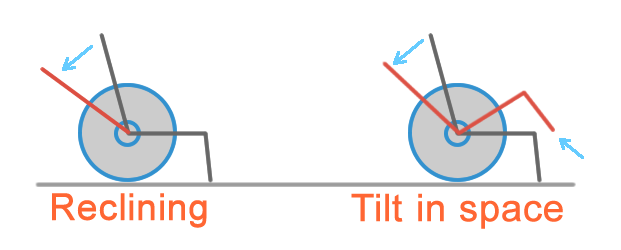
Recliner WC considerations
Seat to back angle
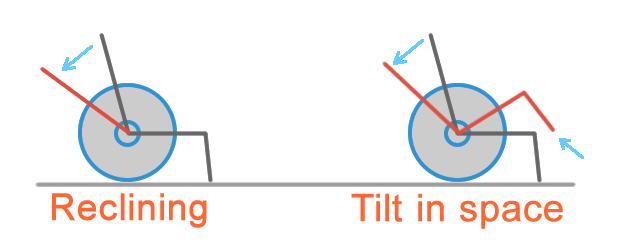
Tilt-in-space WC considerations
Floor to seat angle
Power WC considerations
Power base vs. frame
Position of the drive wheel

K001 WC and use
Standard w/c
used for transport rather than seating
K002 WC and use
Standard hemi wheelchair
used for transport rather than seating
Different than standard due to height
K003 WC and use
Leightweight WC
Adjustability to meet the user’s seating/positioning needs
Access floor for propulsion
Adjust armrests for transfers
WC used >2hrs/day
K004 WC and use
High strength, light weight WC
Allows increased adjustability for long term users, weighs less
Access floor for propulsion
Adjust armrests for transfers
WC used >2hrs/day
K005 WC and use
Ultra lightweight WC (<30lbs)
Lightest and most configurable (no front rigging)
Adjustable rear axle
Individual’s primary mode of mobility and help with ADL participation
K006-7 WC and use
Heavy-duty & Extra heavy duty wheelchair
Match features with K1-3s, reinforced for people >300lbs
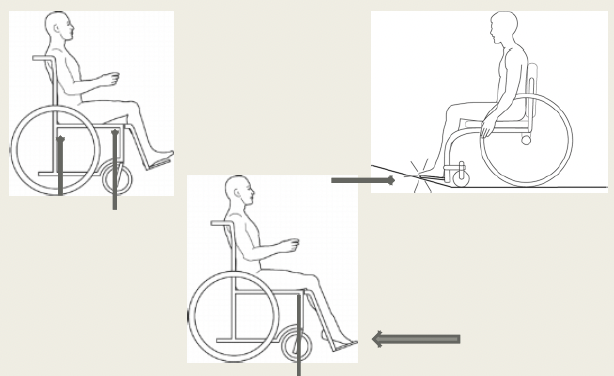
Vertical seat to floor height effects
Influences dump
What is dump
Front Seat-to-Floor Height (FSTH) - Rear Seat-to-Floor Height (RSTH)= Dump
Benefits of increasing dump
Tilting the seat back anchors your pelvis securely against the backrest via gravity.
Keeps you from sliding forward.
Vital if you have limited core strength or poor sitting balance.
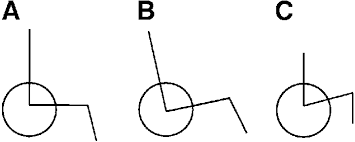
Axle placement
Post=more stable
Ant=more tippy
Scooters
Steer with tiller
Wider turns
Longer length
Able to break down for transport (it weighs 135lbs so think about who’s transporting it)
Group 2 powered WCs
‘Consumer’
Tilt, seat elevator, elevating leg rests
Power recline not available
Need eval by ATP
Group 3 powered WCs
‘Rehab’
Specific diagnoses
Expandable electronics
Multiple functions
Need eval by ATP
Front Wheel Drive
Drive wheels in front
Pulls wheelchair over obstacle
Better traction
Turning is behind user
Midwheel Drive
Drive wheel in middle
2 sets of casters in front and back
Get stuck on obstacles/uneven terrain
Smaller turning radius
Drive wheel under user
Easier to drive
Can pull closer to counters and tables
Rear Wheel Drive
Drive wheel behind user
Less common
Very stable
Large front casters can interfere with foot positioning
Turing happens in front of user
Power seating functions
Posterior Tilt
Anterior Tilt
Recline
Elevating leg rests
Seat elevator
Standing
Posterior tilt function
Pressure relief
OH/posture event
Rest breaks
Changing for incontinent episodes
Anterior tilt function
Transfers
Reaching (30 degrees you need knee blocks)
Recline function
Hamstring contracture prevention
Bladder and spasticity management
Elevating leg rests function
Swelling
Spasticity
Seat elevator function
Reaching
Transfers
Interactions
Standing function
Bladder
Cardiovascular
Stretching
Spasticity
Questions for matching a wheelchair with a person’s lifestyle or activity
Where it’ll be used and the terrain
Activities you do/want to get back to doing
How will you transport the chair
How much of the day will be spent in the chair
How will you transfer
If you need help, who will help and what features do they need
Physician responsibility for WCs
Has the burden of proof for justifying the need for specialized manual and power wheelchairs
Must provide a prescription for the wheelchair
For Medicare to pay for a wheelchair, the physician must complete a face-to-face mobility evaluation Documentation must include five items
Must complete a “seven element order”
Physician 5 items
chief complaint
physical assessment (height, weight, neuro fctn,
cardiovascular)
Medical conditions limiting mobility
Impact on ADLs
Why alternative devices are insufficient
PT/OT responsibilities for WCs
Assessment
What components are appropriate with ATP
Complete trials
Write LMN
Supplier (RTS)/Equipment Rep/Vendor/DME dealer responsibilities for WCs
Can compare the characteristics of wheelchairs and parts, and durability.
Equipment rep
Can provide trial equipment
Could be present during trial
Answer questions
Demonstrate use of equipment
Funding source responsibilities for WCs
Establishes guidelines and requirements for paying for equipment
Different payers have different input on the evaluation process
Case managers
OVR
Home accessibility
Medicare funding source
For home
Used as model
Medicaid funding source
Community
Wheelchair Procurement Process
Initial eval
Vendor visit
Paperwork
Submission to insurance
Determination
Delivery
WC procurement- Physician
Refers pt for eval
Automatic as part of inpatient PT referral
WC procurement- Therapist
Evals pt
Automatic as part of inpatient PT referral
WC clinic if in outpatient
WC procurement- supplier
Measures, orders, contributes to eval
LMN submitted to supplier
Required by most payers for K005, group 2, or above powered WCs and other equipment
*LMN good for 6months for medicare
WC procurement- payer
May require home visits for accessibility
Reviews documentation for auth/denial
30 day turn around
Evaluation
HPI/dx
PLOF
Home environment
Current equipment
Objective measures
Trials
HPI
Dx
PMHx
Falls
Skin integrity
Life roles/activities
Daily routines and lifestyle (can they stand to shower/dress safely)
PLOF/home enviornment
Home set up
Entrance/accessibility
Hours w/ caregivers
Ability to complete MRADLs
Adaptive equipment
Transportation
Current equipment
What
How old
Condition
Hours being used
Why it isnt meeting needs
How to operate
Ability to operate
Objective measures
Pain rating
ROM
MMT
Handheld Dynamometry
Edema
Functional Mobility
Tone/Spasticity
Sensation
Gait
Motor function
Posture and positioning
Measurements
Outcome measures
Motor function
Determines how patient will operate WC
Manual- mode of propulsion
Power- controller type/alternate driving modes
Posture
Essential for max functionality
Ideal sitting position important for
Arousal/eye contact
Respiratory and gastrointestinal health
Minimizing musculoskeletal overuse injuries
Prevent acute and/worsening of chronic postural deformities
Maximize independence
Preserve skin integrity
Functional Seating- Stability
UEs not needed for upright position
Can use UEs for functional activities and participation
Stable BOS (more so when COG behind)
Persons with poor posture control achieve via kyphosis and sacral sitting
Functional Seating- Dynamic
Movement in response to sensory feedback from NM system
Planned movements
Ideal functional seating
WB on ischial tubs, not sacrum
Spine curved with slight kyphosis and lordosis (~5 degrees)
Skin integrity breakdown due to
Poor mobility
Poor sensation
Postural deformities
Previous skin issues
Age
Nutrition
Incontinence
High risk areas in sitting
Occiput
Scapula
Spinous processes
Elbow
Greater troch
Sacrum
Coccyx
Ischial tuberosities
Heels
Posture exam
Observation (with and without support)
Examine the pelvis in unsupported sittingIn all planes
Examine the trunk in unsupported sittingIn all planes
Examine the pelvis and lower extremities in supine
Take anatomical measurements
Non reducible postures
posture that is rigid and unable to be corrected with a reasonable amount of force
Wheelchair will be designed to accommodate the patient’s postural deformities.
Trying to correct a fixed posture can lead to skin breakdown
Reducible postures
posture that is moveable and able to resume/partially resume a neutral position
Wheelchair will be designed to reposition the patient into an optimally functional position to prevent worsening of the postural deformities/skin breakdown
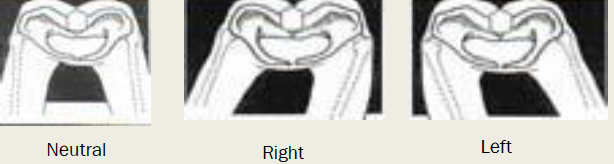
Pelvis movements in anatomical planes
Sagittal Plane: Tilt
Coronal Plane: Obliquity
Transverse Plane: Rotation
Pelvic tilt for WCs
ASIS/PSIS line is parallel to seat plane: neutral pelvic tilt
Neutral pelvic position risks and limitations
Pressure distribution equal across ischial tuberosities and down femurs
No increased areas of pressure
Optimizes UE fctn
Decrease LB strain
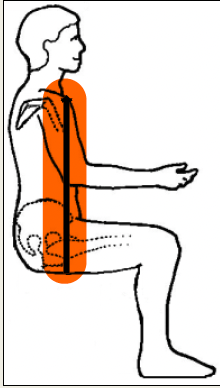
Posterior pelvic tilt risks and limitations
Sacral and coccygeal breakdown
Thoracic and spinous process breakdown
Limited OH movement
Shoulders at risk for pain and injury
Limit ability to scan enviornment
Collapse chest and limit excursion of breath
MOST COMMON
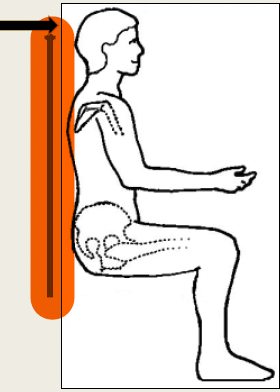
Anterior pelvic tilt risks and limitations
Increased lumbar lordosis
Increased contact of thoracic spine at backrest
Decreased contact with lower backrest
Increased pressure at anterior portion of the pelvis
Impaired trunk control
Tight hip flexors
Increased risk of tipping wheelchair backwards
Pelvic obliquity assessment
Assess Iliac crests
Assess ischial tuberosities for depth of sitting position
Pelvic obliquity risks and limitations
Ischial tuberosity breakdown
Lateral trunk breakdown
Can worsen or promote a scoliosis
Limits shoulder range of motion
Difficult to push a wheelchair straight
Alters perception of environment
Pelvic rotation assessment
Locate ASIS b/l and assess which is most forward
If R ASIS more forward, it’s a R rotation
Pelvic rotation risks and limitations
Ischial tuberosity breakdown
Decreases unilateral femur support
Places shoulders at risk for injury and pain when pushing a wheelchair
Pelvic rotation causes
muscle imbalances such as hemiplegia or decreased range of motion
other premorbid issues, such as fractures and joint replacements
Pelvic rotation effects
Can cause rotations of the spine, trunk deformities, and back pain
If reducible, correct with seatbelt or seating
If non reducible, acomodate with backrest to meet pelvic angle
Trunk movements in anatomical planes
Sagittal Plane: Kyphosis/lordosis
Coronal Plane: Scoliosis
Transverse Plane: Rotation
Trunk position for WC
Heavily affects a patient’s ability to use their upper extremities for ADLs, propulsion/drive power wheelchair
Determines backrest type
Reducible: trunk alignment
Nonreducible: determine most functional position while preventing further postural deformities, skin breakdown
Trunk sagittal plane ideal position
The tragus of the ear should be in line with the acromion process of the scapula
Thoracic spine kyphosis
Lumbar spine lordosis
Trunk sagittal plane deviations
Forward head posture
Increased or decreased thoracic kyphotic curve
Increased or decreased lumbar lordotic curve
Trunk coronal plane ideal position
Seated symmetrically unsupported at edge of mat and able to maintain midline position
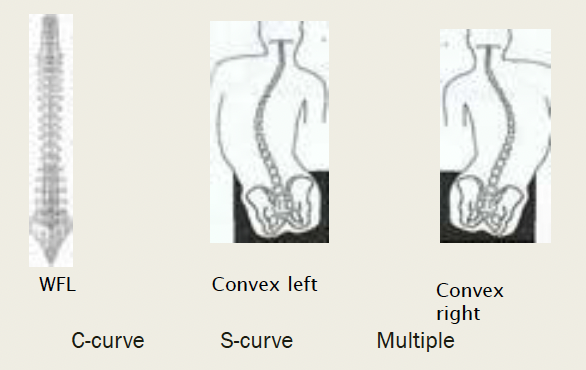
Trunk coronal plane deviations causes
Structural/functional scoliotic or C-curves
Muscular tightness/spasticity
Trunk muscular weakness
*asses where lat support needed!
Trunk coronal plane curves
Trunk transverse plane ideal position
Cervical, thoracic, and lumbar vertebrae are aligned in neutral position
Trunk transverse plane deviations causes
Cervical, thoracic, lumbar segment rotation
Muscular tightness/weakness
Spasticity
Transverse plane pelvic rotation
Left anterior trunk rotation
True hip flexion
determines seat to back angle via PROM of hip in supine before ASIS/PSIS moves
used to prevent sliding in chair and skin breakdown
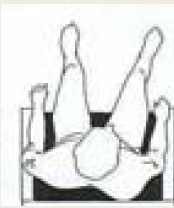
Windswept hips
named the way the knees are going
Knee Extension with True Hip Flexion
Determines angle of leg rest hanger
Measured to point of hamstring tension
Tight hamstrings and large footrest angle
Feet pull backward off leg rests
Slide anterior causing sacral sitting
Feet in danger of becoming entangled in front riggings of the chair
*less tucked someone is=larger turning radius due to longer chair
Ankle DF angle
Determines appropriate angle of leg rest footplate or justify angle adjustable footplate
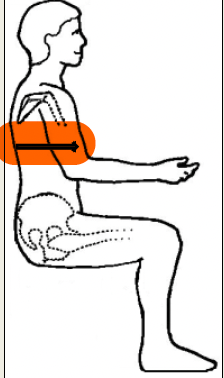
Measurements in the coronal plane
Hip width
Chest width
Shoulder width
Width at widest part of body
*add 1-2” at hips
Measurements in Sagittal Plane
Seat to top of the head
Seat to axilla/inferior angle of the scapula
Seat to shoulder
Seat to elbow
Chest depth
Back to popliteal
Popliteal to heel
Seat to top of head
Note fwd head
Selection of back and headrest
Seat to shoulder
Back and cushion selection
Seat to axilla/inf angle of scap
Determines back height (PSIS to AC joint)
Chair conversion dependent on functional level
If propelling keep scaps free for ROM
Power WC/tilt in space has back above scaps
Seat to elbow
symmetry
armrest type
cushion selection

Chest depth
use of chest positioning devices
Lat position